Inter- and Intra-Rater Reliability of Individual Cerebral Blood Flow Measured by Quantitative Vessel-Flow Phase-Contrast MRI

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
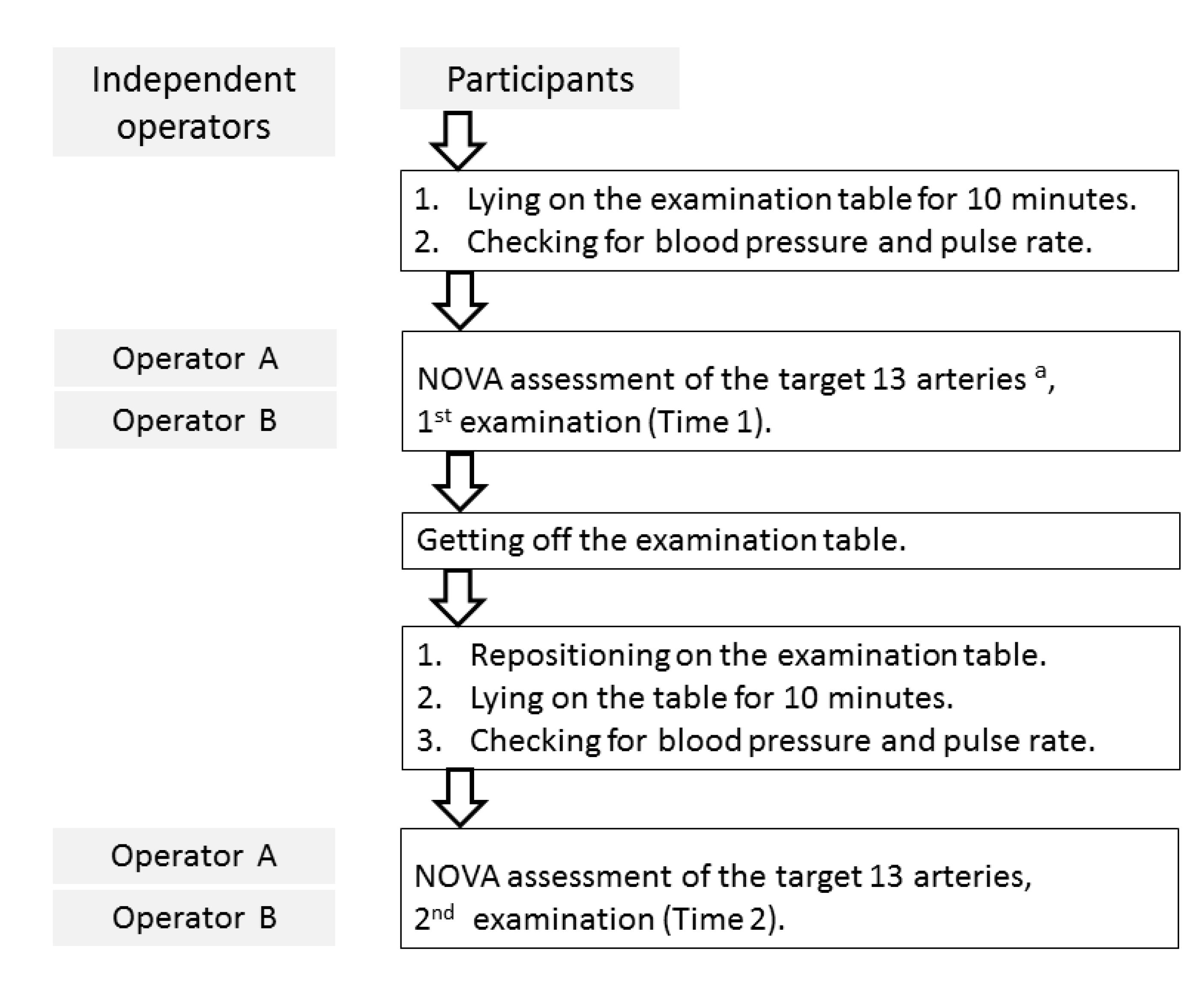
2.2. Techniques
2.3. Image Review and Flow Calculation
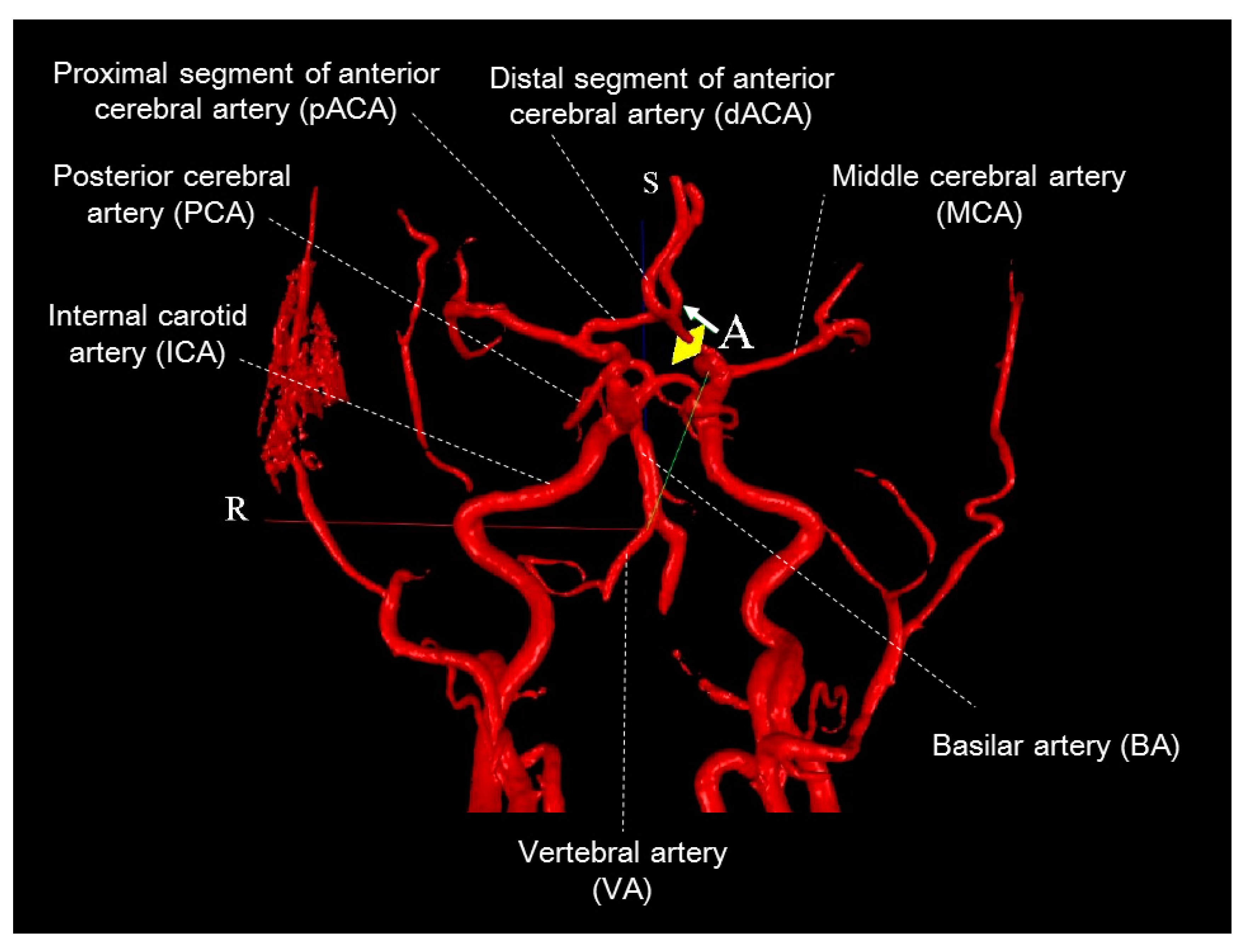
- Vessel identification: In the 2D image frame, the target artery in the flow ROI (region of interest) was centered. The size of the flow ROI was adjusted so that the artery diameter was 1/2–2/3 of the size of the flow ROI. The cut on the 3D image was confirmed to be on the correct artery and perpendicular to the artery’s longitudinal axis. We corrected the measurement with one background ROI to avoid the eddy current effect while image distortion happened.
