Cytomegalovirus Viremia after Living and Deceased Donation in Kidney Transplantation

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. CMV
2.3. Statistical Analysis
3. Results
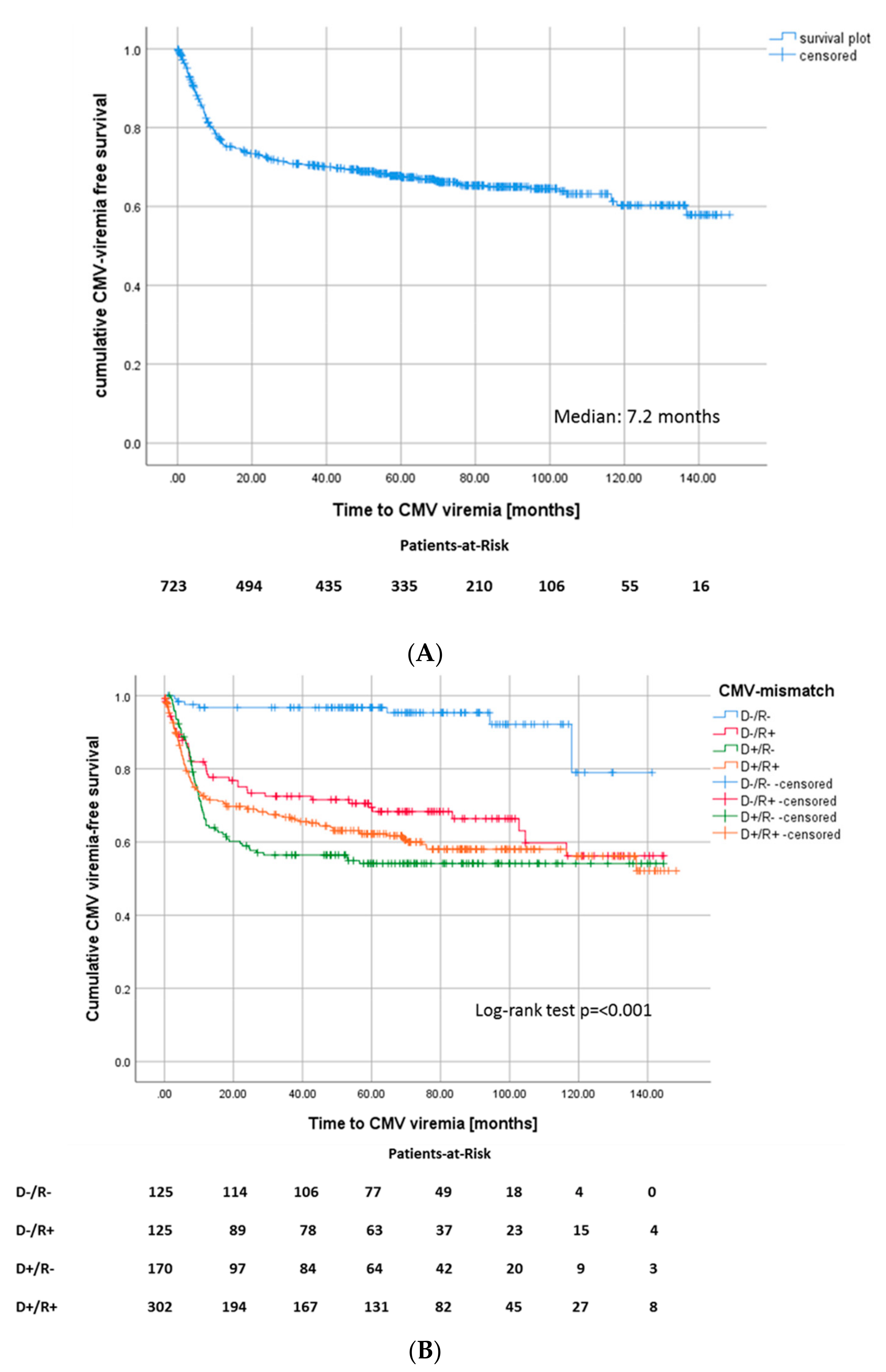
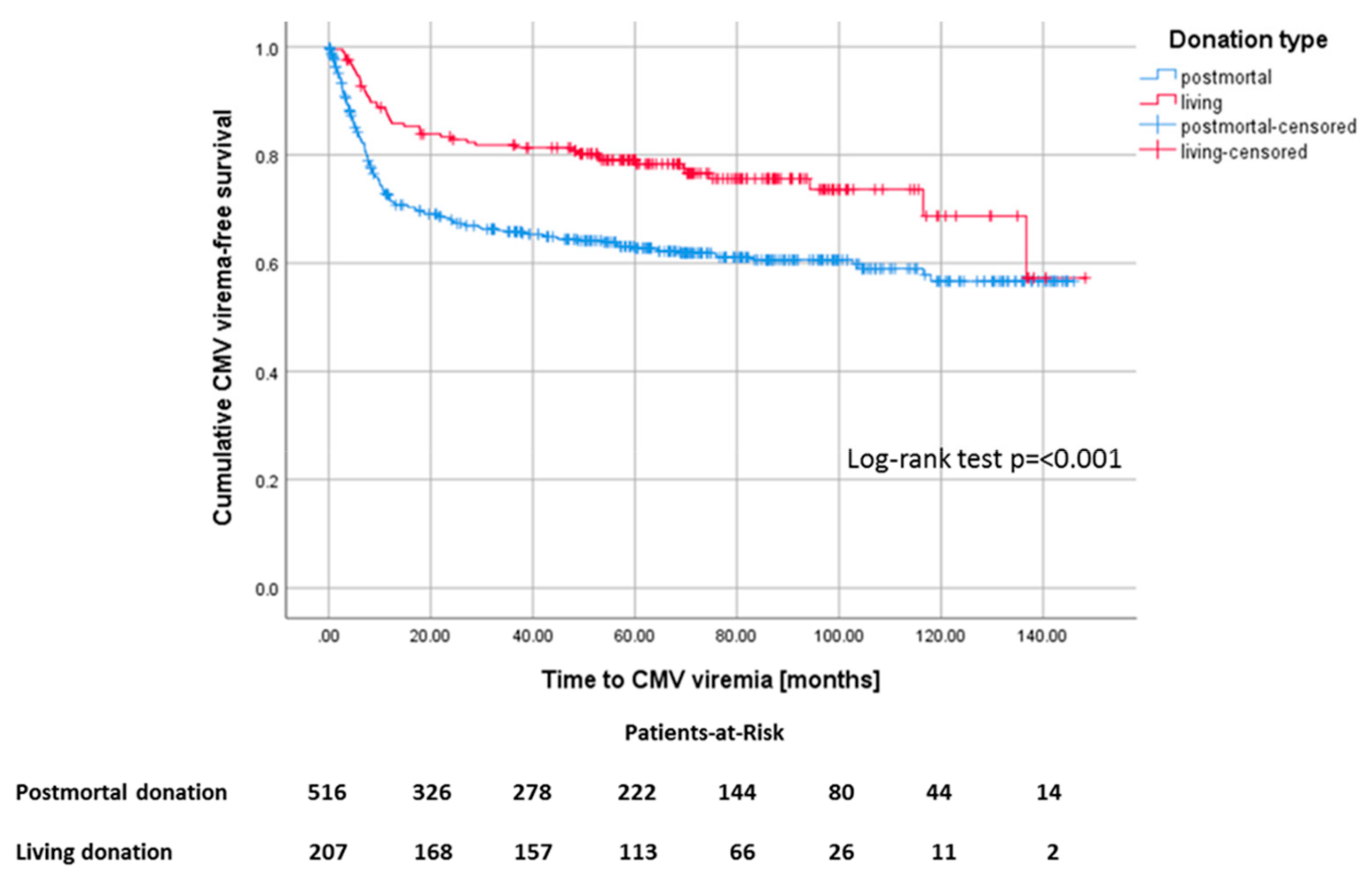
3.1. CMV Viremia
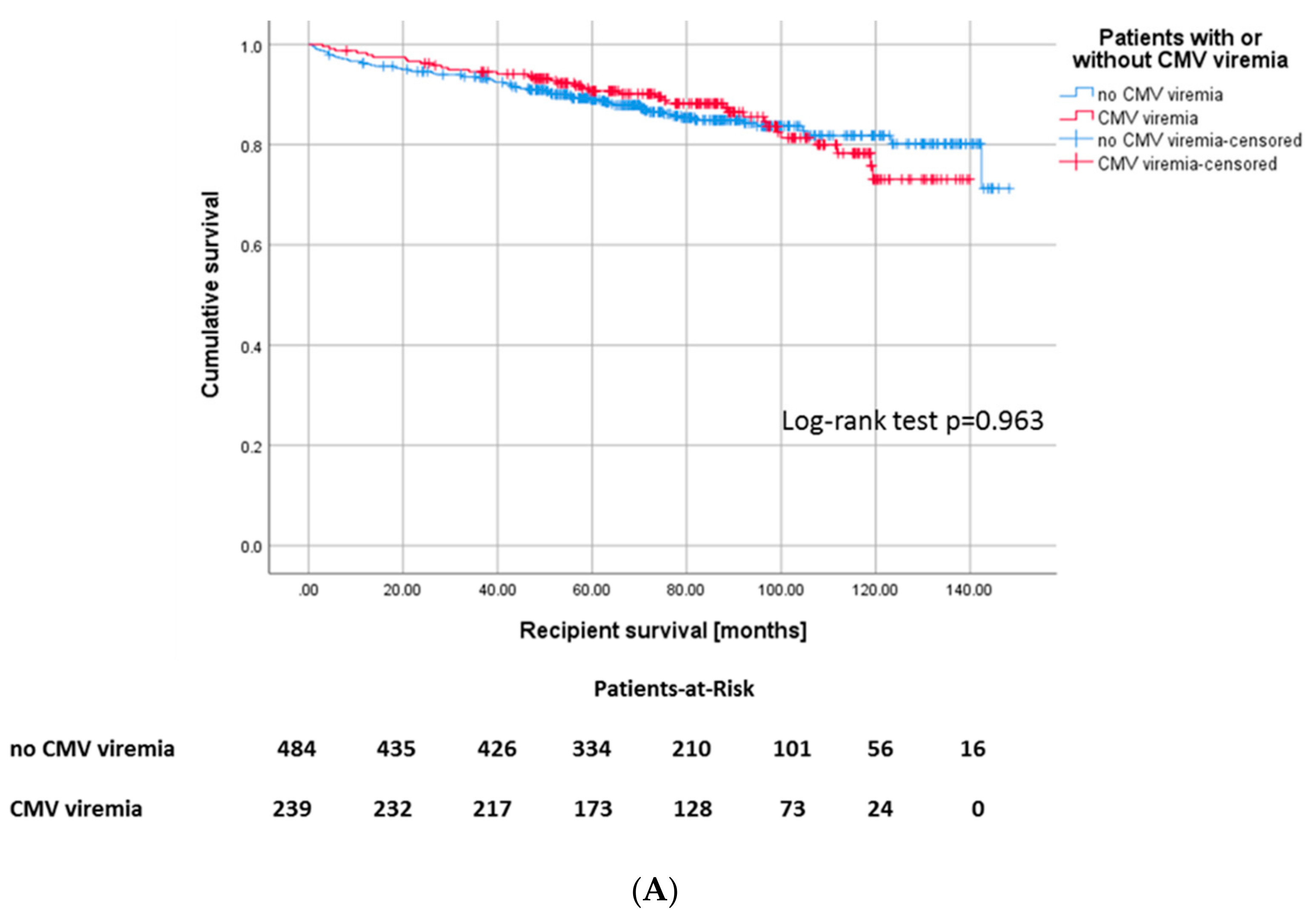
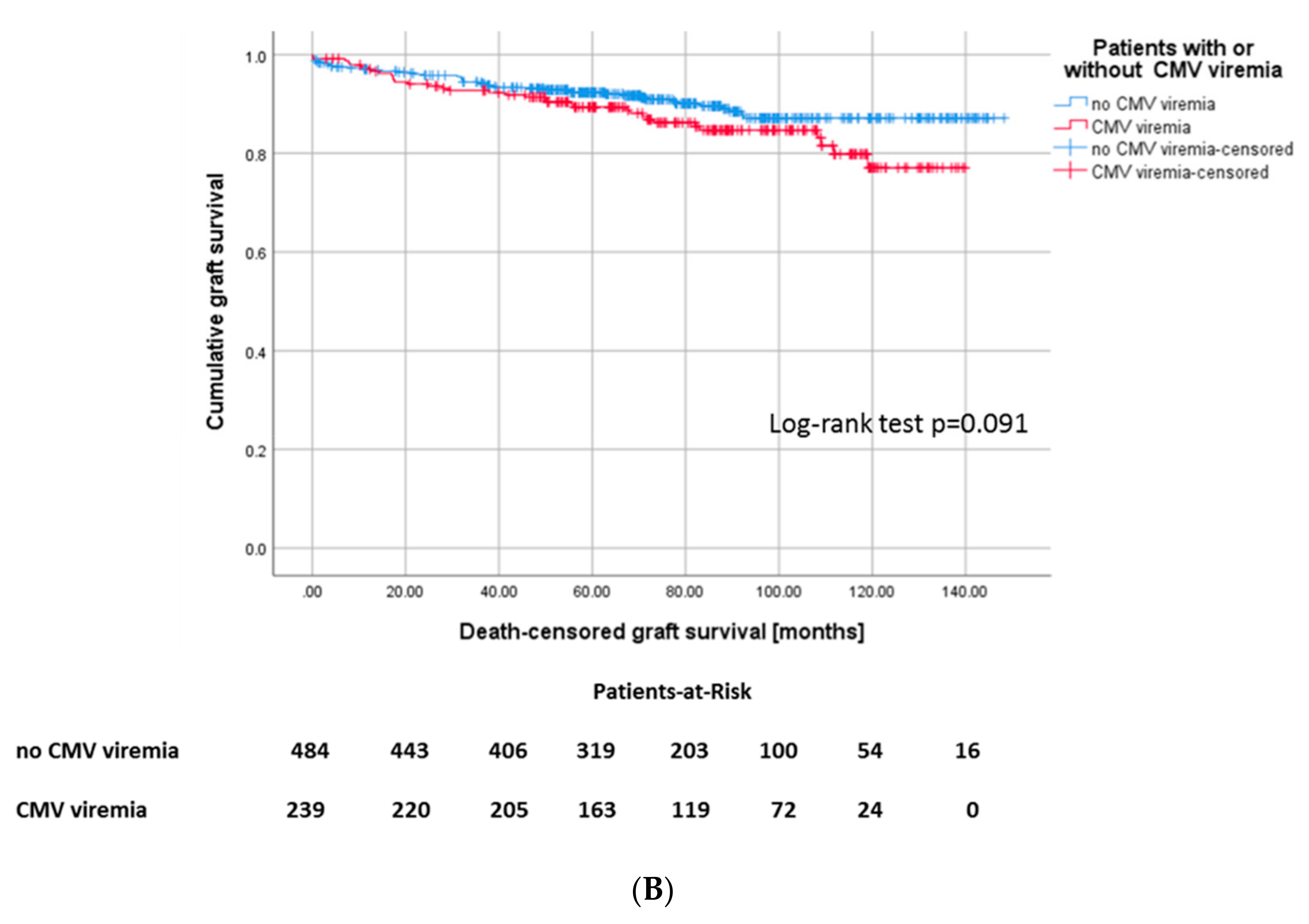
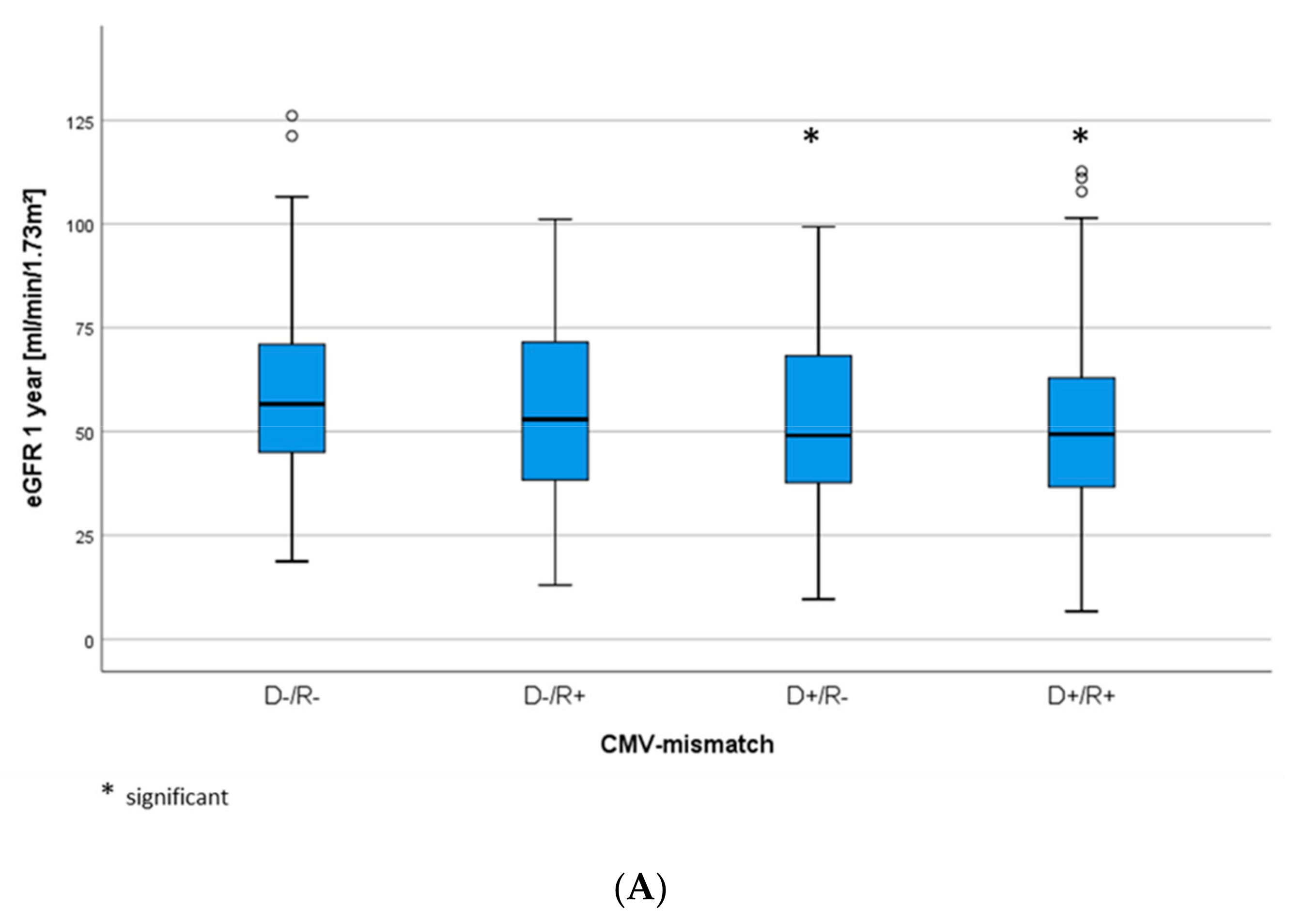
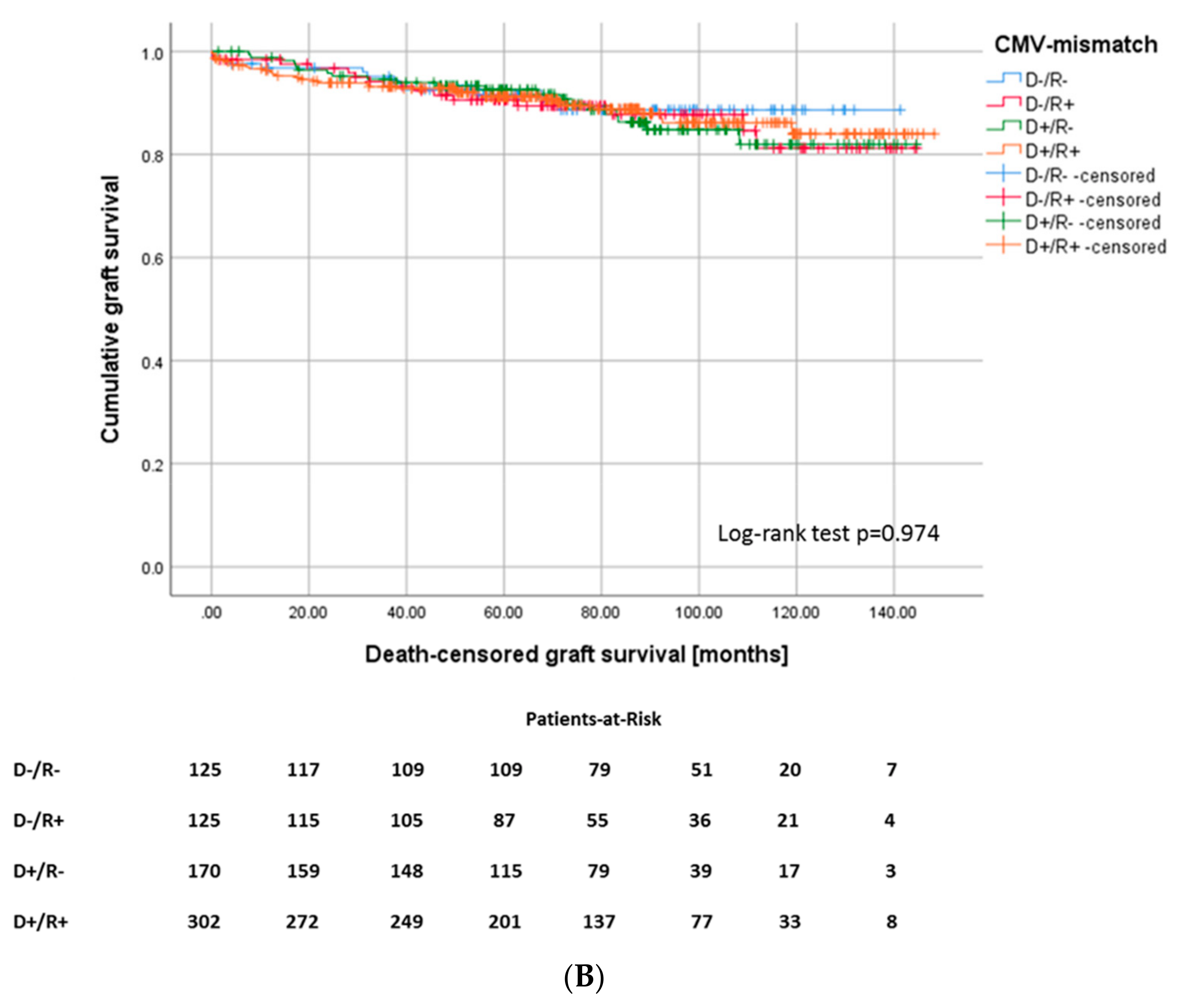
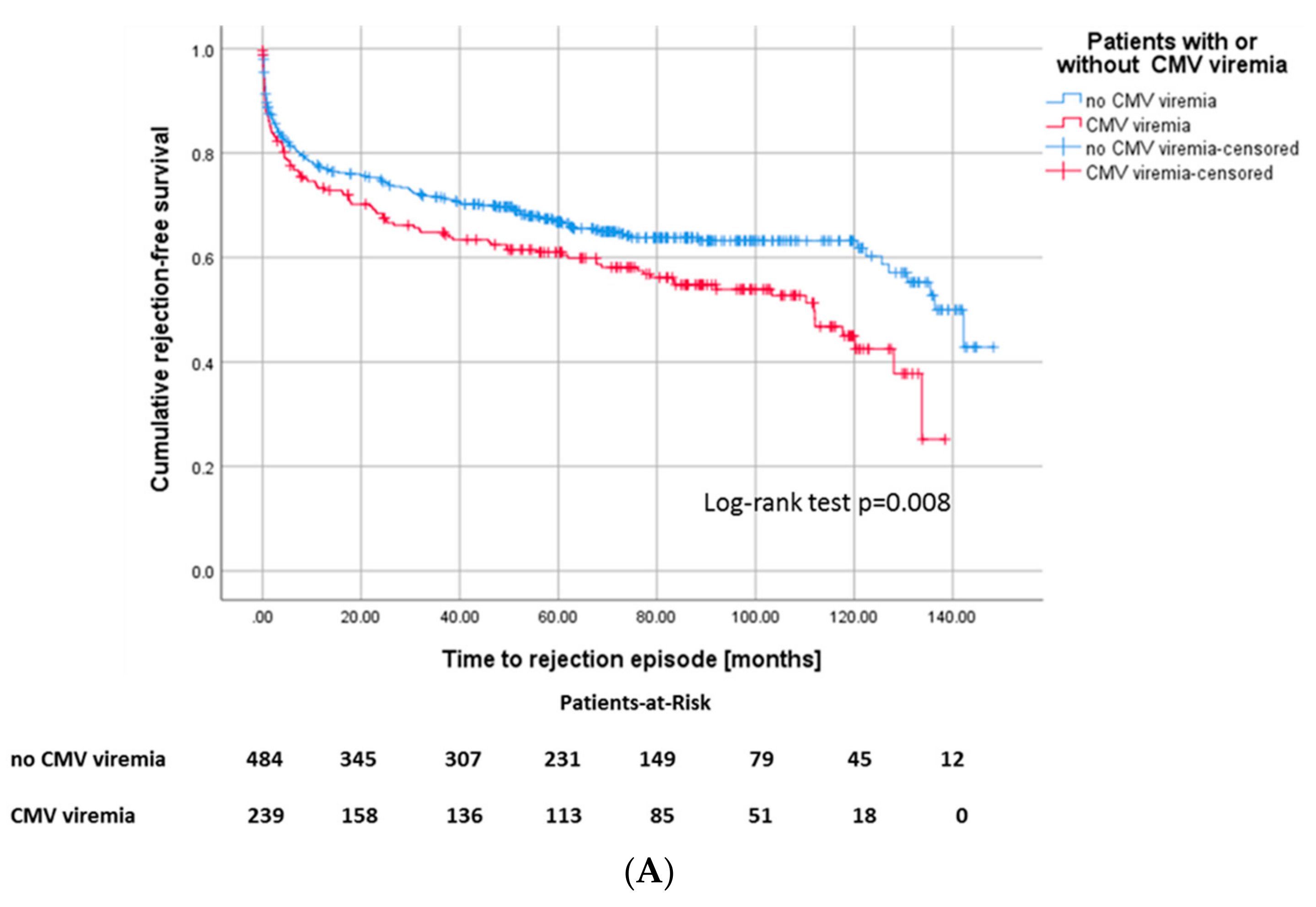
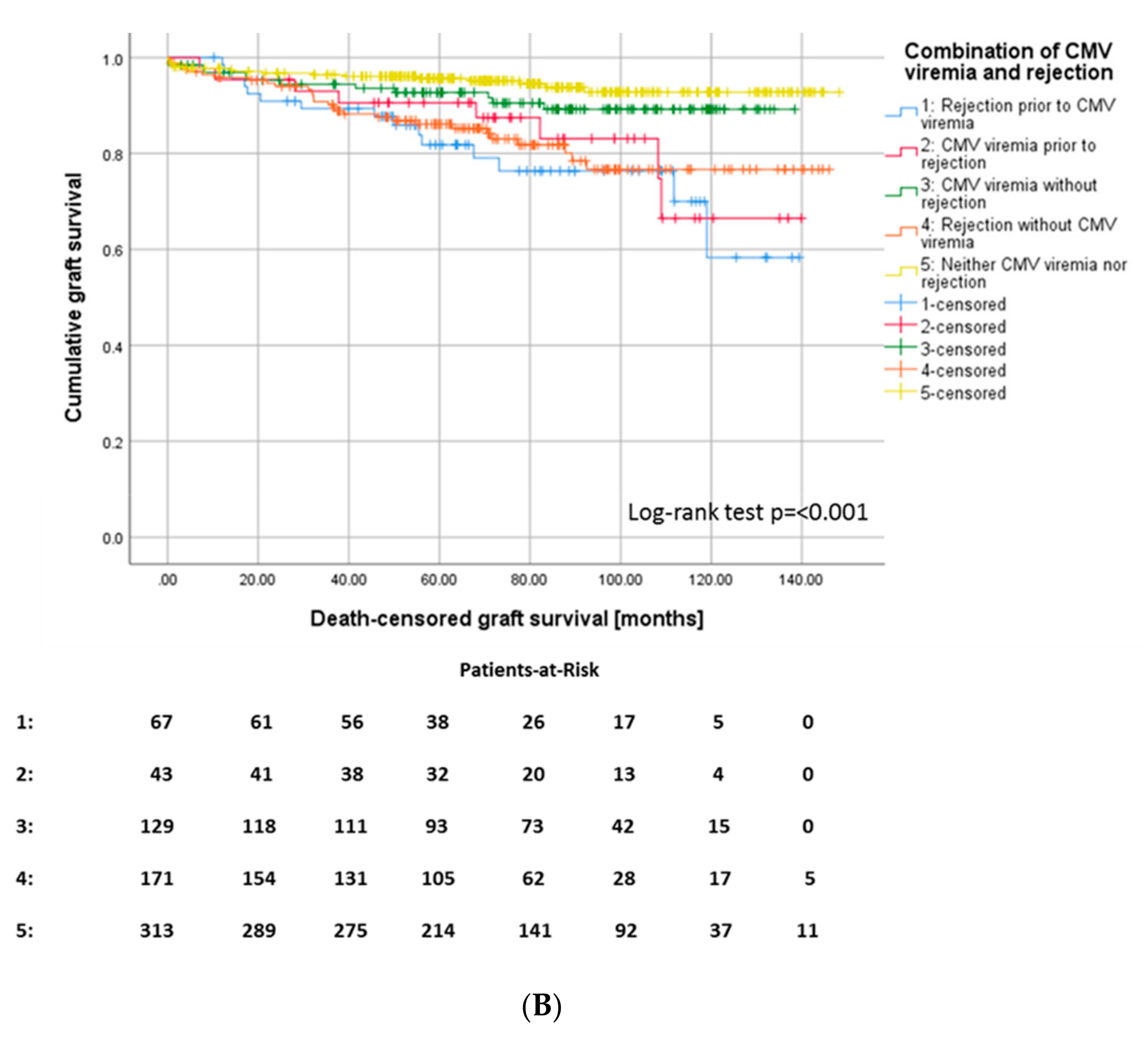
3.2. Association between CMV Viremia, CMV Mismatch, and Outcome Parameters after KTx
3.3. Identified Risk Factors Associated with CMV Viremia
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Fisher, R.A. Cytomegalovirus infection and disease in the new era of immunosuppression following solid organ transplantation. Transpl. Infect. Dis. 2009, 11, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Lentine, K.L.; Kasiske, B.L.; Levey, A.S.; Adams, P.L.; Alberú, J.; Bakr, M.A.; Gallon, L.; Garvey, C.A.; Guleria, S.; Li, P.K.; et al. KDIGO Clinical Practice Guideline on the Evaluation and Care of Living Kidney Donors. Transplantation 2017, 101 (Suppl. 1), S1–S109. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO) Transplant Work Group. KDIGO clinical practice guideline for the care of kidney transplant recipients. Am. J. Transplant. 2009, 9 (Suppl. 3), S1–S155. [Google Scholar] [CrossRef] [PubMed]
- Manicklal, S.; Emery, V.C.; Lazzarotto, T.; Boppana, S.B.; Gupta, R.K. The “silent” global burden of congenital cytomegalovirus. Clin. Microbiol. Rev. 2013, 26, 86–102. [Google Scholar] [CrossRef] [PubMed]
- Rowshani, A.T.; Bemelman, F.J.; van Leeuwen, E.M.; van Lier, R.A.; ten Berge, I.J. Clinical and immunologic aspects of cytomegalovirus infection in solid organ transplant recipients. Transplantation 2005, 79, 381–386. [Google Scholar] [CrossRef] [PubMed]
- Cordero, E.; Casasola, C.; Ecarma, R.; Danguilan, R. Cytomegalovirus disease in kidney transplant recipients: Incidence, clinical profile, and risk factors. Transplant. Proc. 2012, 44, 694–700. [Google Scholar] [CrossRef]
