Do Younger Patients with Muscle-Invasive Bladder Cancer have Better Outcomes?

 ,
, 
Abstract
1. Introduction
2. Material and Methods
2.1. Patient Population
2.2. Follow-Up Regimen
2.3. Statistical Analysis
3. Results
3.1. Association of Age with Clinical–Pathological Characteristics
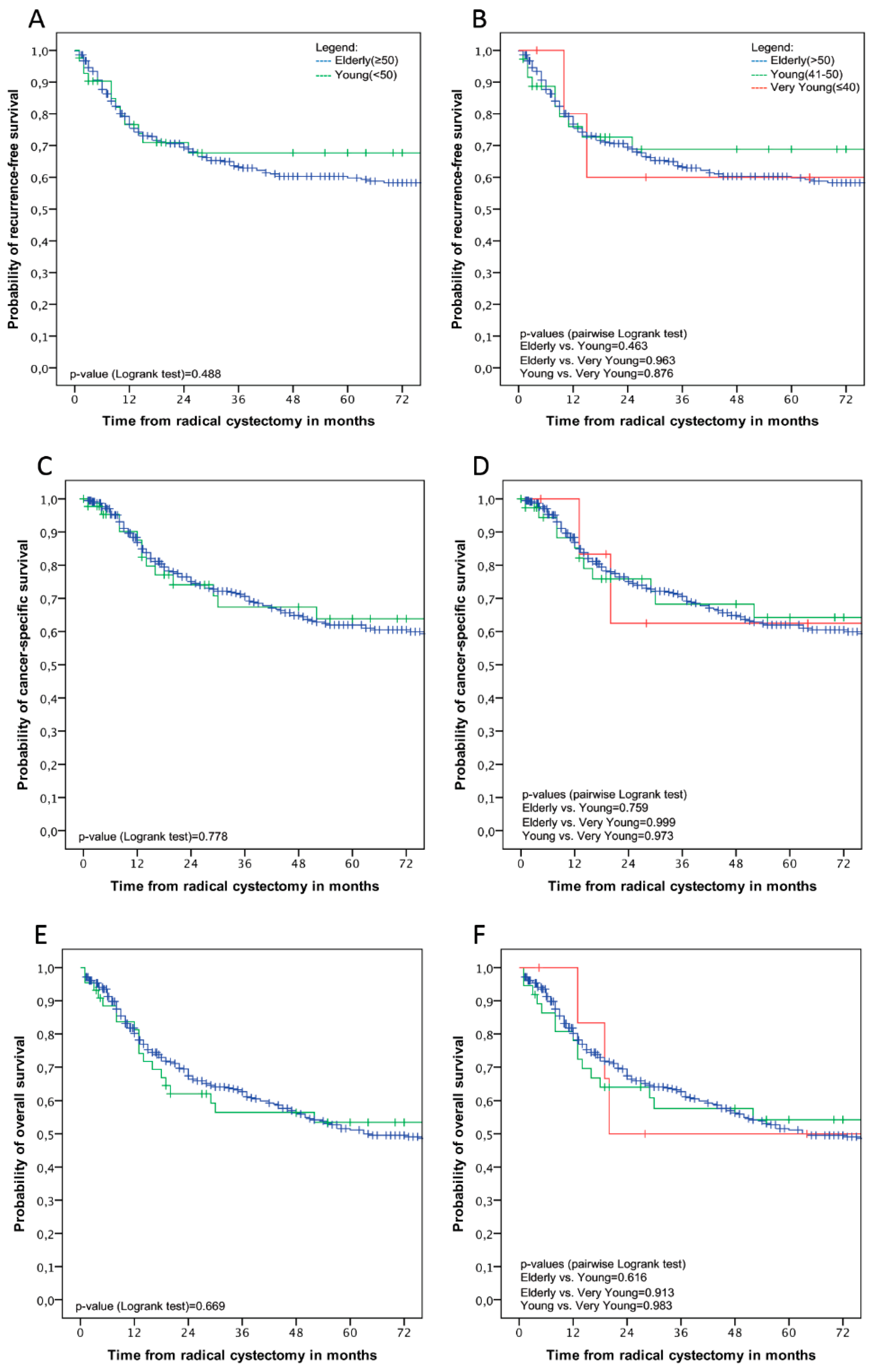
3.2. Association of Age with Disease Recurrence and Survival Outcomes
3.3. Risk Factor Analyses for Disease Recurrence and Survival Outcomes
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2019. CA Cancer J. Clin. 2019, 69, 7–34. [Google Scholar] [CrossRef] [PubMed]
- Guancial, E.A.; Roussel, B.; Bergsma, D.P.; Bylund, K.C.; Sahasrabudhe, D.; Messing, E.; Mohile, S.G.; Fung, C. Bladder cancer in the elderly patient: Challenges and solutions. Clin. Interv. Aging 2015, 10, 939–949. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Shariat, S.F.; Milowsky, M.; Droller, M.J. Bladder cancer in the elderly. Urol. Oncol. 2009, 27, 653–667. [Google Scholar] [CrossRef] [PubMed]
- Organization, W.H. World Health Statistics 2018: Monitoring Health for the SDGs; WHO: Geneva, Switzerland, 2018. [Google Scholar]
- Abdollah, F.; Gandaglia, G.; Thuret, R.; Schmitges, J.; Tian, Z.; Jeldres, C.; Passoni, N.M.; Briganti, A.; Shariat, S.F.; Perrotte, P.; et al. Incidence, survival and mortality rates of stage-specific bladder cancer in United States: A trend analysis. Cancer Epidemiol. 2013, 37, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Leal, J.; Luengo-Fernandez, R.; Sullivan, R.; Witjes, J.A. Economic Burden of Bladder Cancer Across the European Union. Eur. Urol. 2016, 69, 438–447. [Google Scholar] [CrossRef] [PubMed]
- Rink, M.; Crivelli, J.J.; Shariat, S.F.; Chun, F.K.; Messing, E.M.; Soloway, M.S. Smoking and Bladder Cancer: A Systematic Review of Risk and Outcomes. Eur. Urol. Focus 2015, 1, 17–27. [Google Scholar] [CrossRef]
- Rink, M.; Furberg, H.; Zabor, E.C.; Xylinas, E.; Babjuk, M.; Pycha, A.; Lotan, Y.; Karakiewicz, P.I.; Novara, G.; Robinson, B.D.; et al. Impact of smoking and smoking cessation on oncologic outcomes in primary non-muscle-invasive bladder cancer. Eur. Urol. 2013, 63, 724–732. [Google Scholar] [CrossRef]
- Rink, M.; Zabor, E.C.; Furberg, H.; Xylinas, E.; Ehdaie, B.; Novara, G.; Babjuk, M.; Pycha, A.; Lotan, Y.; Trinh, Q.D.; et al. Impact of smoking and smoking cessation on outcomes in bladder cancer patients treated with radical cystectomy. Eur. Urol. 2013, 64, 456–464. [Google Scholar] [CrossRef]