- Vessel contour edit: The artery contours (automatically drawn) were checked to determine if they accurately tracked the artery borders on the magnitude, phase, and/or velocity images; were then modified, as necessary, to ensure that they tracked the velocity images.
- Flow check: Motion correction was applied if necessary.
- VENC check: It was checked to see if improper VENC was detected.
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Moran, P.R. A flow velocity zeugmatographic interlace for NMR imaging in humans. Magn. Reason. Imag. 1982, 1, 197–203. [Google Scholar] [CrossRef]
- Bryant, D.J.; Payne, J.A.; Firmin, D.N.; Longmore, D.B. Measurement of flow with NMR imaging using a gradient pulse and phase difference technique. J. Comput. Assist. Tomogr. 1984, 8, 588–593. [Google Scholar] [CrossRef]
- Nayler, G.L.; Firmin, D.N.; Longmore, D.B. Blood flow imaging by cine magnetic resonance. J. Comput. Assist. Tomogr. 1986, 10, 715–722. [Google Scholar] [CrossRef]
- Firmin, D.N.; Nayler, G.L.; Klipstein, R.H.; Underwood, S.R.; Rees, R.S.; Longmore, D.B. In vivo validation of MR velocity imaging. J. Comput. Assist. Tomogr. 1987, 11, 751–756. [Google Scholar] [CrossRef] [PubMed]
- Sakhare, A.R.; Barisano, G.; Pa, J. Assessing test–retest reliability of phase contrast MRI for measuring cerebrospinal fluid and cerebral blood flow dynamics. Magn. Reason. Med. 2019, 82, 658–670. [Google Scholar] [CrossRef] [PubMed]
- Amin-Hanjani, S.; Du, X.; Zhao, M. Use of Quantitative Magnetic Resonance Angiography to Stratify Stroke Risk in Symptomatic Vertebrobasilar Disease. J. Vasc. Surg. 2005, 42, 591. [Google Scholar] [CrossRef][Green Version]
- Calderon-Arnulphi, M.; Amin-Hanjani, S.; Alaraj, A.; Zhao, M.; Du, X.; Ruland, S.; Zhou, X.; Thulborn, K.; Charbel, F. In Vivo Evaluation of Quantitative MR Angiography in a Canine Carotid Artery Stenosis Model. Amer. J. Neurorad. 2011, 32, 1552–1559. [Google Scholar] [CrossRef]
- Zhao, M.; Charbel, F.T.; Alperin, N.; Loth, F.; Clark, M. Improved phase-contrast flow quantification by three-dimensional vessel localization. Magn. Reason. Imag. 2000, 18, 697–706. [Google Scholar] [CrossRef]
- Zhao, M.; Amin-Hanjani, S.; Ruland, S.; Curcio, A.; Ostergren, L.; Charbel, F. Regional Cerebral Blood Flow Using Quantitative MR Angiography. Am. J. Neurorad. 2007, 28, 1470–1473. [Google Scholar] [CrossRef]
- Neumar, R.W.; Otto, C.W.; Link, M.S.; Kronick, S.L.; Shuster, M.; Callaway, C.W.; Kudenchuk, P.J.; Ornato, J.P.; Mcnally, B.; Silvers, S.M.; et al. l. Part 8: Adult Advanced Cardiovascular Life Support: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2010, 122, S729–S767. [Google Scholar] [CrossRef]
