Serum Exosomal MicroRNA, miR-10b-5p, as a Potential Diagnostic Biomarker for Early-Stage Hepatocellular Carcinoma

 , , ,
, , ,
Abstract
1. Introduction
2. Experimental Section
2.1. HCC Cell Lines and Culture
2.2. Exosome Isolation from Cell Culture Media And Peripheral Blood
2.3. Transmission Electron Microscopy
2.4. MiR Sequencing
2.5. Ingenuity Pathway Analysis (IPA)
2.6. Analysis of Publicly Available Genomic Data
2.7. MiR Target Prediction and Molecular Pathway Mining
2.8. Quantitative Real-Time PCR (qRT-PCR)
2.9. Validation Cohort and Clinical Term Definitions
2.10. Statistical Analysis
3. Results
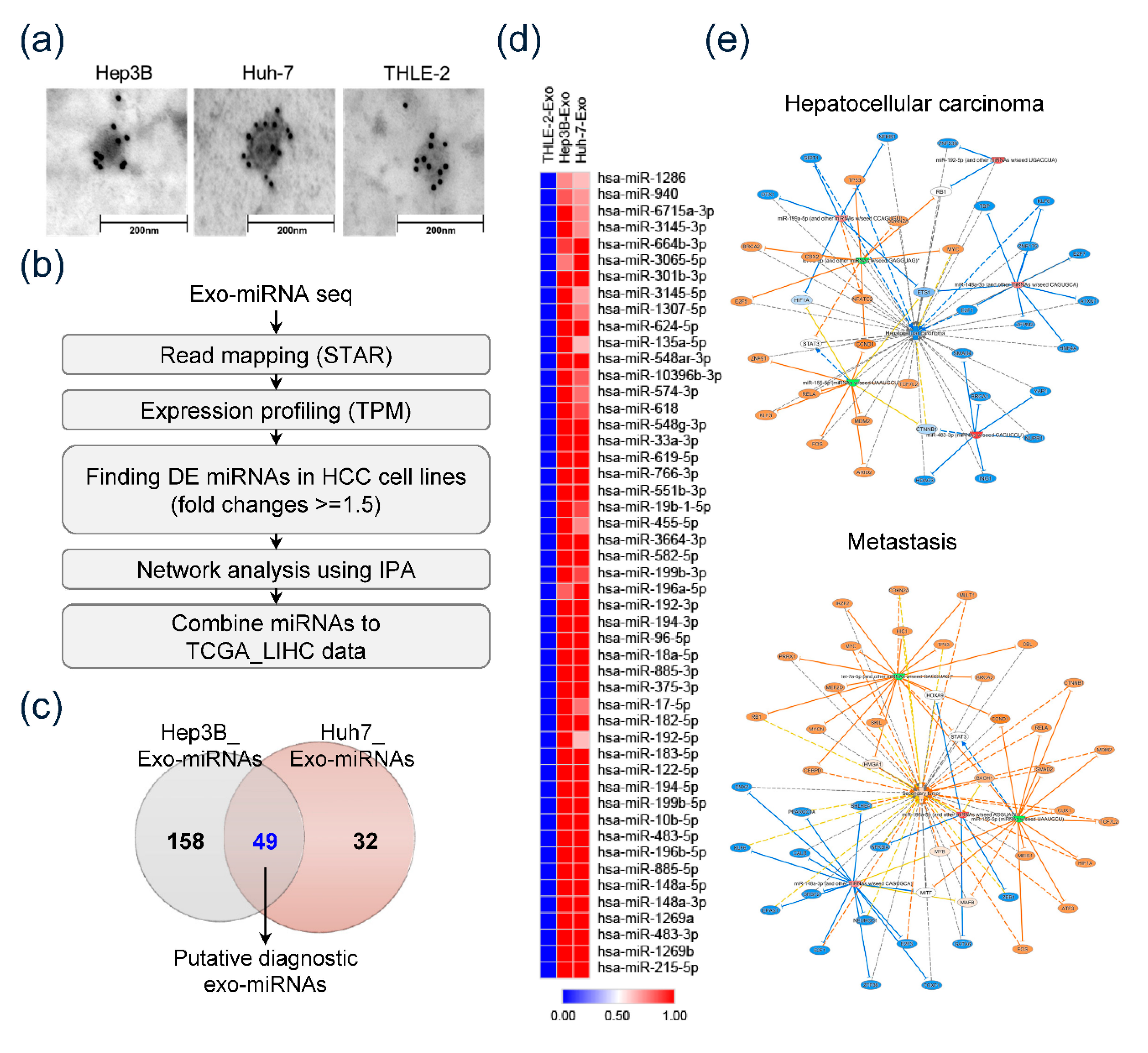
3.1. Confirmation of HEX and Identification of Overexpressed HCC-Derived Exo-MiRs
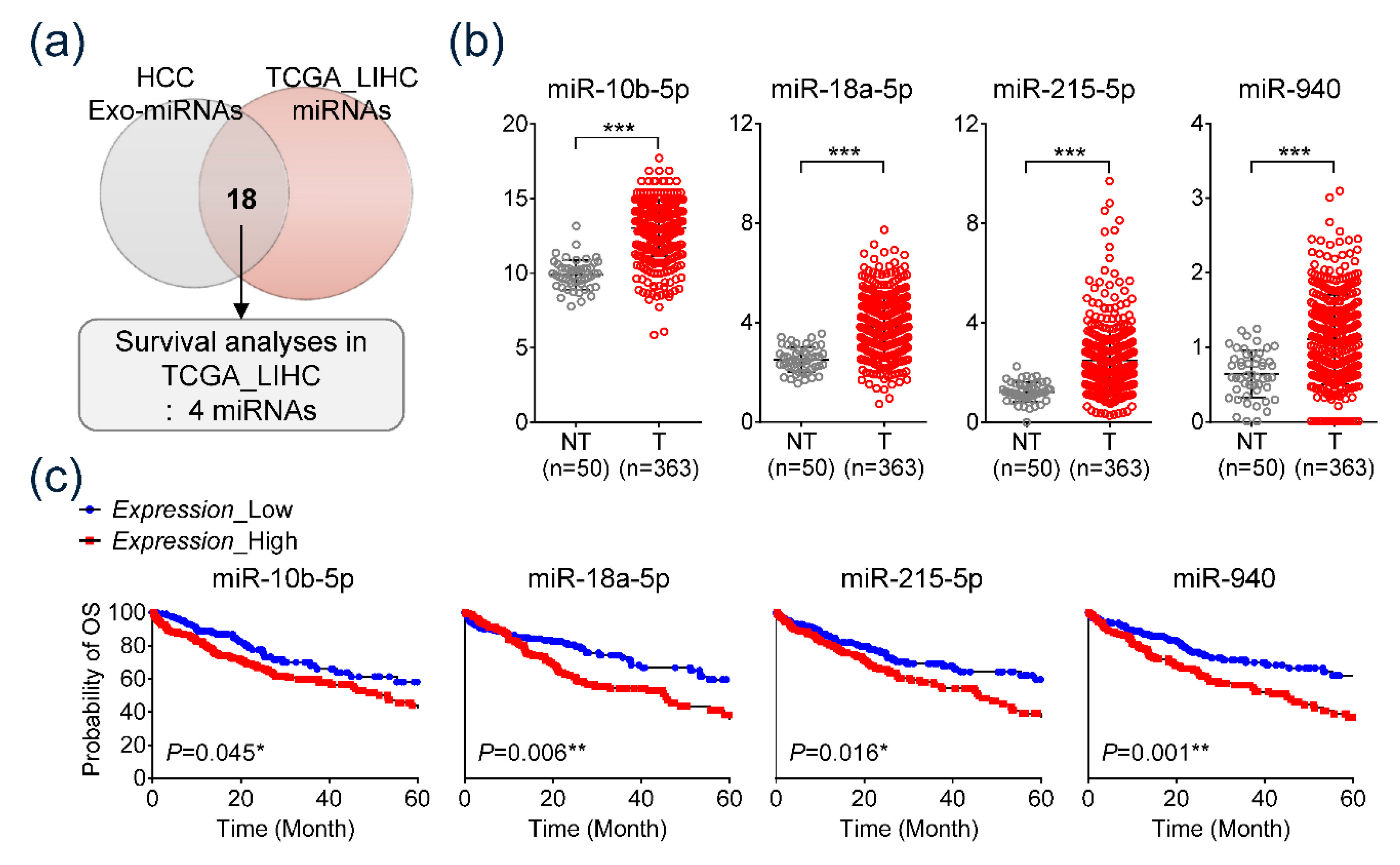
3.2. TCGA Data Analysis of HCC-Derived Exo-MiRs
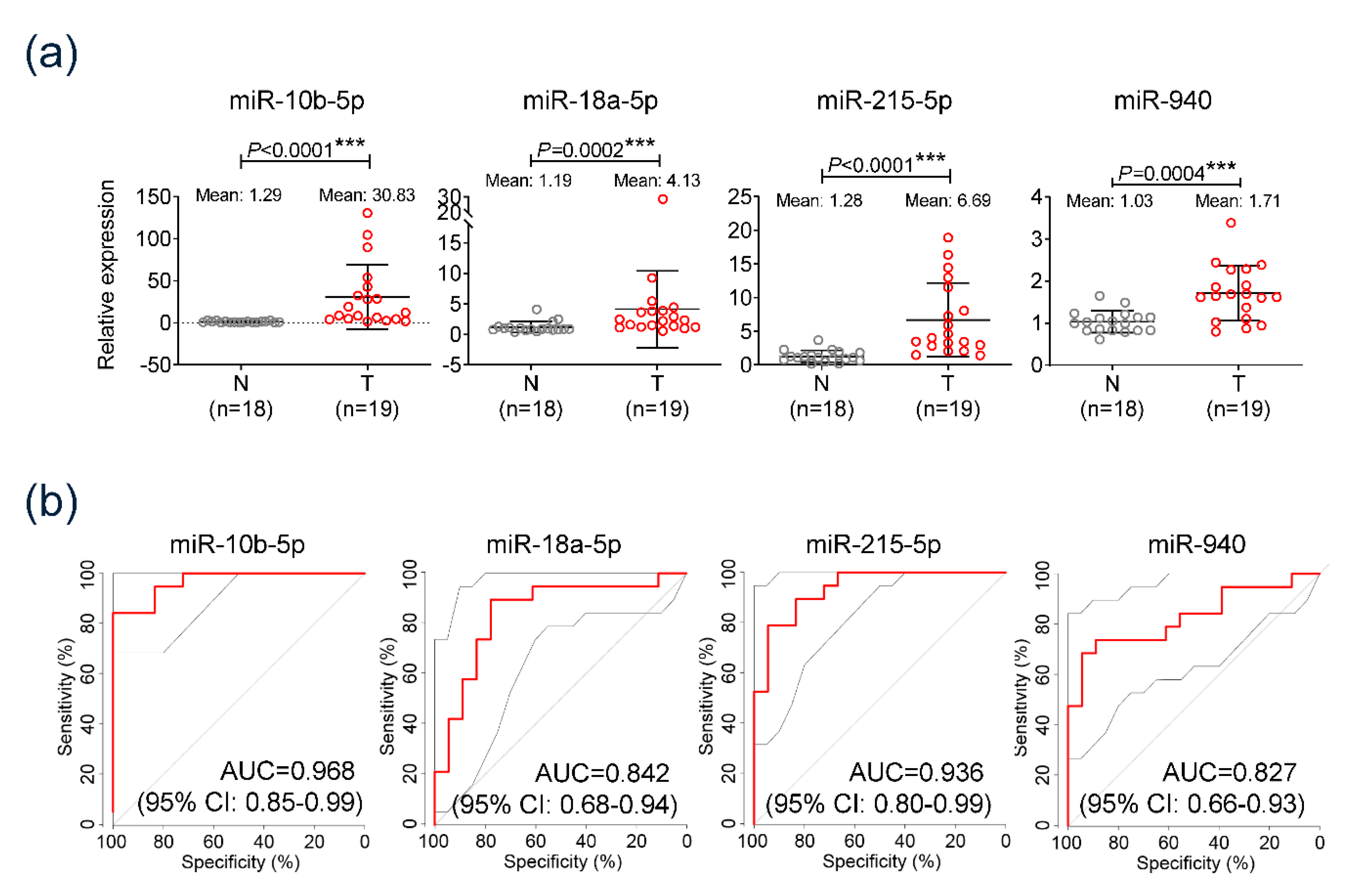
3.3. Diagnostic Significance of the Serum Exo-miRs in Cohort
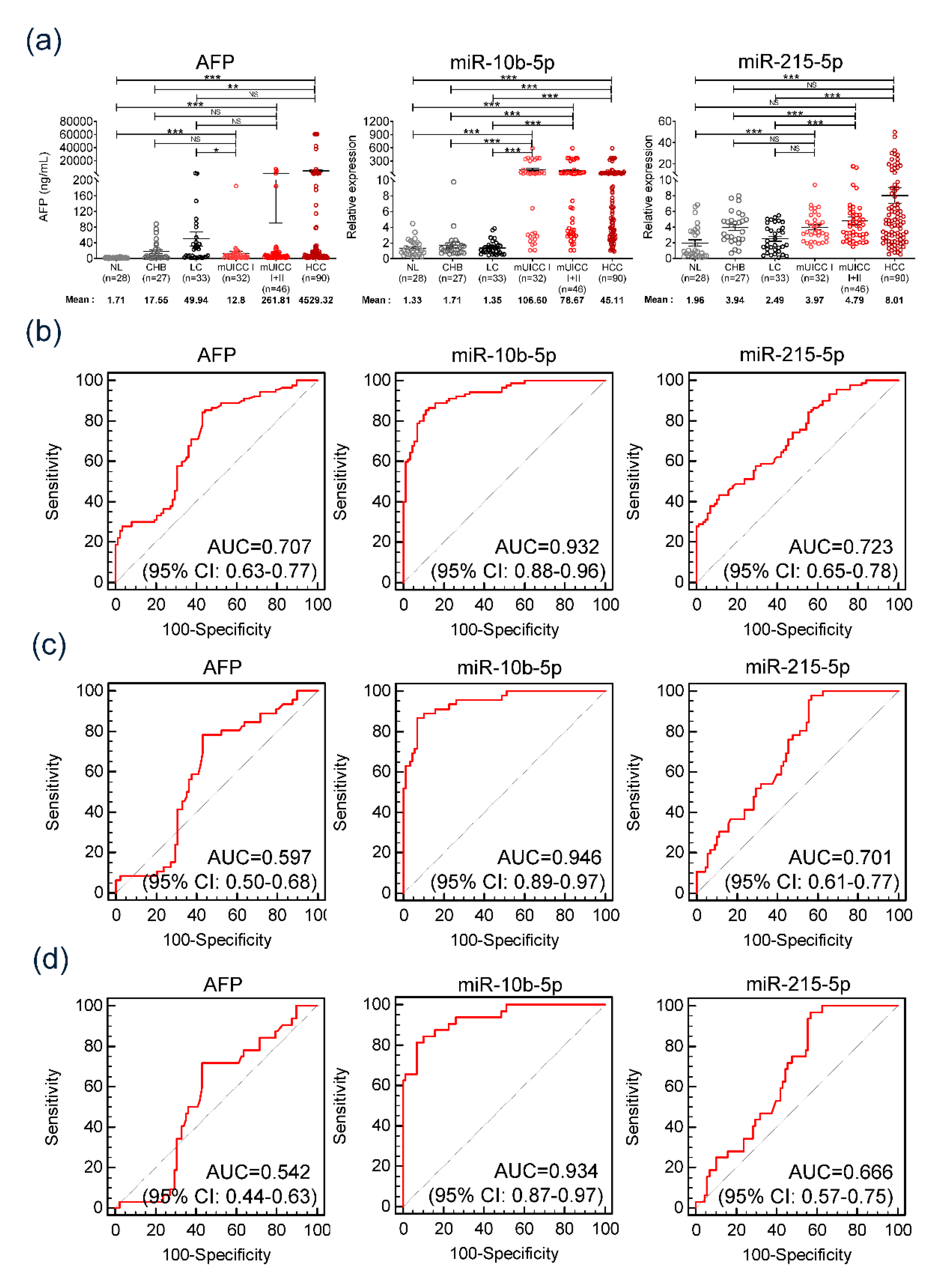
3.4. Significance of Serum Exo-miRs in Diagnosing HCC in the Validation Cohort
3.5. Diagnostic Efficiency of Serum Exo-miR-10b-5p in Patients at High Risk of Developing HCC
3.6. Prognostic Implication of the Serum Exosomal miR-10b-5p and Exosomal miRNA-215-5p
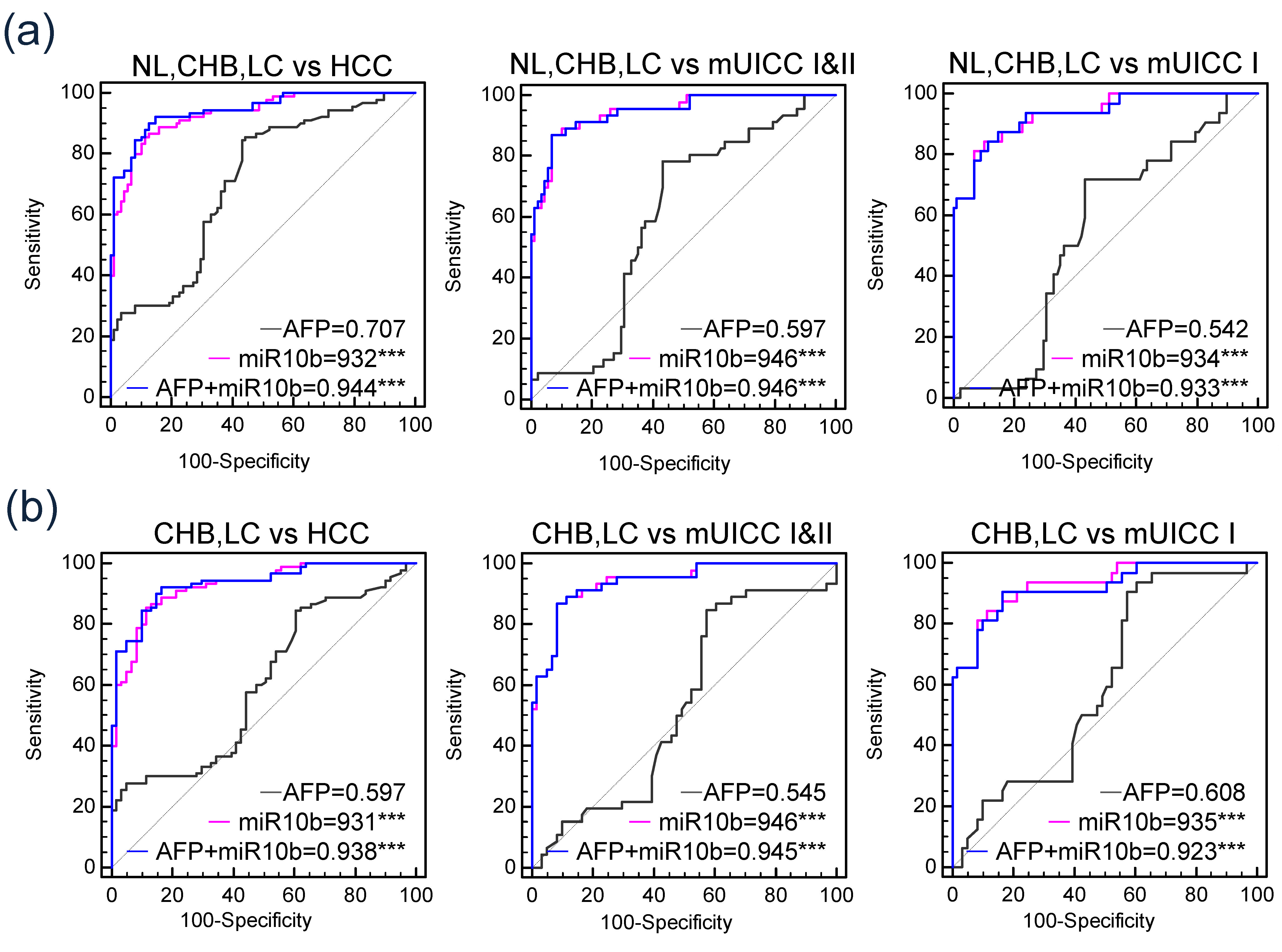
3.7. Comparison between Diagnostic Efficiencies of Serum Exo-miRNA-10b-5p and Serum miRNA-10b-5p