- Denzinger, S.; Fritsche, H.M.; Otto, W.; Blana, A.; Wieland, W.F.; Burger, M. Early versus deferred cystectomy for initial high-risk pT1G3 urothelial carcinoma of the bladder: Do risk factors define feasibility of bladder-sparing approach? Eur. Urol. 2008, 53, 146–152. [Google Scholar] [CrossRef]
- Lara, J.; Brunson, A.; Keegan, T.H.; Malogolowkin, M.; Pan, C.-X.; Yap, S.; deVere White, R. Determinants of survival for adolescents and young adults with urothelial bladder cancer: Results from the California Cancer Registry. J. Urol. 2016, 196, 1378–1382. [Google Scholar] [CrossRef]
- Soave, A.; Dahlem, R.; Hansen, J.; Weisbach, L.; Minner, S.; Engel, O.; Kluth, L.A.; Chun, F.K.; Shariat, S.F.; Fisch, M.; et al. Gender-specific outcomes of bladder cancer patients: A stage-specific analysis in a contemporary, homogenous radical cystectomy cohort. Eur. J. Surg. Oncol. 2015, 41, 368–377. [Google Scholar] [CrossRef] [PubMed]
- Soave, A.; Schmidt, S.; Dahlem, R.; Minner, S.; Engel, O.; Kluth, L.A.; John, L.M.; Hansen, J.; Schmid, M.; Sauter, G.; et al. Does the extent of variant histology affect oncological outcomes in patients with urothelial carcinoma of the bladder treated with radical cystectomy? Urol. Oncol. 2015, 33, 21.e21–21.e29. [Google Scholar] [CrossRef] [PubMed]
- Rink, M.; Fajkovic, H.; Cha, E.K.; Gupta, A.; Karakiewicz, P.I.; Chun, F.K.; Lotan, Y.; Shariat, S.F. Death certificates are valid for the determination of cause of death in patients with upper and lower tract urothelial carcinoma. Eur. Urol. 2012, 61, 854–855. [Google Scholar] [CrossRef] [PubMed]
- Institute, N.C. Closing the Gap: Research and Care Imperatives for Adolescents and Young Adults with Cancer; Institute, N.C.: Bethesda, MD, USA, 2006. [Google Scholar]
- Feng, H.; Zhang, W.; Li, J.; Lu, X. Different patterns in the prognostic value of age for bladder cancer-specific survival depending on tumor stages. Am. J. Cancer Res. 2015, 5, 2090. [Google Scholar] [PubMed]
- Nayak, J.G.; Gore, J.L.; Holt, S.K.; Wright, J.L.; Mossanen, M.; Dash, A. Patient-centered risk stratification of disposition outcomes following radical cystectomy. Urol. Oncol. Semin. Orig. Investig. 2016, 34, 235.e217–235.e223. [Google Scholar] [CrossRef] [PubMed]
- Isbarn, H.; Jeldres, C.; Zini, L.; Perrotte, P.; Baillargeon-Gagne, S.; Capitanio, U.; Shariat, S.F.; Arjane, P.; Saad, F.; McCormack, M.; et al. A population based assessment of perioperative mortality after cystectomy for bladder cancer. J. Urol. 2009, 182, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Chromecki, T.F.; Mauermann, J.; Cha, E.K.; Svatek, R.S.; Fajkovic, H.; Karakiewicz, P.I.; Lotan, Y.; Tilki, D.; Bastian, P.J.; Volkmer, B.G.; et al. Multicenter validation of the prognostic value of patient age in patients treated with radical cystectomy. World J. Urol. 2012, 30, 753–759. [Google Scholar] [CrossRef] [PubMed]