- Willie, C.K.; Tzeng, Y.-C.; Fisher, J.A.; Ainslie, P.N. Integrative regulation of human brain blood flow. J. Phys. 2014, 592, 841–859. [Google Scholar] [CrossRef] [PubMed]
- Hallgren, K.A. Computing Inter-Rater Reliability for Observational Data: An Overview and Tutorial. Tutor. Quant. Meth. Psychol. 2012, 8, 23–34. [Google Scholar] [CrossRef] [PubMed]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chirop. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Braz, I.D.; Fisher, J.P. The impact of age on cerebral perfusion, oxygenation and metabolism during exercise in humans. J. Phys. 2015, 594, 4471–4483. [Google Scholar] [CrossRef]
- Pourahmadi, M.R.; Taghipour, M.; Jannati, E.; Mohseni-Bandpei, M.A.; Takamjani, I.E.; Rajabzadeh, F. Reliability and validity of an iPhone® application for the measurement of lumbar spine flexion and extension range of motion. PeerJ 2016, 4, e2355. [Google Scholar] [CrossRef]
- Papaharilaou, Y.; Doorly, D.J.; Sherwin, S.J. Assessing the accuracy of two-dimensional phase-contrast MRI measurements of complex unsteady flows. J. Magn. Reason. Imag. 2001, 14, 714–723. [Google Scholar] [CrossRef]
- Richter, Y.; Edelman, E.R. Cardiology Is Flow. Circulation 2006, 113, 2679–2682. [Google Scholar] [CrossRef]
- Scholtes, V.A.; Terwee, C.B.; Poolman, R.W. What makes a measurement instrument valid and reliable? Injury 2011, 42, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Lu, H.; Filbey, F.M.; Pinkham, A.E.; Mcadams, C.J.; Adinoff, B.; Daliparthi, V.; Cao, Y. Automatic and Reproducible Positioning of Phase-Contrast MRI for the Quantification of Global Cerebral Blood Flow. PLoS ONE 2014, 9, e25721. [Google Scholar] [CrossRef] [PubMed]
- Markl, M. Velocity Encoding and Flow Imaging. Available online: http://ee-classes.usc.edu/ee591/library/Markl-FlowImaging.pdf (accessed on 25 September 2005).
- Amin-Hanjani, S.; Du, X.; Pandey, D.K.; Thulborn, K.R.; Charbel, F.T. Effect of Age and Vascular Anatomy on Blood Flow in Major Cerebral Vessels. J. Cereb. Blood Flow Metabol. 2014, 35, 312–318. [Google Scholar] [CrossRef]
- Dankaerts, W.; O’Sullivan, P.; Straker, L.; Burnett, A.; Skouen, J. The inter-examiner reliability of a classification method for non-specific chronic low back pain patients with motor control impairment. Man. Ther. 2006, 11, 28–39. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable, Unit | Time 1 | Time 2 |
|---|---|---|
| Group | ||
| Healthy | 22 (73%) | - |
