Clinical Outcome and Toxicity in the Treatment of Anaplastic Thyroid Cancer in Elderly Patients


Abstract
1. Introduction
2. Patients and Methods
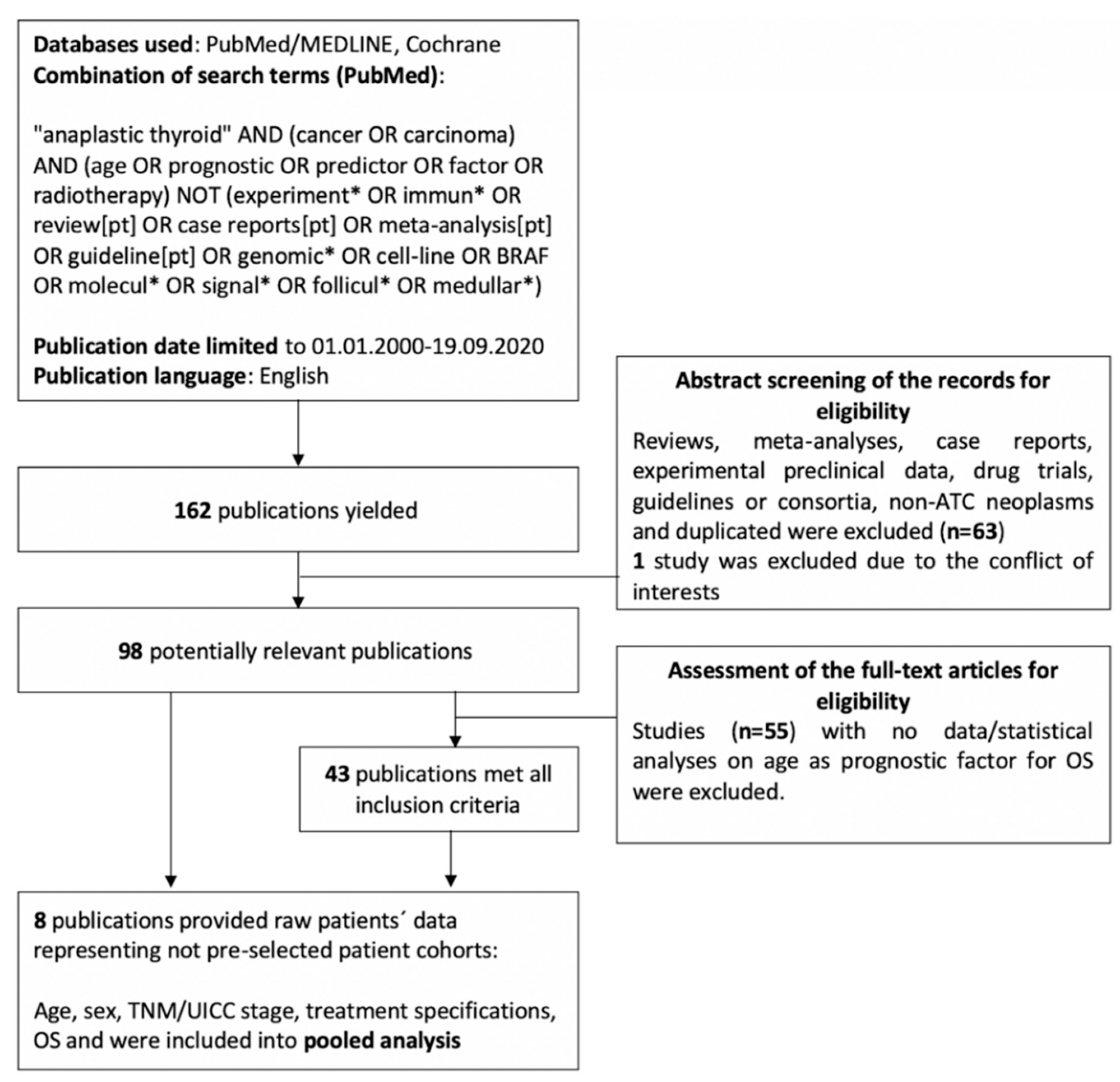
2.1. Systematic Review of Literature
2.2. Pooled Analysis
2.3. Single-Center Patient Cohort
2.4. Data Acquisition
2.5. Criteria for Multimodal Treatment Approach
2.6. Statistical Analysis
3. Results
3.1. Systematic Review of Literature
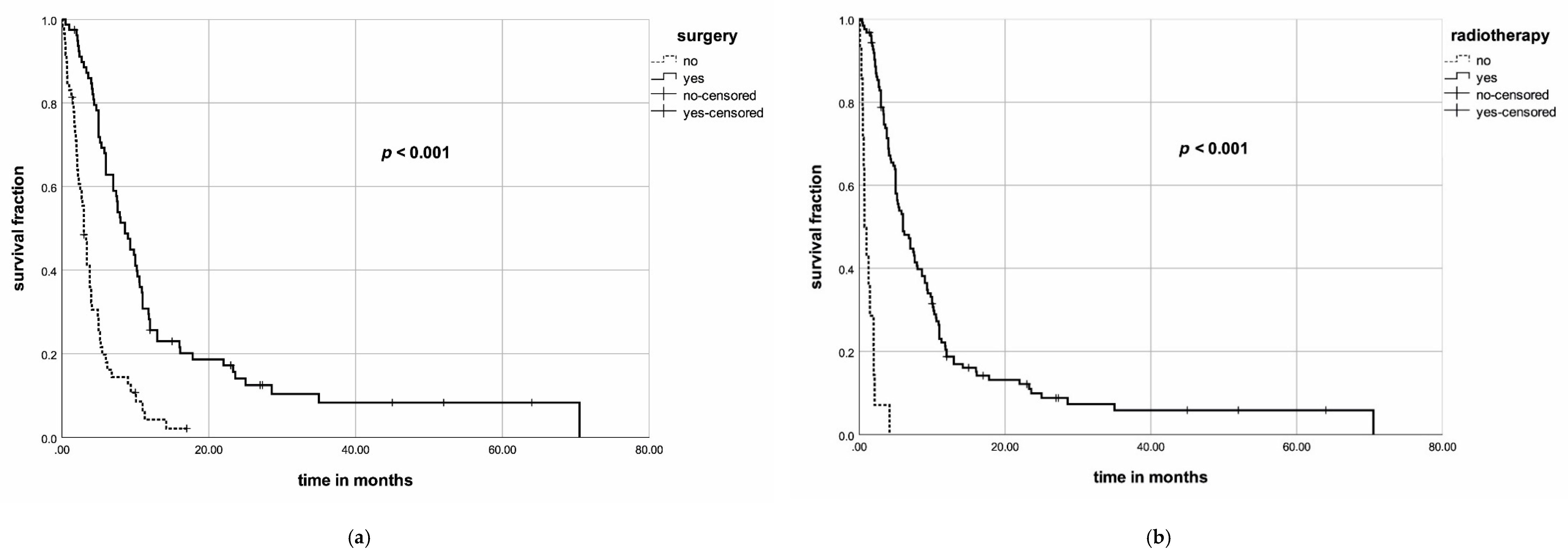
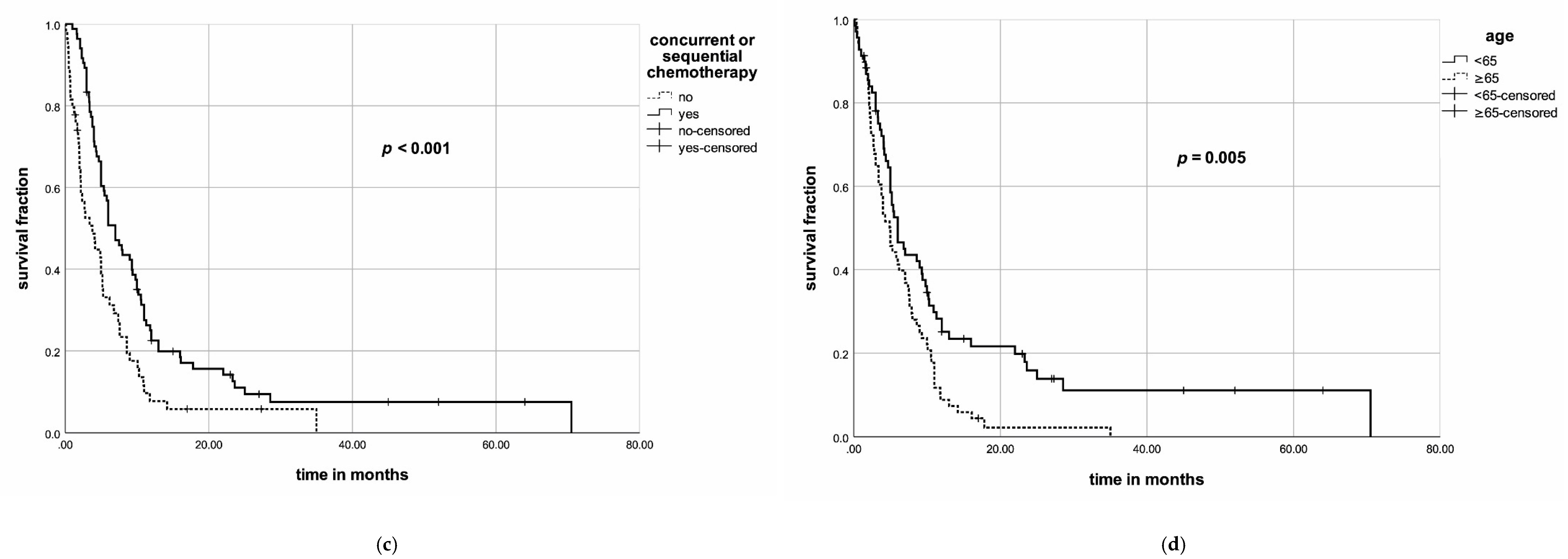
3.2. Results of the Pooled Analysis
3.3. Propensity Score Matching (PSM)
3.4. Patient Characteristics of Our Single-Center Cohort
3.5. Treatment-Related Characteristics
3.6. Treatment-Related Toxicities
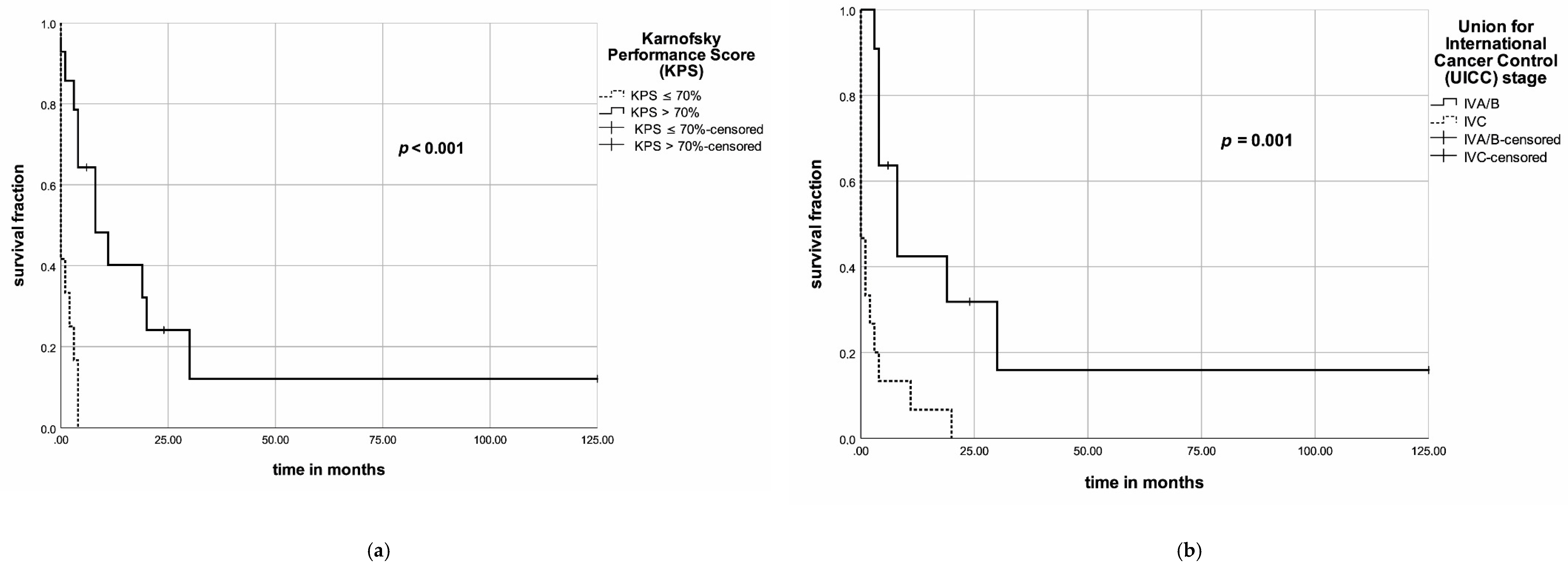
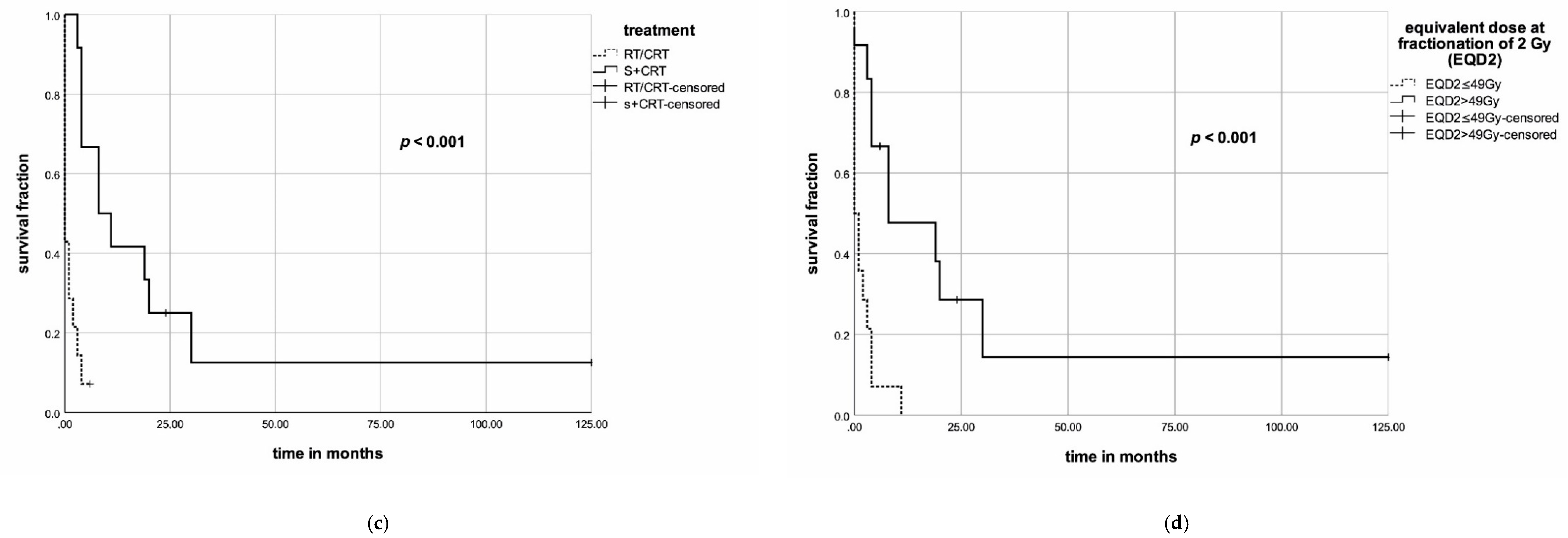
3.7. Outcomes on Survival and Relapse in the Single-Center Evaluation
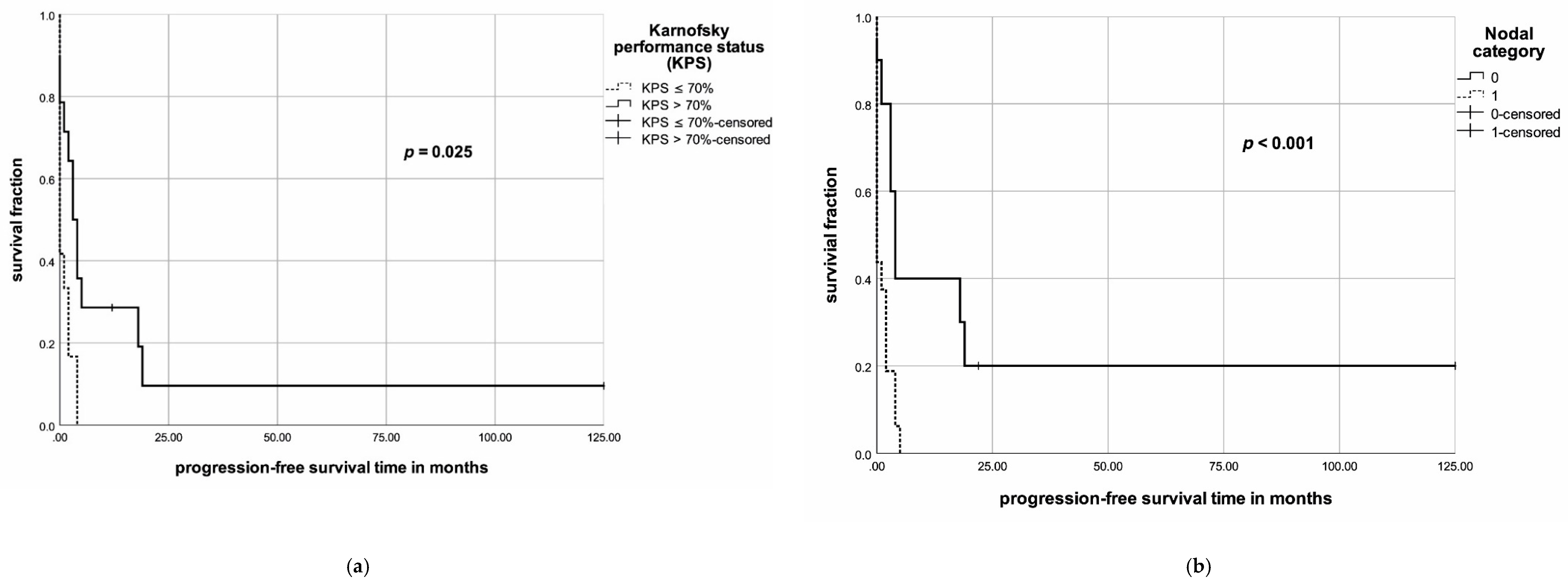
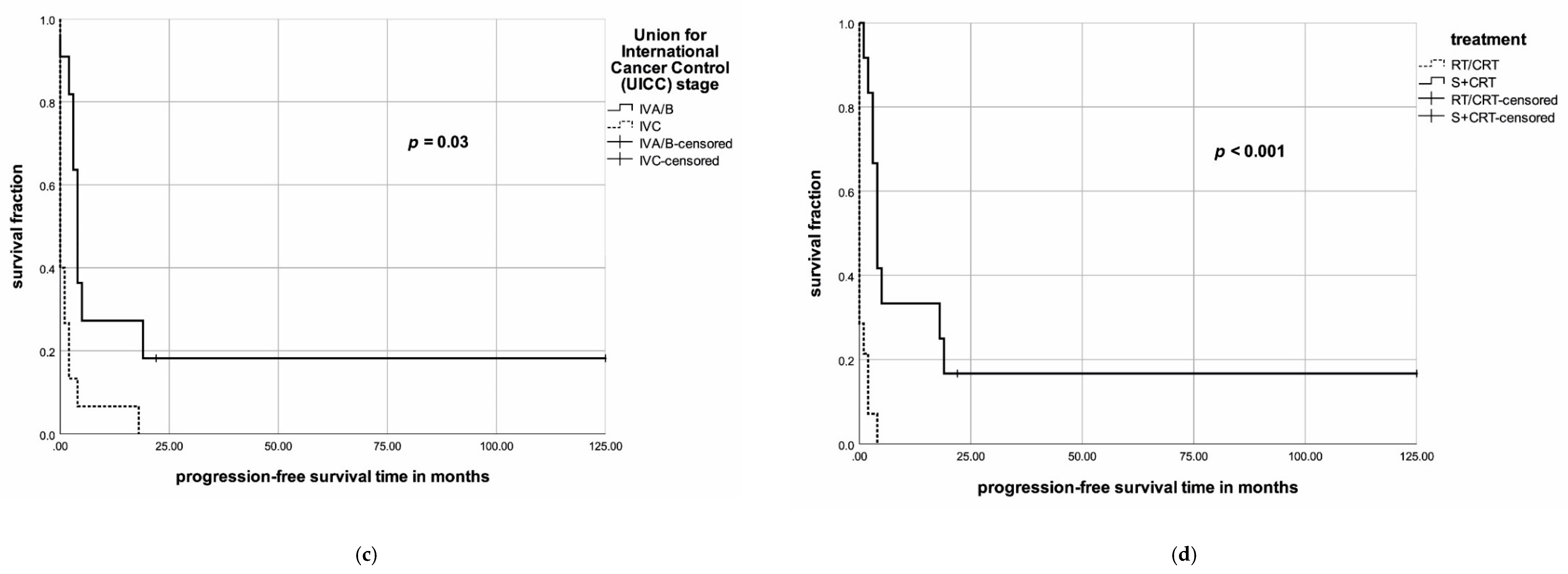
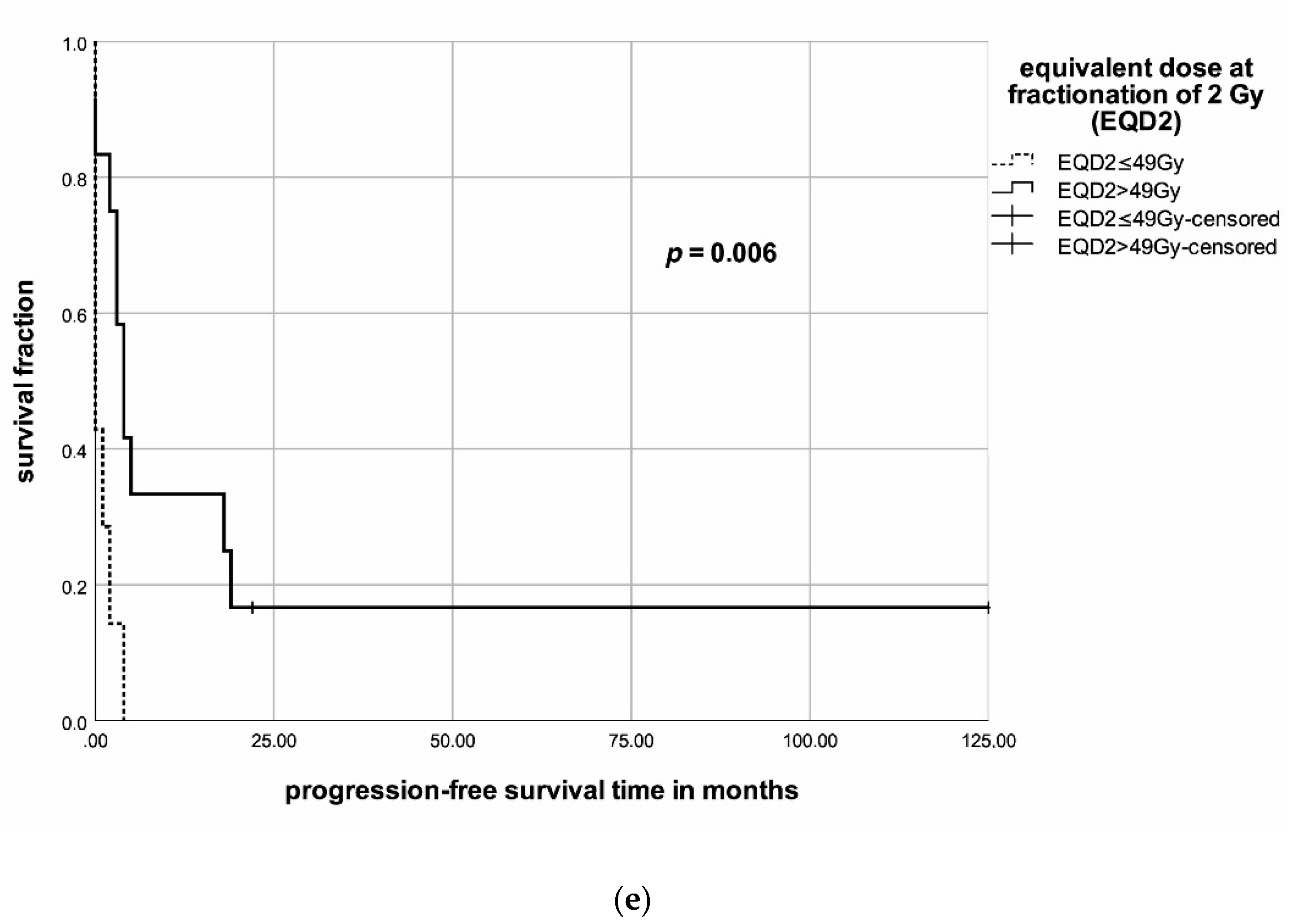
3.8. Patient- and Treatment-Related Factors of Prognosis in the Single-Center Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Smallridge, R.C.; Ain, K.B.; Asa, S.L.; Bible, K.C.; Brierley, J.D.; Burman, K.D.; Kebebew, E.; Lee, N.Y.; Nikiforov, Y.E.; Rosenthal, M.S.; et al. American Thyroid Association Guidelines for management of patients with anaplastic thyroid cancer. Thyroid 2012, 22, 1104–1139. [Google Scholar] [CrossRef] [PubMed]
- Salehian, B.; Liem, S.Y.; Mojazi Amiri, H.; Maghami, E. Clinical trials in management of anaplastic thyroid carcinoma; Progressions and set backs: A systematic review. Int. J. Endocrinol. Metab. 2019, 17. [Google Scholar] [CrossRef] [PubMed]
- Haymart, M.R.; Banerjee, M.; Yin, H.; Worden, F.; Griggs, J.J. Marginal treatment benefit in anaplastic thyroid cancer. Cancer 2013, 119, 3133–3139. [Google Scholar] [CrossRef] [PubMed]
- Sugitani, I.; Onoda, N.; Ito, K.; Suzuki, S. Management of anaplastic thyroid carcinoma: The fruits from the ATC Research Consortium of Japan. J. Nippon Med. Sch. 2018, 85, 18–27. [Google Scholar] [CrossRef]
- Pezzi, T.A.; Mohamed, A.S.R.; Sheu, T.; Blanchard, P.; Sandulache, V.C.; Lai, S.Y.; Cabanillas, M.E.; Williams, M.D.; Pezzi, C.M.; Lu, C.; et al. Radiation therapy dose is associated with improved survival for unresected anaplastic thyroid carcinoma: Outcomes from the National Cancer Data Base. Cancer 2017, 123, 1653–1661. [Google Scholar] [CrossRef]
- Liu, T.-R.; Xiao, Z.-W.; Xu, H.-N.; Long, Z.; Wei, F.-Q.; Zhuang, S.-M.; Sun, X.-M.; Xie, L.-E.; Mu, J.-S.; Yang, A.-K.; et al. Treatment and prognosis of anaplastic thyroid carcinoma: A clinical study of 50 cases. PLoS ONE 2016, 11, e164840. [Google Scholar] [CrossRef]
- Keutgen, X.M.; Sadowski, S.M.; Kebebew, E. Management of anaplastic thyroid cancer. Gland Surg. 2015, 4, 44–51. [Google Scholar] [CrossRef]
- Simões-Pereira, J.; Capitão, R.; Limbert, E.; Leite, V. Anaplastic thyroid cancer: Clinical picture of the last two decades at a single oncology referral centre and novel therapeutic options. Cancers 2019, 11, 1188. [Google Scholar] [CrossRef]
- Rades, D.; Janssen, S.; Käsmann, L.; Bolm, L.; Schild, S.E. Outcomes after irradiation of epidural spinal cord compression due to metastatic thyroid cancer. Anticancer Res. 2016, 36, 2035–2039. [Google Scholar] [PubMed]
- Onoda, N.; Sugitani, I.; Ito, K.; Suzuki, A.; Higashiyama, T.; Fukumori, T.; Suganuma, N.; Masudo, K.; Nakayama, H.; Uno, A.; et al. Evaluation of the 8th edition TNM classification for anaplastic thyroid carcinoma. Cancers 2020, 12, 552. [Google Scholar] [CrossRef]
- Filetti, S.; Durante, C.; Hartl, D.; Leboulleux, S.; Locati, L.D.; Newbold, K.; Papotti, M.G.; Berruti, A. Thyroid cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 1856–1883. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.; Li, Q.; Hu, Z.; He, J.; Li, C.; Li, G.; Tao, X.; Yang, A. Treatment and prognosis of anaplastic thyroid carcinoma: Experience from a single institution in China. PLoS ONE 2013, 8, e80011. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-H.; Ahn, H.K.; Seok, J.Y.; Lee, K.-C.; Chun, Y.S.; Chung, Y.S.; Lee, Y.D. Optimal combination of treatment modality to increase survival in patients with anaplastic thyroid carcinoma. Medicine 2018, 97. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.N.; Zafereo, M.; Dadu, R.; Busaidy, N.L.; Hess, K.; Cote, G.J.; Williams, M.D.; William, W.N.; Sandulache, V.; Gross, N.; et al. Patterns of treatment failure in anaplastic thyroid carcinoma. Thyroid 2017, 27, 672–681. [Google Scholar] [CrossRef]
