Safety of Abatacept in Italian Patients with Rheumatoid Arthritis and Interstitial Lung Disease: A Multicenter Retrospective Study



 , ,
, , 
Abstract
:1. Introduction
2. Patients and Methods
2.1. Outcome Variables
2.2. Statistical Analysis
3. Results
3.1. Previous Treatments
3.2. Current Treatments
3.3. ILD Radiologic Patterns
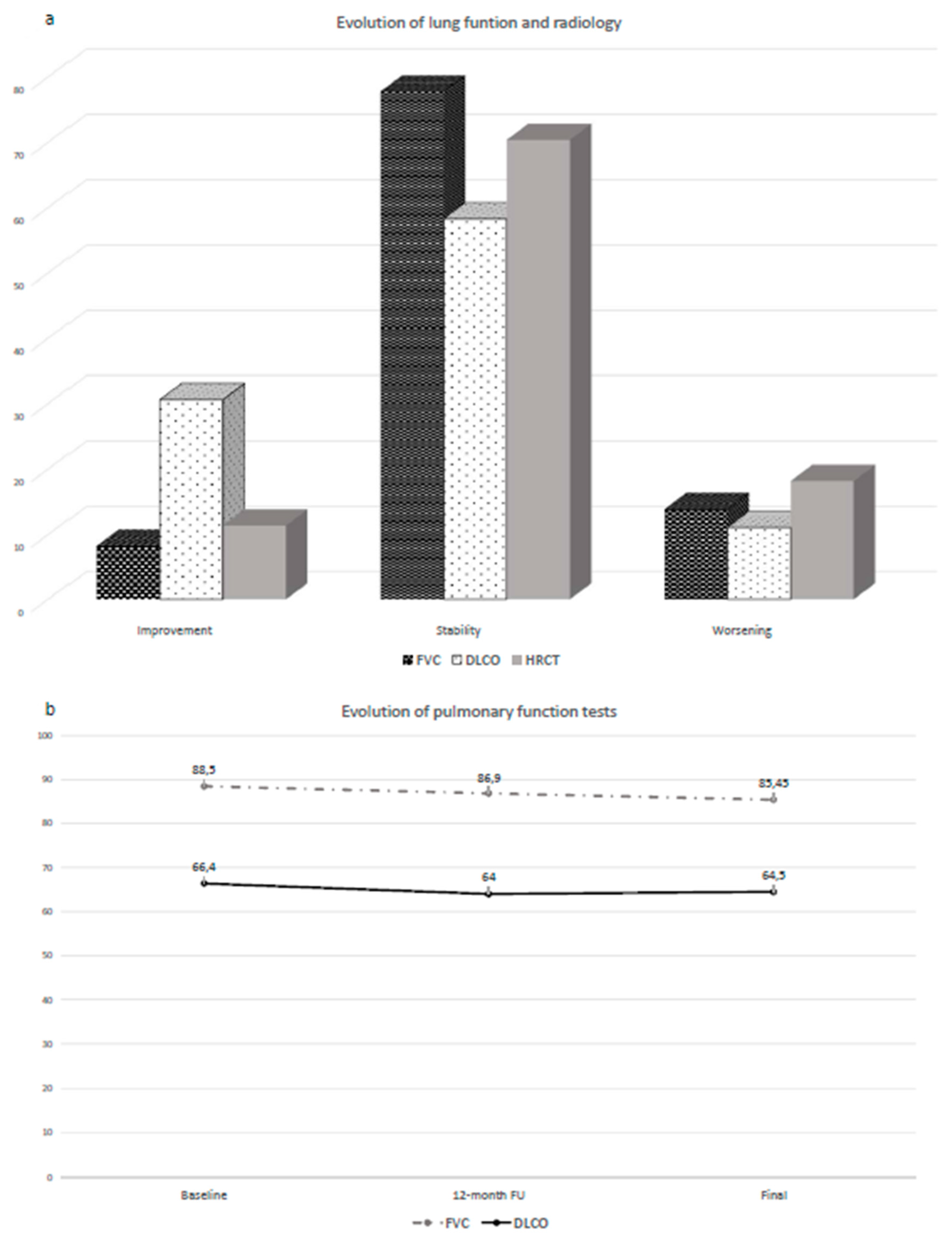
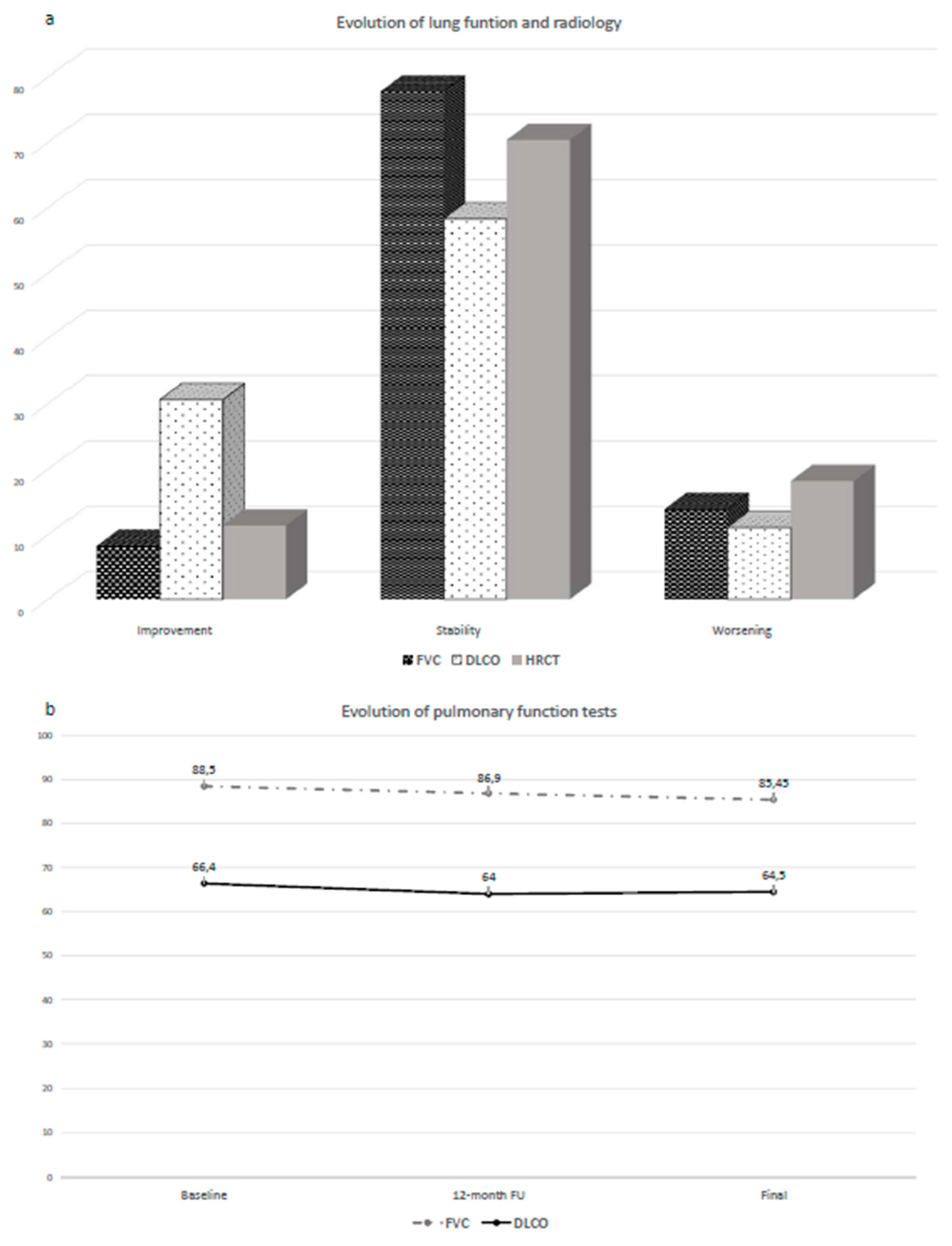
3.4. Pulmonary Function Tests
3.5. Evolution of Lung Function and HRCT
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Smolen, J.S.; Aletaha, D.; McInnes, I.B. Rheumatoid arthritis. Lancet 2016, 22, 2023–2038. [Google Scholar] [CrossRef]
- Spagnolo, P.; Lee, J.S.; Sverzellati, N.; Rossi, G.; Cottin, V. The Lung in Rheumatoid Arthritis: Focus on Interstitial Lung Disease. Arthritis Rheumatol. 2018, 70, 1544–1554. [Google Scholar] [CrossRef] [Green Version]
- Bongartz, T.; Nannini, C.; Medina-Velasquez, Y.F.; Achenbach, S.J.; Crowson, C.S.; Ryu, J.H.; Vassallo, R.; Gabriel, S.E.; Matteson, E.L. Incidence and mortality of interstitial lung disease in rheumatoid arthritis: A population-based study. Arthritis Rheum. 2010, 62, 1583–1591. [Google Scholar] [CrossRef] [Green Version]
- Olson, A.L.; Swigris, J.J.; Sprunger, D.B.; Fischer, A.; Fernandez-Perez, E.R.; Solomon, J.; Murphy, J.; Cohen, M.; Raghu, G.; Brown, K.K. Rheumatoid arthritis-interstitial lung disease-associated mortality. Am. J. Respir. Crit. Care Med. 2011, 183, 372–378. [Google Scholar] [CrossRef] [Green Version]
- Raimundo, K.; Solomon, J.J.; Olson, A.L.; Kong, A.M.; Cole, A.L.; Fischer, A.; Swigris, J.J. Rheumatoid Arthritis-Interstitial Lung Disease in the United States: Prevalence, Incidence, and Healthcare Costs and Mortality. J. Rheumatol. 2019, 46, 360–369. [Google Scholar] [CrossRef]
