Impact of Disease-Specific Fears on Pulmonary Rehabilitation Trajectories in Patients with COPD

 , ,
, ,
Abstract
1. Introduction
2. Experimental Section
2.1. Participants
2.2. Pulmonary Rehabilitation Program
2.3. Measurements
2.3.1. Lung Function and Exercise Capacity
2.3.2. Self-Report Measures
2.4. Procedure
2.5. Data Analysis
3. Results
3.1. Patient Characteristics
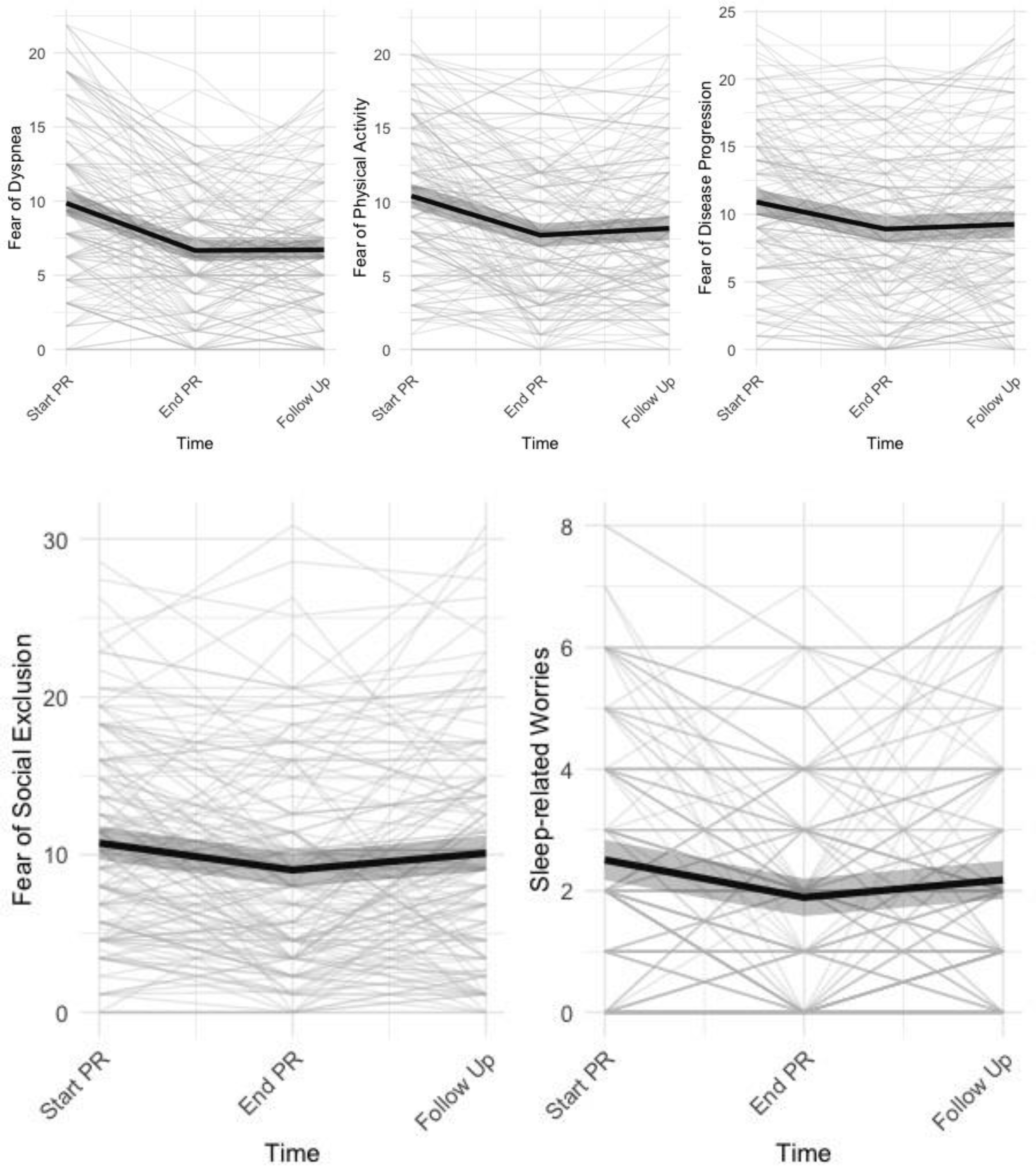
3.2. Change in Disease-Specific Fears and other Pulmonary Rehabilitation Outcomes
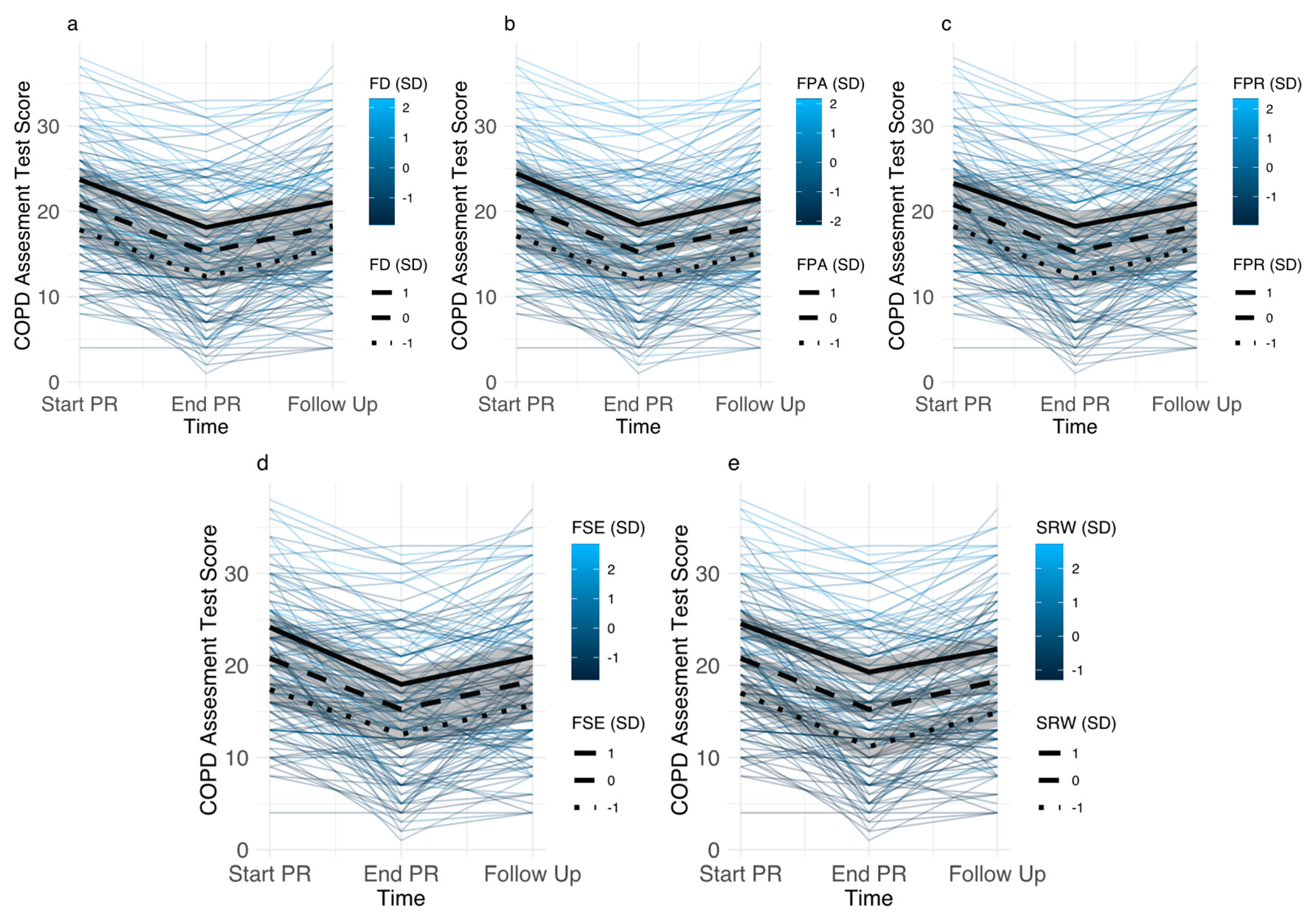
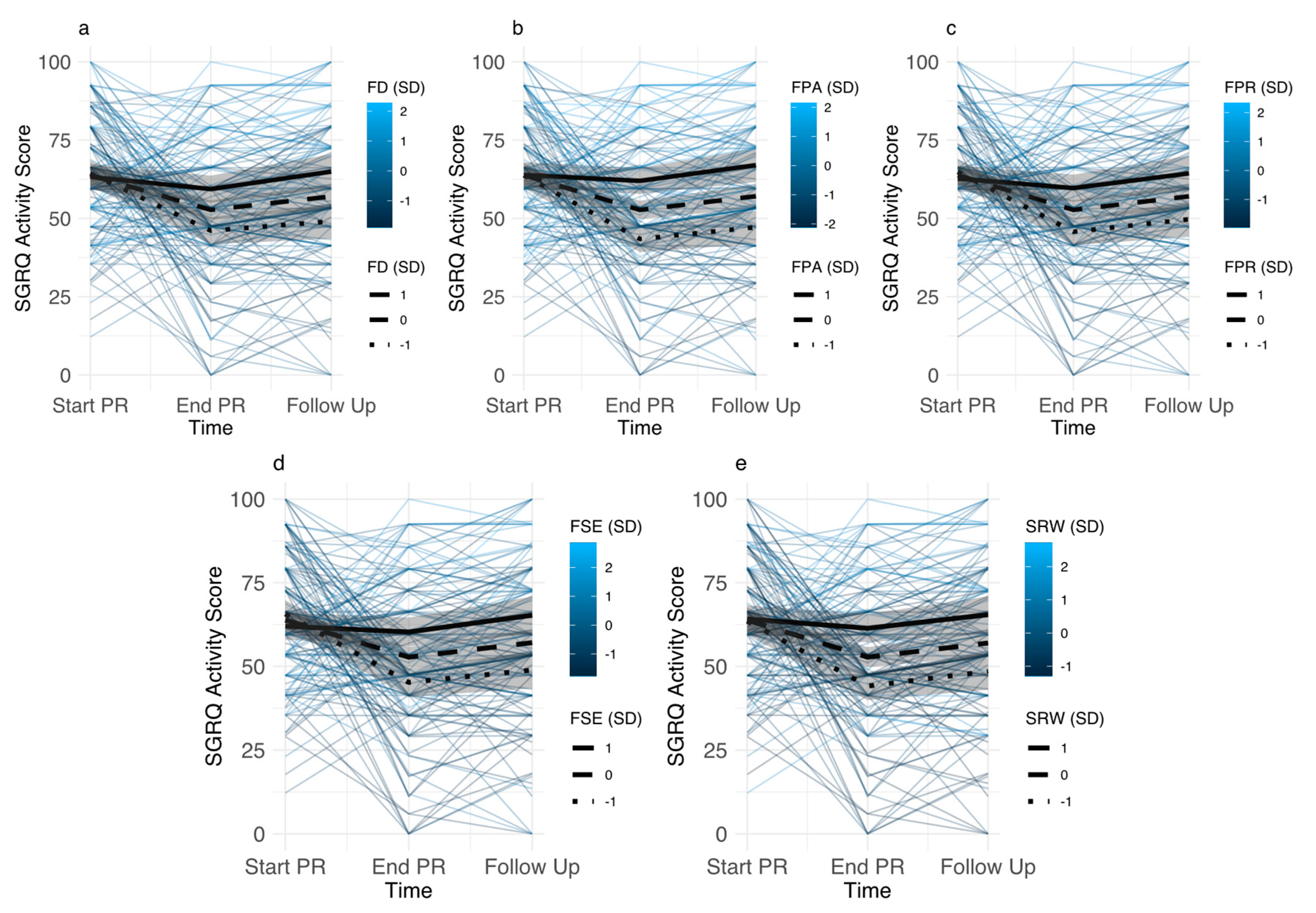
3.3. Impact of Disease-Specific Fears on Pulmonary Rehabilitation Outcomes
3.3.1. Baseline Levels of Disease-Specific Fears