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ghouri, Y.A.; Mian, I.; Rowe, J.H. Review of hepatocellular carcinoma: Epidemiology, etiology, and carcinogenesis. J. Carcinog. 2017, 16. [Google Scholar] [CrossRef]
- Korean Liver Cancer Association. 2018 Korean Liver Cancer Association–National Cancer Center Korea Practice Guidelines for the Management of Hepatocellular Carcinoma. Gut Liver 2019, 13, 227. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.-H.; Kim, S.Y.; Tang, A.; Lee, J.M. Comparison of international guidelines for noninvasive diagnosis of hepatocellular carcinoma: 2018 update. Clin. Mol. Hepatol. 2019, 25, 245–263. [Google Scholar] [CrossRef] [PubMed]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef]
- Cheung, A.H.-K.; Chow, C.; To, K.-F. Latest development of liquid biopsy. J. Thorac. Dis. 2018, 10, S1645. [Google Scholar] [CrossRef]
- Peterson, M.F.; Otoc, N.; Sethi, J.K.; Gupta, A.; Antes, T.J. Integrated systems for exosome investigation. Methods 2015, 87, 31–45. [Google Scholar] [CrossRef]
- Regev-Rudzki, N.; Wilson, D.W.; Carvalho, T.G.; Sisquella, X.; Coleman, B.M.; Rug, M.; Bursac, D.; Angrisano, F.; Gee, M.; Hill, A.F. Cell-cell communication between malaria-infected red blood cells via exosome-like vesicles. Cell 2013, 153, 1120–1133. [Google Scholar] [CrossRef]
