The Effect of Tapered Abutments on Marginal Bone Level: A Retrospective Cohort Study

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion and Exclusion Criteria
2.2. Data Collection and Analysis
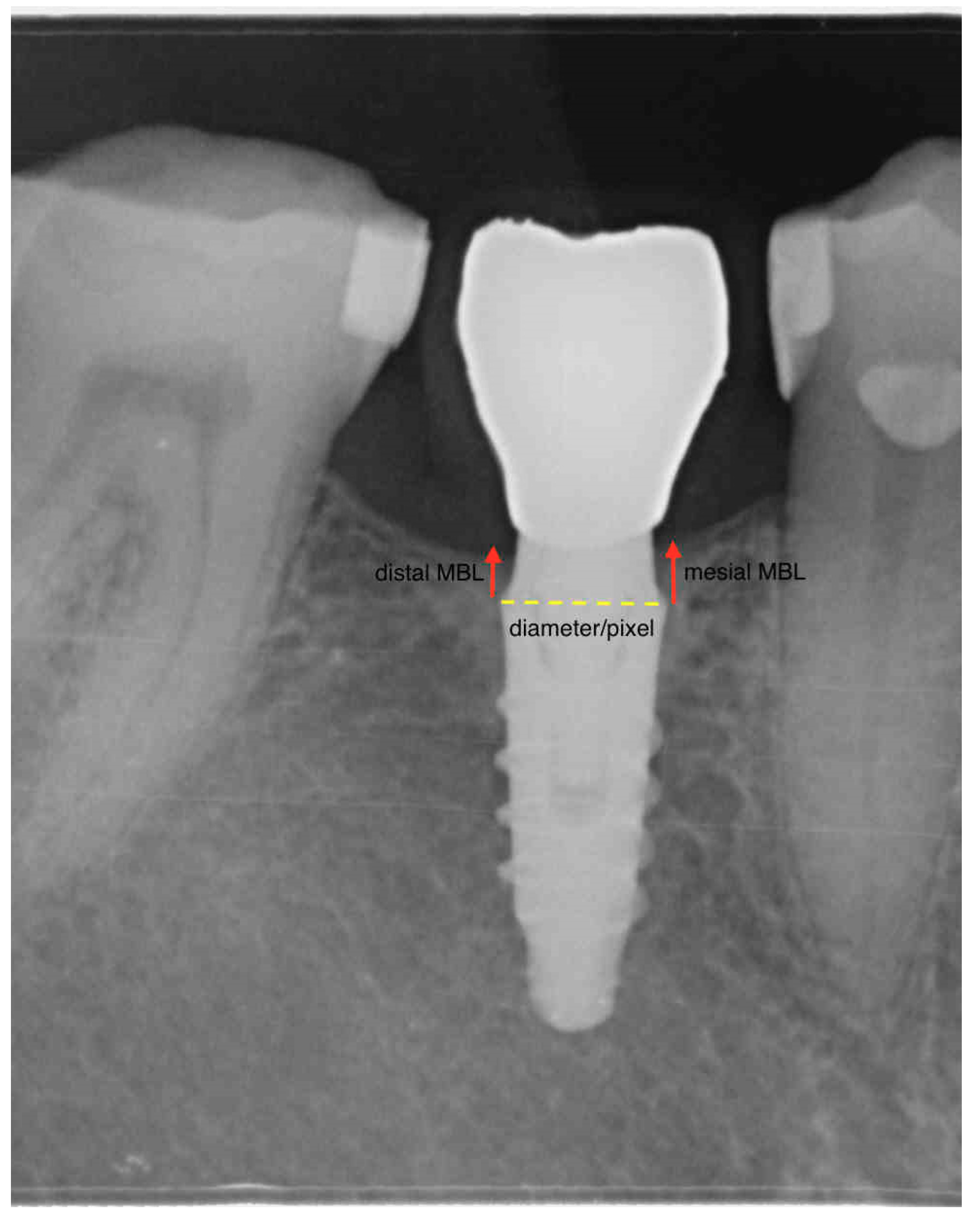
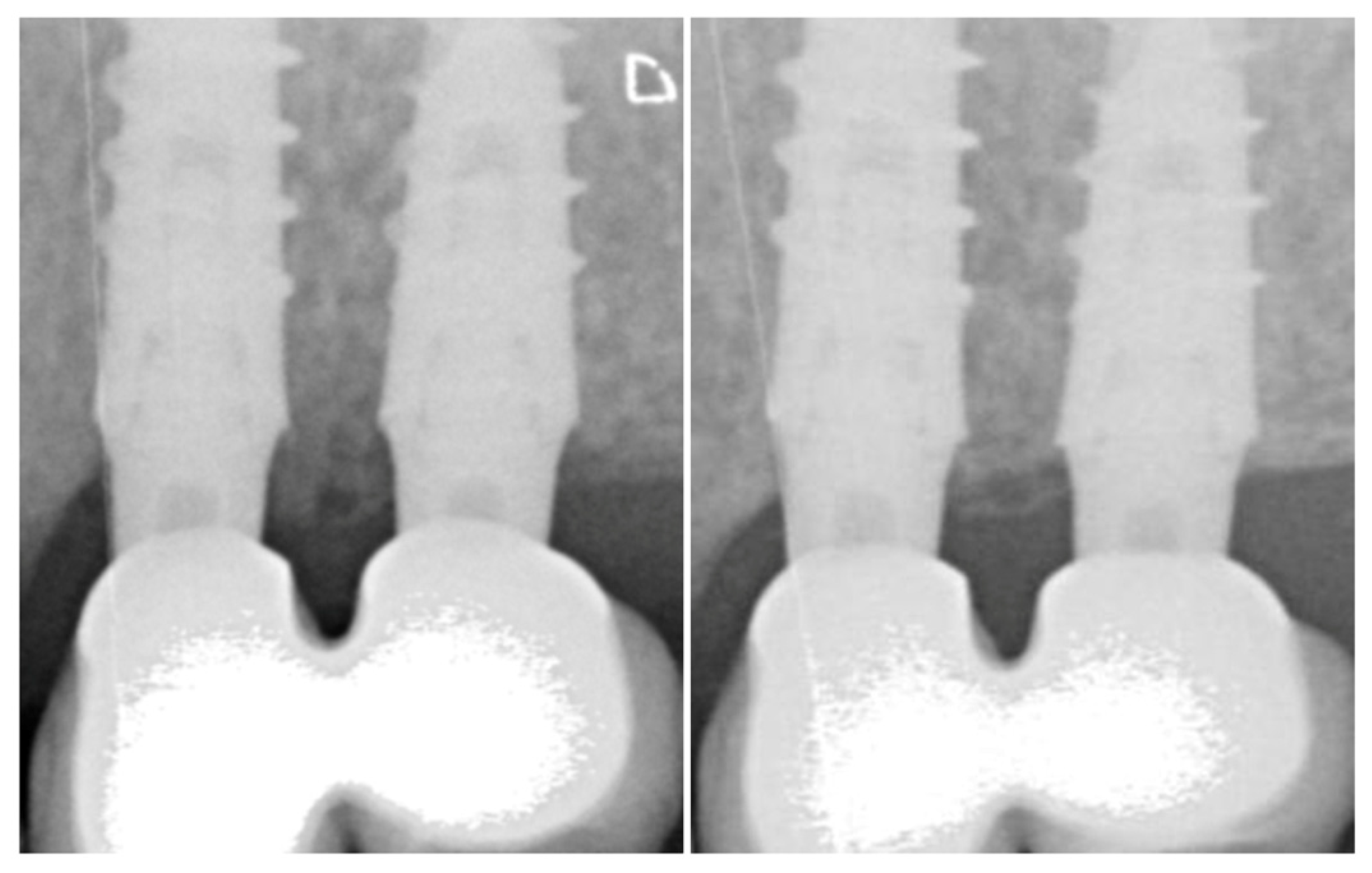
2.3. Radiologic Marginal Bone Level Evaluation
2.4. Dichotomous Outcomes
- Implant failure was identified with eventual implant mobility or persistent infection, and whenever the implant presented signs and symptoms that led to the implant removal.