- Hyldgaard, C.; Hilberg, O.; Pedersen, A.B.; Ulrichsen, S.P.; Løkke, A.; Bendstrup, E.; Ellingsen, T. A population-based cohort study of rheumatoid arthritis-associated interstitial lung disease: Comorbidity and mortality. Ann. Rheum. Dis. 2017, 76, 1700–1706. [Google Scholar] [CrossRef]
- Chatzidionisyou, A.; Catrina, A.I. The lung in rheumatoid arthritis, cause or consequence? Curr. Opin. Rheumatol. 2016, 28, 76–82. [Google Scholar] [CrossRef]
- Roubille, C.; Haraoui, B. Interstitial lung diseases induced or exacerbated by DMARDS and biologic agents in rheumatoid arthritis: A systematic literature review. Semin. Arthritis Rheum. 2014, 43, 613–626. [Google Scholar] [CrossRef]
- Jani, M.; Hirani, N.; Matteson, E.L.; Dixon, W.G. The safety of biologic therapies in RA-associated interstitial lung disease. Nat. Rev. Rheumatol. 2014, 10, 284–294. [Google Scholar] [CrossRef]
- Bes, C. Comprehensive review of current diagnostic and treatment approaches to interstitial lung disease associated with rheumatoid arthritis. Eur. J. Rheumatol. 2018, 6, 146–149. [Google Scholar] [CrossRef]
- Paulin, F.; Babini, A.; Mamani, M.; Mercado, J.; Caro, F. Practical Approach to the Evaluation and Management of Rheumatoid Arthritis-Interstitial Lung Disease Based on its Proven and Hypothetical Mechanisms. Rev. Investig. Clin. 2017, 69, 235–242. [Google Scholar] [CrossRef]
- Morisset, J.; Lee, J.S. New trajectories in the treatment of interstitial lung disease: Treat the disease or treat the underlying pattern? Curr. Opin. Pulm. Med. 2019, 25, 442–449. [Google Scholar] [CrossRef]