| Post-stroke | 8 (27%) | - |
| Sex | ||
| Male | 14 (47%) | - |
| Female | 16 (53%) | - |
| Age, years | 46.9 ± 14.4 (23.0–69.0) | - |
| <50 | 15 (50%) | - |
| >50 | 15 (50%) | - |
| Systolic blood pressure, mm Hg | 120.8 ± 17.3 (92.5–161.0) | 120.2 ± 14.3 (94.5–158.0) |
| Diastolic blood pressure, mm Hg | 74.8 ± 13.8 (45.0–105.5) | 74.5 ± 11.3 (48.5–97.0) |
| Mean arterial pressure, mm Hg | 90.1 ± 14.5 (67.2–121.0) | 89.8 ± 11.4 (64.7–113.7) |
| Pulse rate, beats/min | 72.6 ± 11.7 (49.8–103.4) | 72.7 ± 18 (51–134.3) |
| Mean volume blood flow, mL/min | 755.5 ± 173.4 (472.5–972.5) | 726.8 ± 146.9 (515–1007) |
| Variable, Unit | Time 1 | Time 2 |
|---|---|---|
| Operator A | ||
| LVA | 124.8 ± 48.5 (37–215) | 121.1 ± 50.9 (34–251) |
| RVA | 78.6 ± 36.1 (16–144) | 78.3 ± 26.7 (26–134) |
| BA | 148.2 ± 60.3 (25–306) | 140.7 ± 50.8 (14–243) |
| LPCA | 88.2 ± 29.9 (46–188) | 79.7 ± 18.7 (49–118) |
| RPCA | 83.2 ± 23.5 (41–141) | 77.8 ± 21.8 (42–126) |
| LMCA | 163.6 ± 50.8 (81–298) | 156.7 ± 38.9 (98–223) |
| RMCA | 172.3 ± 42.6 (91–285) | 161.8 ± 35.9 (93–226) |
| pLACA | 111.6 ± 29.9 (60–208) | 103.5 ± 25.1 (54–159) |
| pRACA | 101.1 ± 30.3 (29–168) | 96.8 ± 41.9 (14–222) |
| LICA | 271.5 ± 79.4 (142–477) | 256.1 ± 54.1 (155–361) |
| RICA | 273.8 ± 81.5 (103–446) | 265.8 ± 66.1 (148–419) |
| dLACA | 79.9 ± 23.1 (42–135) | 74.7 ± 18.3 (41–112) |
| dRACA | 69.3 ± 26.1 (34–139) | 66.5 ± 16.4 (31–103) |
| Operator B | ||
| LVA | 129.3 ± 54 (33–257) | 123.9 ± 52.6 (35–235) |
| RVA | 84 ± 37.5 (39–169) | 87.9 ± 32.2 (41–157) |
| BA | 149.2 ± 64.1 (16–261) | 142.4 ± 51.8 (28–232) |
| LPCA | 81.3 ± 28.1 (43–177) | 80.5 ± 20.4 (39–111) |
| RPCA | 76 ± 24 (39–132) | 80.7 ± 21.1 (36–122) |
| LMCA | 158.1 ± 52.4 (30–298) | 157.5 ± 50.2 (72–309) |
| RMCA | 164.3 ± 41.2 (87–265) | 167.7 ± 49.8 (98–335) |
| pLACA | 110.7 ± 34 (57–202) | 106.7 ± 31.5 (48–202) |
| pRACA | 97.1 ± 36.4 (25–172) | 94.4 ± 32.5 (32–159) |
| LICA | 273.7 ± 91.3 (152–629) | 247 ± 49.4 (144–312) |
| RICA | 276 ± 73.6 (141–498) | 257.2 ± 72.7 (115–385) |
| dLACA | 77.9 ± 27.4 (47–178) | 74.7 ± 23.7 (33–140) |
| dRACA | 67.2 ± 25 (21–129) | 70.8 ± 29.4 (35–181) |
| Artery | Operator A | Operator B | Average Measure * | SEM * | MDC95% | |||
|---|---|---|---|---|---|---|---|---|
| ICC (95% CI) | P-Value | ICC (95% CI) | P-Value | ICC (95% CI) | P-Value | (mL/min) | (mL/min) | |
| LVA | 0.85 (0.689–0.931) | <0.001 | 0.773 (0.551–0.893) | <0.001 | 0.925 (0.83–0.967) | <0.001 | 20.1 | 55.7 |
| RVA | 0.794 (0.573–0.907) | <0.001 | 0.883 (0.749–0.948) | <0.001 | 0.954 (0.892–0.981) | <0.001 | 12.0 | 33.3 |
