Clinical Factors Associated with Adherence to the Follow-Up Examination after Positive Fecal Occult Blood Test in National Colorectal Cancer Screening

 , , and
, , and
Abstract
1. Introduction
2. Materials and Methods
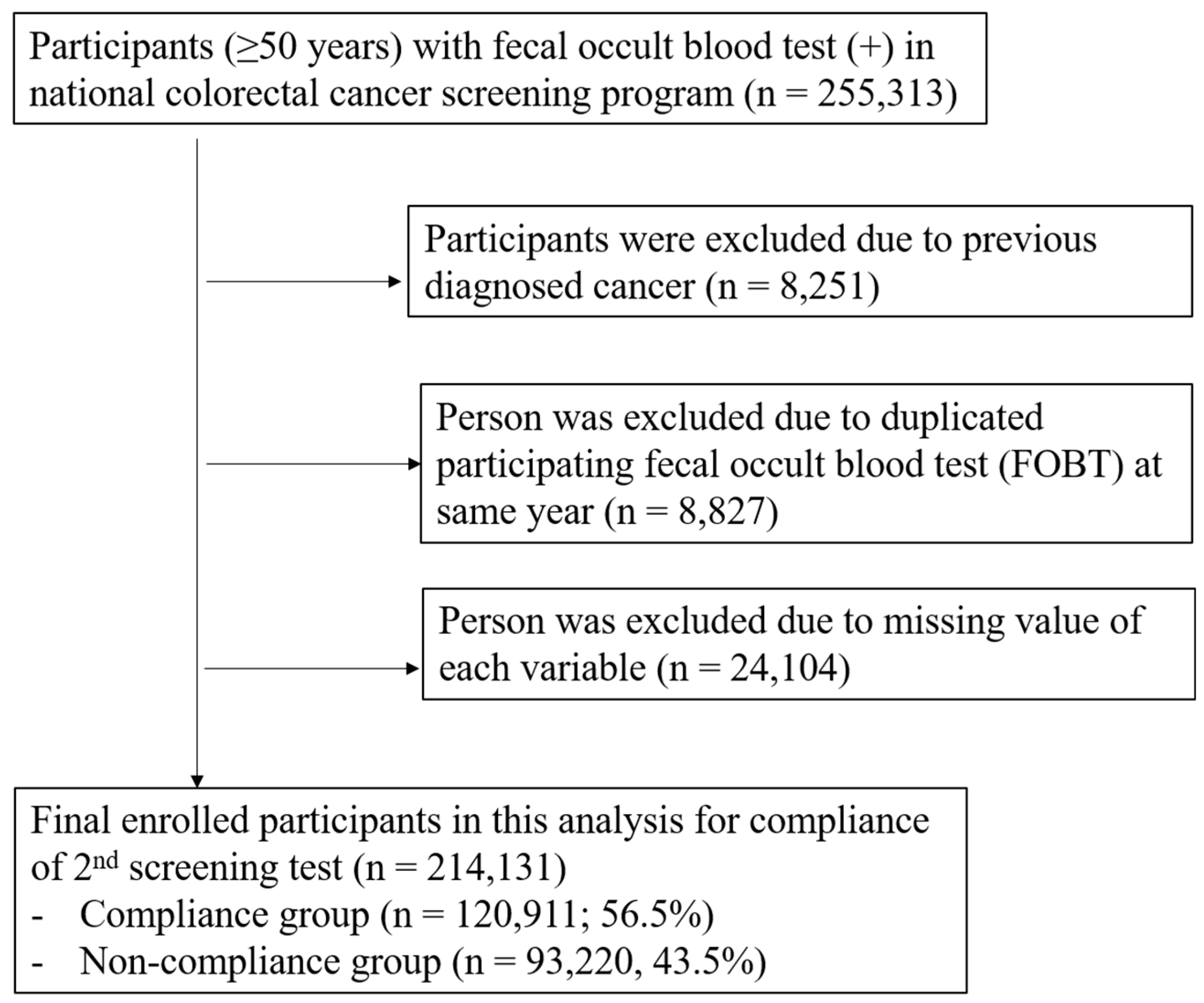
2.1. Data Source and Study Cohort
2.2. Definition
2.3. Statistical Analysis
3. Results
3.1. Demographic and Clinical Factors
3.2. Odds Ratio of Compliance Factors for the Follow-Up Test after a Positive FOBT
3.3. Factors Associated with Adherence to the Follow-Up Test after a Positive FOBT According to Age
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in globocan 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef]
- Jung, K.W.; Won, Y.J.; Oh, C.M.; Kong, H.J.; Lee, D.H.; Lee, K.H. Cancer statistics in korea: Incidence, mortality, survival, and prevalence in 2014. Cancer Res. Treat. 2017, 49, 292–305. [Google Scholar] [CrossRef] [PubMed]
- Mandel, J.S.; Bond, J.H.; Church, T.R.; Snover, D.C.; Bradley, G.M.; Schuman, L.M.; Ederer, F. Reducing mortality from colorectal cancer by screening for fecal occult blood. Minnesota colon cancer control study. N. Engl. J. Med. 1993, 328, 1365–1371. [Google Scholar] [CrossRef] [PubMed]
- Mandel, J.S.; Church, T.R.; Bond, J.H.; Ederer, F.; Geisser, M.S.; Mongin, S.J.; Snover, D.C.; Schuman, L.M. The effect of fecal occult-blood screening on the incidence of colorectal cancer. N. Engl. J. Med. 2000, 343, 1603–1607. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.A.; Cokkinides, V.; Brooks, D.; Saslow, D.; Brawley, O.W. Cancer screening in the united states, 2010: A review of current american cancer society guidelines and issues in cancer screening. CA Cancer J. Clin. 2010, 60, 99–119. [Google Scholar] [CrossRef] [PubMed]
- Sohn, D.K.; Kim, M.J.; Park, Y.; Suh, M.; Shin, A.; Lee, H.Y.; Im, J.P.; Cho, H.-M.; Hong, S.P.; Kim, B.-H. The korean guideline for colorectal cancer screening. J. Korean Med. Assoc. 2015, 58, 420–432. [Google Scholar] [CrossRef]
- Sung, J.J.; Lau, J.Y.; Young, G.P.; Sano, Y.; Chiu, H.M.; Byeon, J.S.; Yeoh, K.G.; Goh, K.L.; Sollano, J.; Rerknimitr, R.; et al. Asia pacific consensus recommendations for colorectal cancer screening. Gut 2008, 57, 1166–1176. [Google Scholar] [CrossRef]
- Choi, K.S.; Lee, H.Y.; Jun, J.K.; Shin, A.; Park, E.C. Adherence to follow-up after a positive fecal occult blood test in an organized colorectal cancer screening program in korea, 2004–2008. J. Gastroenterol. Hepatol. 2012, 27, 1070–1077. [Google Scholar] [CrossRef]
- Towler, B.P.; Irwig, L.; Glasziou, P.; Weller, D.; Kewenter, J. Screening for colorectal cancer using the faecal occult blood test, hemoccult. Cochrane Database Syst. Rev. 2000. [Google Scholar] [CrossRef]