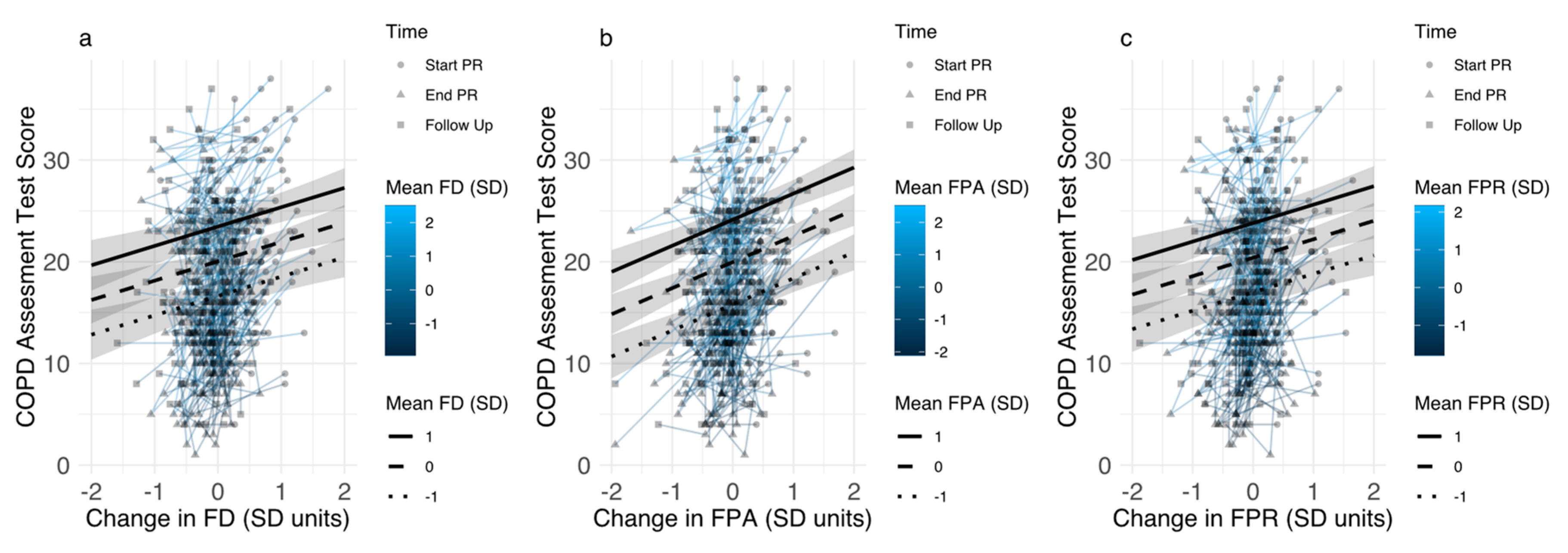
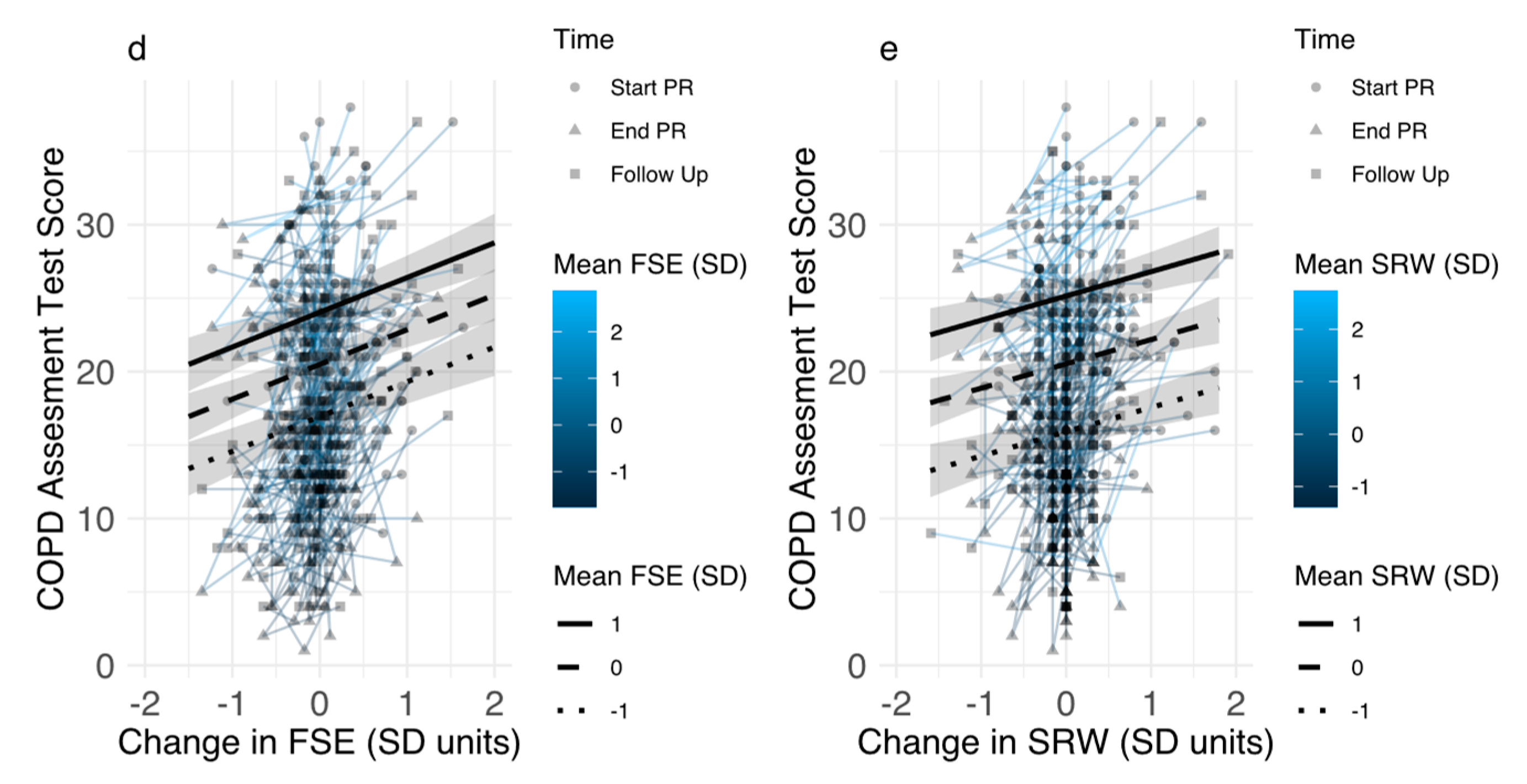
3.3.2. Associations between Changes in Disease-Specific Fears and Pulmonary Rehabilitation Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management and Prevention of COPD. Available online: https://goldcopd.org/gold-reports/ (accessed on 23 August 2019).