- Smolen, J.S.; Landewé, R.; Bijlsma, J.; Burmester, G.; Chatzidionysiou, K.; Dougados, M.; Nam, J.; Ramiro, S.; Voshaar, M.; Van Vollenhoven, R.; et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2016 update. Ann. Rheum. Dis. 2017, 76, 960–977. [Google Scholar] [CrossRef]
- Blair, H.A.; Deeks, E.D. Abatacept: A Review in Rheumatoid Arthritis. Drugs 2017, 77, 1221–1233. [Google Scholar] [CrossRef]
- Boleto, G.; Guignabert, C.; Pezet, S.; Cauvet, A.; Sadoine, J.; Tu, L.; Nicco, C.; Gobeaux, C.; Batteux, F.; Allanore, Y.; et al. T-cell costimulation blockade is effective in experimental digestive and lung tissue fibrosis. Arthritis Res. Ther. 2018, 20, 197. [Google Scholar] [CrossRef]
- Jiménez-Alvarez, L.; Arreola, J.L.; Ramírez-Martínez, G.; Ortiz-Quintero, B.; Gaxiola, M.; Reynoso-Robles, R.; Avila-Moreno, F.; Urrea, F.; Pardo, A.; Selman, M.; et al. The effect of CTLA-4Ig, a CD28/B7 antagonist, on the lung inflammation and T cell subset profile during murine hypersensitivity pneumonitis. Exp. Mol. Pathol. 2011, 91, 718–722. [Google Scholar] [CrossRef]
- Mera-Varela, A.; Pérez-Pampín, E. Abatacept therapy in rheumatoid arthritis with interstitial lung disease. J. Clin. Rheumatol. 2014, 20, 445–446. [Google Scholar] [CrossRef]
- Ye, W.; Fifield, M.C.; Östör, A.J. Refractory Rheumatoid Arthritis and Associated Interstitial Lung Disease: Could Abatacept be the Answer? J. Clin. Rheumatol. 2017, 23, 125–126. [Google Scholar] [CrossRef]
- Nakashita, T.; Ando, K.; Takahashi, K.; Motojima, S. Possible effect of abatacept on the progression of interstitial lung disease in rheumatoid arthritis patients. Respir. Investig. 2016, 54, 376–379. [Google Scholar] [CrossRef]