- Zhang, J.; Li, S.; Li, L.; Li, M.; Guo, C.; Yao, J.; Mi, S. Exosome and exosomal microRNA: Trafficking, sorting, and function. Genom. Proteom. Bioinform. 2015, 13, 17–24. [Google Scholar] [CrossRef]
- Korean Association for the Study of the Liver. KASL clinical practice guidelines for management of chronic hepatitis B. Clin. Mol. Hepatol. 2019, 25, 93. [Google Scholar] [CrossRef]
- Fukui, H.; Saito, H.; Ueno, Y.; Uto, H.; Obara, K.; Sakaida, I.; Shibuya, A.; Seike, M.; Nagoshi, S.; Segawa, M.; et al. Evidence-based clinical practice guidelines for liver cirrhosis 2015. J. Gastroenterol. 2016, 51, 629–650. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G* Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Volk, M.L.; Hernandez, J.C.; Su, G.L.; Lok, A.S.; Marrero, J.A. Risk factors for hepatocellular carcinoma may impair the performance of biomarkers: A comparison of AFP, DCP, and AFP-L3 1. Cancer Biomark. 2007, 3, 79–87. [Google Scholar] [CrossRef] [PubMed]
- Best, J.; Bilgi, H.; Heider, D.; Schotten, C.; Manka, P.; Bedreli, S.; Gorray, M.; Ertle, J.; van Grunsven, L.; Dechêne, A. The GALAD scoring algorithm based on AFP, AFP-L3, and DCP significantly improves detection of BCLC early stage hepatocellular carcinoma. Zeitschrift Für Gastroenterologie 2016, 54, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Q.; Gong, L.; Wang, J.; Tu, Q.; Yao, L.; Zhang, J.