- Spruit, M.A.; Pitta, F.; McAuley, E.; ZuWallack, R.L.; Nici, L. Pulmonary Rehabilitation and Physical Activity in Patients with Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2015, 192, 924–933. [Google Scholar] [CrossRef] [PubMed]
- Coventry, P.A.; Hind, D. Comprehensive pulmonary rehabilitation for anxiety and depression in adults with chronic obstructive pulmonary disease: Systematic review and meta-analysis. J. Psychosom. Res. 2007, 63, 551–565. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, B.; Casey, D.; DeVane, D.; Murphy, K.; Murphy, E.; Lacasse, Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2015, CD003793. [Google Scholar] [CrossRef] [PubMed]
- Spruit, M.A.; Singh, S.J.; Garvey, C.; ZuWallack, R.; Nici, L.; Rochester, C.; Hill, K.; Holland, A.E.; Lareau, S.C.; Man, W.D.-C.; et al. An Official American Thoracic Society/European Respiratory Society Statement: Key Concepts and Advances in Pulmonary Rehabilitation. Am. J. Respir. Crit. Care Med. 2013, 188, e13–e64. [Google Scholar] [CrossRef] [PubMed]
- Matte, D.L.; Pizzichini, M.M.; Hoepers, A.T.; Diaz, A.P.; Karloh, M.; Dias, M.; Pizzichini, E. Prevalence of depression in COPD: A systematic review and meta-analysis of controlled studies. Respir. Med. 2016, 117, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Panagioti, M.; Scott, C.; Blakemore, A.; A Coventry, P. Overview of the prevalence, impact, and management of depression and anxiety in chronic obstructive pulmonary disease. Int. J. Chronic Obstr. Pulm. Dis. 2014, 9, 1289–1306. [Google Scholar]
- Ratcliff, C.G.; Barrera, T.L.; Petersen, N.J.; Sansgiry, S.; Kauth, M.R.; Kunik, M.E.; Stanley, M.A.; Cully, J.A. Recognition of anxiety, depression, and PTSD in patients with COPD and CHF: Who gets missed? Gen. Hosp. Psychiatry 2017, 47, 61–67. [Google Scholar] [CrossRef]
- Yohannes, A.M.; Alexopoulos, G.S. Depression and anxiety in patients with COPD. Eur. Respir. Rev. 2014, 23, 345–349. [Google Scholar] [CrossRef]
- Willgoss, T.G.; Yohannes, A.M. Anxiety Disorders in Patients With COPD: A Systematic Review. Respir. Care 2013, 58, 858–866. [Google Scholar]
- Schuler, M.; Strohmayer, M.; Mühlig, S.; Schwaighofer, B.; Wittmann, M.; Faller, H.; Schultz, K. Assessment of depression before and after inpatient rehabilitation in COPD patients: Psychometric properties of the German version of the Patient Health Questionnaire (PHQ-9/PHQ-2). J. Affect. Disord. 2018, 232, 268–275. [Google Scholar] [CrossRef]
- Kim, H.F.S.; Kunik, M.E.; Molinari, V.A.; Hillman, S.L.; Lalani, S.; Orengo, C.A.; Petersen, N.J.; Nahas, Z.; Goodnight-White, S. Functional Impairment in COPD Patients: The Impact of Anxiety and Depression. J. Psychosom. Res. 2000, 41, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Kunik, M.E.; Roundy, K.; Veazey, C.; Souchek, J.; Richardson, P.; Wray, N.P.; Stanley, M.A. Surprisingly High Prevalence of Anxiety and Depression in Chronic Breathing Disorders. Chest 2005, 127, 1205. [Google Scholar] [CrossRef]
- Blakemore, A.; Dickens, C.; Guthrie, E.; Bower, P.; Kontopantelis, E.; Afzal, C.; Coventry, P.A. Depression and anxiety predict health-related quality of life in chronic obstructive pulmonary disease: Systematic review and meta-analysis. Int. J. Chronic Obstr. Pulm. Dis. 2014, 9, 501. [Google Scholar] [CrossRef] [PubMed]
- Schwab, P.; Dhamane, A.D.; Hopson, S.D.; Moretz, C.; Annavarapu, S.; Burslem, K.; Renda, A.; Kaila, S. Impact of comorbid conditions in COPD patients on health care resource utilization and costs in a predominantly Medicare population. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 735. [Google Scholar] [CrossRef] [PubMed]
- Wacker, M.E.; Kitzing, K.; Jörres, R.A.; Leidl, R.; Schulz, H.; Karrasch, S.; Karch, A.; Koch, A.; Vogelmeier, C.F.; Holle, R. The contribution of symptoms and comorbidities to the economic impact of COPD: An analysis of the German COSYCONET cohort. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 3437. [Google Scholar] [CrossRef] [PubMed]
- Laforest, L.; Roche, N.; Devouassoux, G.; Belhassen, M.; Chouaid, C.; Ginoux, M.; Van Ganse, E. Frequency of comorbidities in chronic obstructive pulmonary disease, and impact on all-cause mortality: A population-based cohort study. Respir. Med. 2016, 117, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Divo, M.; Cote, C.; de Torres, J.P.; Casanova, C.; Marin, J.M.; Pinto-Plata, V.; Zulueta, J.; Cabrera, C.; Zagaceta, J.; Hunninghake, G.; et al. Comorbidities and Risk of Mortality in Patients with Chronic Obstructive Pulmonary Disease. Am. J. Respir. Crit. Care Med. 2012, 186, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Lou, P.; Zhu, Y.; Chen, P.; Zhang, P.; Yu, J.; Zhang, N.; Chen, N.; Zhang, L.; Wu, H.; Zhao, J. Prevalence and correlations with depression, anxiety, and other features in outpatients with chronic obstructive pulmonary disease in China: A cross-sectional case control study. BMC Pulm. Med. 2012, 12, 53. [Google Scholar] [CrossRef]
- Von Leupoldt, A.; Taube, K.; Lehmann, K.; Fritzsche, A.; Magnussen, H. The Impact of Anxiety and Depression on Outcomes of Pulmonary Rehabilitation in Patients With COPD. Chest 2011, 140, 730–736. [Google Scholar] [CrossRef]