- Hodson, E.M.; Ladhani, M.; Webster, A.C.; Strippoli, G.F.; Craig, J.C. Antiviral medications for preventing cytomegalovirus disease in solid organ transplant recipients. Cochrane Database Syst. Rev. 2013, 28, CD003774. [Google Scholar] [CrossRef]
- Razonable, R.R.; Humar, A.; AST Infectious Diseases Community of Practice. Cytomegalovirus in solid organ transplantation. Am. J. Transplant. 2013, 13 (Suppl. 4), 93–106. [Google Scholar] [CrossRef]
- Navarro, D.; San-Juan, R.; Manuel, O.; Giménez, E.; Fernández-Ruiz, M.; Hirsch, H.H.; Grossi, P.A.; Aguado, J.M.; ESGICH CMV Survey Study Group, on behalf of the European Study Group of Infections in Compromised Hosts (ESGICH) from the Society of Clinical Microbiology and Infectious Diseases (ESCMID). Cytomegalovirus infection management in solid organ transplant recipients across European centers in the time of molecular diagnostics: An ESGICH survey. Transpl. Infect. Dis. 2017, 19. [Google Scholar] [CrossRef]
- Radtke, J.; Dietze, N.; Spetzler, V.N.; Fischer, L.; Achilles, E.G.; Li, J.; Scheidat, S.; Thaiss, F.; Nashan, B.; Koch, M. Fewer cytomegalovirus complications after kidney transplantation by de novo use of mTOR inhibitors in comparison to mycophenolic acid. Transpl. Infect. Dis. 2016, 18, 79–88. [Google Scholar] [CrossRef]
- Fehr, T.; Cippà, P.E.; Mueller, N.J. Cytomegalovirus post kidney transplantation: Prophylaxis versus pre-emptive therapy? Transpl. Int. 2015, 28, 1351–1356. [Google Scholar] [CrossRef] [PubMed]
- Ljungman, P.; Griffiths, P.; Paya, C. Definitions of cytomegalovirus infection and disease in transplant recipients. Clin. Infect. Dis. 2002, 34, 1094–1097. [Google Scholar] [CrossRef] [PubMed]
- Pilmore, H.; Pussell, B.; Goodman, D. KHA-CARI guideline: Cytomegalovirus disease and kidney transplantation. Nephrology 2011, 16, 683–687. [Google Scholar] [CrossRef]
- Selvey, L.A.; Lim, W.H.; Boan, P.; Swaminathan, R.; Slimings, C.; Harrison, A.E.; Chakera, A. Cytomegalovirus viraemia and mortality in renal transplant recipients in the era of antiviral prophylaxis. Lessons from the western Australian experience. BMC Infect. Dis. 2017, 17, 501. [Google Scholar] [CrossRef]
- Jamal, A.J.; Husain, S.; Li, Y.; Famure, O.; Kim, S.J. Risk factors for late-onset cytomegalovirus infection or disease in kidney transplant recipients. Transplantation 2014, 97, 569–575. [Google Scholar] [CrossRef]