- Winawer, S.J. Screening sigmoidoscopy: Can the road to colonoscopy be less traveled? Ann. Intern. Med. 2003, 139, 1034–1035. [Google Scholar] [CrossRef]
- Seeff, L.C.; Nadel, M.R.; Klabunde, C.N.; Thompson, T.; Shapiro, J.A.; Vernon, S.W.; Coates, R.J. Patterns and predictors of colorectal cancer test use in the adult u.S. Population. Cancer 2004, 100, 2093–2103. [Google Scholar] [CrossRef] [PubMed]
- Meissner, H.I.; Breen, N.; Klabunde, C.N.; Vernon, S.W. Patterns of colorectal cancer screening uptake among men and women in the united states. Cancer Epidemiol. Prev. Biomark. 2006, 15, 389–394. [Google Scholar] [CrossRef] [PubMed]
- Ioannou, G.N.; Chapko, M.K.; Dominitz, J.A. Predictors of colorectal cancer screening participation in the united states. Am. J. Gastroenterol. 2003, 98, 2082–2091. [Google Scholar] [CrossRef] [PubMed]
- Suh, M.; Song, S.; Cho, H.N.; Park, B.; Jun, J.K.; Choi, E.; Kim, Y.; Choi, K.S. Trends in participation rates for the national cancer screening program in korea, 2002–2012. Cancer Res. Treat. 2017, 49, 798–806. [Google Scholar] [CrossRef]
- Myong, J.P.; Shin, J.Y.; Kim, S.J. Factors associated with participation in colorectal cancer screening in korea: The fourth korean national health and nutrition examination survey (knhanes iv). Int. J. Colorectal. Dis. 2012, 27, 1061–1069. [Google Scholar] [CrossRef]
- Turner, B.; Myers, R.E.; Hyslop, T.; Hauck, W.W.; Weinberg, D.; Brigham, T.; Grana, J.; Rothermel, T.; Schlackman, N. Physician and patient factors associated with ordering a colon evaluation after a positive fecal occult blood test. J. Gen. Intern. Med. 2003, 18, 357–363. [Google Scholar] [CrossRef]
- Miglioretti, D.L.; Rutter, C.M.; Bradford, S.C.; Zauber, A.G.; Kessler, L.G.; Feuer, E.J.; Grossman, D.C. Improvement in the diagnostic evaluation of a positive fecal occult blood test in an integrated health care organization. Med. Care 2008, 46, S91–S96. [Google Scholar] [CrossRef]
- Goulard, H.; Boussac-Zarebska, M.; Ancelle-Park, R.; Bloch, J. French colorectal cancer screening pilot programme: Results of the first round. J. Med. Screen. 2008, 15, 143–148. [Google Scholar] [CrossRef]
- Fisher, D.A.; Jeffreys, A.; Coffman, C.J.; Fasanella, K. Barriers to full colon evaluation for a positive fecal occult blood test. Cancer Epidemiol. Prev. Biomark. 2006, 15, 1232–1235. [Google Scholar] [CrossRef]
- Etzioni, D.A.; Yano, E.M.; Rubenstein, L.V.; Lee, M.L.; Ko, C.Y.; Brook, R.H.; Parkerton, P.H.; Asch, S.M. Measuring the quality of colorectal cancer screening: The importance of follow-up. Dis. Colon Rectum 2006, 49, 1002–1010. [Google Scholar] [CrossRef]