- Corrigan, K.L.; Williamson, H.; Elliott Range, D.; Niedzwiecki, D.; Brizel, D.M.; Mowery, Y.M. Treatment outcomes in anaplastic thyroid cancer. J. Thyroid Res. 2019, 2019. [Google Scholar] [CrossRef]
- Wendler, J.; Kroiss, M.; Gast, K.; Kreissl, M.C.; Allelein, S.; Lichtenauer, U.; Blaser, R.; Spitzweg, C.; Fassnacht, M.; Schott, M.; et al. Clinical presentation, treatment and outcome of anaplastic thyroid carcinoma: Results of a multicenter study in Germany. Eur. J. Endocrinol. 2016, 175, 521–529. [Google Scholar] [CrossRef]
- Zivaljevic, V.; Tausanovic, K.; Paunovic, I.; Diklic, A.; Kalezic, N.; Zoric, G.; Sabljak, V.; Vekic, B.; Zivic, R.; Marinkovic, J.; et al. Age as a prognostic factor in anaplastic thyroid cancer. Int. J. Endocrinol. 2014, 2014, 1–5. [Google Scholar] [CrossRef]
- Kebebew, E.; Greenspan, F.S.; Clark, O.H.; Woeber, K.A.; McMillan, A. Anaplastic thyroid carcinoma. Cancer 2005, 103, 1330–1335. [Google Scholar] [CrossRef]
- Scharf, A.-C.; Gronewold, J.; Dahlmann, C.; Schlitzer, J.; Kribben, A.; Gerken, G.; Frohnhofen, H.; Dodel, R.; Hermann, D.M. Clinical and functional patient characteristics predict medical needs in older patients at risk of functional decline. BMC Geriatr. 2020, 20, 1–11. [Google Scholar] [CrossRef]
- Kaesmann, L.; Janssen, S.; Rades, D. Karnofsky performance score, radiation dose and nodal status predict survival of elderly patients irradiated for limited-disease small-cell lung cancer. Anticancer Res. 2016, 36, 4177–4180. [Google Scholar] [PubMed]
- Oliinyk, D.; Augustin, T.; Koehler, V.F.; Rauch, J.; Belka, C.; Spitzweg, C.; Käsmann, L. Hypofractionated radiotherapy for anaplastic thyroid cancer: Systematic review and pooled analysis. Cancers 2020, 12, 2506. [Google Scholar] [CrossRef] [PubMed]
- Fan, D.; Ma, J.; Bell, A.C.; Groen, A.H.; Olsen, K.S.; Lok, B.H.; Leeman, J.E.; Anderson, E.; Riaz, N.; McBride, S. Outcomes of multimodal therapy in a large series of patients with anaplastic thyroid cancer. Cancer 2019, 126, 444–452. [Google Scholar] [CrossRef] [PubMed]
- Sugitani, I.; Kasai, N.; Fujimoto, Y.; Yanagisawa, A. Prognostic factors and therapeutic strategy for anaplastic carcinoma of the thyroid. World J. Surg. 2001, 25, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Pierie, J.-P.E.N.; Muzikansky, A.; Gaz, R.D.; Faquin, W.C.; Ott, M.J. The effect of surgery and radiotherapy on outcome of anaplastic thyroid carcinoma. Ann. Surg. Oncol. 2002, 9, 57–64. [Google Scholar] [CrossRef]
- Kihara, M.; Miyauchi, A.; Yamauchi, A.; Yokomise, H. Prognostic Factors of Anaplastic Thyroid Carcinoma. Surg. Today 2004, 34, 394–398. [Google Scholar] [CrossRef]
- Brignardello, E.; Gallo, M.; Baldi, I.; Palestini, N.; Piovesan, A.; Grossi, E.; Ciccone, G.; Boccuzzi, G. Anaplastic thyroid carcinoma: Clinical outcome of 30 consecutive patients referred to a single institution in the past 5 years. Eur. J. Endocrinol. 2007, 156, 425–430. [Google Scholar] [CrossRef]
- Kim, T.Y.; Kim, K.W.; Jung, T.S.; Kim, J.M.; Kim, S.W.; Chung, K.; Kim, E.Y.; Gong, G.; Oh, Y.L.; Cho, S.Y. Prognostic factors for Korean patients with anaplastic thyroid carcinoma. Head Neck 2007, 29, 765–772. [Google Scholar] [CrossRef]
- Chen, J.; Tward, J.D.; Shrieve, D.C.; Hitchcock, Y.J. Surgery and radiotherapy improves survival in patients with anaplastic thyroid carcinoma: Analysis of the surveillance, epidemiology, and end results 1983–2002. Am. J. Clin. Oncol. 2008, 31, 460–464. [Google Scholar] [CrossRef]
- Yau, T.; Lo, C.Y.; Epstein, R.J.; Lam, A.K.Y.; Wan, K.Y.; Lang, B.H. Treatment outcomes in anaplastic thyroid carcinoma: Survival improvement in young patients with localized disease treated by combination of surgery and radiotherapy. Ann. Surg. Oncol. 2008, 15, 2500. [Google Scholar] [CrossRef]
- Bhatia, A.; Rao, A.; Ang, K.-K.; Garden, A.S.; Morrison, W.H.; Rosenthal, D.I.; Evans, D.B.; Clayman, G.; Sherman, S.I.; Schwartz, D.L. Anaplastic thyroid cancer: Clinical outcomes with conformal radiotherapy. Head Neck 2010, 32, 829–836. [Google Scholar] [CrossRef]
- Roche, B.; Larroumets, G.; Dejax, C.; Kwiatkowsi, F.; Desbiez, F.; Thieblot, P.; Tauveron, I. Epidemiology, clinical presentation, treatment and prognosis of a regional series of 26 anaplastic thyroid carcinomas (ATC). Comparison with the literature. Ann. Endocrinol. 2010, 71, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Akaishi, J.; Sugino, K.; Kitagawa, W.; Nagahama, M.; Kameyama, K.; Shimizu, K.; Ito, K.; Ito, K. Prognostic factors and treatment outcomes of 100 cases of anaplastic thyroid carcinoma. Thyroid Off. J. Am. Thyroid Assoc. 2011, 21, 1183–1189. [Google Scholar] [CrossRef] [PubMed]