- Survival and success rates (SRs and CSRs, respectively) for implants, were calculated according to the criteria defined by Buser et al. in 1997 [13]. Successful implants were those showing a mean radiological peri-implant bone resorption within 1.5 mm during the first year of loading, and less than 0.2 mm/year during the following years.
2.5. Statistical Analysis
3. Results
3.1. Study Population
3.2. Survival and Adverse Events
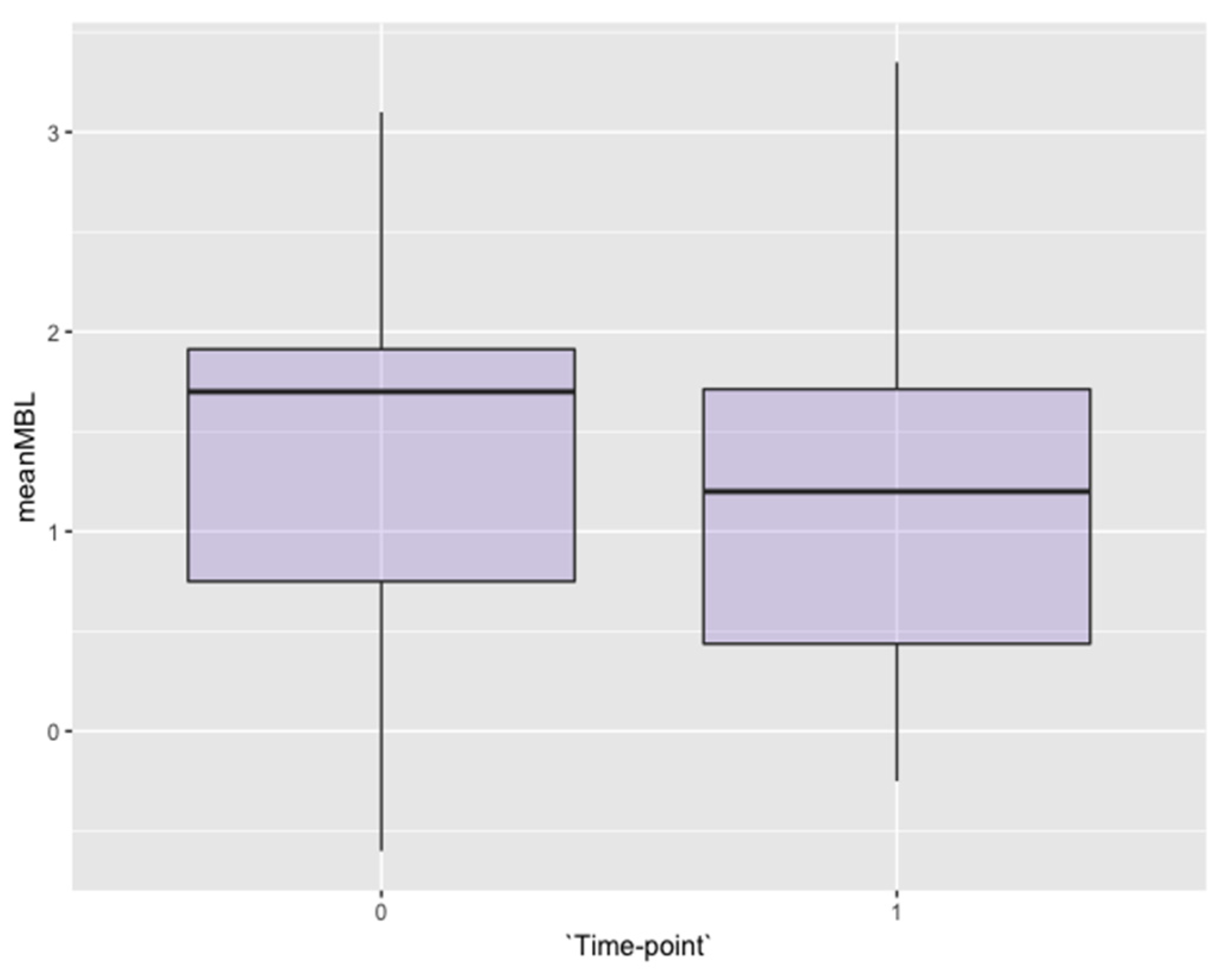
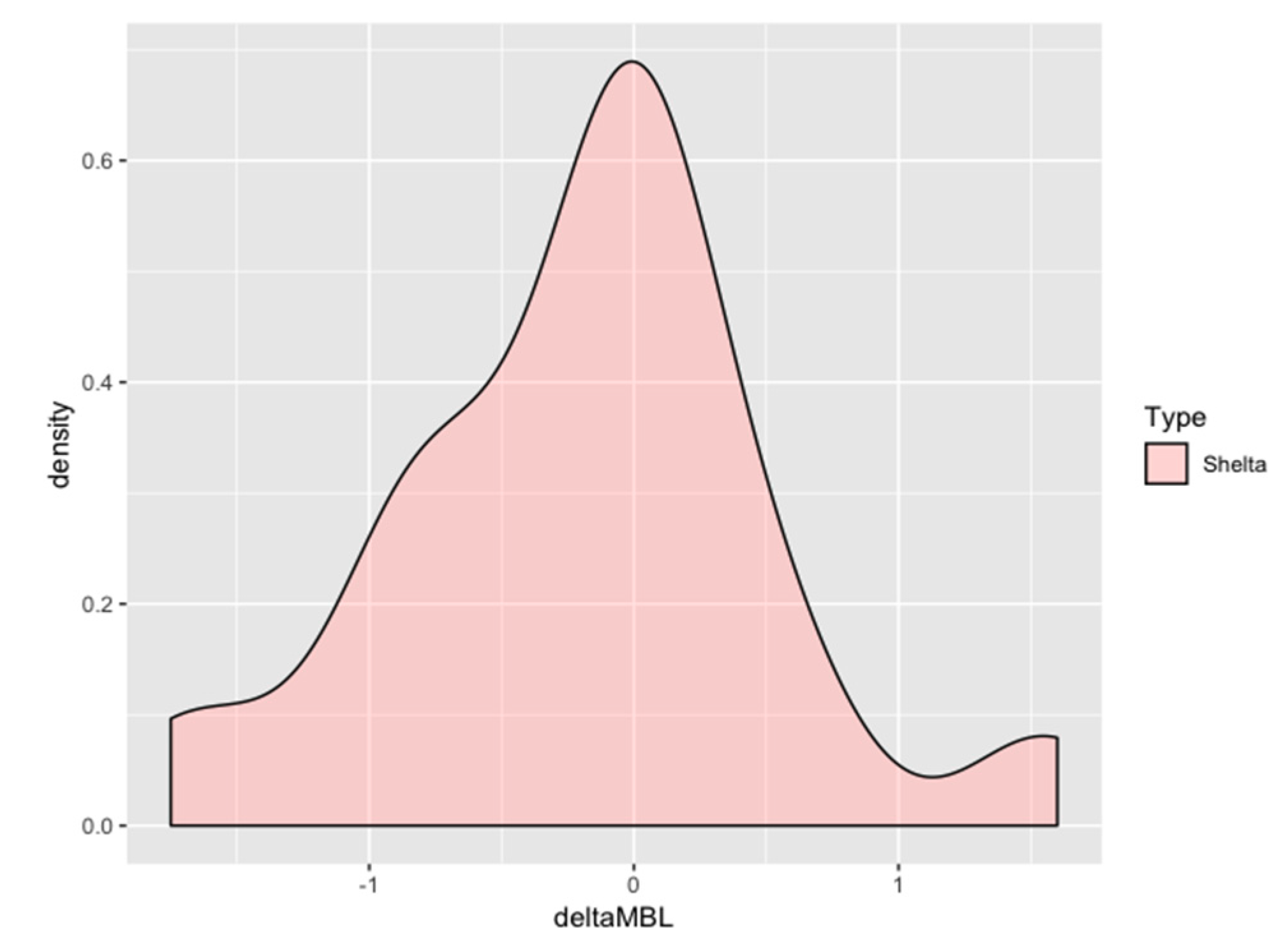
3.3. Bone Levels
3.4. Secondary Outcomes: Soft Tissues
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Oh, T.J.; Yoon, J.; Misch, C.E.; Wang, H.L. The causes of early implant bone loss: Myth or science? J. Periodontol. 2002, 73, 322–333. [Google Scholar] [CrossRef] [PubMed]
- Piattelli, A.; Vrespa, G.; Petrone, G.; Iezzi, G.; Annibali, S.; Scarano, A. Role of the micro-gap between implant and abutment: A retrospective histologic evaluation in monkeys. J. Periodontol. 2003, 74, 346–352. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.C.; Han, C.H.; Lee, K.W. A 1-year radiographic evaluation of marginal bone around dental implants. Int. J. Oral Maxillofac. Implants 1996, 11, 811–818. [Google Scholar] [PubMed]
- Astrand, P.; Engquist, B.; Dahlgren, S.; Gröndahl, K.; Engquist, E.; Feldmann, H. Astra Tech and Brånemark system implants: A 5-year prospective study of marginal bone reactions. Clin. Oral Implant. Res. 2004, 15, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Ericsson, I.; Persson, L.G.; Berglundh, T.; Marinello, C.P.; Lindhe, J.; Klinge, B. Different types of inflammatory reactions in peri-implant soft tissues. J. Clin. Periodontol. 1995, 22, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Quaranta, A.; Teles, R.P. The microbiota associated with implants restored with platform switching: A preliminary report. J. Periodontol. 2010, 81, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Canullo, L.; Pellegrini, G.; Allievi, C.; Trombelli, L.; Annibali, S.; Dellavia, C. Soft tissues around long-term platform switching implant restorations: A histological human evaluation. Preliminary results. J. Clin. Periodontol. 2011, 38, 86–94. [Google Scholar] [CrossRef]