- Curtis, J.R.; Sarsour, K.; Napalkov, P.; Costa, L.A.; Schulman, K.L. Incidence and complications of interstitial lung disease in users of tocilizumab, rituximab, abatacept and anti-tumor necrosis factor α agents, a retrospective cohort study. Arthritis Res. Ther. 2015, 17, 319. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Díaz, C.; Loricera, J.; Castañeda, S.; López-Mejías, R.; Ojeda-García, C.; Olivé, A.; Rodríguez-Muguruza, S.; Carreira, P.E.; Pérez-Sandoval, T.; Retuerto, M.; et al. Abatacept in patients with rheumatoid arthritis and interstitial lung disease: A national multicenter study of 63 patients. Semin. Arthritis Rheum. 2018, 48, 22–27. [Google Scholar] [CrossRef] [Green Version]
- Mochizuki, T.; Ikari, K.; Yano, K.; Sato, M.; Okazaki, K. Long-term deterioration of interstitial lung disease in patients with rheumatoid arthritis treated with abatacept. Mod. Rheumatol. 2018, 29, 413–417. [Google Scholar] [CrossRef]
- Arnett, F.C.; Edworthy, S.M.; Bloch, D.A.; Mcshane, D.J.; Fries, J.F.; Cooper, N.S.; Healey, L.A.; Kaplan, S.R.; Liang, M.H.; Luthra, H.S.; et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988, 31, 315–324. [Google Scholar] [CrossRef]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham III., C.O.; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- Travis, W.D.; Costabel, U.; Hansell, D.M.; King, T.E., Jr.; Lynch, D.A.; Nicholson, A.G.; Ryerson, C.J.; Ryu, J.H.; Selman, M.; Wells, A.U.; et al. ATS/ERS Committee on Idiopathic Interstitial Pneumonias; ATS/ERS Committee on Idiopathic Interstitial Pneumonias. An official American Thoracic Society/European Respiratory Society statement: Update of the international multidisciplinary classification of the idiopathic interstitial pneumonias. Am. J. Respir. Crit. Care Med. 2013, 188, 733–748. [Google Scholar] [CrossRef]