- Derbel, O.; Limem, S.; Ségura-Ferlay, C.; Lifante, J.-C.; Carrie, C.; Peix, J.-L.; Borson-Chazot, F.; Bournaud, C.; Droz, J.-P.; de la Fouchardière, C. Results of combined treatment of anaplastic thyroid carcinoma (ATC). BMC Cancer 2011, 11, 469. [Google Scholar] [CrossRef] [PubMed]
- Sherman, E.J.; Lim, S.H.; Ho, A.L.; Ghossein, R.A.; Fury, M.G.; Shaha, A.R.; Rivera, M.; Lin, O.; Wolden, S.; Lee, N.Y.; et al. Concurrent doxorubicin and radiotherapy for anaplastic thyroid cancer: A critical re-evaluation including uniform pathologic review. Radiother. Oncol. 2011, 101, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Tashima, L.; Mitzner, R.; Durvesh, S.; Goldenberg, D. Dyspnea as a prognostic factor in anaplastic thyroid carcinoma. Eur. Arch. Otorhinolaryngol. 2012, 269, 1251–1255. [Google Scholar] [CrossRef] [PubMed]
- Sugitani, I.; Miyauchi, A.; Sugino, K.; Okamoto, T.; Yoshida, A.; Suzuki, S. Prognostic factors and treatment outcomes for anaplastic thyroid carcinoma: ATC research consortium of Japan cohort study of 677 patients. World J. Surg. 2012, 36, 1247–1254. [Google Scholar] [CrossRef]
- Dumke, A.-K.; Pelz, T.; Vordermark, D. Long-term results of radiotherapy in anaplastic thyroid cancer. Radiat. Oncol. Lond. Engl. 2014, 9, 90. [Google Scholar] [CrossRef]
- Mohebati, A.; DiLorenzo, M.; Palmer, F.; Patel, S.G.; Pfister, D.; Lee, N.; Tuttle, R.M.; Shaha, A.R.; Shah, J.P.; Ganly, I. Anaplastic Thyroid Carcinoma: A 25-year Single-Institution Experience. Ann. Surg. Oncol. 2014, 21, 1665–1670. [Google Scholar] [CrossRef]
- Polistena, A.; Monacelli, M.; Lucchini, R.; Triola, R.; Conti, C.; Avenia, S.; Rondelli, F.; Bugiantella, W.; Barillaro, I.; Sanguinetti, A.; et al. The role of surgery in the treatment of thyroid anaplastic carcinoma in the elderly. Int. J. Surg. 2014, 12, S170–S176. [Google Scholar] [CrossRef][Green Version]
- Lo, T.E.; Jimeno, C.A.; Paz-Pacheco, E. Anaplastic thyroid cancer: Experience of the Philippine general hospital. Endocrinol. Metab. 2015, 30, 195–200. [Google Scholar] [CrossRef]
- Paunovic, I.; Sipetic, S.; Zoric, G.; Diklic, A.; Savic, D.; Marinkovic, J.; Zivaljevic, V. Survival and prognostic factors of anaplastic thyroid carcinoma. Acta Chir. Belg. 2015, 115, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Baek, S.-K.; Lee, M.-C.; Hah, J.H.; Ahn, S.-H.; Son, Y.-I.; Rho, Y.-S.; Chung, P.-S.; Lee, Y.-S.; Koo, B.S.; Jung, K.-Y.; et al. Role of surgery in the management of anaplastic thyroid carcinoma: Korean nationwide multicenter study of 329 patients with anaplastic thyroid carcinoma, 2000 to 2012. Head Neck 2017, 39, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Glaser, S.M.; Mandish, S.F.; Gill, B.S.; Balasubramani, G.K.; Clump, D.A.; Beriwal, S. Anaplastic thyroid cancer: Prognostic factors, patterns of care, and overall survival. Head Neck 2016, 38, E2083–E2090. [Google Scholar] [CrossRef] [PubMed]
- Käsmann, L.; Bolm, L.; Janssen, S.; Rades, D. Prognostic factors for survival in patients treated with multimodal therapy for anaplastic thyroid cancer. Anticancer Res. 2016, 36, 4697–4700. [Google Scholar] [CrossRef][Green Version]
- Lennon, P.; Deady, S.; Healy, M.L.; Toner, M.; Kinsella, J.; Timon, C.I.; O’Neill, J.P. Anaplastic thyroid carcinoma: Failure of conventional therapy but hope of targeted therapy. Head Neck 2016, 38, E1122–E1129. [Google Scholar] [CrossRef]
- Hvilsom, G.B.; Londero, S.C.; Hahn, C.H.; Schytte, S.; Pedersen, H.B.; Christiansen, P.; Kiss, K.; Larsen, S.R.; Jespersen, M.L.; Lelkaitis, G.; et al. Anaplastic thyroid carcinoma in Denmark 1996–2012: A national prospective study of 219 patients. Cancer Epidemiol. 2018, 53, 65–71. [Google Scholar] [CrossRef]
- Jacobsen, A.-B.; Grøholt, K.K.; Lorntzsen, B.; Osnes, T.A.; Falk, R.S.; Sigstad, E. Anaplastic thyroid cancer and hyperfractionated accelerated radiotherapy (HART) with and without surgery. Eur. Arch. Otorhinolaryngol. 2017, 274, 4203–4209. [Google Scholar] [CrossRef]
- Park, J.W.; Choi, S.H.; Yoon, H.I.; Lee, J.; Kim, T.H.; Kim, J.W.; Lee, I.J. Treatment outcomes of radiotherapy for anaplastic thyroid cancer. Radiat. Oncol. J. 2018, 36, 103–113. [Google Scholar] [CrossRef]
- Takahashi, N.; Matsushita, H.; Umezawa, R.; Yamamoto, T.; Ishikawa, Y.; Katagiri, Y.; Tasaka, S.; Takeda, K.; Fukui, K.; Kadoya, N.; et al. Hypofractionated radiotherapy for anaplastic thyroid carcinoma: 15 years of experience in a single institution. Eur. Thyroid J. 2019, 8, 24–30. [Google Scholar] [CrossRef]
- Huang, N.; Shi, X.; Lei, B.; Wei, W.; Lu, Z.; Yu, P.; Wang, Y.; Ji, Q.; Wang, Y. An update of the appropriate treatment strategies in anaplastic thyroid cancer: A population-based study of 735 patients. Int. J. Endocrinol. 2019, 2019, 1–7. [Google Scholar] [CrossRef]
