Outcome of Femoral Varus Derotational Osteotomy for the Spastic Hip Displacement: Implication for the Indication of Concomitant Pelvic Osteotomy

 , , , ,
, , , ,
Abstract
1. Introduction
2. Experimental Section
2.1. Subjects
2.2. Surgical Procedures
2.3. Outcome Assessment
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Shore, B.J.; Graham, H.K. Management of moderate to severe hip displacement in nonambulatory children with cerebral palsy. JBJS Rev. 2017, 5, e4. [Google Scholar] [CrossRef]
- Soo, B.; Howard, J.J.; Boyd, R.N.; Reid, S.M.; Lanigan, A.; Wolfe, R.; Reddihough, D.; Graham, H.K. Hip displacement in cerebral palsy. J. Bone Jt. Surg. Am. 2006, 88, 121–129. [Google Scholar]
- Flynn, J.M.; Miller, F. Management of hip disorders in patients with cerebral palsy. J. Am. Acad. Orthop. Surg. 2002, 10, 198–209. [Google Scholar] [CrossRef]
- Graham, H.K. Painful hip dislocation in cerebral palsy. Lancet 2002, 359, 907–908. [Google Scholar] [CrossRef]
- Jung, N.H.; Pereira, B.; Nehring, I.; Brix, O.; Bernius, P.; Schroeder, S.A.; Kluger, G.J.; Koehler, T.; Beyerlein, A.; Weir, S.; et al. Does hip displacement influence health-related quality of life in children with cerebral palsy? Dev. Neurorehabil. 2014, 17, 420–425. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.W.; Jeon, H.R.; Shin, J.C.; Youk, T.; Kim, J. Incidence of cerebral palsy in korea and the effect of socioeconomic status: A population-based nationwide study. Yonsei Med. J. 2018, 59, 781–786. [Google Scholar] [CrossRef] [PubMed]
- Shrader, M.W.; Wimberly, L.; Thompson, R. Hip surveillance in children with cerebral palsy. J. Am. Acad. Orthop. Surg. 2019, 27, 760–768. [Google Scholar] [CrossRef]
- Wynter, M.; Gibson, N.; Willoughby, K.L.; Love, S.; Kentish, M.; Thomason, P.; Graham, H.K. Australian hip surveillance guidelines for children with cerebral palsy: 5-year review. Dev. Med. Child Neurol. 2015, 57, 808–820. [Google Scholar] [CrossRef]
- Hagglund, G.; Alriksson-Schmidt, A.; Lauge-Pedersen, H.; Rodby-Bousquet, E.; Wagner, P.; Westbom, L. Prevention of dislocation of the hip in children with cerebral palsy: 20-year results of a population-based prevention programme. Bone Jt. J. 2014, 96, 1546–1552. [Google Scholar] [CrossRef]
- Shore, B.J.; Zurakowski, D.; Dufreny, C.; Powell, D.; Matheney, T.H.; Snyder, B.D. Proximal femoral varus derotation osteotomy in children with cerebral palsy: The effect of age, gross motor function classification system level, and surgeon volume on surgical success. J. Bone Jt. Surg. Am. 2015, 97, 2024–2031. [Google Scholar] [CrossRef]