- Werzowa, J.; Schwaiger, B.; Hecking, M.; Strassl, R.; Schmaldienst, S.; Böhmig, G.A.; Genser, B.; Säemann, M.D. Prophylactic CMV therapy does not improve three-yr patient and graft survival compared to preemptive therapy. Clin. Transplant. 2015, 29, 1230–1238. [Google Scholar] [CrossRef]
- Fayek, S.A.; Beshears, E.; Lieber, R.; Alvey, N.; Sauer, A.; Poirier, J.; Hollinger, E.F.; Olaitan, O.K.; Jensik, S.; Geyston, J.; et al. Extended Low-Dose Valganciclovir Is Effective Prophylaxis Against Cytomegalovirus in High-Risk Kidney Transplant Recipients with Near-Complete Eradication of Late-Onset Disease. Transplant. Proc. 2016, 48, 2056–2064. [Google Scholar] [CrossRef]
- Smedbråten, Y.V.; Sagedal, S.; Leivestad, T.; Mjøen, G.; Osnes, K.; Rollag, H.; Reisaeter, A.V.; Foss, A.; Os, I.; Hartmann, A. The impact of early cytomegalovirus infection after kidney transplantation on long-term graft and patient survival. Clin. Transplant. 2014, 28, 120–126. [Google Scholar] [CrossRef]
- Stern, M.; Hirsch, H.; Cusini, A.; van Delden, C.; Manuel, O.; Meylan, P.; Boggian, K.; Mueller, N.J.; Dickenmann, M.; Members of Swiss Transplant Cohort Study. Cytomegalovirus serology and replication remain associated with solid organ graft rejection and graft loss in the era of prophylactic treatment. Transplantation 2014, 98, 1013–1018. [Google Scholar] [CrossRef]
- Erdbrügger, U.; Scheffner, I.; Mengel, M.; Schwarz, A.; Haller, H.; Gwinner, W. Long-term impact of CMV infection on allografts and on patient survival in renal transplant patients with protocol biopsies. Am. J. Physiol. Ren. Physiol. 2015, 309, F925–F932. [Google Scholar] [CrossRef]
- Santos, A.H.; Chen, C.; Casey, M.J.; Womer, K.L.; Wen, X. New-onset diabetes after kidney transplantation: Can the risk be modified by choosing immunosuppression regimen based on pretransplant viral serology? Nephrol. Dial. Transplant. 2018, 33, 177–184. [Google Scholar] [CrossRef] [PubMed]