- Buser, D.; Wittneben, J.; Bornstein, M.M.; Grütter, L.; Chappuis, V.; Belser, U.C. Stability of contour augmentation and esthetic outcomes of implant-supported single crowns in the esthetic zone: 3-year results of a prospective study with early implant placement postextraction. J. Periodontol. 2011, 82, 342–349. [Google Scholar] [CrossRef]
- Östman, P.O.; Hellman, M.; Sennerby, L. Ten years later. Results from a prospective single-centre clinical study on 121 oxidized (TiUnite™) Brånemark implants in 46 patients. Clin. Implant Dent. Relat. Res. 2012, 14, 852–860. [Google Scholar] [CrossRef]
- Finelle, G.; Papadimitriou, D.E.V.; Souza, A.B.; Katebi, N.; Gallucci, G.O.; Araújo, M.G. Peri-implant soft tissue and marginal bone adaptation on implant with non-matching healing abutments: Micro-CT analysis. Clin. Oral Implant. Res. 2015, 26, e42–e46. [Google Scholar] [CrossRef]
- Rodríguez, X.; Navajas, A.; Vela, X.; Fortuño, A.; Jimenez, J.; Nevins, M. Arrangement of Peri-implant Connective Tissue Fibers Around Platform-Switching Implants with Conical Abutments and Its Relationship to the Underlying Bone: A Human Histologic Study. Int. J. Periodontics Restor. Dent. 2016, 36, 533–540. [Google Scholar]
- Canullo, L.; Tallarico, M.; Pradies, G.; Marinotti, F.; Loi, I.; Cocchetto, R. Soft and hard tissue response to an implant with a convergent collar in the esthetic area: Preliminary report at 18 months. Int. J. Esthet. Dent. 2017, 12, 306–323. [Google Scholar] [PubMed]
- Buser, D.; Mericske-Stern, R.; Bernard, J.P.; Behneke, A.; Behneke, N.; Hirt, H.P.; Belser, U.C.; Lang, N.P. Long-term evaluation of non-submerged ITI implants. Part 1: 8-year life table analysis of a prospective multi-center study with 2359 implants. Clin. Oral Implant. Res. 1997, 8, 161–172. [Google Scholar] [CrossRef]
- Hermann, J.S.; Cochran, D.L.; Nummikoski, P.V.; Buser, D. Crestal bone changes around titanium implants. A radiographic evaluation of unloaded nonsubmerged and submerged implants in the canine mandible. J. Periodontol. 1997, 68, 1117–1130. [Google Scholar] [CrossRef] [PubMed]