- Chang, F.M.; May, A.; Faulk, L.W.; Flynn, K.; Miller, N.H.; Rhodes, J.T.; Zhaoxing, P.; Novais, E.N. Outcomes of isolated varus derotational osteotomy in children with cerebral palsy hip dysplasia and predictors of resubluxation. J. Pediatr. Orthop. 2018, 38, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Hoffer, M.M.; Stein, G.A.; Koffman, M.; Prietto, M. Femoral varus-derotation osteotomy in spastic cerebral palsy. J. Bone Jt. Surg. Am. 1985, 67, 1229–1235. [Google Scholar] [CrossRef]
- Noonan, K.J.; Walker, T.L.; Kayes, K.J.; Feinberg, J. Varus derotation osteotomy for the treatment of hip subluxation and dislocation in cerebral palsy: Statistical analysis in 73 hips. J. Pediatr. Orthop. Part B 2001, 10, 279–286. [Google Scholar]
- McNerney, N.P.; Mubarak, S.J.; Wenger, D.R. One-stage correction of the dysplastic hip in cerebral palsy with the san diego acetabuloplasty: Results and complications in 104 hips. J. Pediatr. Orthop. 2000, 20, 93–103. [Google Scholar] [CrossRef]
- Chang, F.M.; Ma, J.; Pan, Z.; Ingram, J.D.; Novais, E.N. Acetabular remodeling after a varus derotational osteotomy in children with cerebral palsy. J. Pediatr. Orthop. 2016, 36, 198–204. [Google Scholar] [CrossRef]
- Shore, B.J.; Powell, D.; Miller, P.E.; Matheney, T.H.; Snyder, B.D. Acetabular and femoral remodeling after varus derotational osteotomy in cerebral palsy: The effect of age and gross motor function classification level. J. Pediatr. Orthop. Part B 2016, 25, 322–330. [Google Scholar] [CrossRef]
- Huh, K.; Rethlefsen, S.A.; Wren, T.A.; Kay, R.M. Surgical management of hip subluxation and dislocation in children with cerebral palsy: Isolated vdro or combined surgery? J. Pediatr. Orthop. 2011, 31, 858–863. [Google Scholar] [CrossRef]
- Song, H.R.; Carroll, N.C. Femoral varus derotation osteotomy with or without acetabuloplasty for unstable hips in cerebral palsy. J. Pediatr. Orthop. 1998, 18, 62–68. [Google Scholar] [CrossRef]
- Oh, C.W.; Presedo, A.; Dabney, K.W.; Miller, F. Factors affecting femoral varus osteotomy in cerebral palsy: A long-term result over 10 years. J. Pediatr. Orthop. Part B 2007, 16, 23–30. [Google Scholar] [CrossRef]
- Al-Ghadir, M.; Masquijo, J.J.; Guerra, L.A.; Willis, B. Combined femoral and pelvic osteotomies versus femoral osteotomy alone in the treatment of hip dysplasia in children with cerebral palsy. J. Pediatr. Orthop. 2009, 29, 779–783. [Google Scholar] [CrossRef]
- Zhang, S.; Wilson, N.C.; Mackey, A.H.; Stott, N.S. Radiological outcome of reconstructive hip surgery in children with gross motor function classification system iv and v cerebral palsy. J. Pediatr. Orthop. Part B 2014, 23, 430–434. [Google Scholar] [CrossRef] [PubMed]