- Shariat, S.F.; Sfakianos, J.P.; Droller, M.J.; Karakiewicz, P.I.; Meryn, S.; Bochner, B.H. The effect of age and gender on bladder cancer: A critical review of the literature. BJU Int. 2010, 105, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Noon, A.P.; Martinsen, J.I.; Catto, J.W.F.; Pukkala, E. Occupation and Bladder Cancer Phenotype: Identification of Workplace Patterns That Increase the Risk of Advanced Disease Beyond Overall Incidence. Eur. Urol. Focus 2018, 4, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Crivelli, J.J.; Xylinas, E.; Kluth, L.A.; Rieken, M.; Rink, M.; Shariat, S.F. Effect of smoking on outcomes of urothelial carcinoma: A systematic review of the literature. Eur. Urol. 2014, 65, 742–754. [Google Scholar] [CrossRef]
- Mathieu, R.; Lucca, I.; Klatte, T.; Babjuk, M.; Shariat, S.F. Trimodal therapy for invasive bladder cancer: Is it really equal to radical cystectomy? Curr. Opin. Urol. 2015, 25, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Ploussard, G.; Daneshmand, S.; Efstathiou, J.A.; Herr, H.W.; James, N.D.; Rodel, C.M.; Shariat, S.F.; Shipley, W.U.; Sternberg, C.N.; Thalmann, G.N.; et al. Critical Analysis of Bladder Sparing with Trimodal Therapy in Muscle-invasive Bladder Cancer: A Systematic Review. Eur. Urol. 2014, 66, 120–137. [Google Scholar] [CrossRef] [PubMed]
- Knoedler, J.; Frank, I. Organ-sparing surgery in urology: Partial cystectomy. Curr. Opin. Urol. 2015, 25, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Katafigiotis, I.; Sfoungaristos, S.; Martini, A.; Stravodimos, K.; Anastasiou, I.; Mykoniatis, I.; Duvdevani, M.; Constantinides, C. Bladder Cancer to Patients Younger than 30 Years: A Retrospective Study and Review of the Literature. Urol. J. 2017, 84, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Telli, O.; Sarici, H.; Ozgur, B.C.; Doluoglu, O.G.; Sunay, M.M.; Bozkurt, S.; Eroglu, M. Urothelial cancer of bladder in young versus older adults: Clinical and pathological characteristics and outcomes. Kaohsiung J. Med. Sci. 2014, 30, 466–470. [Google Scholar] [CrossRef] [PubMed]
- Yossepowitch, O.; Dalbagni, G. Transitional cell carcinoma of the bladder in young adults: Presentation, natural history and outcome. J. Urol. 2002, 168, 61–66. [Google Scholar] [CrossRef]