| BA | 0.799 (0.6–0.904) | <0.001 | 0.773 (0.555–0.891) | <0.001 | 0.893 (0.761–0.952) | <0.001 | 24.2 | 67.1 |
| LPCA | 0.568 (0.231–0.784) | 0.001 | 0.695 (0.42–0.853) | <0.001 | 0.837 (0.63–0.928) | <0.001 | 11.6 | 32.2 |
| RPCA | 0.548 (0.185–0.78) | 0.003 | 0.676 (0.39–0.843) | <0.001 | 0.841 (0.625–0.933) | <0.001 | 12.3 | 34.1 |
| LMCA | 0.75 (0.518–0.88) | <0.001 | 0.888 (0.767–0.948) | <0.001 | 0.881 (0.73–0.948) | <0.001 | 18.2 | 50.4 |
| RMCA | 0.523 (0.177–0.753) | 0.003 | 0.638 (0.34–0.82) | <0.001 | 0.749 (0.43–0.889) | 0.001 | 23.2 | 64.3 |
| pLACA | 0.65 (0.358–0.826) | <0.001 | 0.858 (0.712–0.933) | <0.001 | 0.855 (0.677–0.935) | <0.001 | 12.8 | 35.5 |
| pRACA | 0.786 (0.572–0.9) | <0.001 | 0.861 (0.718–0.934) | <0.001 | 0.936 (0.856–0.972) | <0.001 | 14.0 | 38.8 |
| LICA | 0.687 (0.415–0.846) | <0.001 | 0.624 (0.318–0.812) | <0.001 | 0.841 (0.645–0.929) | <0.001 | 31.7 | 87.9 |
| RICA | 0.787 (0.58–0.899) | <0.001 | 0.554 (0.22–0.772) | 0.001 | 0.880 (0.733–0.946) | <0.001 | 34.7 | 96.2 |
| dLACA | 0.482 (0.124–0.729) | 0.005 | 0.141 (−0.262–0.502) | 0.25 | 0.641 (0.185–0.842) | 0.007 | 13.8 | 38.3 |
| dRACA | 0.526 (0.181–0.755) | 0.002 | 0.687 (0.415–0.847) | <0.001 | 0.796 (0.537–0.91) | <0.001 | 13.0 | 36.0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, K.-H.; Lee, Y.-H.; Chen, C.-Y.; Lin, M.-F.; Lin, Y.C.; Chen, J.-H.; Chan, W.P. Inter- and Intra-Rater Reliability of Individual Cerebral Blood Flow Measured by Quantitative Vessel-Flow Phase-Contrast MRI. J. Clin. Med. 2020, 9, 3099. https://doi.org/10.3390/jcm9103099
Chang K-H, Lee Y-H, Chen C-Y, Lin M-F, Lin YC, Chen J-H, Chan WP. Inter- and Intra-Rater Reliability of Individual Cerebral Blood Flow Measured by Quantitative Vessel-Flow Phase-Contrast MRI. Journal of Clinical Medicine. 2020; 9(10):3099. https://doi.org/10.3390/jcm9103099
Chicago/Turabian StyleChang, Kwang-Hwa, Yuan-Hao Lee, Chia-Yuen Chen, Ming-Fang Lin, Ying Chin Lin, Jyh-Horng Chen, and Wing P. Chan. 2020. "Inter- and Intra-Rater Reliability of Individual Cerebral Blood Flow Measured by Quantitative Vessel-Flow Phase-Contrast MRI" Journal of Clinical Medicine 9, no. 10: 3099. https://doi.org/10.3390/jcm9103099
APA StyleChang, K.-H., Lee, Y.-H., Chen, C.-Y., Lin, M.-F., Lin, Y. C., Chen, J.-H., & Chan, W. P. (2020). Inter- and Intra-Rater Reliability of Individual Cerebral Blood Flow Measured by Quantitative Vessel-Flow Phase-Contrast MRI. Journal of Clinical Medicine, 9(10), 3099. https://doi.org/10.3390/jcm9103099