On Cancer, COVID-19, and CT Scans: A Monocentric Retrospective Study

 , ,
, ,
Abstract
1. Introduction
2. Methods
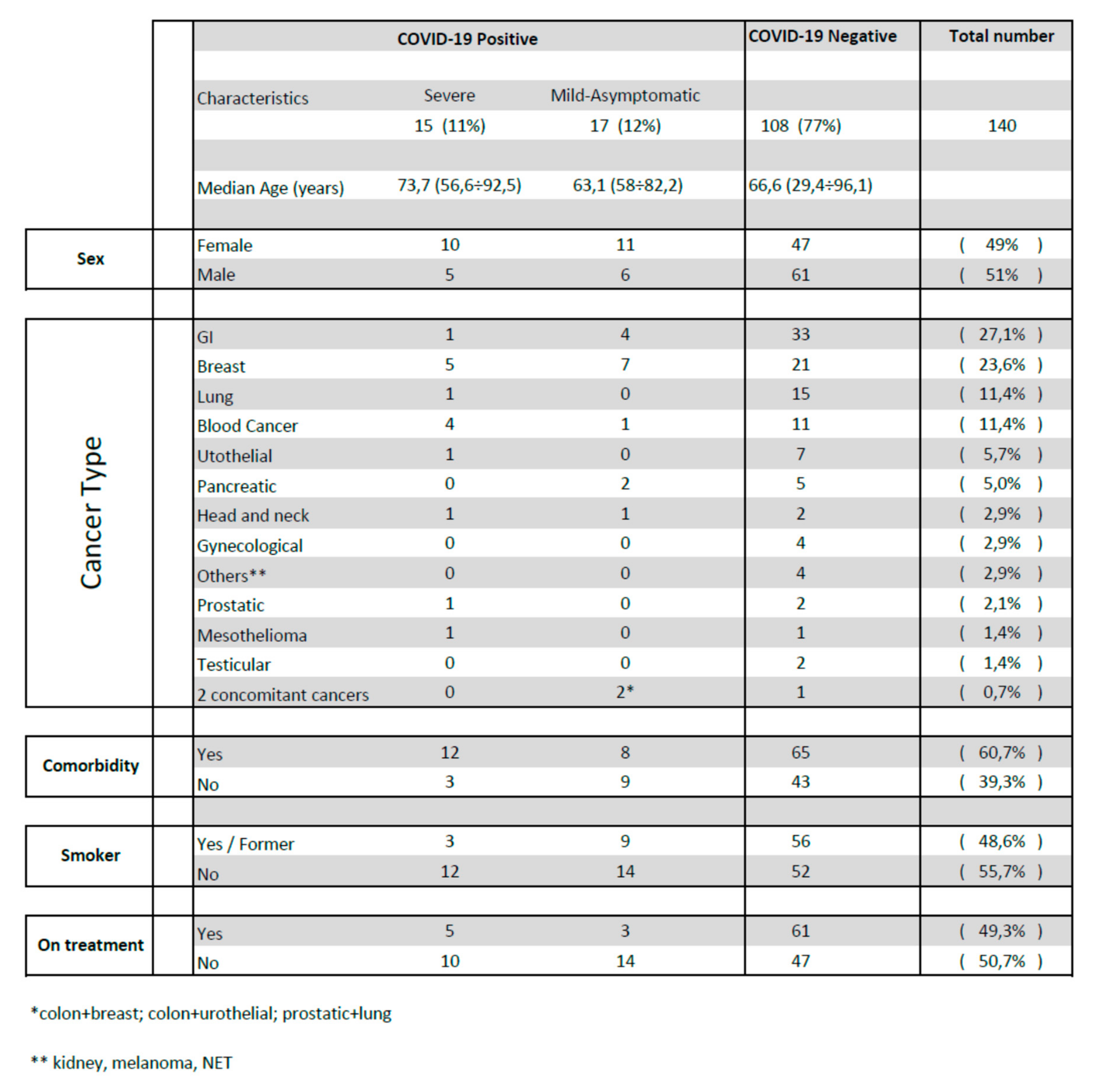
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Ethical Approval and Consent to Participate
Availability of Data and Materials
List of Abbreviations
| CT | computed tomography |
| RT-PCR | Real-time polymerase chain reaction |
| COVID-19 | coronavirus disease 19 |
| GGO | ground-glass opacities |
| CV | cardiovascular |
| OR | odds ratio |
| R-CHOP/R-DHAP | Rituximab–Cyclophosphamide–Hydroxydaunorubicin–Oncovin–Prednisone/Rituximab–Dexamethasone–Ara-C–Cisplatin |
| Mab | monoclonal antibody |
References
- Liang, W.; Guan, W.; Chen, R.; Wang, W.; Li, J.; Xu, K.; Li, C.; Ai, Q.; Lu, W.; Liang, H.; et al. Cancer patients in SARS-CoV-2 infection: A nationwide analysis in China. Lancet Oncol. 2020, 21, 335–337. [Google Scholar] [CrossRef]
- Yu, J.; Ouyang, W.; Chua, M.L.K.; Xie, C. SARS-CoV-2 Transmission in Patients with Cancer at a Tertiary Care Hospital in Wuhan, China. JAMA Oncol. 2020, 6, 1108–1110. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Zhu, F.; Xie, L.; Wang, C.; Wang, J.; Chen, R.; Jia, P.; Guan, H.; Peng, L.; Chen, Y.; et al. Clinical characteristics of COVID-19-infected cancer patients: A retrospective case study in three hospitals within Wuhan, China. Ann. Oncol. 2020, 31, 894–901. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhang, L. Risk of COVID-19 for patients with cancer. Lancet Oncol. 2020, 21, e181. [Google Scholar] [CrossRef]
- Moujaess, E.; Kourie, H.R.; Ghosn, M. Cancer patients and research during COVID-19 pandemic: A systematic review of current evidence. Crit. Rev. Oncol. 2020, 150, 102972. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Yin, J.; Qian, Y.; Wu, Y. Clinical characteristics and prognosis in cancer patients with COVID-19: A single center’s retrospective study. J. Infect. 2020, 81, 318–356. [Google Scholar] [CrossRef] [PubMed]
- Spezzani, V.; Piunno, A.; Iselin, H.U. Benign COVID-19 in an immunocompromised cancer patient—The case of a married couple. Swiss Med. Wkly. 2020, 150, w20246. [Google Scholar] [CrossRef]
- Bhoori, S.; Rossi, R.E.; Citterio, D.; Mazzaferro, V. COVID-19 in long-term liver transplant patients: Preliminary experience from an Italian transplant centre in Lombardy. Lancet Gastroenterol. Hepatol. 2020, 5, 532–533. [Google Scholar] [CrossRef]
- Kuderer, N.M.; Choueiri, T.K.; Shah, D.P.; Shyr, Y.; Rubinstein, S.M.; Rivera, D.R.; Shete, S.; Hsu, C.Y.; Desai, A.; de Lima Lopes, G.; et al. Clinical impact of COVID-19 on patients with cancer (CCC19): A cohort study. Lancet 2020, 395, 1907–1918. [Google Scholar] [CrossRef]
- Lee, L.Y.W.; Cazier, J.B.; Angelis, V.; Arnold, R.; Bisht, V.; Campton, N.A.; Chackathayil, J.; Cheng, V.W.; Curley, H.M.; Fittall, M.W.; et al. COVID-19 mortality in patients with cancer on chemotherapy or other anticancer treatments: A prospective cohort study. Lancet 2020, 395, 1919–1926. [Google Scholar] [CrossRef]