- Carlson, C.M.; Kirby, K.A.; Casadei, M.A.; Partin, M.R.; Kistler, C.E.; Walter, L.C. Lack of follow-up after fecal occult blood testing in older adults: Inappropriate screening or failure to follow up? Arch. Intern. Med. 2011, 171, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Larsen, M.B.; Mikkelsen, E.M.; Rasmussen, M.; Friis-Hansen, L.; Ovesen, A.U.; Rahr, H.B.; Andersen, B. Sociodemographic characteristics of nonparticipants in the danish colorectal cancer screening program: A nationwide cross-sectional study. Clin. Epidemiol. 2017, 9, 345–354. [Google Scholar] [CrossRef] [PubMed]
- Correia, A.; Rabeneck, L.; Baxter, N.N.; Paszat, L.F.; Sutradhar, R.; Yun, L.; Tinmouth, J. Lack of follow-up colonoscopy after positive fobt in an organized colorectal cancer screening program is associated with modifiable health care practices. Prev. Med. 2015, 76, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.W.; Park, E.C.; Chun, S.Y.; Han, K.T.; Han, E.; Kim, T.H. Health care utilization and costs among medical-aid enrollees, the poor not enrolled in medical-aid, and the near poor in south korea. Int. J. Equity Health 2015, 14, 128. [Google Scholar] [CrossRef]
- Sewitch, M.J.; Fournier, C.; Ciampi, A.; Dyachenko, A. Adherence to colorectal cancer screening guidelines in canada. BMC Gastroenterol. 2007, 7, 39. [Google Scholar] [CrossRef]
- Hassan, C.; Kaminski, M.F.; Repici, A. How to ensure patient adherence to colorectal cancer screening and surveillance in your practice. Gastroenterology 2018, 155, 252–257. [Google Scholar] [CrossRef]
- Baig, N.; Myers, R.E.; Turner, B.J.; Grana, J.; Rothermel, T.; Schlackman, N.; Weinberg, D.S. Physician-reported reasons for limited follow-up of patients with a positive fecal occult blood test screening result. Am. J. Gastroenterol. 2003, 98, 2078–2081. [Google Scholar] [CrossRef]


{kind=link}
| Total N = 214,131 | Non-Compliance Group N = 93,220 | Compliance Group N = 120,911 | p-Value | |||
|---|---|---|---|---|---|---|
| N | N | (%) | N | (%) | ||
| Sex | ||||||
| Men | 112,465 | 48,261 | (42.9) | 64,204 | (57.1) | <0.0001 |
| Women | 101,666 | 44,959 | (44.2) | 56,707 | (55.8) | |
| Age, years | ||||||
| 50–59 | 86,466 | 34,628 | (40.0) | 51,838 | (60.0) | <0.0001 |
| 60–69 | 72,177 | 29,281 | (40.6) | 42,896 | (59.4) | |
| 70–79 | 46,942 | 23,427 | (49.9) | 23,515 | (50.1) | |
| ≥80 | 8546 | 5884 | (68.9) | 2662 | (31.1) | |
| Previous experience of colonoscopy or DCBE within 5 years | ||||||
| Yes | 194,788 | 88,064 | (45.2) | 106,724 | (54.8) | <0.0001 |
| No | 19,343 | 5156 | (26.7) | 14,187 | (73.3) | |
| Previous experience of a FOBT within 1 year | ||||||
| Negative | 179,623 | 80,664 | (49.2) | 98,959 | (50.8) | <0.0001 |
| Positive | 24,441 | 10,226 | (41.8) | 14,215 | (58.2) | |