- Lee, R.K.; Abol-Enein, H.; Artibani, W.; Bochner, B.; Dalbagni, G.; Daneshmand, S.; Fradet, Y.; Hautmann, R.E.; Lee, C.T.; Lerner, S.P.; et al. Urinary diversion after radical cystectomy for bladder cancer: Options, patient selection, and outcomes. BJU Int. 2014, 113, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.M.; Martin, J.W.; Jefferson, F.A.; Sidhom, D.A.; Piranviseh, K.; Huang, M.; Nguyen, N.; Chang, J.; Ziogas, A.; Anton-Culver, H.; et al. Racial and Socioeconomic Disparities in Bladder Cancer Survival: Analysis of the California Cancer Registry. Clin. Genitourin. Cancer 2019. [Google Scholar] [CrossRef]
- Gild, P.; Wankowicz, S.A.; Sood, A.; von Landenberg, N.; Friedlander, D.F.; Alanee, S.; Chun, F.K.H.; Fisch, M.; Menon, M.; Trinh, Q.D.; et al. Racial disparity in quality of care and overall survival among black vs. white patients with muscle-invasive bladder cancer treated with radical cystectomy: A national cancer database analysis. Urol. Oncol. 2018, 36, 469.e1–469.e11. [Google Scholar] [CrossRef]
- Dobruch, J.; Daneshmand, S.; Fisch, M.; Lotan, Y.; Noon, A.P.; Resnick, M.J.; Shariat, S.F.; Zlotta, A.R.; Boorjian, S.A. Gender and Bladder Cancer: A Collaborative Review of Etiology, Biology, and Outcomes. Eur. Urol. 2016, 69, 300–310. [Google Scholar] [CrossRef]
- Svatek, R.S.; Shariat, S.F.; Lasky, R.E.; Skinner, E.C.; Novara, G.; Lerner, S.P.; Fradet, Y.; Bastian, P.J.; Kassouf, W.; Karakiewicz, P.I.; et al. The effectiveness of off-protocol adjuvant chemotherapy for patients with urothelial carcinoma of the urinary bladder. Clin. Cancer Res. 2010, 16, 4461–4467. [Google Scholar] [CrossRef] [PubMed]
- Goossens-Laan, C.A.; Leliveld, A.M.; Verhoeven, R.H.; Kil, P.J.; de Bock, G.H.; Hulshof, M.C.; de Jong, I.J.; Coebergh, J.W. Effects of age and comorbidity on treatment and survival of patients with muscle-invasive bladder cancer. Int. J. Cancer 2014, 135, 905–912. [Google Scholar] [CrossRef] [PubMed]
- Megwalu, I.I.; Vlahiotis, A.; Radwan, M.; Piccirillo, J.F.; Kibel, A.S. Prognostic impact of comorbidity in patients with bladder cancer. Eur. Urol. 2008, 53, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Fairey, A.S.; Jacobsen, N.E.; Chetner, M.P.; Mador, D.R.; Metcalfe, J.B.; Moore, R.B.; Rourke, K.F.; Todd, G.T.; Venner, P.M.; Voaklander, D.C.; et al. Associations between comorbidity, and overall survival and bladder cancer specific survival after radical cystectomy: Results from the Alberta Urology Institute Radical Cystectomy database. J. Urol. 2009, 182, 85–92. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| All | Young (≤50) | Elderly (≥51) | p-Value | p-Value | ||
