Prevalence and Outcomes of Acute Hypoxaemic Respiratory Failure in Wales: The PANDORA-WALES Study

 , , ,
, , ,  ,
,  and
and
Abstract
1. Introduction
2. Experimental Section
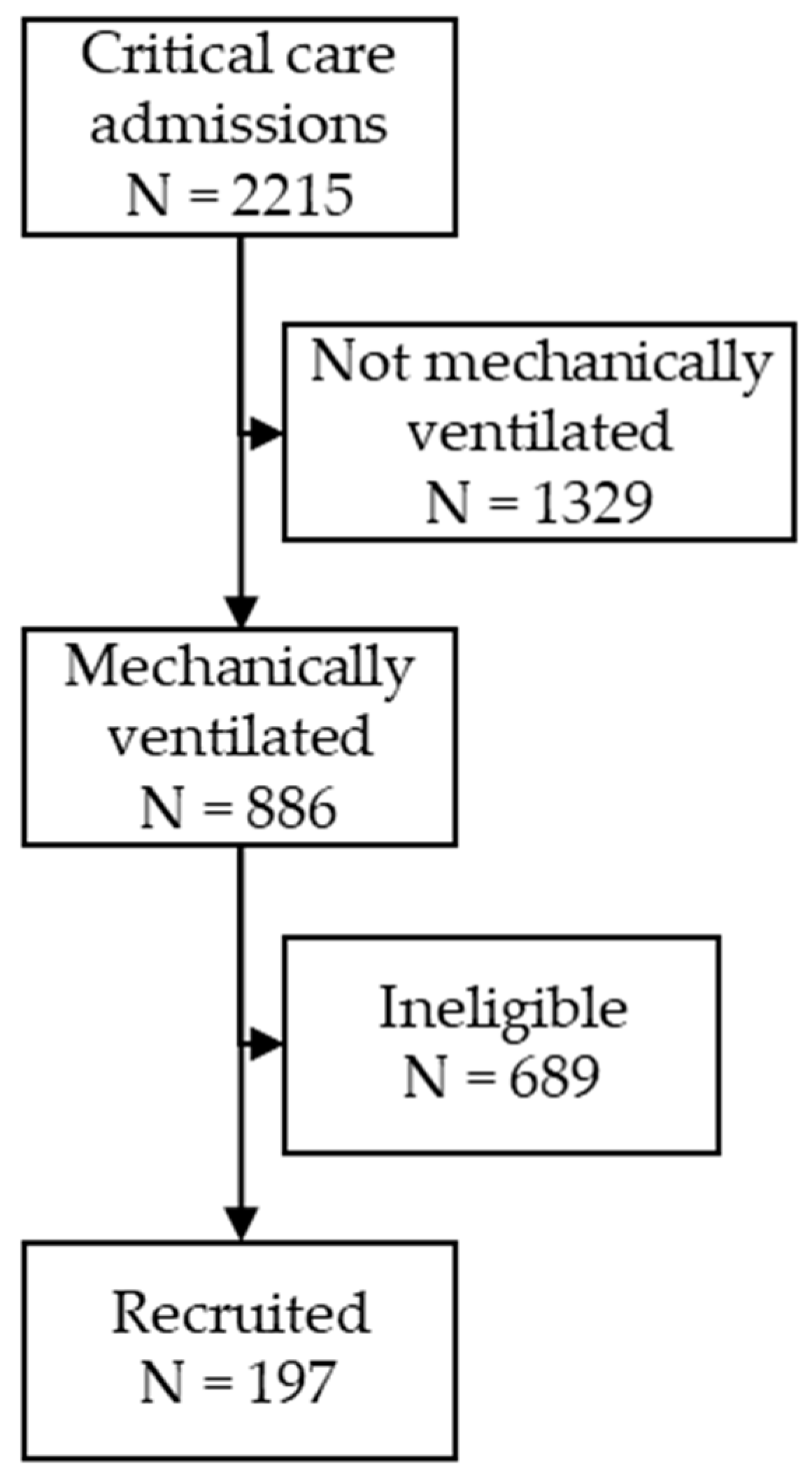
2.1. Study Design and Participants
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
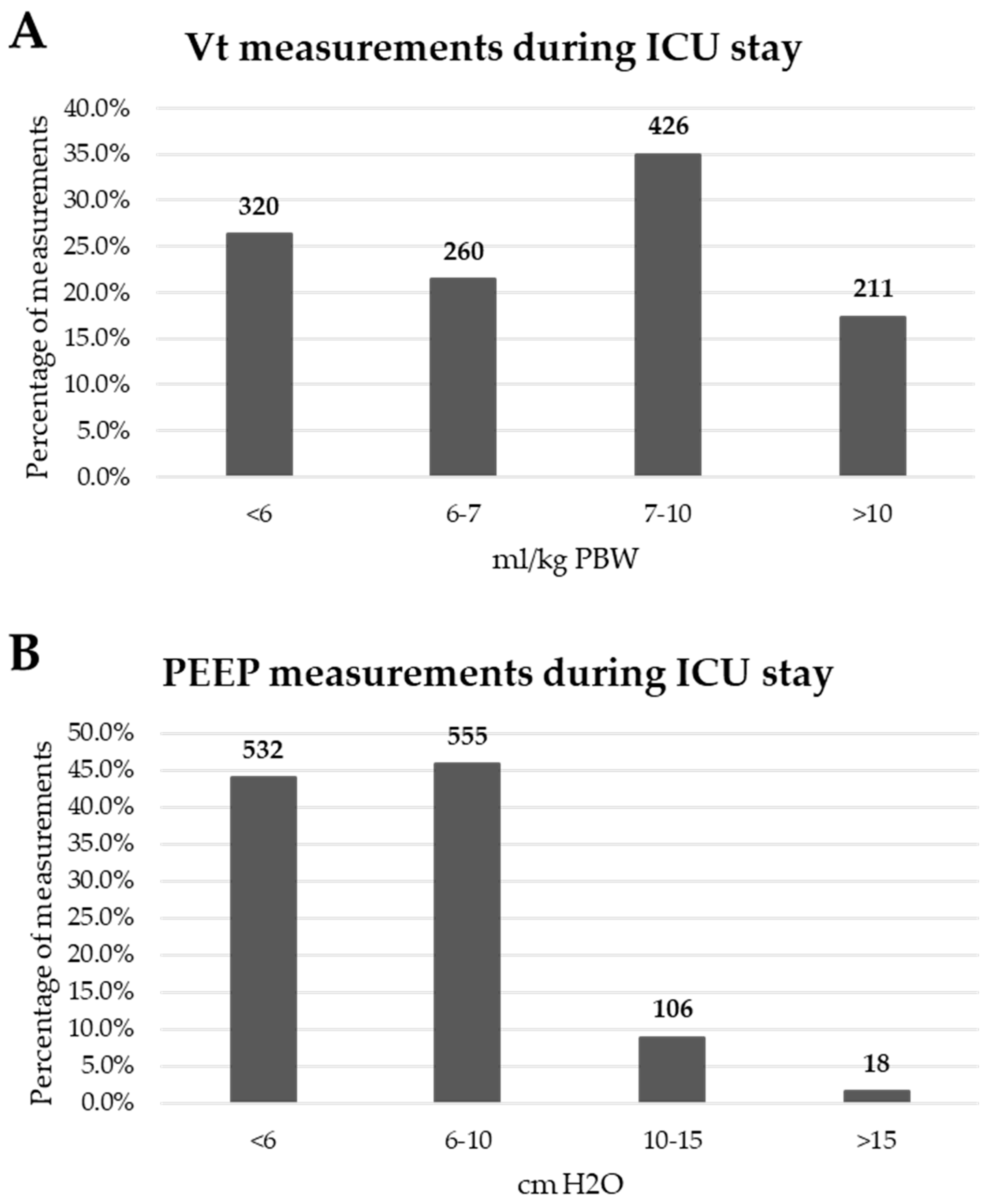
3.2. Patient Ventilation
3.3. Patient Management
3.4. Complications and Survival Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Villar, J.; Blanco, J.; Añón, J.M.; Santos-Bouza, A.; Blanch, L.; Ambrós, A.; Gandía, F.; Carriedo, D.; Mosteiro, F.; Basaldúa, S.; et al. The ALIEN study: Incidence and outcome of acute respiratory distress syndrome in the era of lung protective ventilation. Intensive Care Med. 2011, 37, 1932–1941. [Google Scholar] [CrossRef] [PubMed]
- Luhr, O.R.; Antonsen, K.; Karlsson, M.; Aardal, S.; Thorsteinsson, A.; Frostell, C.; Bonde, J.; the ARF Study Group. Incidence and Mortality after Acute Respiratory Failure and Acute Respiratory Distress Syndrome in Sweden, Denmark, and Iceland. Am. J. Respir. Crit. Care Med. 1999, 159, 1849–1861. [Google Scholar] [CrossRef] [PubMed]
- The ARDS Definition Task Force. Acute Respiratory Distress Syndrome: The Berlin Definition of ARDS. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Villar, J.; Epidemiology, S.S.I.F.; Pérez-Méndez, L.; Blanco, J.; Anon, J.M.; Blanch, L.; Belda, J.; Santos-Bouza, A.; Fernández, R.L.; Kacmarek, R.M. A universal definition of ARDS: The PaO2/FiO2 ratio under a standard ventilatory setting—A prospective, multicenter validation study. Intensive Care Med. 2013, 39, 583–592. [Google Scholar] [CrossRef] [PubMed]
- Papazian, L.; Forel, J.-M.; Gacouin, A.; Penot-Ragon, C.; Perrin, G.; Loundou, A.; Jaber, S.; Arnal, J.-M.; Perez, D.; Seghboyan, J.-M.; et al. Neuromuscular Blockers in Early Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2010, 363, 1107–1116. [Google Scholar] [CrossRef] [PubMed]
- Valta, P.; Uusaro, A.; Nunes, S.; Ruokonen, E.; Takala, J. Acute respiratory distress syndrome: Frequency, clinical course, and costs of care. Crit. Care Med. 1999, 27, 2367–2374. [Google Scholar] [CrossRef]
- Azevedo, L.C.P.; Park, M.; Salluh, J.I.F.; Rea-Neto, A.; Souza-Dantas, V.C.; Varaschin, P.; Oliveira, M.C.; Tierno, P.F.; Dal-Pizzol, F.; Silva, U.V.A.; et al. Clinical outcomes of patients requiring ventilatory support in Brazilian intensive care units: A multicenter, prospective, cohort study. Crit. Care 2013, 17, R63. [Google Scholar] [CrossRef]