- Hermann, J.S.; Schoolfield, J.D.; Schenk, R.K.; Buser, D.; Cochran, D.L. Influence of the size of the microgap on crestal bone changes around titanium implants. A histometric evaluation of unloaded non-submerged implants in the canine mandible. J. Periodontol. 2001, 72, 1372–1383. [Google Scholar] [CrossRef] [PubMed]
- Welander, M.; Abrahamsson, I.; Berglundh, T. The mucosal barrier at implant abutments of different materials. Clin. Oral Implant. Res. 2008, 19, 635–641. [Google Scholar]
- Qian, J.; Wennerberg, A.; Albrektsson, T. Reasons for marginal bone loss around oral implants. Clin. Implant. Dent. Relat. Res. 2012, 14, 792–807. [Google Scholar] [CrossRef]
- Sanz-Sánchez, I.; Sanz-Martín, I.; Carrillo de Albornoz, A.; Figuero, E.; Sanz, M. Biological effect of the abutment material on the stability of peri-implant marginal bone levels: A systematic review and meta-analysis. Clin. Oral Implant. Res. 2018, 29 (Suppl. 18), 124–144. [Google Scholar] [CrossRef]
- Albrektsson, T.; Buser, D.; Sennerby, L. Crestal bone loss and oral implants. Clin. Implant. Dent. Relat. Res. 2012, 14, 783–791. [Google Scholar] [CrossRef]
- Schwarz, F.; Hegewald, A.; Becker, J. Impact of implant-abutment connection and positioning of the machined collar/microgap on crestal bone level changes: A systematic review. Clin. Oral Implant. Res. 2014, 225, 417–425. [Google Scholar] [CrossRef]
- Valles, C.; Rodríguez-Ciurana, X.; Clementini, M.; Baglivo, M.; Paniagua, B.; Nart, J. Influence of subcrestal implant placement compared with equicrestal position on the peri-implant hard and soft tissues around platform-switched implants: A systematic review and meta-analysis. Clin. Oral Investig. 2018, 22, 555–570. [Google Scholar] [CrossRef] [PubMed]
- Khayat, P.G.; Hallage, P.G.; Toledo, R.A. An investigation of 131 consecutively placed wide screw-vent implants. Int. J. Oral Maxillofac. Implant. 2001, 16, 827–832. [Google Scholar]
- Davarpanah, M.; Martinez, H.; Tecucianu, J.F. Apical-coronal implant position: Recent surgical proposals. Technical note. Int. J. Oral Maxillofac. Implant. 2000, 15, 865–872. [Google Scholar]