-R.; Han, X.-J.; Zhu, S.-J.; Wang, S.-M.; Li, Y.-H.; et al. miR-10b exerts oncogenic activity in human hepatocellular carcinoma cells by targeting expression of CUB and sushi multiple domains 1 (CSMD1). BMC Cancer 2016, 16, 806. [Google Scholar] [CrossRef]
- Li, Q.-J.; Zhou, L.; Yang, F.; Wang, G.-X.; Zheng, H.; Wang, D.-S.; He, Y.; Dou, K.-F. MicroRNA-10b promotes migration and invasion through CADM1 in human hepatocellular carcinoma cells. Tumor Biol. 2012, 33, 1455–1465. [Google Scholar] [CrossRef]
- Liao, C.-G.; Kong, L.-M.; Zhou, P.; Yang, X.-L.; Huang, J.-G.; Zhang, H.-L.; Lu, N. miR-10b is overexpressed in hepatocellular carcinoma and promotes cell proliferation, migration and invasion through RhoC, uPAR and MMPs. J. Transl. Med. 2014, 12, 234. [Google Scholar] [CrossRef]
- Jiang, L.; Cheng, Q.; Zhang, B.-H.; Zhang, M.-Z. Circulating microRNAs as biomarkers in hepatocellular carcinoma screening: A validation set from China. Medicine 2015, 94, e603. [Google Scholar] [CrossRef]
- Wang, H.; Hou, L.; Li, A.; Duan, Y.; Gao, H.; Song, X. Expression of serum exosomal microRNA-21 in human hepatocellular carcinoma. BioMed Res. Int. 2014, 2014. [Google Scholar] [CrossRef]
- White, N.; Khella, H.; Grigull, J.; Adzovic, S.; Youssef, Y.; Honey, R.; Stewart, R.; Pace, K.; Bjarnason, G.; Jewett, M.A.S.; et al. miRNA profiling in metastatic renal cell carcinoma reveals a tumour-suppressor effect for miR-215. Br. J. Cancer 2011, 105, 1741. [Google Scholar] [CrossRef]