- Papaioannou, V.E.; Pneumatikos, I.; Maglaveras, N. Association of heart rate variability and inflammatory response in patients with cardiovascular diseases: Current strengths and limitations. Front. Physiol. 2013, 4, 4. [Google Scholar] [CrossRef]
- A Coventry, P.; Gemmell, I.; Todd, C.J. Psychosocial risk factors for hospital readmission in COPD patients on early discharge services: A cohort study. BMC Pulm. Med. 2011, 11, 49. [Google Scholar] [CrossRef] [PubMed]
- Laurin, C.; Moullec, G.; Bacon, S.L.; Lavoie, K.L. Impact of Anxiety and Depression on Chronic Obstructive Pulmonary Disease Exacerbation Risk. Am. J. Respir. Crit. Care Med. 2012, 185, 918–923. [Google Scholar] [CrossRef] [PubMed]
- Pikoula, M.; Quint, J.K.; Nissen, F.; Hemingway, H.; Smeeth, L.; Denaxas, S. Identifying clinically important COPD sub-types using data-driven approaches in primary care population based electronic health records. BMC Med. Inform. Decis. Mak. 2019, 19, 86. [Google Scholar] [CrossRef] [PubMed]
- Khdour, M.R.; Hawwa, A.F.; Kidney, J.C.; Smyth, B.M.; McElnay, J.C. Potential risk factors for medication non-adherence in patients with chronic obstructive pulmonary disease (COPD). Eur. J. Clin. Pharmacol. 2012, 68, 1365–1373. [Google Scholar] [CrossRef] [PubMed]
- Paine, N.J.; Bacon, S.L.; Bourbeau, J.; Tan, W.C.; Lavoie, K.L.; Aaron, S.D.; Chapman, K.R.; FitzGerald, J.M.; Hernandez, P.; Marciniuk, D.D.; et al. Psychological distress is related to poor health behaviours in COPD and non-COPD patients: Evidence from the CanCOLD study. Respir. Med. 2018, 146, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Von Leupoldt, A.; Janssens, T. Could targeting disease specific fear and anxiety improve COPD outcomes? Expert Rev. Respir. Med. 2016, 10, 835–837. [Google Scholar] [CrossRef] [PubMed]
- Wortz, K.; Cade, A.; Menard, J.R.; Lurie, S.; Lykens, K.; Bae, S.; Jackson, B.; Su, F.; Singh, K.; Coultas, D. A qualitative study of patients’ goals and expectations for self-management of COPD. Prim. Care Respir. J. 2012, 21, 384–391. [Google Scholar] [CrossRef] [PubMed]
- De Peuter, S.; Janssens, T.; Van Diest, I.; Stans, L.; Troosters, T.; Decramer, M.; Van den Bergh, O.; Vlaeyen, J.W.S. Dyspnea-related anxiety: The Dutch version of the Breathlessness Beliefs Questionnaire. Chronic Respir. Dis. 2011, 8, 11–19. [Google Scholar] [CrossRef]
- Keil, D.C.; Stenzel, N.M.; Kühl, K.; Vaske, I.; Mewes, R.; Rief, W.; Kenn, K. The impact of chronic obstructive pulmonary disease-related fears on disease-specific disability. Chronic Respir. Dis. 2014, 11, 31–40. [Google Scholar] [CrossRef]
- Vlaeyen, J.W.S.; Crombez, G.; Linton, S.J. The fear-avoidance model of pain. Pain 2016, 157, 1588–1589. [Google Scholar] [CrossRef]
- Lethem, J.; Slade, P.; Troup, J.; Bentley, G. Outline of a fear-avoidance model of exaggerated pain perception—I. Behav. Res. Ther. 1983, 21, 401–408. [Google Scholar] [CrossRef]
- Kühl, K.; Kuhn, C.; Kenn, K.; Rief, W. Der COPD-Angst-Fragebogen (CAF): Ein neues Instrument zur Erfassung krankheitsspezifischer Ängste bei COPD-Patienten. PPmP-Psychother. Psychosom. Med. Psychol. 2011, 61, e1–e9. [Google Scholar]
- Vercoulen, J.H.; Daudey, L.; Molema, J.; Vos, P.J.; Peters, J.B.; Top, M.; Folgering, H. An integral assessment framework of health status in chronic obstructive pulmonary disease (COPD). Int. J. Behav. Med. 2008, 15, 263–279. [Google Scholar] [CrossRef] [PubMed]
- Peters, J.B.; Daudey, L.; Heijdra, Y.F.; Molema, J.; Dekhuijzen, P.N.R.; Vercoulen, J.H. Development of a battery of instruments for detailed measurement of health status in patients with COPD in routine care: The Nijmegen Clinical Screening Instrument. Qual. Life Res. 2009, 18, 901–912. [Google Scholar] [CrossRef] [PubMed]
- Janssens, T.; De Peuter, S.; Stans, L.; Verleden, G.; Troosters, T.; Decramer, M.; Van den Bergh, O. Dyspnea Perception in COPD Association Between Anxiety, Dyspnea-Related Fear, and Dyspnea in a Pulmonary Rehabilitation Program. Chest 2011, 140, 618–625. [Google Scholar] [CrossRef]
- Reijnders, T.; Schuler, M.; Wittmann, M.; Jelusic, D.; Troosters, T.; Janssens, W.; Stenzel, N.M.; Schultz, K.; von Leupoldt, A. The Impact of Disease-Specific Fears on Outcome Measures of Pulmonary Rehabilitation in Patients with COPD. Respir. Med. 2018, 146, 87–95. [Google Scholar] [CrossRef]
- Esser, R.W.; Stoeckel, M.C.; Kirsten, A.; Watz, H.; Taube, K.; Lehmann, K.; Petersen, S.; Magnussen, H.; Von Leupoldt, A. Structural Brain Changes in Patients With COPD. Chest 2016, 149, 426–434. [Google Scholar] [CrossRef]
- Harris, D.; Hayter, M.; Allender, S. Improving the uptake of pulmonary rehabilitation in patients with COPD: Qualitative study of experiences and attitudes. Br. J. Gen. Pract. 2008, 58, 703–710. [Google Scholar] [CrossRef]
- Peters, J.B.; Boer, L.M.; Molema, J.; Heijdra, Y.F.; Prins, J.B.; Vercoulen, J.H. Integral Health Status-Based Cluster Analysis in Moderate–Severe COPD Patients Identifies Three Clinical Phenotypes: Relevant for Treatment as Usual and Pulmonary Rehabilitation. Int. J. Behav. Med. 2017, 24, 571–583. [Google Scholar] [CrossRef]