- Garassino, M.C.; Whisenant, J.G.; Huang, L.C.; Trama, A.; Torri, V.; Agustoni, F.; Baena, J.; Banna, G.; Berardi, R.; Bettini, A.C.; et al. COVID-19 in patients with thoracic malignancies (TERAVOLT): First results of an international, registry-based, cohort study. Lancet Oncol. 2020, 21, 914–992. [Google Scholar] [CrossRef]
- Robilotti, E.V.; Babady, N.E.; Mead, P.A.; Rolling, T.; Perez-Johnston, R.; Bernardes, M.; Bogler, Y.; Caldararo, M.; Figueroa, C.J.; Glickman, M.S.; et al. Determinants of COVID-19 disease severity in patients with cancer. Nat. Med. 2020, 26, 1218–1223. [Google Scholar] [CrossRef] [PubMed]
- Albiges, L.; Foulon, S.; Bayle, A.; Gachot, B.; Pommeret, F.; Willekens, C.; Stoclin, A.; Merad, M.; Griscelli, F.; Lacroix, L.; et al. Determinants of the outcomes of patients with cancer infected with SARS-CoV-2: Results from the Gustave Roussy cohort. Nat. Cancer 2020, 1, 965–975. [Google Scholar] [CrossRef]
- Fang, Y.; Zhang, H.; Xie, J.; Lin, M.; Ying, L.; Pang, P.; Ji, W. Sensitivity of Chest CT for COVID-19: Comparison to RT-PCR. Radiology 2020, 296, E115–E117. [Google Scholar] [CrossRef]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of Chest CT and RT-PCR Testing for Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef]
- Liu, J.; Yu, H.; Zhang, S. The indispensable role of chest CT in the detection of coronavirus disease 2019 (COVID-19). Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 1638–1639. [Google Scholar] [CrossRef]
- Amalou, A.; Turkbey, B.; Sanford, T.; Harmon, S.; Turkbey, E.B.; Xu, S.; An, P.; Carrafiello, G.; Cariati, M.; Patella, F.; et al. Targeted early chest CT in COVID-19 outbreaks as diagnostic tool for containment of the pandemic—A multinational opinion. Diagn. Interv. Radiol. 2020, 26, 292–295. [Google Scholar] [CrossRef]
- Xu, B.; Xing, Y.; Peng, J.; Zheng, Z.; Tang, W.; Sun, Y.; Xu, C.; Peng, F. Chest CT for detecting COVID-19: A systematic review and meta-analysis of diagnostic accuracy. Eur. Radiol. 2020, 30, 5720–5727. [Google Scholar] [CrossRef]
- Sverzellati, N.; Milanese, G.; Milone, F.; Balbi, M.; Ledda, R.E.; Silva, M. Integrated Radiologic Algorithm for COVID-19 Pandemic. J. Thorac. Imaging 2020, 35, 228–233. [Google Scholar] [CrossRef]
- Shi, H.; Han, X.; Jiang, N.; Cao, Y.; Alwalid, O.; Gu, J.; Fan, Y.; Zheng, C. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: A descriptive study. Lancet Infect. Dis. 2020, 20, 425–434. [Google Scholar] [CrossRef]
- Kelesidis, T.; Daikos, G.; Boumpas, D.; Tsiodras, S. Does rituximab increase the incidence of infectious complications? A narrative review. Int. J. Infect. Dis. 2011, 15, e2–e16. [Google Scholar] [CrossRef] [PubMed]