- Walsh, S.L.; Sverzellati, N.; Devaraj, A.; Keir, G.J.; Wells, A.U.; Hansell, D.M. Connective tissue disease related fibrotic lung disease: High resolution computed tomographic and pulmonary function indices as prognostic determinants. Thorax 2014, 69, 216–222. [Google Scholar] [CrossRef] [Green Version]
- Karimi-Shah, B.A.; Chowdhury, B.A. Forced vital capacity in idiopathic pulmonary fibrosis—FDA review of pirfenidone and nintedanib. N. Engl. J. Med. 2015, 372, 1189–1191. [Google Scholar] [CrossRef]
- Altman, D.G. Practical Statistics for Medical Research, 1st ed.; Chapman and Hall: London, UK, 1991. [Google Scholar]
- Wada, T.; Akiyama, Y.; Yokota, K.; Sato, K.; Funakubo, Y.; Mimura, T. A case of rheumatoid arthritis complicated with deteriorated interstitial pneumonia after the administration of abatacept. Nihon Rinsho Meneki Gakkai Kaishi 2012, 35, 433–438. [Google Scholar] [CrossRef] [Green Version]
- Nakashita, T.; Ando, K.; Kaneko, N.; Takahashi, K.; Motojima, S. Potential risk of TNF inhibitors on the progression of interstitial lung disease in patients with rheumatoid arthritis. BMJ Open 2014, 4, e005615. [Google Scholar] [CrossRef]
- Kurata, I.; Tsuboi, H.; Terasaki, M.; Shimizu, M.; Toko, H.; Honda, F.; Ohyama, A.; Yagishita, M.; Osada, A.; Ebe, H.; et al. Effect of Biological Disease-modifying Anti-rheumatic Drugs on Airway and Interstitial Lung Disease in Patients with Rheumatoid Arthritis. Intern. Med. 2019, 15, 1703–1712. [Google Scholar] [CrossRef] [Green Version]
- Clinicaltrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT03084419 (accessed on 30 December 2019).