- Flores-Guillen, J.; Álvarez-Novoa, C.; Barbieri, G.; Martín, C.; Sanz, M. Five-year outcomes of a randomized clinical trial comparing bone-level implants with either submerged or transmucosal healing. J. Clin. Periodontol. 2018, 45, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Messias, A.; Nicolau, P.; Guerra, F. Titanium dental implants with different collar design and surface modifications: A systematic review on survival rates and marginal bone levels. Clin. Oral Implant. Res. 2019, 30, 20–48. [Google Scholar] [CrossRef] [PubMed]
- Cocchetto, R.; Canullo, L. The “hybrid abutment”: A new design for implant cemented restorations in the esthetic zones. Int. J. Esthet. Dent. 2015, 10, 186–208. [Google Scholar] [PubMed]
- Rodríguez-Ciurana, X.; Vela-Nebot, X.; Segalà-Torres, M.; Calvo-Guirado, J.L.; Cambra, J.; Méndez-Blanco, V.; Tarnow, D.P. The effect of interimplant distance on the height of the interimplant bone crest when using platform-switched implants. Int. J. Periodontics Restor. Dent. 2008, 29, 141–151. [Google Scholar]
- Galindo-Moreno, P.; León-Cano, A.; Ortega-Oller, I.; Monje, A.; Suárez, F.; ÓValle, F.; Spinato, S.; Catena, A. Prosthetic Abutment Height is a Key Factor in Peri-implant Marginal Bone Loss. J. Dent. Res. 2014, 93, 80S–85S. [Google Scholar] [CrossRef]
- De Bruyn, H.; Vandeweghe, S.; Ruyffelaert, C.; Cosyn, J.; Sennerby, L. Radiographic evaluation of modern oral implants with emphasis on crestal bone level and relevance to peri-implant health. Periodontol 2000, 62, 256–270. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Male | Female | Total | |
|---|---|---|---|
| Number of Patients | 7 | 13 | 20 |
| Number of Implants | 9 | 27 | 36 |
| Mean Age | 56.2 ± 10.2 | ||
| Age Range | 39–76 |
| Time-point | Mesial MBL | Distal MBL | Mean MBL | Delta MBL | p-value |
|---|---|---|---|---|---|
| Mean MBL in function by year, mm (per implant analysis) and statistical significance of time-effect. | |||||
| Overall | |||||
| Baseline | 1.47 ± 0.87 | 1.30 ± 1.01 | 1.39 ± 0.91 | ||
| 1-year | 1.28 ± 0.98 | 1.04 ± 0.92 | 1.16 ± 0.91 | −0.18 ± 0.72 | 0.01 |