- Li, M.; Gu, S.; Mao, R.; Ning, Y.; Trivedi, N.; Siddiqui, A.; Li, P.; Huo, L. County median family income is an independent prognostic factor for stage IV anaplastic thyroid cancer. Anticancer Res. 2019, 39, 949–956. [Google Scholar] [CrossRef] [PubMed]
- de Ridder, M.; van Dijkum, E.N.; Engelsman, A.; Kapiteijn, E.; Klümpen, H.-J.; Rasch, C.R.N. Anaplastic thyroid carcinoma: A nationwide cohort study on incidence, treatment and survival in the Netherlands over 3 decades. Eur. J. Endocrinol. 2020, 183, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Gui, W.; Zhu, W.; Lu, W.; Shang, C.; Zheng, F.; Lin, X.; Li, H. Development and validation of a prognostic nomogram to predict overall survival and cancer-specific survival for patients with anaplastic thyroid carcinoma. PeerJ 2020, 8, e9173. [Google Scholar] [CrossRef]
- Lin, B.; Ma, H.; Ma, M.; Zhang, Z.; Sun, Z.; Hsieh, I.; Okenwa, O.; Guan, H.; Li, J.; Lv, W. The incidence and survival analysis for anaplastic thyroid cancer: A SEER database analysis. Am. J. Transl. Res. 2019, 11, 5888–5896. [Google Scholar] [PubMed]
- Saeed, N.A.; Kelly, J.R.; Deshpande, H.A.; Bhatia, A.K.; Burtness, B.A.; Judson, B.L.; Mehra, S.; Edwards, H.A.; Yarbrough, W.G.; Peter, P.R.; et al. Adjuvant external beam radiotherapy for surgically resected, nonmetastatic anaplastic thyroid cancer. Head Neck 2020, 42, 1031–1044. [Google Scholar] [CrossRef] [PubMed]
- Wächter, S.; Wunderlich, A.; Roth, S.; Mintziras, I.; Maurer, E.; Hoffmann, S.; Verburg, F.A.; Fellinger, S.A.; Holzer, K.; Bartsch, D.K.; et al. Individualised multimodal treatment strategies for anaplastic and poorly differentiated thyroid cancer. J. Clin. Med. 2018, 7, 115. [Google Scholar] [CrossRef]
- Lim, S.M.; Shin, S.-J.; Chung, W.Y.; Park, C.S.; Nam, K.-H.; Kang, S.-W.; Keum, K.C.; Kim, J.H.; Cho, J.Y.; Hong, Y.K.; et al. Treatment outcome of patients with anaplastic thyroid cancer: A single center experience. Yonsei Med. J. 2012, 53, 352–357. [Google Scholar] [CrossRef]
- Stavas, M.J.; Shinohara, E.T.; Attia, A.; Ning, M.S.; Friedman, J.M.; Cmelak, A.J. short course high dose radiotherapy in the treatment of anaplastic thyroid carcinoma. J. Thyroid Res. 2014, 2014. [Google Scholar] [CrossRef]
- Busnardo, B.; Daniele, O.; Pelizzo, M.R.; Mazzarotto, R.; Nacamulli, D.; DeVido, D.; Mian, C.; Girelli, M.E. A multimodality therapeutic approach in anaplastic thyroid carcinoma: Study on 39 patients. J. Endocrinol. Investig. 2000, 23, 755–761. [Google Scholar] [CrossRef]
- So, K.; Smith, R.E.; Davis, S.R. Radiotherapy in anaplastic thyroid carcinoma: An Australian experience. J. Med. Imaging Radiat. Oncol. 2017, 61, 279–287. [Google Scholar] [CrossRef]
- Aslan, Z.A.T.; Granados-García, M.; Luna-Ortiz, K.; Guerrero-Huerta, F.J.; Gómez-Pedraza, A.; Ñamendys-Silva, S.A.; Meneses-García, A.; Ordoñez-Mosquera, J.M. Anaplastic thyroid cancer: Multimodal treatment results. Ecancermedicalscience 2014, 8. [Google Scholar] [CrossRef]
- Crevoisier, R.D.; Baudin, E.; Bachelot, A.; Leboulleux, S.; Travagli, J.-P.; Caillou, B.; Schlumberger, M. Combined treatment of anaplastic thyroid carcinoma with surgery, chemotherapy, and hyperfractionated accelerated external radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2004, 60, 1137–1143. [Google Scholar] [CrossRef] [PubMed]
- Rades, D.; Manig, L.; Janssen, S.; Schild, S.E. Factors impacting the overall survival of patients irradiated for invasive carcinoma of the urinary bladder. In Vivo 2017, 31, 741–744. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rades, D.; Bolm, L.; Kaesmann, L.; Bartscht, T. Karnofsky performance score is predictive of survival after palliative irradiation of metastatic bile duct cancer. Anticancer Res. 2017, 37, 949–951. [Google Scholar] [CrossRef]
- Edwards, B.J.; Zhang, X.; Sun, M.; Song, J.; Khalil, P.; Karuturi, M.S.; Pang, L.; Geng, Y.; Dinney, C.P.; Valero, V. Overall survival in older patients with cancer. BMJ Support. Palliat. Care 2020, 10, 25–35. [Google Scholar] [CrossRef]
- Brignardello, E.; Palestini, N.; Felicetti, F.; Castiglione, A.; Piovesan, A.; Gallo, M.; Freddi, M.; Ricardi, U.; Gasparri, G.; Ciccone, G.; et al. Early surgery and survival of patients with anaplastic thyroid carcinoma: Analysis of a case series referred to a single institution between 1999 and 2012. Thyroid 2014, 24, 1600–1606. [Google Scholar] [CrossRef]
- He, X.; Li, D.; Hu, C.; Wang, Z.; Ying, H.; Wu, Y. Outcome after intensity modulated radiotherapy for anaplastic thyroid carcinoma. BMC Cancer 2014, 14, 235. [Google Scholar] [CrossRef][Green Version]