- Fragoulis, G.; Nikiphorou, E.; Larsen, J.; Korsten, P.; Conway, R. Methotrexate-Associated Pneumonitis and Rheumatoid Arthritis-Interstitial Lung Disease: Current Concepts for the Diagnosis and Treatment. Front. Med. (Lausanne) 2019, 6, 238. [Google Scholar] [CrossRef]
- Kiely, P.; Busby, A.D.; Nikiphorou, E.; Sullivan, K.; Walsh, D.A.; Creamer, P.; Dixey, J.; Young, A. Is incident rheumatoid arthritis interstitial lung disease associated with methotrexate treatment? Results from a multivariate analysis in the ERAS and ERAN inception cohorts. BMJ Open 2019, 9, e028466. [Google Scholar] [CrossRef] [Green Version]
- Sebastiani, M.; Manfredi, A.T.; Cassone, G.; Sandri, G.; Cerri, S.; Ferri, C. Interstitial lung disease is associated to infections of lower respiratory tract in immunocompromised rheumatoid arthritis patients. Clin. Exp. Rheumatol. 2017, 35, 542. [Google Scholar]
- Manfredi, A.; Cassone, G.; Furini, F.; Gremese, E.; Venerito, V.; Atzeni, F.; Arrigoni, E.; Della Casa, G.; Cerri, S.; Govoni, M.; et al. Tocilizumab therapy in rheumatoid arthritis with interstitial lung disease: A multicenter retrospective study. Intern. Med. J. 2019, 29. [Google Scholar] [CrossRef]
- Picchianti Diamanti, A.; Markovic, M.; Argento, G.; Giovagnoli, S.; Ricci, A.; Laganà, B.; D’Amelio, R. Therapeutic management of patients with rheumatoid arthritis and associated interstitial lung disease: Case report and literature review. Ther. Adv Respir. Dis. 2017, 11, 64–72. [Google Scholar] [CrossRef] [Green Version]
- Cohen, S.; Curtis, J.R.; DeMasi, R.; Chen, Y.; Fan, H.; Soonasra, A.; Fleischmann, R. Worldwide, 3-Year, Post-Marketing Surveillance Experience with Tofacitinib in Rheumatoid Arthritis. Rheumatol. Ther. 2018, 5, 283–291. [Google Scholar] [CrossRef] [Green Version]
- Fleischmann, R.; Wollenhaupt, J.; Takiya, L.; Maniccia, A.; Kwok, K.; Wang, L.; van Vollenhoven, R.F. Safety and maintenance of response for tofacitinib monotherapy and combination therapy in rheumatoid arthritis: An analysis of pooled data from open-label long-term extension studies. RMD Open 2017, 3, e000491. [Google Scholar] [CrossRef]
- Manfredi, A.; Cassone, G.; Cerri, S.; Venerito, V.; Fedele, A.L.; Trevisani, M.; Furini, F.; Addimanda, O.; Pancaldi, F.; Della Casa, G.; et al. Diagnostic accuracy of a velcro sound detector (VECTOR) for interstitial lung disease in rheumatoid arthritis patients: The InSPIRAtE validation study (INterStitial pneumonia in rheumatoid ArThritis with an electronic device). BMC Pulm. Med. 2019, 19, 111. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Demographic and Clinical Data | Result |
|---|---|
| Mean age | 65 (11) |
| Female/Male ratio | 2.7/1 |
| Current/Ever smoker | 6 (13.6%)/17 (38.6%) |
| COPD | 8 (18.2%) |
| Disease duration | |
| ILD duration before ABA therapy (months) | 20 (58) |
| Follow-up (months) | 26.5 (38) |
| Rheumatoid factor | 38 (86.4%) |
| ACPA | 40 (90.1%) |
| HRCT pattern | |
| UIP | 19 (43.2%) |
| NSIP | 22 (50%) |
| CPFE | 2 (4.5%) |
| OP | 1 (2.3%) |
| Forced vital capacity (%) | 88.5 (18.5) |
| Diffusion lung CO (%) | 66.4 (34.5) |
| Use of cDMARDs before ABA | 44 (100%) |
| Mehotrexate | 32 (72.3%) |