| No experience | 10,067 | 2330 | (23.1) | 7737 | (76.9) | |
| History of medical facility use (within 6 months before and after a FOBT) | ||||||
| General Hospital | 33,894 | 13,913 | (41.0) | 19,981 | (59.0) | <0.0001 |
| Hospital | 41,493 | 16,017 | (38.6) | 25,476 | (61.4) | |
| Clinic | 133,023 | 59,980 | (45.1) | 73,043 | (54.9) | |
| Others * | 5721 | 3310 | (57.9) | 2411 | (42.1) | |
| Type of Health Insurance ** | ||||||
| NHI (local) | 63,692 | 26,897 | (42.2) | 36,795 | (57.8) | <0.0001 |
| NHI (company) | 144,277 | 63,262 | (43.8) | 81,015 | (56.2) | |
| MAP | 6162 | 3061 | (49.7) | 3101 | (50.3) | |
| Residence area | ||||||
| Urban area *** | 86,293 | 37,449 | (43.4) | 48,844 | (56.6) | 0.2949 |
| Rural area † | 127,838 | 55,771 | (43.6) | 72,067 | (56.4) | |
| Health insurance premium level (based on the quartile) ‡ | ||||||
| Quartile 25% | 50,761 | 23,504 | (46.3) | 27,257 | (53.7) | <0.0001 |
| Quartile 50% | 46,357 | 20,570 | (44.4) | 25,787 | (55.6) | |
| Quartile 75% | 49,381 | 20,669 | (41.9) | 28,712 | (58.1) | |
| Quartile 100% | 67,632 | 28,477 | (42.1) | 39,155 | (57.9) | |
| Types of medical facility that performed a FOBT | ||||||
| General Hospital | 47,236 | 19,988 | (42.3) | 27,248 | (57.7) | <0.0001 |
| Hospital | 67,078 | 29,393 | (43.8) | 37,685 | (56.2) | |
| Clinic | 99,643 | 43,737 | (43.9) | 55,906 | (56.1) | |
| Others * | 174 | 102 | (58.6) | 72 | (41.4) | |
| CCI | ||||||
| 0 | 79,457 | 35,318 | (44.4) | 44,139 | (55.6) | <0.0001 |
| 1 | 65,016 | 28,220 | (43.4) | 36,796 | (56.6) | |
| 2 | 39,895 | 16,868 | (42.3) | 23,027 | (57.7) | |
| 3 | 29,763 | 12,814 | (43.1) | 16,949 | (56.9) | |
| Anemia | ||||||
| Absent | 186,172 | 80,997 | (43.5) | 105,175 | (56.5) | 0.5069 |
| Present | 27,959 | 12,223 | (43.7) | 15,736 | (56.3) | |
| Hemorrhagic and hematologic diseases | ||||||
| Absent | 210,124 | 91,414 | (43.5) | 118,710 | (56.5) | 0.0476 |
| Present | 4007 | 1806 | (45.1) | 2201 | (54.9) | |
| Osteoporosis | ||||||
| Absent | 172,796 | 74,847 | (43.3) | 97,949 | (56.7) | <0.0001 |
| Present | 41,335 | 18,373 | (44.4) | 22,962 | (55.6) | |
| Depression | ||||||
| Absent | 181,782 | 79,538 | (43.8) | 102,244 | (56.2) | <0.0001 |
| Present | 32,349 | 13,682 | (42.3) | 18,667 | (57.7) | |
| BMI (kg/m2) | ||||||
| <25 | 134,107 | 58,972 | (44.0) | 75,135 | (56.0) | <0.0001 |
| ≥25 | 80,024 | 34,248 | (42.8) | 45,776 | (57.2) | |
| Alcohol intake | ||||||
| Absent | 134,894 | 59,517 | (44.1) | 75,377 | (55.9) | <0.0001 |
| Present | 79,237 | 33,703 | (42.5) | 45,534 | (57.5) | |
| Smoking | ||||||
| Absent | 136,636 | 59,438 | (43.5) | 77,198 | (56.5) | 0.6815 |
| Present | 77,495 | 33,782 | (43.6) | 43,713 | (56.4) | |