- De Matos, S.B.; Meyer, R.; Lima, F.W.M. Cytomegalovirus Infection after Renal Transplantation: Occurrence, Clinical Features, and the Cutoff for Antigenemia in a University Hospital in Brazil. J. Infect. Chemother. 2017, 49, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Roman, A.; Manito, N.; Campistol, J.M.; Cuervas-Mons, V.; Almenar, L.; Arias, M.; Casafont, F.; del Castillo, D.; Crespo-Leiro, M.G.; Delgado, J.F.; et al. ATOS working group. The impact of the prevention strategies on the indirect effects of CMV infection in solid organ transplant recipients. Transplant. Rev. 2014, 28, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Davis, S.; Cooper, J.E. Acute antibody-mediated rejection in kidney transplant recipients. Transplant. Rev. 2017, 31, 47–54. [Google Scholar] [CrossRef]
- Lautenschlager, I.; Soots, A.; Krogerus, L.; Inkinen, K.; Kloover, J.; Loginov, R.; Holma, K.; Kauppinen, H.; Bruggeman, C.; Ahonen, J. Time-related effects of cytomegalovirus infection on the development of chronic renal allograft rejection in a rat model. Intervirology 1999, 42, 279–284. [Google Scholar] [CrossRef]
- Felipe, C.; Ferreira, A.N.; de Paula, M.; Viana, L.; Cristelli, M.; Medina Pestana, J.; Tedesco-Silva, H. Incidence and risk factors associated with cytomegalovirus infection after the treatment of acute rejection during the first year in kidney transplant recipients receiving preemptive therapy. Transpl. Infect. Dis. 2019, 21, e13106. [Google Scholar] [CrossRef]
- Schachtner, T.; Babel, N.; Reinke, P. Different risk factor profiles distinguish early-onset from late-onset BKV-replication. Transpl. Int. 2015, 28, 1081–1091. [Google Scholar] [CrossRef]
- Elfadawy, N.; Flechner, S.M.; Liu, X. CMV Viremia is associated with a decreased incidence of BKV reactivation after kidney and kidney-pancreas transplantation. Transplantation 2013, 96, 1097–1103. [Google Scholar] [CrossRef]
- Reischig, T.; Kacer, M.; Hes, O.; Machova, J.; Nemcova, J.; Lysak, D.; Jindra, P.; Pivovarcikova, K.; Kormunda, S.; Bouda, M. BK polyomavirus and valganciclovir: Highly suspected association urgently calling for a new randomized trial. Am. J. Transplant. 2019, 19, 3434–3435. [Google Scholar] [CrossRef]
- Jehn, U.; Schütte-Nütgen, K.; Bautz, J.; Suwelack, B.; Reuter, S. Valganciclovir is not a risk factor of BK polyomavirus viremia. Am. J. Transplant. 2019, 19, 3436–3437. [Google Scholar] [CrossRef]