| Leflunomide | 20 (45.5%) |
| TNFα inhibitors | 19 (43.2%) |
| Tocilizumab | 9 (20.5%) |
| Rituximab | 5 (11.4%) |
| Janus kinases inhibitors | 3 (6.8%) |
| ABA monotherapy | 11 (25%) |
| ABA + methotrexate | 17 (38.6%) |
| Corticosteroids | 33 (75%) |
| Continuous data are reported as median (IQR). |
| HRCT Improved/Stable | HRCT Worsened | p | |
|---|---|---|---|
| 36 | 8 | ||
| Mean age | 64 (10) | 67 (22) | 0.94 |
| Female/Male ratio | 3/1 | 1.7/1 | 0.063 |
| Smoking habit | 7 (19.4%)/16 (44.4%) | 1 (12.5%)/2 (25%) | 0.36/0.63 |
| COPD | 8 (22.2%) | 2 (25%) | 0.55 |
| Disease duration | 120 (149) | 87 (167) | 0.87 |
| ILD duration before ABA therapy (months) | 14 (60) | 26 (44) | 26 (44) |
| Follow-up (months) | 25 (29) | 52 (49) | 0.48 |
| Rheumatoid factor | 31 (86.1%) | 7 (87.5%) | 0.92 |
| ACPA | 40 (90.1%) | 7 (87.5%) | 0.57 |
| HRCT pattern | |||
| UIP | 13 (36.1%) | 6 (75%) | |
| NSIP | 20 (55.5%) | 2 (25%) | 0.24 |
| CPFE | 2 (5.6%) | – | |
| OP | 1 (2.8%) | – | |
| Forced vital capacity (%) | 88 (17) | 93 (22) | 0.46 |
| Diffusion lung CO (%) | 61 (34) | 81 (22) | 0.14 |
| Use of cDMARDs before TCZ | 36 (100%) | 8 (100%) | |
| Mehotrexate | 26 (72.2%) | 6 (75%) | 0.87 |
| Leflunomide | 17 (47.2%) | 3 (37.5%) | 0.71 |
| TNFi | 16 (44.4%) | 3 (37.5%) | 0.72 |
| Tocilizumab | 8 (22.2%) | 1 (12.5%) | 0.54 |
| Rituximab | 3 (8.3%) | 2 (25%) | 0.22 |
| Janus kinases inhibitors | 2 (5.6%) | 1 (12.5%) | 0.46 |
| ABA monotherapy | 9 (25%) | 2 (25%) | 1 |
| ABA + methotrexate | 13 (36.1%) | 4 (50%) | 0.69 |
| Corticosteroids | 29 (80.6%) | 4 (50%) | 0.09 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cassone, G.; Manfredi, A.; Atzeni, F.; Venerito, V.; Vacchi, C.; Picerno, V.; Furini, F.; Erre, G.L.; Tomietto, P.; Fedele, A.L.; et al. Safety of Abatacept in Italian Patients with Rheumatoid Arthritis and Interstitial Lung Disease: A Multicenter Retrospective Study. J. Clin. Med. 2020, 9, 277. https://doi.org/10.3390/jcm9010277
Cassone G, Manfredi A, Atzeni F, Venerito V, Vacchi C, Picerno V, Furini F, Erre GL, Tomietto P, Fedele AL, et al. Safety of Abatacept in Italian Patients with Rheumatoid Arthritis and Interstitial Lung Disease: A Multicenter Retrospective Study. Journal of Clinical Medicine. 2020; 9(1):277. https://doi.org/10.3390/jcm9010277
Chicago/Turabian StyleCassone, Giulia, Andreina Manfredi, Fabiola Atzeni, Vincenzo Venerito, Caterina Vacchi, Valentina Picerno, Federica Furini, Gian Luca Erre, Paola Tomietto, Anna Laura Fedele, and et al. 2020. "Safety of Abatacept in Italian Patients with Rheumatoid Arthritis and Interstitial Lung Disease: A Multicenter Retrospective Study" Journal of Clinical Medicine 9, no. 1: 277. https://doi.org/10.3390/jcm9010277
APA StyleCassone, G., Manfredi, A., Atzeni, F., Venerito, V., Vacchi, C., Picerno, V., Furini, F., Erre, G. L., Tomietto, P., Fedele, A. L., Della Casa, G., Nucera, V., Giannitti, C., Salvarani, C., & Sebastiani, M. (2020). Safety of Abatacept in Italian Patients with Rheumatoid Arthritis and Interstitial Lung Disease: A Multicenter Retrospective Study. Journal of Clinical Medicine, 9(1), 277. https://doi.org/10.3390/jcm9010277