- Lancman, G.; Mascarenhas, J.; Bar-Natan, M. Severe COVID-19 virus reactivation following treatment for B cell acute lymphoblastic leukemia. J. Hematol. Oncol. 2020, 13, 131. [Google Scholar] [CrossRef] [PubMed]
- Sahu, K.K.; Jindal, V.; Siddiqui, A.D.; Cerny, J. Facing COVID-19 in the hematopoietic cell transplant setting: A new challenge for transplantation physicians. Blood Cells Mol. Dis. 2020, 83, 102439. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patient | Sex | Age | CT Features | Cancer Type | Chemotherapy or Follow Up | Radiotherapy | Setting | Comorbidities | Smoking | SIAARTI Stage | Hospital Admission | Nasofaringeal Swabbing | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| B.G. | F | 74.8 | GGO (24 March 2020) | Pancreas | Gemcitabine-Abraxane | T2 N + M0 | Diabetes mellitus; Hypertension | former | Asymptomatic | No | Negative (30 March 2020) | Alive | |
| B.V. | M | 56.8 | GGO (28 April 2020) | Colon | FOLFIRI–Bevacizumab | Advanced | No | No | II (fever) | No | Negative (27 April 2020) | Alive | |
| B.M. | F | 53.5 | GGO (resolving) 28 April 2020 | Breast | Follow-up | T2N3M0 | No | Former | Asymtomatic | No | No | Alive | |
| B.G. | M | 73.0 | GGO (12 March 2020) | Abdominal mesothelioma | Carboplatin–pemetrexed | Advanced, progression of disease | Dyslipidemia, previous colon cancer | No | III (fatigue, anorexia, abdominal pain) | No | Negative (12 March 2020) | Alive | |
| C.M. | F | 61.01 | GGO (7 February 2020) | Colon + breast | FOLFOX; Everolimus + exemestane ongoing | T3 N1b M0 (colon); IV stadio (breast) | No | Former | Asymptomatic | No | No | Alive | |
| F.G. | F | 72.1 | GGO (6 February 2020) | Breast | Follow-up | T1bN0 | Diabetes mellitus; Hypertension; ischemic cardiomiopathy | Former | Asymtpomatic | No | No (household members affected by COVID-19) | Alive | |
| F.T. | F | 79.52 | GGO (12 March 2020) | Colon and Breast | Yes | Advanced (colon); T2N0 (breast) | Pulmonary Embolism; Hypertension; Congestive heart failure; Chronic kidney disease | No | Asymptomatic | No | No | Alive | |
| G.M. | F | 74.5 | GGO and left pulmonary consolidation (27 April 2020) | Breast | Carboplatin | Advanced | Pulmonary embolism; dyslipidemia | No | II (cought) | No | No (symptoms referred after remission) | Alive | |
| M.M. | F | 58.02 | GGO (1 February 2020) | Oesophageal | FLOT | Locally advanced (neoadjuvant) | Si | Asymptomatic | No | No | Alive | ||
| M.T. | F | 70.3 | GGO (14 March 2020) | Breast | Paclitaxel–Bevacizumab | 20 Gy (bone metastasis) | T2 N0 M1 | Pulmonary embolism | former | III (fever dyspnea) | Yes | Positive (14 March 2020) | Alive |
| S.G. | M | 82.15 | GGO and pulmonary consolidation (20 April 2020) | Urothelial and colon | FOLFOX | T3N2b (colon) adjuvant | Hypertension, COPD | Former | II (fever) | No | Positive (20 April 2020) | Alive | |