- Leeaphorn, N.; Garg, N.; Thamcharoen, N.; Khankin, E.V.; Cardarelli, F.; Pavlakis, M. Cytomegalovirus mismatch still negatively affects patient and graft survival in the era of routine prophylactic and preemptive therapy: A paired kidney analysis. Am. J. Transplant. 2019, 19, 573–584. [Google Scholar] [CrossRef] [PubMed]
- Blazquez-Navarro, A.; Dang-Heine, C.; Wittenbrink, N.; Bauer, C.; Wolk, K.; Sabat, R.; Westhoff, T.H.; Sawitzki, B.; Reinke, P.; Thomusch, O.; et al. BKV, CMV, and EBV Interactions and their Effect on Graft Function One Year Post-Renal Transplantation: Results from a Large Multi-Centre Study. EBioMedicine 2019, 34, 113–121. [Google Scholar] [CrossRef]
- Reischig, T.; Kacer, M.; Hruba, P.; Jindra, P.; Hes, O.; Lysak, D.; Bouda, M.; Viklicky, O. The impact of viral load and time to onset of cytomegalovirus replication on long-term graft survival after kidney transplantation. Antivir. Ther. 2017, 22, 503–513. [Google Scholar] [CrossRef] [PubMed]
- Helanterä, I.; Schachtner, T.; Hinrichs, C.; Salmela, K.; Kyllönen, L.; Koskinen, P.; Lautenschlager, I.; Reinke, P. Current characteristics and outcome of cytomegalovirus infections after kidney transplantation. Transpl. Infect. Dis. 2014, 16, 568–577. [Google Scholar] [CrossRef] [PubMed]
- Owers, D.S.; Webster, A.C.; Strippoli, G.F.; Kable, K.; Hodson, E.M. Pre-emptive treatment for cytomegalovirus viraemia to prevent cytomegalovirus disease in solid organ transplant recipients. Cochrane Database Syst. Rev. 2013, 28, CD005133. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Non-CMV | CMV | p Value |
|---|---|---|---|
| Patients (n) | 484 (68.2%) | 239 (33.1%) | 0.000 a |
| Age at Tx * (years) | 50.8 ± 13.9 | 54.35 ± 14.1 | 0.010 a |
| Sex male (n) | 300 (62%) | 137 (57.3%) | 0.258 b |
| ABO incompatible Tx * (n) | 30 (6.2%) | 11 (4.6%) | 0.494 b |
| mismatch-HLA-A | 0.838 b | ||
| none | 173 (35.7%) | 80 (33.5%) | |
| 1 | 228 (47.1%) | 117 (49%) | |
| 2 | 81 (16.7%) | 41 (17.2%) | |
| mismatch-HLA-B | 0.925 b | ||
| none | 113 (23.3%) | 55 (23%) | |
| 1 | 232 (47.9%) | 112 (46.9%) | |
| 2 | 137 (28.3%) | 71 (29.7%) | |
| mismatch-HLA-DR | 0.482 b | ||
| none | 129 (26.7%) | 56 (23.4%) | |
| 1 | 231 (47.7%) | 113 (47.3%) | |
| 2 | 122 (25.2%) | 69 (28.9%) | |