| Mandible | |||||
| Baseline | 0.90 ± 0.76 | 0.55 ± 0.87 | 0.72 ± 0.77 | ||
| 1-year | 0.76 ± 0.67 | 0.47 ± 0.61 | 0.61 ± 0.60 | −0.10 ± 0.29 | 0.19 |
| Sub-plot factor analysis for “Mandible vs. Maxilla relative treatment effect” <MBL ~ jaw p-value 6.58 × 10−7 | |||||
| Maxilla | |||||
| Baseline | 1.72 ± 0.81 | 1.63 ± 0.89 | 1.68 ± 0.72 | ||
| 1-year | 1.51 ± 1.02 | 1.29 ± 0.92 | 1.40 ± 0.93 | −0.22 ± 0.84 | 0.06 |
| Sub-plot factor analysis for “Abutment Height treatment effect” <MBL ~ abutment height p-value 0.05 | |||||
| Time-point | mesial MBL | distal MBL | mean MBL | delta MBL | p-value |
| 4 mm | |||||
| Baseline | 1.31 ± 0.96 | 0.97 ± 0.98 | 1.15 ± 0.94 | ||
| 1-year | 1.08 ± 0.91 | 0.77 ± 1.03 | 0.93 ± 0.93 | −0.20 ± 0.83 | 0.36 |
| 5 mm | |||||
| Baseline | 1.54 ± 0.86 | 1.52 ± 1.03 | 1.53 ± 0.92 | ||
| 1-year | 1.34 ± 1.08 | 1.16 ± 0.86 | 1.25 ± 0.94 | −0.20 ± 0.70 | 0.17 |
| 6 mm | |||||
| Baseline | 1.80 ± 0.69 | 1.43 ± 0.80 | 1.62 ± 0.70 | ||
| 1-year | 1.87 ± 0.35 | 1.53 ± 0.56 | 1.70 ± 0.43 | 0.08 ± 0.34 | 0.05 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marconcini, S.; Giammarinaro, E.; Covani, U.; Mijiritsky, E.; Vela, X.; Rodríguez, X. The Effect of Tapered Abutments on Marginal Bone Level: A Retrospective Cohort Study. J. Clin. Med. 2019, 8, 1305. https://doi.org/10.3390/jcm8091305
Marconcini S, Giammarinaro E, Covani U, Mijiritsky E, Vela X, Rodríguez X. The Effect of Tapered Abutments on Marginal Bone Level: A Retrospective Cohort Study. Journal of Clinical Medicine. 2019; 8(9):1305. https://doi.org/10.3390/jcm8091305
Chicago/Turabian StyleMarconcini, Simone, Enrica Giammarinaro, Ugo Covani, Eitan Mijiritsky, Xavier Vela, and Xavier Rodríguez. 2019. "The Effect of Tapered Abutments on Marginal Bone Level: A Retrospective Cohort Study" Journal of Clinical Medicine 8, no. 9: 1305. https://doi.org/10.3390/jcm8091305
APA StyleMarconcini, S., Giammarinaro, E., Covani, U., Mijiritsky, E., Vela, X., & Rodríguez, X. (2019). The Effect of Tapered Abutments on Marginal Bone Level: A Retrospective Cohort Study. Journal of Clinical Medicine, 8(9), 1305. https://doi.org/10.3390/jcm8091305