- Tiedje, V.; Stuschke, M.; Weber, F.; Dralle, H.; Moss, L.; Führer, D. Anaplastic thyroid carcinoma: Review of treatment protocols. Endocr. Relat. Cancer 2018, 25, R153–R161. [Google Scholar] [CrossRef]
- Haddad, R.I.; Kandeel, F.; Scheri, R.P. NCCN Guidelines Index Table of Contents Discussion. 2019, p. 137. Available online: https://www.nccn.org/professionals/physician_gls/pdf/thyroid.pdf (accessed on 28 March 2020).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Number of Patients (N) | Treatment | Age Cut-Off (Years) | Results |
|---|---|---|---|---|
| Sugitani et al. (2001) [23] | 47 | Multimodal—20% Other—80% | 40–49 (7%) 50–59 (16%) 60–69 (34%) 70–79 (35%) 80–89 (7%) | Age was not a significant prognostic factor in the uni- or multivariate analysis |
| Pierie et al. (2002) [24] | 67 | Surgery—67% EBRT—84% ChT—31% | Cut-off: 70 ≤70 (45%) >70 (55%) | An age of ≤70 years was an independent predictor for beneficial OS (HR = 0.47, p < 0.023) |
| Kihara et al. (2004) [25] | 19 | Surgery—53% RT—68% ChT—63% | Cut-off: 70 40–49 (5%) 50–59 (0%) 60–69 (26%) 70–79 (32%) 80–89 (37%) | Age was not a significant prognostic factor in the uni- or multivariate analysis |
| Kebebew et al. (2005) [18] | 516 | Surgery—49% EBRT—63.2% ChT—not reported | Cut-off: 60 Mean: 71.3 (15–95) | An age of <60 years was an independent predictor for beneficial survival (HR = 0.482, 95% CI = 0.268–0.867, p < 0.05) |
| Brignardello et al. (2007) [26] | 27 | Surgery + adjuvant RT/ChT—56% Surgery + neoadjuvant RT/ChT—19% ChT alone—19% | Median: 70 (46–92) | Age was not a significant prognostic factor in the uni- or multivariate analysis |
| Kim et al. (2007) [27] | 121 | Unilateral palliative surgery—12% postoperative: 42.9% only RT, 7.1% only ChT and 14.3% both Bilateral curative surgery—59% postoperative: 50.7% only RT, 8.5% only ChT and 12.7% both RT alone—10.7% ChT alone—1.7% ChT/RT—4.1% | Cut-off: 60 <60 (33%) ≥60 (67%) | An age of <60 years was an independent predictor for lower disease-specific mortality(HR = 0.47, 95% CI = 0.30–0.74, p = 0.001) |
| Chen et al. (2008) [28] | 261 | Surgery only—26.1% EBRT alone—14.2% Surgery + EBRT—49.4% | <45 (5.7%) 45–54 (9.2%) 55–64 (19.9%) 65–74 (29.1%) 75–84 (23.4%) ≥85 (12.6%) | Younger age was an independent predictor for improved overall survival (HR = 1.02, 95% CI = 1.00–1.03, p = 0.007) |
| Yau et al. (2008) [29] | 50 | Surgery—68% EBRT—46% ChT—36% | Cut-off: 65 ≤65 (28%) >65 (72%) | In the univariate analysis, an age of ≤65 years was significantly associated with improved survival (p = 0.025) No significance in the multivariate analysis |
| Bhatia et al. (2009) [30] | 53 | Surgery—58.5% RT—100% CRT—73.6% Sequential ChT—16.9% | Median: 66.1 (27–88) | Age was not a significant prognostic factor in the uni- or multivariate analysis |
| Roche et al. (2010) [31] | 26 | Surgery—84.6% RT—53.8% ChT—19.2% | Mean: 75 (52.3–90.8) | Age >75 years was an independent predictor for poor prognosis (p < 0.05) |
| Akaishi et al. (2011) [32] | 100 | Surgery—70% RT—78% ChT—28% | Cut-off: 70 <70 (52%) ≥70 (48%) | Age ≥70 years was a significant risk factor for poorer survival in the multivariate analysis (RR = 1.03, 95% CI = 1.01–1.05, p = 0.014) |
| Derbel et al. (2011) [33] | 44 | Surgery alone—4.5% Surgery + CT—7% Surgery + RT + CT—79.5% RT alone—4.5% Surgery + RT—4.5% | Cut-off: 65 Median 65 (44–80) | An age of >65 years was associated with poorer outcome in the univariate analysis (HR = 2.36, 95% CI = 1.15–4.84, no p-value reported) |
| Sherman et al. (2011) [34] | 37 | Surgery + CRT—51% CRT—100% | Cut-off: 70 <70 (73%) ≥70 (27%) | An age of <70 years was an independent predictor for beneficial OS (HR = 0.32, 95% CI = 0.13–0.78, p = 0.013) |
| Tashima et al. (2011) [35] | 33 | Surgery—58% RT—52% ChT—39% RT + ChT—36% | Cut-off: 60 Median: 68 (26–93) | In the univariate analysis, an age of >60 years was associated with decreased survival (p = 0.04). No significance in the multivariate analysis |
| Sugitani et al. (2012) [36] | 677 | Surgery—45% EBRT—59% ChT—47% | Cut-off: 70 <70 (48%) ≥70 (52%) | An age of <70 years was an independent predictor for beneficial survival (HR = 1.28, 95% CI = 1.04–1.58, p = 0.020) |
| Haymart et al. (2013) [3] | 2742 | Surgery—50.2% RT—58.2% ChT—38.8% | ≤44 (3.0%) 45–64 (27.5%) 65–74 (27.5%) 75–84 (30.4%) ≥85 (11.7%) | An age of ≥85 years was associated with greater mortality in the adjusted Cox regression model (HR = 3.43, 95% CI = 2.34–5.03, p < 0.05) |
| Dumke et al. (2014) [37] | 40 | Surgery—80% RT—98% ChT—15% | Median: 67 (38–84) | Age was not a significant prognostic factor in the uni- or multivariate analysis |