- Sharif, B.; Lundin, R.M.; Morgan, P.; Hall, J.; Dhadda, A.; Mann, C.; Donoghue, D.; Brownlow, E.; Hill, F.; Carr, G.; et al. Developing a digital data collection platform to measure the prevalence of sepsis in Wales. J. Am. Med. Inform. Assoc. 2016, 23, 1185–1189. [Google Scholar] [CrossRef]
- Bertolini, G.; Lewandowski, K.; Bion, J.; Romand, J.-A.; Villar, J.S.; Thorsteinsson, A.; Damas, P.; Armaganidis, A.; Lemaire, F.; Brun-Buisson, C.; et al. Epidemiology and outcome of acute lung injury in European intensive care units. Intensive Care Med. 2004, 30, 51–61. [Google Scholar] [CrossRef]
- Grimaldi, D.; Hraiech, S.; Boutin, E.; Lacherade, J.C.; Boissier, F.; Pham, T.; Richard, J.C.; Thille, A.W.; Ehrmann, S.; Lascarrou, J.B.; et al. Hypoxemia in the ICU: Prevalence, treatment, and outcome. Ann. Intensive Care 2018, 8, 82. [Google Scholar] [CrossRef]
- Linko, R.; Okkonen, M.; Pettilä, V.; Perttilä, J.; Parviainen, I.; Ruokonen, E.; Tenhunen, J.; Ala-Kokko, T.; Varpula, T.; The FINNALI-study group. Acute respiratory failure in intensive care units. FINNALI: A prospective cohort study. Intensive Care Med. 2009, 35, 1352–1361. [Google Scholar] [CrossRef] [PubMed]
- Neto, A.S.; Barbas, C.S.V.; Simonis, F.D.; Artigas-Raventos, A.; Canet, J.; Determann, R.M.; Anstey, J.; Hedenstierna, G.; Hemmes, S.N.T.; Hermans, G.; et al. Epidemiological characteristics, practice of ventilation, and clinical outcome in patients at risk of acute respiratory distress syndrome in intensive care units from 16 countries (PRoVENT): An international, multicentre, prospective study. Lancet Respir. Med. 2016, 4, 882–893. [Google Scholar] [CrossRef]
- Bellani, G.; Laffey, J.G.; Pham, T.; Fan, E.; Brochard, L.; Esteban, A.; Gattinoni, L.; Van Haren, F.; Larsson, A.; McAuley, D.F.; et al. Epidemiology, Patterns of Care, and Mortality for Patients With Acute Respiratory Distress Syndrome in Intensive Care Units in 50 Countries. JAMA 2016, 315, 788–800. [Google Scholar] [CrossRef]
- Laffey, J.G.; Madotto, F.; Pham, T.; Bajwa, E.K.; Lorente, J.A.; Jiménez, J.I.S.; McAuley, D.F.; Slutsky, A.S.; Laffey, J.G.; Bellani, G.; et al. Geo-economic variations in epidemiology, patterns of care, and outcomes in patients with acute respiratory distress syndrome: Insights from the LUNG SAFE prospective cohort study. Lancet Respir. Med. 2017, 5, 627–638. [Google Scholar] [CrossRef]