- Vychytilova-Faltejskova, P.; Merhautova, J.; Machackova, T.; Gutierrez-Garcia, I.; Garcia-Solano, J.; Radova, L.; Brchnelova, D.; Slaba, K.; Svoboda, M.; Halamkova, J.; et al. MiR-215-5p is a tumor suppressor in colorectal cancer targeting EGFR ligand epiregulin and its transcriptional inducer HOXB9. Oncogenesis 2017, 6, 399. [Google Scholar] [CrossRef]
- Ullmann, P.; Nurmik, M.; Schmitz, M.; Rodriguez, F.; Weiler, J.; Qureshi-Baig, K.; Felten, P.; Nazarov, P.V.; Nicot, N.; Zuegel, N.; et al. Tumor suppressor miR-215 counteracts hypoxia-induced colon cancer stem cell activity. Cancer Lett. 2019, 450, 32–41. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Wang, Y.M.; Xu, S.; Wang, W.G.; Chen, Y.; Mao, J.Y.; Tian, B.L. MicroRNA-215 is upregulated by treatment with Adriamycin and leads to the chemoresistance of hepatocellular carcinoma cells and tissues. Mol. Med. Rep. 2015, 12, 5274–5280. [Google Scholar] [CrossRef]
- Mao, B.; Wang, G. MicroRNAs involved with hepatocellular carcinoma. Oncol. Rep. 2015, 34, 2811–2820. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.-Q.; Meng, H.; Wang, N.; Liang, L.-N.; Liu, L.-N.; Lu, S.