| PRA >85% (n) | 61 (12.6%) | 26 (10.9%) | 0.539 b |
| PRA >5% (n) | 10 (2.1%) | 7 (2.9%) | 0.447 b |
| Living donor Tx * (n) | 158 (32.6%) | 49 (20.5%) | 0.001 b |
| Cold ischemia time (hours) | 8.1 ± 5.3) | 8.53 ± 4.76 | 0.175 a |
| Warm ischemia time (minutes) | 32.7 ± 8.2 | 33.5 ± 8.5 | 0.332 a |
| Dialysis prior to Tx * (n) | 443 (91.5%) | 228 (95.4%) | 0.054 b |
| Time on dialysis (months) | 57.7 ± 43.7 | 56.8 ± 36.8 | 0.747 a |
| Previous Tx * (n) | 58 (12%) | 36 (15.1%) | 0.29 b |
| CMV mismatch D/R | 0.000 b | ||
| D−/R− | 118 (24.4%) | 7 (2.9%) | |
| D−/R+ | 84 (17.4%) | 41 (17.2%) | |
| D+/R− | 95 (19.6%) | 73 (31.4%) | |
| D+/R+ | 186 (38.4%) | 116 (48.5%) | |
| Induction therapy | 0.543 c | ||
| No induction therapy | 15 (3.1%) | 12 (5%) | |
| Basiliximab induction (n) | 407 (84.1%) | 198 (82.8%) | |
| Thymoglobulin (n) | 21 (4.4%) | 16 (6.7%) | |
| Alemtuzumab (n) | 9 (1.9%) | 5 (2.1%) | |
| Eculizumab (n) | 2 (0.4%) | 1 (0.4%) | |
| Rituximab (n) | 30 (6.2%) | 10 (4.2%) | |
| Initial steroid use | 473 (97.8%) | 235 (98.3%) | 0.758 b |
| Initial MMF * use | 456 (94.2%) | 235 (98.3%) | 0.039 b |
| Initial CyA * use | 21 (4.4%) | 2 (0.8%) | 0.007 b |
| Initial tacrolimus use (n) | 459 (94.8%) | 237 (99.2%) | 0.007 b |
| Initial mTOR * inhibitor use (n) | 24 (5.0%) | 5 (2.1%) | 0.071 b |
| Diagnosis of ESRD, (n) | 0.522 c | ||
| Hypertension | 34 (7%) | 24 (10%) | |
| Diabetes | 27 (5.6%) | 16 (6.7%) | |
| Polycystic kidney disease | 75 (15.8%) | 30 (12.6%) | |
| Obstructive Nephropathy | 23 (4.8%) | 12 (5%) | |
| Glomerulonephritis | 160 (33.1%) | 71 (29.7%) | |
| FSGS * | 18 (3.7%) | 15 (6.3%) | |
| Interstitial nephritis | 22 (4.5%) | 15 (6.3%) | |
| Vasculitis | 17 (3.5%) | 6 (2.5%) | |
| Other | 69 (14.3%) | 35 (14.6%) | |
| Unknown | 39 (8.1%) | 15 (6.3%) |
| Variable | Non-CMV | CMV | p Value |
|---|---|---|---|
| Time until CMV viremia in months | 16.6 ± 23.9 | - | |
| DGF (n) | 103 (21.3%) | 73 (30.5%) | 0.018 b |
| eGFR at year 1 (mL/min/1.73 m2) | 55.2 ± 21.0 | 48.8 ± 19.8 | 0.000 a |
| eGFR at year 3 (mL/min/1.73 m2) | 54.7 ± 20.3 | 51.2 ± 20.9 | 0.008 a |
| eGFR at year 5 (mL/min/1.73 m2) | 51.2 ± 20.6 | 47.4 ± 20.7 | 0.002 a |