- Villar, J.; Pérez-Méndez, L.; Kacmarek, R.M. The Berlin definition met our needs: No. Intensive Care Med. 2016, 42, 648–650. [Google Scholar] [CrossRef]
- Pham, T.; Neto, A.S.; Pelosi, P.; Laffey, J.G.; De Haro, C.; Lorente, M.D.C.; Bellani, G.; Fan, E.; Brochard, L.J.; Pesenti, A.; et al. Outcomes of Patients Presenting with Mild Acute Respiratory Distress Syndrome. Anesthesiology 2019, 130, 263–283. [Google Scholar] [CrossRef]
- Hsu, C.-H.; Hung, Y.; Chu, K.-A.; Chen, C.-F.; Yin, C.-H.; Lee, C.-C. Prognostic nomogram for elderly patients with acute respiratory failure receiving invasive mechanical ventilation: A nationwide population-based cohort study in Taiwan. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- Schmidt, M.F.S.; Amaral, A.C.K.B.; Fan, E.; Rubenfeld, G. Driving Pressure and Hospital Mortality in Patients without ARDS: A Cohort Study. Chest 2017, 153, 46–54. [Google Scholar] [CrossRef]
- Urner, M.; Jüni, P.; Hansen, B.; Wettstein, M.S.; Ferguson, N.D.; Fan, E. Time-varying intensity of mechanical ventilation and mortality in patients with acute respiratory failure: A registry-based, prospective cohort study. Lancet Respir. Med. 2020, 8, 905–913. [Google Scholar] [CrossRef]
- Rezoagli, E.; Gatti, S.; Villa, S.; Villa, G.; Muttini, S.; Rossi, F.; Faraldi, L.; Fumagalli, R.; Grasselli, G.; Foti, G.; et al. ABO blood types and major outcomes in patients with acute hypoxaemic respiratory failure: A multicenter retrospective cohort study. PLoS ONE 2018, 13, e0206403. [Google Scholar] [CrossRef]
- Szakmany, T.; Walters, A.M.; Pugh, R.; Battle, C.; Berridge, D.M.; Lyons, R.A. Risk Factors for 1-Year Mortality and Hospital Utilization Patterns in Critical Care Survivors. Crit. Care Med. 2019, 47, 15–22. [Google Scholar] [CrossRef] [PubMed]
- Sakr, Y.; Moreira, C.L.; Rhodes, A.; Ferguson, N.D.; Kleinpell, R.; Pickkers, P.; Kuiper, M.A.; Lipman, J.; Vincent, J.-L. The Impact of Hospital and ICU Organizational Factors on Outcome in Critically Ill Patients. Crit. Care Med. 2015, 43, 519–526. [Google Scholar] [CrossRef] [PubMed]
- Capuzzo, M.; Volta, C.A.; Tassinati, T.; Moreno, R.P.; Valentin, A.; Guidet, B.; Iapichino, G.; Martin, C.; Perneger, T.; Combescure, C.; et al. Hospital mortality of adults admitted to Intensive Care Units in hospitals with and without Intermediate Care Units: A multicentre European cohort study. Crit. Care 2014, 18, 1–15. [Google Scholar] [CrossRef]