-M.; Luan, Y. Serum microRNA 143 and microRNA 215 as potential biomarkers for the diagnosis of chronic hepatitis and hepatocellular carcinoma. Diagn. Pathol. 2014, 9, 135. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.H.; Zhou, H.; Zhao, X.X.; Ding, H.; Li, W.; Qin, L.; Pan, Y.L. Role of exosomes and exosomal microRNAs in hepatocellular carcinoma: Potential in diagnosis and antitumour treatments. Int. J. Mol. Med. 2018, 41, 1809–1816. [Google Scholar] [CrossRef] [PubMed]
- Sohn, W.; Kim, J.; Kang, S.H.; Yang, S.R.; Cho, J.Y.; Cho, H.C.; Shim, S.G.; Paik, Y.H. Serum exosomal microRNAs as novel biomarkers for hepatocellular carcinoma. Exp. Mol. Med. 2015, 47, e184. [Google Scholar] [CrossRef] [PubMed]
- Jun, L.; Yang, G.; Zhisu, L. The utility of serum exosomal microRNAs in hepatocellular carcinoma. Biomed. Pharmacother. 2019, 111, 1221–1227. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Validation Cohort | |||
|---|---|---|---|---|
| Normal (n = 28) | CHB (n = 27) | LC (n = 33) | HCC (n = 90) | |
| Age, mean ± SD | 34.1 ± 7.6 | 45.2 ± 11.1 | 53.1 ± 10.1 | 55.2 ± 9.02 |
| Male sex, n (%) | 2 (7.1) | 15 (55.6) | 19 (57.6) | 70 (77.8) |
| AST, IU/mL | 19.60 ±5.46 | 50.44 ± 51.50 | 79.19 ± 100.91 | 71.57 ± 96.77 |
| ALT, IU/mL | 20.00 ± 15.12 | 57.26 ± 66.31 | 77.25 ± 100.99 | 48.12 ± 59.28 |
| Platelet, x109/L | 290.40 ± 42.18 | 190.56 ± 4.39 | 123.35 ± 65.59 | 166.44 ± 84.17 |