- Palisano, R.; Rosenbaum, P.; Walter, S.; Russell, D.; Wood, E.; Galuppi, B. Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev. Med. Child Neurol. 1997, 39, 214–223. [Google Scholar] [CrossRef] [PubMed]
- Terjesen, T. The natural history of hip development in cerebral palsy. Dev. Med. Child Neurol. 2012, 54, 951–957. [Google Scholar] [CrossRef] [PubMed]
- Reimers, J. The stability of the hip in children. A radiological study of the results of muscle surgery in cerebral palsy. Acta Orthop. Scand. 1980, 184, 1–100. [Google Scholar] [CrossRef]
- Tonnis, D. Normal values of the hip joint for the evaluation of x-rays in children and adults. Clin. Orthop. Relat. Res. 1976, 119, 39–47. [Google Scholar]
- Southwick, W.O. Osteotomy through the lesser trochanter for slipped capital femoral epiphysis. J. Bone Jt. Surg. Am. 1967, 49, 807–835. [Google Scholar] [CrossRef]
- Rutz, E.; Vavken, P.; Camathias, C.; Haase, C.; Junemann, S.; Brunner, R. Long-term results and outcome predictors in one-stage hip reconstruction in children with cerebral palsy. J. Bone Jt. Surg. Am. 2015, 97, 500–506. [Google Scholar] [CrossRef]
- Heidt, C.; Hollander, K.; Wawrzuta, J.; Molesworth, C.; Willoughby, K.; Thomason, P.; Khot, A.; Graham, H.K. The radiological assessment of pelvic obliquity in cerebral palsy and the impact on hip development. Bone Jt. J. 2015, 97, 1435–1440. [Google Scholar] [CrossRef]
- Shore, B.J.; Yu, X.; Desai, S.; Selber, P.; Wolfe, R.; Graham, H.K. Adductor surgery to prevent hip displacement in children with cerebral palsy: The predictive role of the gross motor function classification system. J. Bone Jt. Surg. Am. 2012, 94, 326–334. [Google Scholar] [CrossRef]
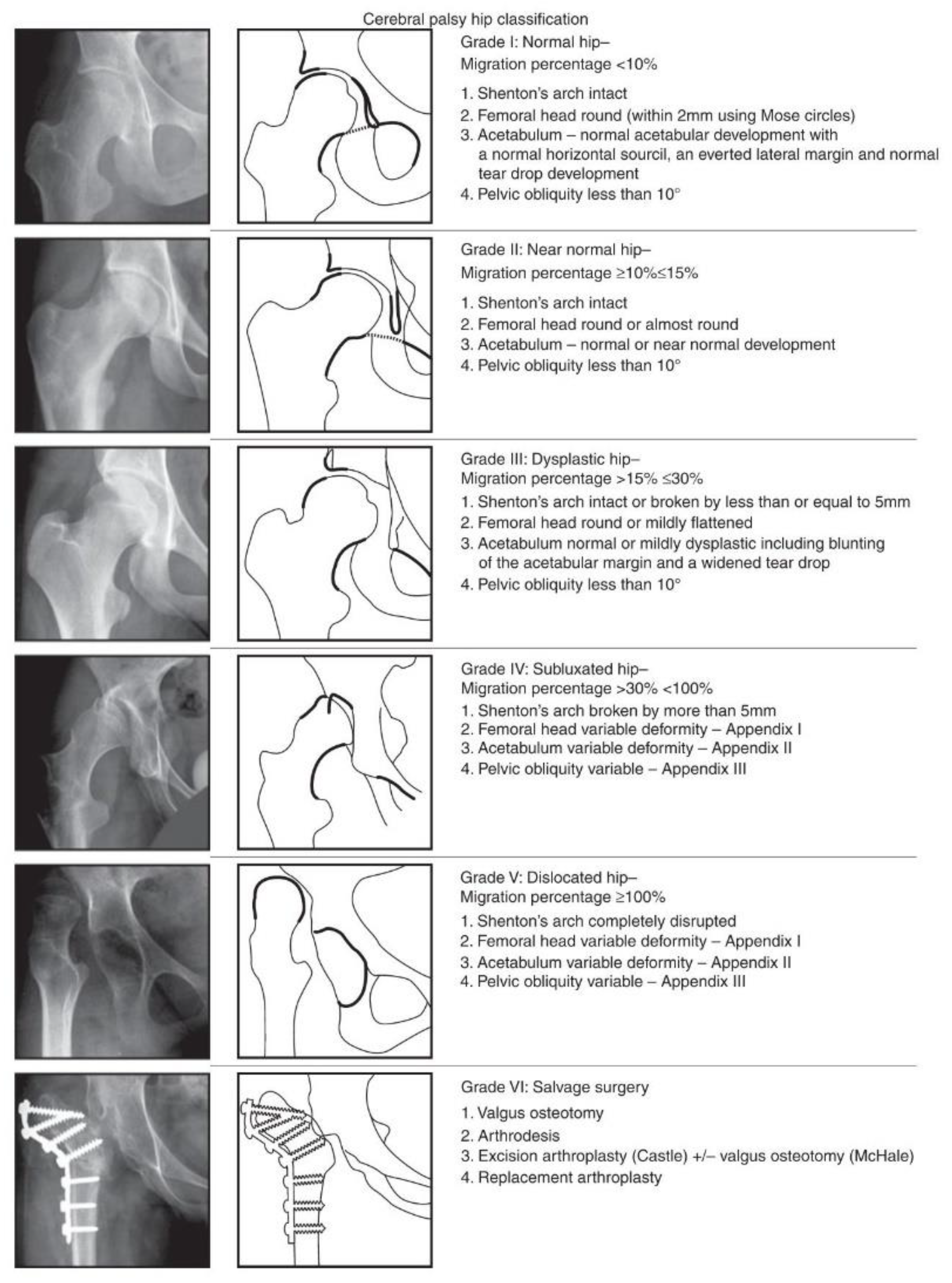
- Robin, J.; Graham, H.K.; Baker, R.; Selber, P.; Simpson, P.; Symons, S.; Thomason, P. A classification system for hip disease in cerebral palsy. Dev. Med. Child Neurol. 2009, 51, 183–192. [Google Scholar] [CrossRef]
- Foroohar, A.; McCarthy, J.J.; Yucha, D.; Clarke, S.; Brey, J. Head-shaft angle measurement in children with cerebral palsy. J. Pediatr. Orthop. 2009, 29, 248–250. [Google Scholar] [CrossRef] [PubMed]
- Kruczynski, J. Avascular necrosis of the proximal femur in developmental dislocation of the hip. Incidence, risk factors, sequelae and mr imaging for diagnosis and prognosis. Acta Orthop. Scand. 1996, 268, 1–48. [Google Scholar] [CrossRef]