|---|---|---|---|---|---|---|
| ≤40 | 41–50 | ≥51 | ≤50 vs. ≥51 | ≤40 vs. 41–50 vs. ≥51 | ||
| Patients, n | 669 | 8 | 39 | 622 | - | - |
| Gender (%) | 0.85 | 0.98 | ||||
| Male | 520 (77.7) | 6 (75.0) | 30 (76.9) | 484 (77.8) | ||
| Female | 149 (22.3) | 2 (25.0) | 9 (23.1) | 138 (22.2) | ||
| ASA (%) | <0.001 | <0.001 | ||||
| 1 | 52 (7.8) | 4 (50.0) | 7 (18.0) | 41 (6.6) | ||
| 2 | 386 (57.7) | 3 (37.5) | 27 (69.2) | 356 (57.2) | ||
| 3 | 225 (33.6) | 1 (12.5) | 3 (7.7) | 221 (35.5) | ||
| 4 | 6 (0.9) | 0 (0) | 2 (5.1) | 4 (0.7) | ||
| Pathological Tumor Stage (%) | 0.92 | 0.34 | ||||
| pT0 | 73 (10.9) | 3 (37.5) | 4 (10.3) | 66 (10.6) | ||
| pTa | 26 (3.9) | 0 (0) | 1 (2.6) | 25 (4.0) | ||
| pTis | 66 (9.9) | 0 (0) | 3 (7.7) | 63 (10.1) | ||
| pT1 | 74 (11.1) | 1 (12.5) | 4 (10.3) | 69 (11.1) | ||
| pT2 | 132 (19.7) | 0 (0) | 10 (25.6) | 122 (19.6) | ||
| pT3 | 182 (27.2) | 4 (50.0) | 8 (20.5) | 170 (27.3) | ||
| pT4 | 116 (17.3) | 0 (0) | 9 (23.1) | 107 (17.2) | ||
| Pathological Tumor Grade (%) | 0.58 | 0.42 | ||||
| No grading (pT0) | 73 (10.9) | 3 (37.5) | 4 (10.3) | 66 (10.6) | ||
| G2 | 65 (9.7) | 1 (12.5) | 6 (15.4) | 58 (9.3) | ||
| G3 | 531 (79.4) | 4 (50.0) | 29 (74.3) | 498 (80.1) | ||
| Concomitant carcinoma in situ (%) | 0.051 | 0.12 | ||||
| Absent | 424 (63.4) | 7 (87.5) | 29 (74.4) | 388 (62.4) | ||
| Present | 245 (36.6) | 1 (12.5) | 10 (25.6) | 234 (37.6) | ||
| Lymph node status (%) | 0.91 | 0.58 | ||||
| pN0 | 479 (71.6) | 7 (87.5) | 27 (69.2) | 445 (71.5) | ||
| pN+ | 190 (28.4) | 1 (12.5) | 12 (30.8) | 177 (28.5) | ||
| Margin status (%) | 0.94 | 0.99 | ||||
| R0 | 586 (87.6) | 7 (87.5) | 34 (87.2) | 545 (87.6) | ||
| R+ | 83 (12.4) | 1 (12.5) | 5 (12.8) | 77 (12.4) | ||
| Lymphovascular invasion (%) | 0.52 | 0.62 | ||||
| L0 | 455 (68.0) | 6 (75) | 24 (61.5) | 425 (68.3) | ||
| L1 | 214 (32.0) | 2 (25) | 15 (38.5) | 197 (31.7) | ||
| Adjuvant Chemotherapy (%) | 0.089 | 0.21 | ||||
| No | 522 (78.0) | 6 (75.0) | 26 (66.7) | 490 (78.8) | ||
| Yes | 147 (22.0) | 2 (25.0) | 13 (33.3) | 132 (21.2) | ||
| Age Stratifications | RFS | CSS | OS | ||||||
|---|---|---|---|---|---|---|---|---|---|
| HR | 95%CI | p-Value | HR | 95%CI | p-Value | HR | 95%CI | p-Value | |
| Continuous age | 1.017 | 1.002–1.032 | 0.029 | 1.023 | 1.007–1.039 | 0.005 | 1.030 | 1.016–1.044 | <0.001 |