| Mohebati et al. (2014) [38] | 83 | Surgery alone—12% RT alone—4% ChT/RT—5% Surgery + RT + ChT—46% | Cut-off: 60 ≤60 (35%) >60 (65%) | 1-year DSS (p = 0.012) in the univariate analysis ≤60 (52%) >60 (24%) No significance in the multivariate analysis |
| Polistena et al. (2014) [39] | 79 | Surgery—57% RT—59% ChT—100% | Cut-off: 75 <75 (53%) >75 (47%) | Patients <75 years and with tumors <5 cm in extent had the most favorable prognosis among subgroups in the univariate analysis (p < 0.05) |
| Sun et al. (2014) [12] | 42 | Surgery alone—29% EBRT alone—12% ChT alone—5% Surgery + RT—26% Surgery + RT/ChT—14% Surgery + ChT—10% | Cut-off: 55 <55 (33%) ≥55 (67%) | In the univariate analysis, an age of ≤55 years was significantly associated with improved 1- and 3-year overall survival rates (p = 0.012) No significance in the multivariate analysis |
| Ziveljevic et al. (2014) [17] | 150 | Surgery—57% Pre-OP RT—2.4% Post-OP RT—78.7% ChT—79% | ≤50 (7.3%) 51–70 (73.3%) ≥70 (19.3%) | Younger age was an independent predictor of favorable survival (OR = 0.68, 95% CI = 0.49–0.95, p = 0.023) |
| Lo et al. (2015) [40] | 15 | Surgery—47% RT—20% ChT—0% | Median: 63 (36–73) | Age was not a significant prognostic factor in the uni- or multivariate analysis |
| Paunovic et al. (2015) [41] | 150 | Surgery—56.7% Pre-OP RT—2.4% Post-OP RT—78.8% ChT—2.4% | <40 (1.3%) 41–50 (6.1%) 51–60 (19.3%) 61–70 (54.0%) >70 (19.3%) | An age of <50 years is an independent predictor associated with overall survival (RR = 0.68, 95% CI = 0.49–0.95, p = 0.023) |
| Baek et al. (2016) [42] | 329 | RT/cCRT—15.2% Curative resection—28.6% Curative resection and adjuvant RT/cCRT—25.5% Curative resection and adjuvant ChT—3.0% ChT alone—3.0% | Cut-off: 70 <70 (51.7%) ≥70 (48.3%) | An age of ≥70 years was an independent predictor for poorer disease-specific survival (HR = 1.493, 95% CI = 1.134–1.965, p < 0.01) |
| Glaser et al. (2016) [43] | 3552 | Surgery—49.5% RT—58.7% ChT—41.6% | Cut-off: 65 <65 (31.6%) ≥65 (68.4%) | An age of <65 years was an independent predictor for improved overall survival (HR = 1.42, 95% CI = 1.26–1.60, p < 0.0005) |
| Käsmann et al. (2016) [44] | 9 | Surgery—78% RT—78% ChT—78% | Cut-off: 64 ≤64 (56%) >64 (44%) | Age was not a significant prognostic factor in the uni- or multivariate analysis |
| Lee et al. (2016) [13] | 98 (ATC) | Surgery-based—58.2% EBRT-based—17.3% ChT—7.1% | Mean: 63.4 ± 13.4 | Age at diagnosis in years achieved significance in the multivariate analysis (OR = 1.022, 95% CI = 0.01–1.10, p = 0.029) in a group, where resectability was adjusted with age, tumor size, WBC count and N status |
| Lennon et al. (2016) [45] | 64 | Surgery alone—17.2% RT alone—26.6% ChT alone—4.7% Surgery + RT—10.9% RT + ChT—9.4% Surgery + RT + ChT—12.5% | Cut-off: 70 Median: 72 (47–93) | In the univariate analysis, an age of >70 years was associated with improved overall survival (p = 0.041) No significance in the multivariate analysis |
| Liu et al. (2016) [6] | 50 | Total or extensive thyroidectomy—76% Palliative resection of cervical lymph nodes—6% RT—32% ChT—16% | Cut-off: 60 ≤60 (52%) >60 (48%) | Age was not a significant prognostic factor in the uni- or multivariate analysis |
| Pezzi et al. (2016) [5] | 1288 | Surgery (any neck, but only R2)—11.6% RT—47.7% ChT—53.8% | Cut-off: 65 Average: 70.4 | An age of <65 years was an independent predictor for beneficial patient survival (HR = 1.317, 95% CI = 1.137–1.526, p < 0.001) |
| Wendler et al. (2016) [16] | 100 | Surgery—83% EBRT—81% ChT—56% | Cut-off: 70 <70 (46%) ≥70 (54%) | An age of <70 years was an independent predictor for beneficial survival (HR = 1.048, 95% CI = 1.015–1.082, p = 0.004) |
| Hvilsom et al. (2017) [46] | 219 | Thyroid surgery (R0—2)—50.7% Lymph node surgery—72% ChT/RT—Not reported | Median: 74 (30–94) | An age of ≤73.6 years was an independent predictor for improved overall survival (HR = 1.4, 95% CI = 1.0−2.0) |
| Jacobsen et al. (2017) [47] | 31 | Surgery—42% RT—100% ChT—74% | Median: 69 (26–87) | In the univariate analysis, age at diagnosis in years achieved significance (HR = 1.02, 95% CI = 0.98−1.07) No significance in the multivariate analysis |
| Park et al. (2018) [48] | 41 | Surgery + RT + ChT—39% Surgery + RT—12.2% RT + ChT—36.6% RT alone—12.2% | Cut-off: 65 <65 (31.7%) ≥65 (68.3%) | Age was not associated with better/poorer outcome in the univariate analysis (HR = 1.44, 95% CI = 0.69–3.01, p = 0.328) |
| Takahashi et al. (2018) [49] | 33 | Surgery—39% ChT—52% CRT—45% | Median 68 (41–87) | Age (≥ median vs. < median) was not associated with better/poorer outcome in the univariate analysis (HR= 1.22, 95% CI = 0.57–2.60, p = 0.605) |