- McNicholas, B.A.; Madotto, F.; Pham, T.; Rezoagli, E.; Masterson, C.H.; Horie, S.; Bellani, G.; Brochard, L.; Laffey, J.G. Demographics, management and outcome of women and men with Acute Respiratory Distress Syndrome in the LUNG SAFE prospective cohort study. Eur. Respir. J. 2019, 54, 1900609. [Google Scholar] [CrossRef]
- Acute Respiratory Distress Syndrome Network; Brower, R.G.; Matthay, M.A.; Morris, A.; Schoenfeld, D.; Thompson, B.T.; Wheeler, A. Ventilation with Lower Tidal Volumes as Compared with Traditional Tidal Volumes for Acute Lung Injury and the Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2000, 342, 1301–1308. [Google Scholar] [CrossRef]
- Tenney, S.M.; Remmers, J.E. Comparative Quantitative Morphology of the Mammalian Lung: Diffusing Area. Nat. Cell Biol. 1963, 197, 54–56. [Google Scholar] [CrossRef] [PubMed]
- Calfee, C.S.; Delucchi, K.L.; Sinha, P.; Matthay, M.A.; Hackett, J.; Shankar-Hari, M.; McDowell, C.; Laffey, J.G.; O’Kane, C.M.; McAuley, D.F.; et al. Acute respiratory distress syndrome subphenotypes and differential response to simvastatin: Secondary analysis of a randomised controlled trial. Lancet Respir. Med. 2018, 6, 691–698. [Google Scholar] [CrossRef]
- Davies, J.D.; Senussi, M.H.; Mireles-Cabodevila, E. Should a Tidal Volume of 6 mL/kg Be Used in All Patients? Respir. Care 2016, 61, 774–790. [Google Scholar] [CrossRef]
- Lanspa, M.J.; Peltan, I.D.; Jacobs, J.; Sorensen, J.S.; Carpenter, L.; Ferraro, J.P.; Brown, S.M.; Berry, J.G.; Srivastava, R.; Grissom, C.K. Driving pressure is not associated with mortality in mechanically ventilated patients without ARDS. Crit. Care 2019, 23, 424–428. [Google Scholar] [CrossRef]
- Simonis, F.D.; Serpa Neto, A.; Binnekade, J.M.; Braber, A.; Bruin, K.C.M.; Determann, R.M.; Goekoop, G.-J.; Heidt, J.; Horn, J.; Innemee, G.; et al. Effect of a Low vs Intermediate Tidal Volume Strategy on Ventilator-Free Days in Intensive Care Unit Patients Without ARDS A Randomized Clinical Trial. JAMA 2018, 320, 1872–1880. [Google Scholar] [CrossRef]