- Stenzel, N.M.; Vaske, I.; Kühl, K.; Kenn, K.; Rief, W. Prediction of end-of-life fears in COPD—Hoping for the best but preparing for the worst. Psychol. Health 2015, 30, 1–18. [Google Scholar] [CrossRef]
- Herigstad, M.; Faull, O.K.; Hayen, A.; Evans, E.; Hardinge, F.M.; Wiech, K.; Pattinson, K.T. Treating breathlessness via the brain: Changes in brain activity over a course of pulmonary rehabilitation. Eur. Respir. J. 2017, 50, 1701029. [Google Scholar] [CrossRef] [PubMed]
- Solomon, B.K.; Wilson, K.G.; Henderson, P.R.; Poulin, P.A.; Kowal, J.; McKim, D.A. A Breathlessness Catastrophizing Scale for chronic obstructive pulmonary disease. J. Psychosom. Res. 2015, 79, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Zoeckler, N.; Kenn, K.; Kuehl, K.; Stenzel, N.; Rief, W. Illness perceptions predict exercise capacity and psychological well-being after pulmonary rehabilitation in COPD patients. J. Psychosom. Res. 2014, 76, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Fischer, M.J.; Scharloo, M.; Abbink, J.; van ’t Hul, A.; van Ranst, D.; Rudolphus, A.; Weinman, J.; Rabe, K.F.; Kaptein, A.A. Concerns About Exercise Are Related to Walk Test Results in Pulmonary Rehabilitation for Patients with COPD. Int. J. Behav. Med. 2012, 19, 39–47. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Geidl, W.; Semrau, J.; Streber, R.; Lehbert, N.; Wingart, S.; Tallner, A.; Wittmann, M.; Wagner, R.; Schultz, K.; Pfeifer, K. Effects of a brief, pedometer-based behavioral intervention for individuals with COPD during inpatient pulmonary rehabilitation on 6-week and 6-month objectively measured physical activity: Study protocol for a randomized controlled trial. Trials 2017, 18, 396. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.R. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [PubMed]
- Quanjer, P.H.; Stanojevic, S.; Cole, T.J.; Baur, X.; Hall, G.L.; Culver, B.H.; Enright, P.L.; Hankinson, J.L.; Ip, M.S.; Zheng, J.; et al. multi-ethnic reference values for spirometry for the 3–95 year age range: The global lung function 2012 equations. Eur. Respir. J. 2012, 40, 1324–1343. [Google Scholar] [CrossRef] [PubMed]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS Statement Guidelines for the Six-Minute Walk Test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef]
- Wingart, S.; Lehbert, N.; Krämer, B.; Huber, V.; Fuchs, S.; Wittmann, M.; Jelusic, D.; Schuler, M.; Schultz, K. Is a double 6-min walk test required as part of the routine assessment of pulmonary rehabilitation in COPD patients? Eur. Respir. J. 2014, 44, P1293. [Google Scholar]
- Jenkins, S.C. 6-Minute walk test in patients with COPD: Clinical applications in pulmonary rehabilitation. Physiotherapy 2007, 93, 175–182. [Google Scholar]
- Jones, P.W.; Harding, G.; Berry, P.; Wiklund, I.; Chen, W.-H.; Leidy, N.K. Development and first validation of the COPD Assessment Test. Eur. Respir. J. 2009, 34, 648–654. [Google Scholar] [CrossRef]
- Ringbaek, T.; Martinez, G.; Lange, P. A Comparison of the Assessment of Quality of Life with CAT, CCQ, and SGRQ in COPD Patients Participating in Pulmonary Rehabilitation. COPD J. Chronic Obstr. Pulm. Dis. 2012, 9, 12–15. [Google Scholar] [CrossRef] [PubMed]
- Gupta, N.; Pinto, L.M.; Morogan, A.; Bourbeau, J. The COPD assessment test: A systematic review. Eur. Respir. J. 2014, 44, 873–884. [Google Scholar] [CrossRef] [PubMed]
- Alma, H.; de Jong, C.; Jelusic, D.; Wittmann, M.; Schuler, M.; Blok, B.F.; Kocks, J.; Schultz, K.; van der Molen, T. Health status instruments for patients with COPD in pulmonary rehabilitation: Defining a minimal clinically important difference. NPJ Prim. Care Resp. Med. 2016, 26, 16041. [Google Scholar] [CrossRef] [PubMed]
- Von Leupoldt, A.; Reijnders, T.; Schuler, M.; Wittmann, M.; Jelusic, D.; Schultz, K. Validity of a Self-administered Questionnaire Version of the Transition Dyspnea Index in Patients with COPD. COPD J. Chronic Obstr. Pulm. Dis. 2017, 14, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Witek, T.; Mahler, D. Minimal important difference of the transition dyspnoea index in a multinational clinical trial. Eur. Respir. J. 2003, 21, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Mahler, D.A.; Weinberg, D.H.; Wells, C.K.; Feinstein, A.R. The Measurement of Dyspnea: Contents, Interobserver Agreement, and Physiologic Correlates of Two New Clinical Indexes. Chest 1984, 85, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Jones, P.W.; Quirk, F.H.; Baveystock, C.M. The St George’s Respiratory Questionnaire. Respir. Med. 1991, 85, 25–31. [Google Scholar] [CrossRef]
- Gräfe, K.; Zipfel, S.; Herzog, W.; Löwe, B. Screening psychischer Störungen mit dem “Gesundheitsfragebogen für Patienten (PHQ-D)”. Diagnostica 2004, 50, 171–181. [Google Scholar] [CrossRef]
- Bates, D.; Mächler, M.; Bolker, B.; Walker, S. Fitting Linear Mixed-Effects Models Using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Lenth, R.; Singmann, H.; Love, J.; Buerkner, P.; Herve, M. Emmeans: Estimated Marginal Means, aka Least-Squares Means. Available online: https://CRAN.R-project.org/package=emmeans (accessed on 23 August 2019).