| Median Age | 1.454 | 1.095–1.932 | 0.010 | 1.550 | 1.150–2.088 | 0.004 | 1.663 | 1.299–2.129 | <0.001 |
| Age ≤50 vs. >50 | 1.227 | 0.684–2.202 | 0.49 | 1.084 | 0.616–1.909 | 0.78 | 1.107 | 0.693–1.767 | 0.67 |
| Age (three categories) | |||||||||
| ≤40 vs. >50 | 0.818 | 0.179–3.733 | 0.80 | 0.910 | 0.202–4.111 | 0.90 | 0.832 | 0.242–2.858 | 0.77 |
| 41–50 vs. >50 | 1.035 | 0.257–4.170 | 0.96 | 1.001 | 0.248–4.038 | 0.99 | 0.946 | 0.303–2.955 | 0.92 |
| Age (Tertiles) | |||||||||
| first vs. third tertile | 1.242 | 0.861–1.793 | 0.25 | 1.364 | 0.926–2.008 | 0.12 | 1.576 | 1.137–2.185 | 0.006 |
| second vs. third tertile | 1.699 | 1.151–2.507 | 0.008 | 1.931 | 1.278–2.917 | 0.002 | 2.194 | 1.546–3.112 | <0.001 |
| Age Stratifications | RFS | CSS | OS | ||||||
|---|---|---|---|---|---|---|---|---|---|
| HR | 95%CI | p-Value | HR | 95%CI | p-Value | HR | 95%CI | p-Value | |
| Continuous Age | 1.019 | 1.003–1.035 | 0.018 | 1.025 | 1.008–1.042 | 0.004 | 1.030 | 1.016–1.045 | 0.000 |
| Median age | 1.472 | 1.081–2.005 | 0.014 | 1.553 | 1.124–2.146 | 0.008 | 1.596 | 1.225–2.080 | 0.001 |
| Age (Tertiles) | |||||||||
| first vs. third tertile | 1.339 | 0.914–1.962 | 0.13 | 1.545 | 1.033–2.312 | 0.034 | 1.728 | 1.230–2.428 | 0.002 |
| second vs. third tertile | 1.862 | 1.211–2.864 | 0.005 | 2.085 | 1.328–3.276 | 0.001 | 2.256 | 1.541–3.304 | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Janisch, F.; Yu, H.; Vetterlein, M.W.; Dahlem, R.; Engel, O.; Fisch, M.; Shariat, S.F.; Soave, A.; Rink, M. Do Younger Patients with Muscle-Invasive Bladder Cancer have Better Outcomes? J. Clin. Med. 2019, 8, 1459. https://doi.org/10.3390/jcm8091459
Janisch F, Yu H, Vetterlein MW, Dahlem R, Engel O, Fisch M, Shariat SF, Soave A, Rink M. Do Younger Patients with Muscle-Invasive Bladder Cancer have Better Outcomes? Journal of Clinical Medicine. 2019; 8(9):1459. https://doi.org/10.3390/jcm8091459
Chicago/Turabian StyleJanisch, Florian, Hang Yu, Malte W. Vetterlein, Roland Dahlem, Oliver Engel, Margit Fisch, Shahrokh F. Shariat, Armin Soave, and Michael Rink. 2019. "Do Younger Patients with Muscle-Invasive Bladder Cancer have Better Outcomes?" Journal of Clinical Medicine 8, no. 9: 1459. https://doi.org/10.3390/jcm8091459
APA StyleJanisch, F., Yu, H., Vetterlein, M. W., Dahlem, R., Engel, O., Fisch, M., Shariat, S. F., Soave, A., & Rink, M. (2019). Do Younger Patients with Muscle-Invasive Bladder Cancer have Better Outcomes? Journal of Clinical Medicine, 8(9), 1459. https://doi.org/10.3390/jcm8091459