- Guérin, C.; Reignier, J.; Richard, J.-C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone Positioning in Severe Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2013, 368, 2159–2168. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, C.L.; Goligher, E.C.; Young, M.E.; Keating, J.L.; Holland, A.E.; Romero, L.; Bradley, S.J.; Tuxen, D. Recruitment manoeuvres for adults with acute respiratory distress syndrome receiving mechanical ventilation. Cochrane Database Syst. Rev. 2016, 11, CD006667. [Google Scholar] [CrossRef] [PubMed]
- Constantin, J.-M.; Jabaudon, M.; Lefrant, J.-Y.; Jaber, S.; Quenot, J.-P.; Langeron, O.; Ferrandière, M.; Grelon, F.; Seguin, P.; Ichai, C.; et al. Personalised mechanical ventilation tailored to lung morphology versus low positive end-expiratory pressure for patients with acute respiratory distress syndrome in France (the LIVE study): A multicentre, single-blind, randomised controlled trial. Lancet Respir. Med. 2019, 7, 870–880. [Google Scholar] [CrossRef]
- Cavalcanti, A.B.; Suzumura, É.A.; Laranjeira, L.N.; Paisani, D.D.M.; Damiani, L.P.; Guimarães, H.P.; Romano, E.R.; Regenga, M.D.M.; Taniguchi, L.N.T.; de Oliveira, R.P.; et al. Effect of Lung Recruitment and Titrated Positive End-Expiratory Pressure (PEEP) vs Low PEEP on Mortality in Patients with Acute Respiratory Distress Syndrome. JAMA 2017, 318, 1335–1345. [Google Scholar] [CrossRef] [PubMed]
- National Heart, Lung, and Blood Institute PETAL Clinical Trials Network; Moss, M.; Huang, D.T.; Brower, R.G.; Ferguson, N.D.; Ginde, A.A.; Gong, M.N.; Grissom, C.K.; Gundel, S.; Hayden, D.; et al. Early Neuromuscular Blockade in the Acute Respiratory Distress Syndrome. N. Engl. J. Med. 2019, 380, 1997–2008. [Google Scholar] [CrossRef]
- Szakmany, T.; Pugh, R.; Kopczynska, M.; Lundin, R.M.; Sharif, B.; Morgan, P.; Ellis, G.; Abreu, J.; Kulikouskaya, S.; Bashir, K.; et al. Defining sepsis on the wards: Results of a multi-centre point-prevalence study comparing two sepsis definitions. Anaesthesia 2017, 73, 195–204. [Google Scholar] [CrossRef]
- Kopczynska, M.; Sharif, B.; Unwin, H.; Lynch, J.; Forrester, A.; Zeicu, C.; Cleaver, S.; Kulikouskaya, S.; Chandy, T.; Ang, E.; et al. Real World Patterns of Antimicrobial Use and Microbiology Investigations in Patients with Sepsis outside the Critical Care Unit: Secondary Analysis of Three Nation-Wide Point Prevalence Studies. J. Clin. Med. 2019, 8, 1337. [Google Scholar] [CrossRef]
- Sinha, P.; Calfee, C.S.; Cherian, S.; Brealey, D.; Cutler, S.; King, C.; Killick, C.; Richards, O.; Cheema, Y.; Bailey, C.; et al. Prevalence of phenotypes of acute respiratory distress syndrome in critically ill patients with COVID-19: A prospective observational study. Lancet Respir. Med. 2020. [Google Scholar] [CrossRef]