- Shrader, M.W.; Koenig, A.L.; Falk, M.; Belthur, M.; Boan, C. An independent assessment of reliability of the melbourne cerebral palsy hip classification system. J. Child. Orthop. 2017, 11, 334–338. [Google Scholar] [CrossRef] [PubMed]
- Wawrzuta, J.; Willoughby, K.L.; Molesworth, C.; Ang, S.G.; Shore, B.J.; Thomason, P.; Graham, H.K. Hip health at skeletal maturity: A population-based study of young adults with cerebral palsy. Dev. Med. Child Neurol. 2016, 58, 1273–1280. [Google Scholar] [CrossRef]
- Settecerri, J.J.; Karol, L.A. Effectiveness of femoral varus osteotomy in patients with cerebral palsy. J. Pediatr. Orthop. 2000, 20, 776–780. [Google Scholar] [CrossRef]
- Maddock, C.L.; Noor, S.; Kothari, A.; Bradley, C.S.; Kelley, S.P. Reliability of the sourcil method of acetabular index measurement in developmental dysplasia of the hip. J. Child. Orthop. 2019, 13, 167–171. [Google Scholar] [CrossRef]
- Shore, B.J.; Martinkevich, P.; Riazi, M.; Baird, E.; Encisa, C.; Willoughby, K.; Narayanan, U.G. Reliability of radiographic assessments of the hip in cerebral palsy. J. Pediatr. Orthop. 2019, 39, e536–e541. [Google Scholar] [CrossRef]
- Bayusentono, S.; Choi, Y.; Chung, C.Y.; Kwon, S.S.; Lee, K.M.; Park, M.S. Recurrence of hip instability after reconstructive surgery in patients with cerebral palsy. J. Bone Jt. Surg. Am. 2014, 96, 1527–1534. [Google Scholar] [CrossRef]
- Bagg, M.R.; Farber, J.; Miller, F. Long-term follow-up of hip subluxation in cerebral palsy patients. J. Pediatr. Orthop. 1993, 13, 32–36. [Google Scholar] [CrossRef]
- Schmale, G.A.; Eilert, R.E.; Chang, F.; Seidel, K. High reoperation rates after early treatment of the subluxating hip in children with spastic cerebral palsy. J. Pediatr. Orthop. 2006, 26, 617–623. [Google Scholar] [CrossRef]
- Mallet, C.; Ilharreborde, B.; Presedo, A.; Khairouni, A.; Mazda, K.; Pennecot, G.F. One-stage hip reconstruction in children with cerebral palsy: Long-term results at skeletal maturity. J. Child. Orthop. 2014, 8, 221–228. [Google Scholar] [CrossRef] [PubMed]
- Dhawale, A.A.; Karatas, A.F.; Holmes, L.; Rogers, K.J.; Dabney, K.W.; Miller, F. Long-term outcome of reconstruction of the hip in young children with cerebral palsy. Bone Jt. J. 2013, 95, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Root, L.; Laplaza, F.J.; Brourman, S.N.; Angel, D.H. The severely unstable hip in cerebral palsy. Treatment with open reduction, pelvic osteotomy, and femoral osteotomy with shortening. J. Bone Jt. Surg. Am. 1995, 77, 703–712. [Google Scholar] [CrossRef] [PubMed]
- Kasser, J.R.; Bowen, J.R.; MacEwen, G.D. Varus derotation osteotomy in the treatment of persistent dysplasia in congenital dislocation of the hip. J. Bone Jt. Surg. Am. 1985, 67, 195–202. [Google Scholar] [CrossRef]