| Physical activity | ||||||
| <3 times/week | 79,729 | 36,675 | (46.0) | 43,054 | (54.0) | <0.0001 |
| ≥3 times/week | 134,402 | 56,545 | (42.1) | 77,857 | (57.9) | |
| Variables | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| OR | (95% CI) | p-Value | OR | (95% CI) | p-Value | |
| Gender | ||||||
| Men | 1.06 | (1.04–1.07) | <0.0001 | 1.12 | (1.09–1.15) | <0.0001 |
| Women | 1.00 | 1.00 | ||||
| Age | ||||||
| 50–59 years | 3.31 | (3.15–3.47) | <0.0001 | 3.57 | (3.39–3.75) | <0.0001 |
| 60–69 years | 3.24 | (3.09–3.40) | <0.0001 | 3.29 | (3.13–3.46) | <0.0001 |
| 70–79 years | 2.22 | (2.11–2.33) | <0.0001 | 2.19 | (2.09–2.31) | <0.0001 |
| ≥80 years | 1.00 | 1.00 | ||||
| Previous experience of colonoscopy or DCBE within 5 years | ||||||
| Yes | 1.00 | 1.00 | ||||
| No | 2.27 | (2.20–2.35) | <0.0001 | 2.06 | (1.99–2.13) | <0.0001 |
| Previous experience of a FOBT within 1 year | ||||||
| Negative | 1.13 | (1.10–1.16) | <0.0001 | 1.18 | (1.15–1.21) | <0.0001 |
| Positive | 2.71 | (2.58–2.84) | <0.0001 | 2.42 | (2.31–2.54) | <0.0001 |
| No experience | 1.00 | 1.00 | ||||
| History of medical facility used (within 6 months before and after a FOBT) | ||||||
| Clinic | 1.00 | 1.00 | ||||
| General Hospital | 1.18 | (1.15–1.21) | <0.0001 | 1.14 | (1.11–1.17) | <0.0001 |
| Hospital | 1.31 | (1.28–1.34) | <0.0001 | 1.46 | (1.42–1.50) | <0.0001 |
| Others * | 0.60 | (0.57–0.63) | <0.0001 | 0.71 | (0.67–0.75) | <0.0001 |
| Type of Health Insurance ** | ||||||
| MAP | 1.00 | 1.00 | ||||
| NHI (company) | 1.26 | (1.20–1.33) | <0.0001 | 1.38 | (1.31–1.46) | <0.0001 |
| NHI (local) | 1.35 | (1.28–1.42) | <0.0001 | 1.44 | (1.36–1.53) | <0.0001 |
| Residence area | ||||||
| Rural area *** | 1.00 | 1.00 | ||||
| Urban area † | 1.01 | (0.99–1.03) | 0.29 | 1.00 | (0.98–1.02) | 0.82 |
| Health insurance premium level (based on the quartile) ‡ | ||||||
| Quartile 25% | 1.00 | 1.00 | ||||
| Quartile 50% | 1.08 | (1.05–1.11) | <0.0001 | 1.02 | (0.99–1.04) | 0.29 |
| Quartile 75% | 1.20 | (1.17–1.23) | <0.0001 | 1.14 | (1.11–1.17) | <0.0001 |
| Quartile 100% | 1.19 | (1.16–1.21) | <0.0001 | 1.22 | (1.19–1.25) | <0.0001 |
| Types of medical facility that performed a FOBT | ||||||
| Clinic | 1.00 | 1.00 | ||||
| General Hospital | 1.07 | (1.04–1.09) | <0.0001 | 1.02 | (0.99–1.04) | 0.21 |
| Hospital | 1.00 | (0.98–1.02) | 0.76 | 0.82 | (0.80–0.84) | <0.0001 |
| Others * | 0.55 | (0.41–0.75) | 0.0001 | 0.72 | (0.53–0.98) | 0.04 |
| CCI | ||||||
| 0 | 1.00 | 1.00 | ||||
| 1 | 1.04 | (1.02–1.07) | <0.0001 | 1.08 | (1.06–1.11) | <0.0001 |
| 2 | 1.09 | (1.07–1.12) | <0.0001 | 1.16 | (1.13–1.19) | <0.0001 |
| 3 | 1.06 | (1.03–1.09) | <0.0001 | 1.16 | (1.12–1.19) | <0.0001 |