| UPCR at year 1 (mg/g crea) | 231 ± 503 | 278 ± 339 | 0.001 a |
| UPCR at year 5 (mg/g crea) | 392 ± 544 | 368 ± 496 | 0.831 a |
| Overall graft survival (mean, months) (95% CI) | 124.3 (119.8–128.8) | 114.8 (108.8–120.7) | 0.444 c |
| NODAT * (n) | 109 (22.5%) | 74 (31.5%) | 0.018 b |
| BK viremia | 109 (22.5%) | 59 (24.7%) | 0.514 b |
| Rejection yes (n) | 171 (35.3%) | 110 (46%) | 0.006 b |
| Donation Type | Living | Postmortal | p Value |
|---|---|---|---|
| Patients (n) | 207 (28.6%) | 516 (71.4%) | <0.001 a |
| Recipient Age (years) * | 43.6 (±13.9) | 55.4 (±12.6) | <0.001 a |
| ABO incompatible Tx * (n) | 41 (19.8%) | 0 (0%) | <0.001 b |
| PRA >5% (n) | 23 (11.1%) | 62 (12.0%) | 0.799 b |
| Cold ischemia time (hours) | 2.3 ± 0.5 | 10.7 ± 4.0 | <0.001 a |
| Warm ischemia time (minutes) | 30.7 ± 10.3 | 33.8 ± 7.2 | <0.001 a |
| Time on dialysis (months) | 20.0 ± 23.9 | 72.5 ± 37.5 | <0.001 a |
| Preemptive Tx * (n) | 48 (23.2%) | 0 (0%) | <0.001 b |
| Donor age (years) | 51.7 ± 9.4 | 54.2 ± 16.3 | 0.002 a |
| DGF * (n) | 12 (5.8%) | 164 (31.8%) | <0.001 b |
| NODAT * (n) | 32 (15.5%) | 151 (29.3%) | <0.001 b |
| HLA mismatch (0–6) | 3.4 ± 1.5 | 2.7 ± 1.7 | <0.001 c |
| CMV mismatch (D/R)D−/R− | 52 (25.1%) | 73 (14.1%) | 0.003 b |
| D−/R+ | 26 (12.6%) | 99 (19.2%) | |
| D+/R− | 48 (23.2%) | 122 (23.6%) | |
| D+/R+ | 81 (39.1%) | 221 (42.8%) |
| Variable | Regression-Coefficient | Odds Ratio | 95% CI | p Value |
|---|---|---|---|---|
| Age at KTx | 0.018 | 1.019 | 1.007–1.030 | 0.002 |
| Previous KTx | 0.264 | 1.303 | 0.832–2.093 | 0.248 |
| CMV Match | 0.456 | 1.577 | 1.353–1.838 | <0.001 |
| Living Donation | −0.631 | 0.532 | 0.369–0.768 | 0.001 |
| Donor age | 0.028 | 1.028 | 1.016–1.046 | <0.001 |
| Mode of dialysis | −0.110 | 0.896 | 0.746–1.076 | 0.240 |
| Time of dialysis | 0.000 | 1.000 | 0.996–1.003 | 0.799 |
| Cold ischemia time | 0.016 | 1.016 | 0.986–1.048 | 0.296 |
| Warm ischemia time | 0.011 | 1.011 | 0.912–1.030 | 0.270 |
| Highest PRA | −0.002 | 0.998 | 0.991–1.006 | 0.683 |
| Etiology of kidney failure | −0.020 | 0.980 | 0.924–1.039 | 0.500 |
| NODAT | 0.434 | 1.543 | 1.040–2.154 | 0.014 |
| Delayed graft function | 0.484 | 1.622 | 1.142–2.305 | 0.007 |
| BKV viremia | 0.120 | 1.128 | 0.784–1.612 | 0.517 |