- Bos, L.D.J.; Paulus, F.; Vlaar, A.P.J.; Beenen, L.F.M.; Schultz, M.J. Subphenotyping Acute Respiratory Distress Syndrome in Patients with COVID-19: Consequences for Ventilator Management. Ann. Am. Thorac. Soc. 2020, 17, 1161–1163. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patient Characteristics | Number of Patients, Percentage (n = 197) |
|---|---|
| Demographics | |
| Age (years) | 60 (49–70) |
| Male sex | 117 (59.4%) |
| Comorbidities | |
| HTN | 81 (41.1%) |
| HF | 16 (8.1%) |
| Diabetes | 27 (13.7%) |
| Obesity | 26 (13.2%) |
| Liver cirrhosis | 11 (5.6%) |
| Chronic kidney failure | 17 (8.6%) |
| Immunosuppression | 12 (6.1%) |
| Neuromuscular disease | 1 (0.5%) |
| Malignancy | 11 (5.6%) |
| Use of NIV at home | 3 (1.5%) |
| Smoking | 46 (23.4%) |
| Alcohol excess | 32 (16.2%) |
| Hospital type | |
| Tertiary hospital | 44 (22.3%) |
| District general hospital | 153 (77.7%) |
| Reason for ICU admission | |
| Clinical condition | 174 (88.3%) |
| Emergency surgery | 32 (16.2%) |
| Planned surgery | 2 (1.0%) |
| Physiology at the time of recruitment | |
| Baseline PaO2/FiO2–median mmHg (IQR) | 150 (99–209) |
| VT–median mL/kg PBW (IQR) | 6.9 (6.1–8.2) |
| Respiratory rate–median (IQR) | 19 (16–23) |
| Plateau pressure–median cm H2O (IQR) | 22 (17–25) |
| Peak pressure–median cm H2O (IQR) | 23 (19–29) |
| PEEP–median cm H2O (IQR) | 7 (5–10) |
| pH–median (IQR) | 7.28 (7.17–7.37) |
| PaCO2–median kPa (IQR) | 6.2 (5.2–7.9) |
| Ventilation Type | |||
|---|---|---|---|
| VT | Volume Controlled (n = 126) | Pressure Controlled (n = 57) | p Value |
| VT in optimal range | 76 (60.3%) | 25 (43.9%) | 0.049 |
| VT above 7 mL/kg PBW | 50 (39.7%) | 32 (56.1%) | 0.038 |
| Intervention and Monitoring | Number of Patients, Percentage (n = 197) |
|---|---|
| During the ICU stay | |
| Oesophageal pressure monitoring | 1 (0.5%) |
| Pulmonary artery catheter | 1 (0.5%) |
| Nitric oxide | 3 (1.5%) |
| Vasopressor use | 80 (40.6%) |
| Corticosteroids | 56 (28.4%) |
| Systemic vasodilators | 6 (3%) |
| Blood transfusion | 12 (6.1%) |
| Renal replacement therapy | 26 (13.2%) |
| High frequency ventilation | 2 (1%) |
| ECMO | 1 (0.5%) |
| ECCO2R | 1 (0.5%) |
| NAVA | 1 (0.5%) |
| PiCCO | 4 (2%) |
| NIV after being extubated | 1 (0.5%) |