- Dobson, F.; Boyd, R.N.; Parrott, J.; Nattrass, G.R.; Graham, H.K. Hip surveillance in children with cerebral palsy. Impact on the surgical management of spastic hip disease. J. Bone Jt. Surg. Br. 2002, 84, 720–726. [Google Scholar] [CrossRef]
- Khalife, R.; Ghanem, I.; El Hage, S.; Dagher, F.; Kharrat, K. Risk of recurrent dislocation and avascular necrosis after proximal femoral varus osteotomy in children with cerebral palsy. J. Pediatr. Orthop. Part B 2010, 19, 32–37. [Google Scholar] [CrossRef]
- Siffert, R.S. Patterns of deformity of the developing hip. Clin. Orthop. Relat. Res. 1981, 160, 14–29. [Google Scholar] [CrossRef]
- Valencia, F.G. Management of hip deformities in cerebral palsy. Orthop. Clin. N. Am. 2010, 41, 549–559. [Google Scholar] [CrossRef]
- DiFazio, R.; Shore, B.; Vessey, J.A.; Miller, P.E.; Snyder, B.D. Effect of hip reconstructive surgery on health-related quality of life of non-ambulatory children with cerebral palsy. J. Bone Jt. Surg. Am. 2016, 98, 1190–1198. [Google Scholar] [CrossRef]
- Murnaghan, M.L.; Simpson, P.; Robin, J.G.; Shore, B.J.; Selber, P.; Graham, H.K. The cerebral palsy hip classification is reliable: An inter- and intra-observer reliability study. J. Bone Jt. Surg. Br. 2010, 92, 436–441. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Measurement | Inter-Rater Reliability | Intra-Rater Reliability | ||
|---|---|---|---|---|
| ICC | 95% CI | ICC | 95% CI | |
| Migration percentage | 0.97 | 0.96–0.99 | 0.92 | 0.90–0.94 |
| Acetabular index | 0.81 | 0.76–0.86 | 0.78 | 0.70–0.82 |
| Neck-shaft angle | 0.94 | 0.91–0.96 | 0.91 | 0.87–0.93 |
| Head-shaft angle | 0.88 | 0.83–0.93 | 0.84 | 0.81–0.90 |
| Variables | Preoperative | Postoperative | Final Follow-Up |
|---|---|---|---|
| Migration percentage (%) | 62.0 ± 27.9 | 12.8 ± 15.5 | 27.9 ± 19.6 |
| Acetabular index (°) | 22.8 ± 4.1 | N/A | 19.3 ± 4.3 |
| Neck-shaft angle (°) | 154.4 ± 9.9 | 125.7 ± 10.6 | 138.5 ± 17.2 |
| Head-shaft angle (°) | 164.5 ± 10.1 | 133.9 ± 11.3 | 147.4 ± 13.7 |
| MCPHCS grade (no. (%)) | |||
| I | 0 | 19 (13.2%) | |
| II | 0 | 31 (21.5%) | |
| III | 0 | 63 (43.8%) | |
| IV | 106 (73.6%) | 25 (17.3%) | |
| V | 38 (26.4%) | 4 (2.8%) | |
| VI | 0 | 2 (1.4%) |
| Factors | Univariate | Multivariate | ||
|---|---|---|---|---|
| Coefficient 1 | p-Value | Coefficient 1 | p-Value | |
| Age at surgery | −0.002 (−0.1 to 0.1) | 0.9 | 0.04 (–0.08 to 0.15) | 0.5 |
| Sex | 0.01 (−0.4 to 0.4) | 0.9 | −0.15 (−0.6 to 0.3) | 0.5 |