| AFP (ng/mL), mean ± SD | 1.71 ± 0.77 | 17.55 ± 24.97 | 49.94 ± 104.09 | 4290.43 ± 14525.79 |
| Etiology, n (%) HBV/HCV/alcohol/others | 26 (96.3)/1 (3.7)/0/0 | 28 (84.8)/3 (9.1)/2 (6.1)/0 | 82 (91.1)/4 (4.5))/3 (3.3)/1 (1.1) | |
| Albumin (g/L), mean ± SD | 4.56 ± 0.42 | 4.05 ± 0.53 | 4.28 ± 0.55 | |
| Bilirubin (mg/dL), mean ± SD | 0.81 ± 0.33 | 1.05 ± 1.03 | 1.34± 3.53 | |
| INR, mean ± SD | 1.23 ± 0.31 | 1.24 ± 0.11 | 1.25 ± 0.55 | |
| Modified UICC stage I/II/III/IVa/Ivb, n (%) | 32 (36)/14 (16)/26 (29)/11 (12)/ 7 (8) | |||
| HCC vs. Non Tumor | |||||
| P vs. AFP | AUC | 95% CI | Sensitivity (%) | Specificity (%) | |
| AFP (20 ng/mL) | 1 | 0.707 | 0.635–0.773 | 37.778 | 71.591 |
| miR-10b-5p (1.8-fold) | <0.0001 | 0.932 | 0.884–0.964 | 91.111 | 75.000 |
| miR-215b-5p (5.25-fold) | 0.761 | 0.723 | 0.651–0.787 | 43.333 | 88.636 |
| mUICC I&II vs. Non Tumor | |||||
| P vs. AFP | AUC | 95% CI | Sensitivity (%) | Specificity (%) | |
| AFP (20 ng/mL) | 1 | 0.597 | 0.509–0.681 | 15.217 | 71.591 |
| miR-10b-5p (1.8-fold) | <0.0001 | 0.946 | 0.894–0.978 | 93.478 | 75.000 |
| miR-215b-5p (5.25-fold) | 0.1037 | 0.701 | 0.616–0.777 | 30.435 | 88.636 |
| mUICC I vs. Non Tumor | |||||
| P vs. AFP | AUC | 95% CI | Sensitivity (%) | Specificity (%) | |
| AFP (20 ng/mL) | 1 | 0.542 | 0.449–0.634 | 9.375 | 71.591 |