| On the day of recruitment | |
| Neuromuscular blockade | 42 (21.3%) |
| Recruitment manoeuvres | 35 (17.8%) |
| Prone by protocol | |
| First 48 h | 2 (1%) |
| During the evolution | 1 (0.5%) |
| As a rescue | 1 (0.5%) |
| Complication | Number of Patients, Percentage (n = 197) |
|---|---|
| Pneumothorax | 2 (1%) |
| Pneumonia | 36 (18.3%) |
| Pleural effusion | 11 (5.5%) |
| Atelectasis | 4 (2%) |
| New lung infiltrates | 21 (10.7%) |
| Pulmonary oedema | 5 (2.5%) |
| Shock | 27 (13.7%) |
| Sepsis | 38 (19.3%) |
| Major surgical operation | 16 (8.1%) |
| Risk Factor | Survivor (n = 125) | Non-Survivor (n = 70) | p Value |
|---|---|---|---|
| Age | 57 (47–68) | 65 (52–72) | 0.034 |
| SOFA score | 8 (6–9) | 9 (7–11) | 0.019 |
| Alcohol excess | 15 (12.0%) | 17 (24.3%) | 0.026 |
| Inotropic support | 73 (58.4%) | 51 (72.9%) | 0.044 |
| Recruitment manoeuvres | 17 (13.6%) | 17 (24.3%) | 0.059 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kopczynska, M.; Sharif, B.; Pugh, R.; Otahal, I.; Havalda, P.; Groblewski, W.; Lynch, C.; George, D.; Sutherland, J.; Pandey, M.; et al. Prevalence and Outcomes of Acute Hypoxaemic Respiratory Failure in Wales: The PANDORA-WALES Study. J. Clin. Med. 2020, 9, 3521. https://doi.org/10.3390/jcm9113521
Kopczynska M, Sharif B, Pugh R, Otahal I, Havalda P, Groblewski W, Lynch C, George D, Sutherland J, Pandey M, et al. Prevalence and Outcomes of Acute Hypoxaemic Respiratory Failure in Wales: The PANDORA-WALES Study. Journal of Clinical Medicine. 2020; 9(11):3521. https://doi.org/10.3390/jcm9113521
Chicago/Turabian StyleKopczynska, Maja, Ben Sharif, Richard Pugh, Igor Otahal, Peter Havalda, Wojciech Groblewski, Ceri Lynch, David George, Jayne Sutherland, Manish Pandey, and et al. 2020. "Prevalence and Outcomes of Acute Hypoxaemic Respiratory Failure in Wales: The PANDORA-WALES Study" Journal of Clinical Medicine 9, no. 11: 3521. https://doi.org/10.3390/jcm9113521
APA StyleKopczynska, M., Sharif, B., Pugh, R., Otahal, I., Havalda, P., Groblewski, W., Lynch, C., George, D., Sutherland, J., Pandey, M., Jones, P., Murdoch, M., Hatalyak, A., Jones, R., Kacmarek, R. M., Villar, J., Szakmany, T., & on behalf of the PANDORA-WALES Investigators. (2020). Prevalence and Outcomes of Acute Hypoxaemic Respiratory Failure in Wales: The PANDORA-WALES Study. Journal of Clinical Medicine, 9(11), 3521. https://doi.org/10.3390/jcm9113521