| Preoperative MP | 0.01 (0.005 to 0.02) | 0.001 | 0.008 (0 to 0.02) | 0.04 |
| Preoperative AI | 0.07 (0.02 to 0.12) | 0.004 | 0.04 (−0.01 to 0.09) | 0.14 |
| Postoperative NSA | −0.02 (−0.04 to 0.01) | 0.2 | ||
| Postoperative HSA | 0.01 (−0.01 to 0.04) | 0.2 | ||
| Postoperative MP | 0.03 (0.01 to 0.04) | <0.001 | 0.02 (0.008 to 0.03) | 0.002 |
| Factor | Univariate | Multivariate | Multivariate | |||
|---|---|---|---|---|---|---|
| Odds Ratio 1 | p-Value | Odds Ratio 1 | p-Value | Odds Ratio 1 | p-Value | |
| Age at surgery | 0.9 (0.8 to 1.2) | 0.9 | 0.9 (0.7 to 1.1) | 0.3 | 0.9 (0.7 to 1.1) | 0.3 |
| Sex | 1.1 (0.5 to 2.4) | 0.9 | 1.7 (0.6 to 4.7) | 0.3 | 1.7 (0.6 to 4.7) | 0.3 |
| Preoperative MP | 0.98 (0.96 to 0.99) | 0.005 | 0.98 (0.95 to 0.99) | 0.03 | ||
| Preoperative MP (per 10 unit) | 0.78 0.65 to 0.93) | 0.005 | 0.78 (0.61 to 0.98) | 0.03 | ||
| Preoperative AI | 0.87 (0.78 to 0.97) | 0.013 | 0.9 (0.8 to 1.0) | 0.07 | 0.9 (0.8 to 1.0) | 0.07 |
| Postoperative NSA | 1.03 (0.97 to 1.1) | 0.36 | ||||
| Postoperative HSA | 0.99 (0.95 to 1.03) | 0.68 | ||||
| Postoperative MP | 0.96 (0.94 to 0.98) | 0.001 | 0.96 (0.94 to 0.99) | 0.007 | ||
| Postoperative MP (per 10 unit) | 0.67 (0.53 to 0.86) | 0.001 | 0.71 (0.55 to 0.91) | 0.007 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, H.; Abdel-Baki, S.W.; Park, K.-B.; Park, B.K.; Rhee, I.; Hong, S.-P.; Kim, H.W. Outcome of Femoral Varus Derotational Osteotomy for the Spastic Hip Displacement: Implication for the Indication of Concomitant Pelvic Osteotomy. J. Clin. Med. 2020, 9, 256. https://doi.org/10.3390/jcm9010256
Park H, Abdel-Baki SW, Park K-B, Park BK, Rhee I, Hong S-P, Kim HW. Outcome of Femoral Varus Derotational Osteotomy for the Spastic Hip Displacement: Implication for the Indication of Concomitant Pelvic Osteotomy. Journal of Clinical Medicine. 2020; 9(1):256. https://doi.org/10.3390/jcm9010256
Chicago/Turabian StylePark, Hoon, Sharkawy Wagih Abdel-Baki, Kun-Bo Park, Byoung Kyu Park, Isaac Rhee, Seung-Pyo Hong, and Hyun Woo Kim. 2020. "Outcome of Femoral Varus Derotational Osteotomy for the Spastic Hip Displacement: Implication for the Indication of Concomitant Pelvic Osteotomy" Journal of Clinical Medicine 9, no. 1: 256. https://doi.org/10.3390/jcm9010256
APA StylePark, H., Abdel-Baki, S. W., Park, K.-B., Park, B. K., Rhee, I., Hong, S.-P., & Kim, H. W. (2020). Outcome of Femoral Varus Derotational Osteotomy for the Spastic Hip Displacement: Implication for the Indication of Concomitant Pelvic Osteotomy. Journal of Clinical Medicine, 9(1), 256. https://doi.org/10.3390/jcm9010256