| miR-10b-5p (1.8-fold) | <0.0001 | 0.934 | 0.874–0.971 | 90.652 | 75.000 |
| miR-215b-5p (5.25-fold) | 0.1016 | 0.666 | 0.574–0.749 | 25.000 | 88.636 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, H.J.; Eun, J.W.; Baek, G.O.; Seo, C.W.; Ahn, H.R.; Kim, S.S.; Cho, S.W.; Cheong, J.Y. Serum Exosomal MicroRNA, miR-10b-5p, as a Potential Diagnostic Biomarker for Early-Stage Hepatocellular Carcinoma. J. Clin. Med. 2020, 9, 281. https://doi.org/10.3390/jcm9010281
Cho HJ, Eun JW, Baek GO, Seo CW, Ahn HR, Kim SS, Cho SW, Cheong JY. Serum Exosomal MicroRNA, miR-10b-5p, as a Potential Diagnostic Biomarker for Early-Stage Hepatocellular Carcinoma. Journal of Clinical Medicine. 2020; 9(1):281. https://doi.org/10.3390/jcm9010281
Chicago/Turabian StyleCho, Hyo Jung, Jung Woo Eun, Geum Ok Baek, Chul Won Seo, Hye Ri Ahn, Soon Sun Kim, Sung Won Cho, and Jae Youn Cheong. 2020. "Serum Exosomal MicroRNA, miR-10b-5p, as a Potential Diagnostic Biomarker for Early-Stage Hepatocellular Carcinoma" Journal of Clinical Medicine 9, no. 1: 281. https://doi.org/10.3390/jcm9010281
APA StyleCho, H. J., Eun, J. W., Baek, G. O., Seo, C. W., Ahn, H. R., Kim, S. S., Cho, S. W., & Cheong, J. Y. (2020). Serum Exosomal MicroRNA, miR-10b-5p, as a Potential Diagnostic Biomarker for Early-Stage Hepatocellular Carcinoma. Journal of Clinical Medicine, 9(1), 281. https://doi.org/10.3390/jcm9010281