| S.G. | M | 68.6 | GGO (6 April 2020) | Bone metastasis of gastric cancer | 20 Gy (bone metastasis) | Advanced | Pulmonary embolism | Asymptomatic | yes for pulmonary embolism | Negative (16 April 2020) 10 days after CT scan) | Alive | ||
| S.O. | F | 41.95 | GGO and pulmonary consolidation (17 March 2020) | Breast | Adriamycine-cyclophosphamide–taxol | T4 N2bM0 (neoadjuvant) | No | No | Asymptomatic | No | Positive (24 March 2020) | Alive | |
| T.E. | M | 56.8 | GGO (1 April 2020) | Pancreas | FOLFIRINOX | T4N1 | Hypertension | No | II (fever, cought) | No | Positive (2 April 2020) | Alive | |
| T.A. | F | 70.8 | GGO (28 February 2020) | Breast | Adriamycine–cyclophosphamide | T1c N0 M0 (adjuvant) | HBV-related HCC; hypothyroidism, previous gastric cancer; coeliac disease; COPD | former | Asymptomatic | No | No | Alive | |
| V.G. | M | 76.3 | GGO and pulmonary consolidation (17 March 2020) | NHL DLBCL | Follow-up | I A Ann Arbor | Hypertension, rheumatoid arthritis | No | Asymptomatic | No | No | Alive | |
| V.M. | M | 51.6 | GGO (7 April 2020) | Head and neck | Cisplatin | Yes | T3 N0/1 M0 | HCV | Yes | Asymptomatic | No | Negative (17 April 2020) | Alive |
| Z.L. | F | 56.7 | GGO (26 March 2020) | NHL MCL | R-CHOP/R-DHAP | IV Ann Arbor | Previous choroidal melanoma | No | III → VI (fever and cough at the onset) | Yes ICU | Positive (26 March 2020) | Dead | |
| S.G. | M | 74.3 | GGO (2 April 2020) | Prostatic | Follow-up | Not followed in our hospital | Hypovitaminosis D | No | III (fever, cought) | Yes | Positive (2 April 2020) | Alive | |
| R.R. | F | 65.47 | patchy shadowing pulmonary consolidation (8 April 2020) | Head and neck | Carboplatin | Yes | T1N3b adjuvant. Not followed in our hospital | Hypertension, COPD, peripheral arterial disease, pulmonary embolism | Former | III (dyspnea, cough) concomitant pulmonary embolism | Yes | Negative (8 April 2020) | Alive |
| M.L. | F | 78.15 | GGO (19 March 2020) | Breast | Follow-up | Not followed in our hospital | Hypertension, radiation induced pulmonary fibrosis | No | III → VI (fever, dyspnea, cough at the onset) | Yes ICU | Positive (19 March 2020) | Dead | |
| B.A. | F | 72.27 | GGO (16 March 2020) | Breast | Follow-up | T1cN0 | Hypertension, Diabetes mellitus, Dyslipidemia | No | III (fever, dyspnea) | Yes | Positive (16 March 2020) | Alive | |
| C.M. | F | 77.4 | GGO, pulmonary consolidation (30 March 2020) | Breast | Follow-up | Advanced | Hypertension | No | II → VI (nausea, fever, anorexia) | Yes ICU | Positive (30 March 2020) | Dead | |
| R.M. | M | 78.3 | GGO (16 March 2020) | Urothelial | Follow-up | Not followed in our hospital | Hypertension, COPD, congestive heart failure, atrial fibrilation, ictus | No | III → VI (nausea, fever, anorexia) | Yes | Positive (16 March 2020) | Dead | |
| N.G. | F | 86.7 | Bilateral interstitial abnormalities; pulmonary consolidation (6 April 2020) | CLL | Watch-and-wait follow up (never treated) | Hypertension, diabetes mellitus | No | III → VI (fever, cough, dyspnea, asthenia) | Yes | Positive (6 April 2020) | Dead | ||