- Kuznetsova, A.; Brockhoff, P.B.; Christensen, R.H.B. lmerTest: Tests in Linear Mixed Effects Models. Available online: https://CRAN.R-project.org/package=lmerTest (accessed on 21 August 2019).
- Carrieri-Kohlman, V.; Gormley, J.M.; Douglas, M.K.; Paul, S.M.; Stulbarg, M.S. Exercise Training Decreases Dyspnea and the Distress and Anxiety Associated with It. Chest 1996, 110, 1526–1535. [Google Scholar] [CrossRef]
- Wadell, K.; Webb, K.A.; Preston, M.E.; Amornputtisathaporn, N.; Samis, L.; Patelli, J.; Guenette, J.A.; O’Donnell, D.E. Impact of Pulmonary Rehabilitation on the Major Dimensions of Dyspnea in COPD. COPD J. Chronic Obstr. Pulm. Dis. 2013, 10, 425–435. [Google Scholar] [CrossRef] [PubMed]
- McNicholas, W.T.; Verbraecken, J.; Marín, J.M. Sleep disorders in COPD: The forgotten dimension. Eur. Respir. Rev. 2013, 22, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Scharf, S.M.; Maimon, N.; Simon-Tuval, T.; Bernhard-Scharf, B.J.; Reuveni, H.; Tarasiuk, A. Sleep quality predicts quality of life in chronic obstructive pulmonary disease. Int. J. Chronic Obstruct. Pulm. Dis. 2011, 6, 1. [Google Scholar] [CrossRef] [PubMed]
- Zeidler, M.R.; Martin, J.L.; Kleerup, E.C.; Schneider, H.; Mitchell, M.N.; Hansel, N.N.; Sundar, K.; Schotland, H.; Basner, R.C.; Wells, J.M.; et al. Sleep disruption as a predictor of quality of life among patients in the subpopulations and intermediate outcome measures in COPD study (SPIROMICS). Sleep 2018, 41, zsy044. [Google Scholar] [CrossRef] [PubMed]
- Reijnders, T.; Schuler, M.; Jelusic, D.; Troosters, T.; Janssens, W.; Schultz, K.; Leupoldt, A. von The Impact of Loneliness on Outcomes of Pulmonary Rehabilitation in Patients with COPD. COPD J. Chronic Obstr. Pulm. Dis. 2018, 15, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Halding, A.-G.; Wahl, A.; Heggdal, K. ‘Belonging’. ‘Patients’ experiences of social relationships during pulmonary rehabilitation. Disabil. Rehabil. 2010, 32, 1272–1280. [Google Scholar] [CrossRef] [PubMed]
- Spruit, M.A.; Pitta, F.; Garvey, C.; ZuWallack, R.L.; Roberts, C.M.; Collins, E.G.; Goldstein, R.; McNamara, R.; Surpas, P.; Atsuyoshi, K.; et al. Differences in content and organisational aspects of pulmonary rehabilitation programmes. Eur. Respir. J. 2014, 43, 1326–1337. [Google Scholar] [CrossRef] [PubMed]
- Desveaux, L.; Janaudis-Ferreira, T.; Goldstein, R.; Brooks, D. An International Comparison of Pulmonary Rehabilitation: A Systematic Review. COPD J. Chronic Obstr. Pulm. Dis. 2015, 12, 144–153. [Google Scholar] [CrossRef]
- Livermore, N.; Sharpe, L.; McKenzie, D. Prevention of panic attacks and panic disorder in COPD. Eur. Respir. J. 2010, 35, 557–563. [Google Scholar] [CrossRef]
- Heslop-Marshall, K.; Baker, C.; Carrick-Sen, D.; Newton, J.; Echevarria, C.; Stenton, C.; Jambon, M.; Gray, J.; Pearce, K.; Burns, G.; et al. Randomised controlled trial of cognitive behavioural therapy in COPD. ERJ Open Res. 2018, 4, 00094–2018. [Google Scholar] [CrossRef]
- Barrera, T.L.; Grubbs, K.M.; Kunik, M.E.; Teng, E.J. A Review of Cognitive Behavioral Therapy for Panic Disorder in Patients with Chronic Obstructive Pulmonary Disease: The Rationale for Interoceptive Exposure. J. Clin. Psychol. Med. Settings 2014, 21, 144–154. [Google Scholar] [CrossRef] [PubMed]
- Wouters, E.F.; Wouters, B.B.; Augustin, I.M.; Houben-Wilke, S.; Vanfleteren, L.E.; Franssen, F.M. Personalised pulmonary rehabilitation in COPD. Eur. Respir. Rev. 2018, 27, 170125. [Google Scholar] [CrossRef] [PubMed]
- Agusti, A.; Bel, E.; Thomas, M.; Vogelmeier, C.; Brusselle, G.; Holgate, S.; Humbert, M.; Jones, P.; Gibson, P.G.; Vestbo, J.; et al. Treatable traits: Toward precision medicine of chronic airway diseases. Eur. Respir. J. 2016, 47, 410–419. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | N | Data | Association with Baseline Disease-Specific Fears p < 0.05 |