| Anemia | ||||||
| Absent | 1.00 | 1.00 | ||||
| Present | 0.99 | (0.97–1.02) | 0.51 | 1.00 | (0.98–1.03) | 0.75 |
| Hemorrhagic and hematologic diseases | ||||||
| Absent | 1.00 | 1.00 | ||||
| Present | 0.94 | (0.88–1.00) | 0.05 | 0.93 | (0.87–0.99) | 0.03 |
| Osteoporosis | ||||||
| Absent | 1.00 | 1.00 | ||||
| Present | 0.96 | (0.94–0.98) | <0.0001 | 1.09 | (1.06–1.11) | <0.0001 |
| Depression | ||||||
| Absent | 1.00 | 1.00 | ||||
| Present | 1.06 | (1.04–1.09) | <0.0001 | 1.11 | (1.08–1.14) | <0.0001 |
| BMI (kg/m2) | ||||||
| <25 | 1.00 | 1.00 | ||||
| ≥25 | 1.05 | (1.03–1.07) | <0.0001 | 1.01 | (0.99–1.03) | 0.45 |
| Alcohol intake | ||||||
| Absent | 1.00 | 1.00 | ||||
| Present | 1.07 | (1.05–1.09) | <0.0001 | 1.03 | (1.01–1.05) | 0.01 |
| Smoking | ||||||
| Absent | 1.00 | 1.00 | ||||
| Present | 1.00 | (0.98–1.01) | 0.68 | 1.12 | (1.09–1.15) | <0.0001 |
| Physical activity | ||||||
| <3 times/week | 1.00 | 1.00 | ||||
| ≥3 times/week | 1.17 | (1.15–1.19) | <0.0001 | 1.13 | (1.11–1.15) | <0.0001 |
| Variables | <65 Years Old | ≥65 Years Old | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | |||||||||
| OR | (95% CI) | p-Value | OR | (95% CI) | p-Value | OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Gender | ||||||||||||
| Men | 0.96 | (0.94–0.98) | 0.0003 | 1.04 | (1.01–1.07) | <0.0001 | 1.21 | (1.18–1.24) | <0.0001 | 1.20 | (1.15–1.24) | <0.0001 |
| Women | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Previous experience of colonoscopy or DCBE within 5 years | ||||||||||||
| Yes | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| No | 2.18 | (2.09–2.28) | <0.0001 | 1.98 | (1.89–2.07) | 0.02 | 2.45 | (2.33–2.57) | <0.0001 | 2.26 | (2.15–2.37) | <0.0001 |
| Previous experience of a FOBT within 1 year | ||||||||||||
| Negative | 1.07 | (1.03–1.11) | 0.0005 | 1.10 | (1.06–1.14) | <0.0001 | 1.27 | (1.22–1.33) | <0.0001 | 1.28 | (1.23–1.34) | <0.0001 |
| Positive | 3.22 | (3.02–3.44) | <0.0001 | 2.97 | (2.78–3.18) | <0.0001 | 2.18 | (2.03–2.34) | <0.0001 | 1.85 | (1.72–1.99) | <0.0001 |
| No experience | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| History of medical facility used (within 6 months before and after a FOBT) | ||||||||||||
| Clinic | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| General Hospital | 1.17 | (1.13–1.20) | <0.0001 | 1.17 | (1.13–1.21) | <0.0001 | 1.18 | (1.14–1.23) | <0.0001 | 1.11 | (1.06–1.16) | <0.0001 |
| Hospital | 1.32 | (1.28–1.36) | <0.0001 | 1.47 | (1.41–1.52) | <0.0001 | 1.20 | (1.15–1.24) | <0.0001 | 1.44 | (1.18–1.51) | <0.0001 |
| Others * | 0.67 | (0.61–0.73) | <0.0001 | 0.70 | (0.63–0.76) | <0.0001 | 0.63 | (0.59–0.68) | <0.0001 | 0.68 | (0.63–0.73) | <0.0001 |