| Initial Steroids | −0.148 | 0.862 | 0.250–2.974 | 0.862 |
| Initial MMF use | 1.120 | 3.065 | 1.051–8.937 | 0.040 |
| Initial CyA use | −1.730 | 0.177 | 0.041–0.760 | 0.020 |
| Initial tacrolimus use | 1.730 | 5.643 | 1.316–24.200 | 0.020 |
| Initial mTor use | −0.893 | 0.410 | 0.154–1.087 | 0.073 |
| Number of acute rejections | 0.256 | 1.292 | 1.117–1.495 | 0.001 |
| HLA-mismatches | 0.040 | 1.049 | 0.949–1.142 | 0.390 |
| Variable | Regression-Coefficient | Odds Ratio | 95% CI | p Value |
|---|---|---|---|---|
| Recipient age | 0.000 | 1.000 | 0.984–1.015 | 0.959 |
| Donor age | 0.020 | 1.020 | 1.006–1.034 | 0.004 |
| CMV match | 0.419 | 1.521 | 1.292–1.720 | <0.001 |
| Living donation | −0.614 | 0.541 | 0.351–0.834 | 0.005 |
| NODAT | 0.197 | 1.217 | 0.825–1.795 | 0.197 |
| DGF | 0.271 | 1.312 | 0.894–1.927 | 0.165 |
| Initial MMF use | 0.533 | 1.705 | 0.496–5.855 | 0.397 |
| Initial CyA use | −2.059 | 0.128 | 0.021–0.766 | 0.024 |
| Number of acute rejections | 0.346 | 1.413 | 1.206–1.655 | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jehn, U.; Schütte-Nütgen, K.; Bautz, J.; Pavenstädt, H.; Suwelack, B.; Thölking, G.; Heinzow, H.; Reuter, S. Cytomegalovirus Viremia after Living and Deceased Donation in Kidney Transplantation. J. Clin. Med. 2020, 9, 252. https://doi.org/10.3390/jcm9010252
Jehn U, Schütte-Nütgen K, Bautz J, Pavenstädt H, Suwelack B, Thölking G, Heinzow H, Reuter S. Cytomegalovirus Viremia after Living and Deceased Donation in Kidney Transplantation. Journal of Clinical Medicine. 2020; 9(1):252. https://doi.org/10.3390/jcm9010252
Chicago/Turabian StyleJehn, Ulrich, Katharina Schütte-Nütgen, Joachim Bautz, Hermann Pavenstädt, Barbara Suwelack, Gerold Thölking, Hauke Heinzow, and Stefan Reuter. 2020. "Cytomegalovirus Viremia after Living and Deceased Donation in Kidney Transplantation" Journal of Clinical Medicine 9, no. 1: 252. https://doi.org/10.3390/jcm9010252
APA StyleJehn, U., Schütte-Nütgen, K., Bautz, J., Pavenstädt, H., Suwelack, B., Thölking, G., Heinzow, H., & Reuter, S. (2020). Cytomegalovirus Viremia after Living and Deceased Donation in Kidney Transplantation. Journal of Clinical Medicine, 9(1), 252. https://doi.org/10.3390/jcm9010252