| Corrigan et al. (2019) [15] | 28 | Surgery—71.4% EBRT—75% ChT—50% | Not reported | Younger age is an independent predictor for better overall survival (HR = 1.079; 95% CI = 1.022−1.139; p = 0.006) |
| Fan et al. (2019) [22] | 104 | ChT/RT—95.2% Surgery + RT + ChT— 51% | Cut-off: 70 Median: 63.5 (28–87) | In the univariate analysis, the age of <70 years was significantly associated with improved overall survival (p = < 0.001) No significance in the multivariate analysis |
| Huang et al. (2019) [50] | 735 | Surgery—26% RT—36% ChT—31% No treatment—22% | Cut-off: 70 Median: 70 IQR: 60–80 | Age at diagnosis in years achieved significance in the multivariate analysis (HR = 1.022, 95% CI = 1.010–1.034, p < 0.001) No difference in favor for the subgroups ≤/>70 years in terms of total thyroidectomy |
| Li et al. (2019) [51] | 1048 | Primary surgery—45% EBRT—55% ChT—42% | Cut-off: 65 <65 (33%) ≥65 (67%) | An age of ≥65 years was an independent predictor for overall survival (HR = 1.34, 95% CI = 1.16–1.55, p < 0.001) |
| De Ridder et al. (2020) [52] | 812 | Surgery—12% Surgery + RT—15% Surgery + cCRT—2% Surgery + RT + ChT—3% Surgery + ChT—1% RT—28% cCRT—1% RT + ChT—3% ChT—1% | Median: 73 (29–99) | Age at diagnosis was an independent prognostic factor for poorer outcome (HR = 1.014, 95% CI = 1.006–1.020, p < 0.001) |
| Gui et al. (2020) [53] | 1404 | Surgery—44% EBRT—59% ChT—not reported | Cut-off: 65 <65 (34%) ≥65 (66%) | An age of ≥65 years was an independent predictor for worse overall survival (HR = 1.525, 95% CI = 1.326–1.752, p < 0.001) |
| Lin et al. (2020) [54] | 1567/717 | Surgery—566/1567 (36%) Not reported for RT/ChT | Median: 71 (23–100) | Younger age is an independent predictor for overall survival (HR = 1.02, 95% CI = 1.01–1.02, p < 0.001) |
| Saeed et al. (2020) [55] | 496 | Surgery—100% Adjuvant EBRT—76% Adjuvant Chemotherapy—59% Adjuvant CRT—56.4% | Cut-off: 65 <65 (42%) ≥65 (58%) | In the univariate analysis, an age of ≥65 years was a significant prognostic factor for overall survival (p = 0.04) No significance in the multivariate analysis |
| Parameter | Value (%) |
|---|---|
| Total | 186 (100) |
| Age, years (range) | 68 (35–92) |
| Gender | |
| Male | 54 (39) |
| Female | 60 (44) |
| Unknown | 24 (17) |
| UICC stage | |
| IVA/B | 113 (61) |
| IVC | 51 (27) |
| Unknown | 22 (12) |
| Surgery | |
| No | 91 (49) |
| Yes | 95 (51) |
| Radiotherapy | |
| No | 34 (18) |
| Yes | 152 (82) |
| Sequential or concurrent chemotherapy | |
| No | 72 (39) |
| Yes | 114 (61) |
| Multimodal treatment | |
| No | 112 (60) |
| Yes | 74 (40) |
| Parameter | Entire PSM Cohort, | Subgroup with | Subgroup with | p-Value |
|---|---|---|---|---|
| N (%) | Patients Aged < 65 Years, N (%) | Patients Aged ≥ 65 Years, N (%) | ||
| Total | 138 (100) | 69 (50) | 69 (50) | |
| Age, years (range) | 65 (35–92) | 56 (35–64) | 74 (65–92) | <0.001 |
| Gender | ||||
| Male | 54 (39) | 33 (48) | 21 (30) | |
| Female | 60 (44) | 22 (32) | 38 (55) | 0.009 |
| Unknown | 24 (17) | 14 (20) | 10 (15) | |
| UICC stage | ||||
| IVA/B | 92 (67) | 46 (67) | 46 (67) | 0.999 |
| IVC | 46 (33) | 23 (33) | 23 (33) | |
| Surgery | ||||
| No | 59 (43) | 27 (39) | 32 (46) | 0.391 |
| Yes | 79 (57) | 42 (61) | 37 (54) | |
| Radiotherapy | ||||
| No | 14 (10) | 8 (12) | 6 (9) | 0.574 |
| Yes | 124 (90) | 61 (88) | 63 (91) | |
| Sequential or concurrent chemotherapy | ||||
| No | 54 (39) | 18 (26) | 36 (52) | 0.002 |
| Yes | 84 (61) | 51 (74) | 33 (48) |
| Stage | Eighth Edition of UICC TNM |
|---|---|
| IVA | T1–3a, N0 and M0 T1: Tumor ≤ 2 cm in the greatest dimension limited to the thyroid T2: Tumor > 2 cm but ≤4 cm in the greatest dimension limited to the thyroid T3a: Tumor > 4 cm limited to the thyroid |
| IVB | T1–3a, N1 and M0 or T3b–T4b, any N and M0 T3b: Gross extrathyroidal extension invading only strap muscles (sternohyoid, sternothyroid, thyrohyoid and omohyoid muscles) from a tumor of any size T4a: Gross extrathyroidal extension invading subcutaneous soft tissues, larynx, trachea, esophagus or recurrent laryngeal nerve from a tumor of any size T4b: Gross extrathyroidal extension invading prevertebral fascia or encasing a carotid artery or mediastinal vessels from a tumor of any size |
| IVC | Any T, any N and M1 |
| Parameter | n |
|---|---|
| Age, years | |
| <74 | 11 (42%) |
| ≥74 | 15 (58%) |
| Gender | |
| Male | 13 (50%) |
| Female | 13 (50%) |
| KPS, % | |
| ≤70 | 12 (46%) |
| >70 | 14 (54%) |
| T stage | |
| 2–3 | 2 (8%) |
| 4 | 24 (92%) |
| N stage | |
| 0 | 10 (39%) |
| 1 | 16 (62%) |
| M stage | |
| 0 | 10 (39%) |