| M.L. | F | 62.29 | GGO (4 April 2020) | HD | ABVD 6 cycles | IV b Ann Arbor. Not followed in our hospital | Previous gynecological cancer | No | III (fever) | Yes | Positive (4 April 2020) | Alive | |
| S.M. | F | 75.13 | GGO (30 March 2020) | Breast | Follow-up | Not followed in our hospital | Hypertension, atrial fibrillation, diabetes mellitus | No | III → VI (fever, asthenia, cough) | Yes | Positive (30 March 2020) | Dead | |
| G.C. | F | 92.54 | GGO (30 April 2020) | Gastric | Follow-up | T3N0 | Previous breast cancer, hypertension, chronic gastric reflux | No | III (dyspnea) concomitant atrial fibrillation and congestive heart failure | Yes | Negative (30 April 2020) | Alive | |
| C.E. | M | 56.5 | GGO and pulmonary consolidations (9 April 2020) | CLL | Follow-up | Not followed in our hospital | No | No | III (fever, cought, dyspnea) | Yes | Positive (9 April 2020) | Alive | |
| M.L. | M | 85.79 | GGO (31 March 2020) | Lung | Follow-up | Advanced, Progression disease. Not followed in our hospital | Dyslipidemia, hypertension, COPD, chronic renal disease | Former | III (dyspnea, fever) | Yes | Positive (31 March 2020) | Alive | |
| F.N. | F | 54 | Negative (14 March 2020) | Breast | Adriamycine–cyclophosphamide | Locally advanced (neoadjuvant) | No | No | II (fever) | No | Positive (3 March 2020) | Alive | |
| S.A. | F | 40 | Negative (2 April 2020) CT scan after symptoms’ remission | Breast | Trastuzumab | T2N1M1 | Hypothyroidism, multiple sclerosis | No | II (fever, cought) | No | Positive (20th March 2020) | Alive |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martini, F.; D’Alessio, A.; Bracchi, F.; Di Mauro, D.; Fargnoli, A.; Motta, M.; Giussani, C.; Meazza Prina, M.; Gobbin, G.; Taverna, M. On Cancer, COVID-19, and CT Scans: A Monocentric Retrospective Study. J. Clin. Med. 2020, 9, 3935. https://doi.org/10.3390/jcm9123935
Martini F, D’Alessio A, Bracchi F, Di Mauro D, Fargnoli A, Motta M, Giussani C, Meazza Prina M, Gobbin G, Taverna M. On Cancer, COVID-19, and CT Scans: A Monocentric Retrospective Study. Journal of Clinical Medicine. 2020; 9(12):3935. https://doi.org/10.3390/jcm9123935
Chicago/Turabian StyleMartini, Francesca, Andrea D’Alessio, Federico Bracchi, Daniela Di Mauro, Anna Fargnoli, Marco Motta, Cristina Giussani, Marco Meazza Prina, Giovanni Gobbin, and Monica Taverna. 2020. "On Cancer, COVID-19, and CT Scans: A Monocentric Retrospective Study" Journal of Clinical Medicine 9, no. 12: 3935. https://doi.org/10.3390/jcm9123935
APA StyleMartini, F., D’Alessio, A., Bracchi, F., Di Mauro, D., Fargnoli, A., Motta, M., Giussani, C., Meazza Prina, M., Gobbin, G., & Taverna, M. (2020). On Cancer, COVID-19, and CT Scans: A Monocentric Retrospective Study. Journal of Clinical Medicine, 9(12), 3935. https://doi.org/10.3390/jcm9123935