| Type of Health Insurance ** | ||||||||||||
| MAP | 1.00 | 1.00 | 1.00 | |||||||||
| NHI (company) | 1.49 | (1.40–1.58) | <0.0001 | 1.48 | (1.39–1.58) | <0.0001 | 0.98 | (0.89–1.09) | 0.73 | 0.92 | (0.83–1.02) | 0.24 |
| NHI (local) | 1.63 | (1.53–1.73) | <0.0001 | 1.57 | (1.46–1.67) | <0.0001 | 0.98 | (0.89–1.09) | 0.73 | 0.94 | (0.84–1.04) | 0.12 |
| Residence area | ||||||||||||
| Rural area *** | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Urban area † | 0.96 | (0.94–0.98) | 0.0002 | 0.97 | (0.95–0.99) | 0.01 | 1.07 | (1.04–1.09) | <0.0001 | 1.05 | (1.02–1.08) | 0.001 |
| Health insurance premium level (based on the quartile) ‡ | ||||||||||||
| Quartile 25% | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Quartile 50% | 1.05 | (1.02–1.09) | 0.002 | 1.01 | (0.98–1.05) | 0.48 | 1.06 | (1.02–1.11) | 0.004 | 1.05 | (1.00–1.09) | 0.04 |
| Quartile 75% | 1.21 | (1.17–1.25) | <0.0001 | 1.15 | (1.11–1.19) | <0.0001 | 1.14 | (1.09–1.18) | <0.0001 | 1.14 | (1.09–1.18) | <0.0001 |
| Quartile 100% | 1.29 | (1.25–1.33) | <0.0001 | 1.22 | (1.17–1.26) | <0.0001 | 1.17 | (1.13–1.21) | <0.0001 | 1.17 | (1.13–1.22) | <0.0001 |
| Types of medical facility that performed a FOBT | ||||||||||||
| Clinic | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| General Hospital | 1.03 | (1.00–1.06) | 0.03 | 0.97 | (0.94–1.00) | 0.07 | 1.11 | (1.07–1.15) | <0.0001 | 1.09 | (1.05–1.13) | <0.0001 |
| Hospital | 1.06 | (1.03–1.09) | <0.0001 | 0.86 | (0.84–0.89) | <0.0001 | 0.90 | (0.87–0.93) | <0.0001 | 0.77 | (0.74–0.80) | <0.0001 |
| Others * | 0.52 | (0.33–0.81) | 0.004 | 0.60 | (0.38–0.94) | 0.03 | 0.62 | (0.41–0.94) | 0.02 | 0.85 | (0.56–1.29) | 0.45 |
| CCI | ||||||||||||
| 0 | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| 1 | 1.11 | (1.08–1.14) | <0.0001 | 1.10 | (1.07–1.13) | <0.0001 | 1.05 | (1.01–1.08) | 0.01 | 1.03 | (1.00–1.07) | 0.07 |
| 2 | 1.19 | (1.15–1.22) | <0.0001 | 1.17 | (1.13–1.21) | <0.0001 | 1.13 | (1.09–1.18) | <0.0001 | 1.10 | (1.06–1.15) | <0.0001 |
| 3 | 1.17 | (1.12–1.22) | <0.0001 | 1.14 | (1.10–1.19) | <0.0001 | 1.15 | (1.10–1.19) | <0.0001 | 1.10 | (1.05–1.14) | <0.0001 |
| Anemia | ||||||||||||
| Absent | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Present | 1.07 | (1.03–1.11) | 0.0003 | 1.02 | (0.98–1.06) | 0.31 | 0.99 | (0.95–1.02) | 0.45 | 0.96 | (0.93–1.00) | 0.06 |
| Hemorrhagic and Hematologic diseases | ||||||||||||
| Absent | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Present | 0.96 | (0.88–1.06) | 0.43 | 0.91 | (0.83–1.00) | 0.04 | 0.99 | (0.90–1.08) | 0.73 | 0.94 | (0.86–1.03) | 0.1536 |
| Osteoporosis | ||||||||||||
| Absent | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Present | 1.17 | (1.13–1.21) | <0.0001 | 1.12 | (1.07–1.16) | <0.0001 | 0.98 | (0.95–1.01) | 0.19 | 1.07 | (1.04–1.11) | <0.0001 |