|---|---|---|---|
| Age, mean (SD) | 146 | 57.5 (4.4) | ns |
| Gender, n (%) | 146 | ns | |
| Males | 98 (67) | ||
| Females | 48 (33) | ||
| Smoking status, n (%) | 146 | SRW | |
| Active smokers | 66 (45) | ||
| Non-smokers | 80 (55) | ||
| Pack years, mean (SD) | 142 | 44.4 (22.8) | ns |
| Exacerbation history (past year), n (%) | 140 | FD, FP, FSE | |
| 0 or 1 exacerbation | 68 (49) | ||
| 2 or more exacerbations | 72 (51) | ||
| Inhaled Medication, n (%) | 146 | ns | |
| ICS + LABA + LAMA | 64 (44) | ||
| ICS + LABA/LAMA | 15 (10) | ||
| LABA + LAMA | 50 (34) | ||
| LABA/LAMA monotherapy | 10 (7) | ||
| SABA or no inhaled medication | 7 (5) | ||
| FEV1% predicted, mean (SD) | 142 | 55.4 (16.6) | FD, FPA, FSE |
| 6MWT, mean (SD) | 144 | 460.8 (102.5) | FD, FPA, FSE |
| Baseline PHQ-9, mean (SD) | 138 | 7.9 (5.4) | FD, FPA, FP, FSE, SRW |
| Start PR | End PR | Follow-Up | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Mean | SE | Mean | SE | Mean | SE | F | df | p | |
| Disease-Specific Fears (CAF) | ||||||||||
| Fear of Social Exclusion | 10.74 a | 0.542 | 9.03 b | 0.555 | 10.09 a | 0.582 | 8.376 | (2, 146.16) | 0.0004 | |
| Fear of Dyspnea | 9.86 a | 0.44 | 6.67 b | 0.372 | 6.72 b | 0.337 | 53.203 | (2, 146) | <0.0001 | |
| Fear of Physical Activity | 10.4 a | 0.425 | 7.75 b | 0.413 | 8.22 b | 0.414 | 31.614 | (2, 145.98) | <0.0001 | |
| Fear of Progression | 10.90 a | 0.489 | 8.91 b | 0.488 | 9.25 b | 0.507 | 14.391 | (2, 146) | <0.0001 | |
| Sleep-Related Worries | 2.51 a | 0.17 | 1.89 b | 0.158 | 2.18 ab | 0.16 | 10.759 | (2, 146) | <0.0001 | |
| Symptom Burden (CAT) | 20.8 a | 0.579 | 15.2 b | 0.603 | 18.3 c | 0.646 | 70.322 | (2, 145.98) | <0.0001 | |
| Quality of Life (SGRQ) | ||||||||||
| Symptoms | 61.1 a | 1.81 | 36.6 b | 1.91 | 52.9 c | 2.03 | 35.853 | (2,142.28) | <0.0001 | |
| Activity | 63.8 a | 1.47 | 52.7 b | 1.62 | 57.0 b | 2.15 | 16.289 | (2, 144.91) | <0.0001 | |
| Impact | 41.8 a | 1.37 | 27.7 b | 1.44 | 31.8 c | 1.81 | 39.083 | (2, 145.69) | <0.0001 | |
| Transition Dyspnea Index (TDI) | 1.92 a | 0.107 | 1.04 b | 0.135 | 45.484 | (1, 169.9) | <0.0001 | |||
| Depressive Symptoms (PHQ-9) | 7.9 a | 0.422 | 5.02 b | 0.406 | 7.12 a | 0.407 | 31.592 | (2, 143.24) | <0.0001 | |
| 6 Min walking test Distance (m) | 461 a | 6.68 | 542 b | 9.24 | 81.711 | (1, 226.17) | <0.0001 | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Janssens, T.; Van de Moortel, Z.; Geidl, W.; Carl, J.; Pfeifer, K.; Lehbert, N.; Wittmann, M.; Schultz, K.; von Leupoldt, A. Impact of Disease-Specific Fears on Pulmonary Rehabilitation Trajectories in Patients with COPD. J. Clin. Med. 2019, 8, 1460. https://doi.org/10.3390/jcm8091460
Janssens T, Van de Moortel Z, Geidl W, Carl J, Pfeifer K, Lehbert N, Wittmann M, Schultz K, von Leupoldt A. Impact of Disease-Specific Fears on Pulmonary Rehabilitation Trajectories in Patients with COPD. Journal of Clinical Medicine. 2019; 8(9):1460. https://doi.org/10.3390/jcm8091460
Chicago/Turabian StyleJanssens, Thomas, Zora Van de Moortel, Wolfgang Geidl, Johannes Carl, Klaus Pfeifer, Nicola Lehbert, Michael Wittmann, Konrad Schultz, and Andreas von Leupoldt. 2019. "Impact of Disease-Specific Fears on Pulmonary Rehabilitation Trajectories in Patients with COPD" Journal of Clinical Medicine 8, no. 9: 1460. https://doi.org/10.3390/jcm8091460
APA StyleJanssens, T., Van de Moortel, Z., Geidl, W., Carl, J., Pfeifer, K., Lehbert, N., Wittmann, M., Schultz, K., & von Leupoldt, A. (2019). Impact of Disease-Specific Fears on Pulmonary Rehabilitation Trajectories in Patients with COPD. Journal of Clinical Medicine, 8(9), 1460. https://doi.org/10.3390/jcm8091460