| 1 | 16 (62%) |
| Number of metastatic sites | |
| 1 | 7 (44%) |
| 2 | 7 (44%) |
| 3 | 1 (6%) |
| 4 | 1 (6%) |
| UICC stage | |
| IVA | 1 (4%) |
| IVB | 9 (35%) |
| IVC | 16 (62%) |
| Surgery | |
| No | 14 (54%) |
| Yes | 12 (46%) |
| Chemotherapy | |
| No | 13 (50%) |
| Yes | 13 (50%) |
| Treatment | |
| RT/CRT | 14 (54%) |
| S+CRT | 12 (46%) |
| Resection status | |
| R0 | 1 (8%) |
| R1 | 7 (58%) |
| R2 | 4 (33%) |
| EQD2 level | |
| ≤49 | 14 (54%) |
| >49 | 12 (46%) |
| RT technique | |
| 3D-CRT | 17 (65%) |
| IMRT | 9 (35%) |
| Univariate Analysis | Multivariate Analysis | |||||||
|---|---|---|---|---|---|---|---|---|
| Parameter | At 6 Months | At 12 Months | At 24 Months | p-Value | p-Value | Hazard Ratio | 95% CI Lower | 95% CI Upper |
| Age, years | - | - | - | - | ||||
| ≤74 | 55% | 36% | 12% | 0.15 | ||||
| >74 | 22% | 10% | 10% | |||||
| Gender | - | - | - | - | ||||
| Male | 23% | 23% | 12% | 0.45 | ||||
| Female | 46% | 19% | 9% | |||||
| KPS, % | ||||||||
| ≤70 | 0% | 0% | 0% | <0.001 | 0.357 | 0.422 | 0.068 | 2.64 |
| >70 | 64% | 40% | 20% | |||||
| N stage | - | - | - | - | ||||
| 0 | 50% | 40% | 27% | 0.028 | ||||
| 1 | 25% | 8% | 0% | |||||
| M stage | - | - | - | - | ||||
| 0 | 70% | 47% | 31% | 0.001 | ||||
| 1 | 13% | 6% | 0% | |||||
| UICC stage | ||||||||
| IVA | 100% | 100% | 100% | 0.004 | 0.618 | 1.449 | 0.337 | 6.223 |
| IVB | 67% | 40% | 27% | |||||
| IVC | 13% | 6% | 0% | |||||
| Surgery | - | - | - | - | ||||
| No | 7% | 0% | 0% | <0.001 | ||||
| Yes | 67% | 42% | 21% | |||||
| Chemotherapy | - | - | - | - | ||||
| No | 31% | 21% | 21% | 0.78 | ||||
| Yes | 39% | 23% | 0% | |||||
| Treatment | ||||||||
| RT/CRT | 7% | 0% | 0% | <0.001 | 0.524 | 0.519 | 0.069 | 3.911 |
| S+CRT | 67% | 42% | 21% | |||||
| EQD2 level | ||||||||
| ≤49 | 7% | 0% | 0% | <0.001 | 0.426 | 0.562 | 0.136 | 2.32 |
| >49 | 67% | 42% | 24% | |||||
| RT technique | - | - | - | - | ||||
| 3D-CRT | 29% | 12% | 6% | 0.18 | ||||
| IMRT | 44% | 44% | 22% | |||||
| Univariate Analysis | Multivariate Analysis | |||||||
|---|---|---|---|---|---|---|---|---|
| Parameter | At 3 Months | At 6 Months | At 12 Months | p-Value | p-Value | Hazard Ratio | 95% CI Lower | 95% CI Upper |
| Age, years | - | - | - | - | ||||
| ≤74 | 27% | 27% | 27% | 0.29 | ||||
| >74 | 27% | 7% | 7% | |||||
| Gender | - | - | - | - | ||||
| Male | 31% | 23% | 23% | 0.82 | ||||
| Female | 23% | 8% | 8% | |||||
| KPS, % | ||||||||
| ≤70 | 17% | 0% | 0% | 0.025 | 0.532 | 1.625 | 0.354 | 7.452 |
| >70 | 36% | 29% | 29% | |||||
| N stage | ||||||||
| 0 | 60% | 40% | 40% | <0.001 | 0.325 | 1.812 | 0.555 | 5.919 |
| 1 | 6% | 0% | 0% | |||||
| M stage | ||||||||
| 0 | 40% | 30% | 30% | 0.03 | 0.373 | 1.939 | 0.452 | 8.318 |
| 1 | 19% | 6% | 6% | |||||
| UICC stage | - | - | - | - | ||||
| IVA | 100% | 100% | 100% | 0.056 | ||||
| IVB | 33% | 22% | 22% | |||||
| IVC | 19% | 6% | 6% | |||||
| Surgery | - | - | - | - | ||||
| No | 7% | 0% | 0% | <0.001 | ||||
| Yes | 50% | 33% | 33% | |||||
| Chemotherapy | - | - | - | - | ||||
| No | 15% | 15% | 15% | 0.36 | ||||
| Yes | 39% | 15% | 15% | |||||
| Treatment | ||||||||
| RT/CRT | 7% | 0% | 0% | <0.001 | 0.352 | 0.405 | 0.06 | 2.718 |
| S+CRT | 50% | 33% | 33% | |||||
| EQD2 level | ||||||||
| ≤49 | 14% | 0% | 0% | 0.006 | 0.944 | 0.947 | 0.207 | 4.34 |
| >49 | 42% | 33% | 33% | |||||
| RT technique | - | - | - | - | ||||
| 3D-CRT | 18% | 6% | 6% | 0.18 | ||||
| IMRT | 44% | 33% | 33% | |||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Augustin, T.; Oliinyk, D.; Koehler, V.F.; Rauch, J.; Belka, C.; Spitzweg, C.; Käsmann, L. Clinical Outcome and Toxicity in the Treatment of Anaplastic Thyroid Cancer in Elderly Patients. J. Clin. Med. 2020, 9, 3231. https://doi.org/10.3390/jcm9103231
Augustin T, Oliinyk D, Koehler VF, Rauch J, Belka C, Spitzweg C, Käsmann L. Clinical Outcome and Toxicity in the Treatment of Anaplastic Thyroid Cancer in Elderly Patients. Journal of Clinical Medicine. 2020; 9(10):3231. https://doi.org/10.3390/jcm9103231
Chicago/Turabian StyleAugustin, Teresa, Dmytro Oliinyk, Viktoria Florentine Koehler, Josefine Rauch, Claus Belka, Christine Spitzweg, and Lukas Käsmann. 2020. "Clinical Outcome and Toxicity in the Treatment of Anaplastic Thyroid Cancer in Elderly Patients" Journal of Clinical Medicine 9, no. 10: 3231. https://doi.org/10.3390/jcm9103231
APA StyleAugustin, T., Oliinyk, D., Koehler, V. F., Rauch, J., Belka, C., Spitzweg, C., & Käsmann, L. (2020). Clinical Outcome and Toxicity in the Treatment of Anaplastic Thyroid Cancer in Elderly Patients. Journal of Clinical Medicine, 9(10), 3231. https://doi.org/10.3390/jcm9103231