| Depression | ||||||||||||
| Absent | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Present | 1.11 | (1.07–1.15) | <0.0001 | 1.08 | (1.04–1.12) | <0.0001 | 1.11 | (1.07–1.15) | <0.0001 | 1.11 | (1.07–1.15) | <0.0001 |
| BMI (kg/m2) | ||||||||||||
| <25 | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| ≥25 | 1.01 | (0.99–1.04) | 0.30 | 0.99 | (0.97–1.02) | 0.63 | 1.09 | (1.06–1.12) | <0.0001 | 1.09 | (1.06–1.13) | <0.0001 |
| Alcohol intake | ||||||||||||
| Absent | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Present | 1.06 | (1.04–1.09) | <0.0001 | 1.03 | (1.00–1.06) | 0.02 | 0.88 | (0.86–0.91) | <.0001 | 0.96 | (0.93–0.99) | 0.01 |
| Smoking | ||||||||||||
| Absent | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| Present | 1.11 | (1.09–1.14) | <0.0001 | 1.12 | (1.09–1.16) | <0.0001 | 0.92 | (0.89–0.95) | <0.0001 | 1.05 | (1.02–1.09) | 0.004 |
| Physical activity | ||||||||||||
| <3 times/week | 1.00 | 1.00 | 1.00 | 1.00 | ||||||||
| ≥3 times/week | 1.08 | (1.06–1.11) | <0.0001 | 1.09 | (1.06–1.11) | <0.0001 | 1.29 | (1.26–1.33) | <0.0001 | 1.25 | (1.22–1.29) | <0.0001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, B.C.; Kang, M.; Park, E.; Shim, J.-I.; Kang, S.; Lee, J.; Tchoe, H.J.; Kong, K.A.; Kim, D.H.; Kim, Y.J.; et al. Clinical Factors Associated with Adherence to the Follow-Up Examination after Positive Fecal Occult Blood Test in National Colorectal Cancer Screening. J. Clin. Med. 2020, 9, 260. https://doi.org/10.3390/jcm9010260
Kim BC, Kang M, Park E, Shim J-I, Kang S, Lee J, Tchoe HJ, Kong KA, Kim DH, Kim YJ, et al. Clinical Factors Associated with Adherence to the Follow-Up Examination after Positive Fecal Occult Blood Test in National Colorectal Cancer Screening. Journal of Clinical Medicine. 2020; 9(1):260. https://doi.org/10.3390/jcm9010260
Chicago/Turabian StyleKim, Byung Chang, Minjoo Kang, Eunjung Park, Jeong-Im Shim, Shinhee Kang, Jessie Lee, Ha Jin Tchoe, Kyeong Ae Kong, Duk Hwan Kim, Yu Jin Kim, and et al. 2020. "Clinical Factors Associated with Adherence to the Follow-Up Examination after Positive Fecal Occult Blood Test in National Colorectal Cancer Screening" Journal of Clinical Medicine 9, no. 1: 260. https://doi.org/10.3390/jcm9010260
APA StyleKim, B. C., Kang, M., Park, E., Shim, J.-I., Kang, S., Lee, J., Tchoe, H. J., Kong, K. A., Kim, D. H., Kim, Y. J., Choi, K. S., & Moon, C. M. (2020). Clinical Factors Associated with Adherence to the Follow-Up Examination after Positive Fecal Occult Blood Test in National Colorectal Cancer Screening. Journal of Clinical Medicine, 9(1), 260. https://doi.org/10.3390/jcm9010260