Body Weight Effects on Extra-Osseous Subtalar Arthroereisis

 , ,
, ,
Abstract
1. Introduction
2. Experimental Section
2.1. Patient Criteria
2.2. Preoperative Preparation and Postoperative Assessment
2.3. Study Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Bernasconi, A.; Lintz, F.; Sadile, F. The role of arthroereisis of the subtalar joint for flatfoot in children and adults. EFORT Open Rev. 2017, 2, 438–446. [Google Scholar] [CrossRef] [PubMed]
- Ozan, F.; Dogar, F.; Gencer, K.; Koyuncu, S.; Vatansever, F.; Duygulu, F.; Altay, T. Symptomatic flexible flatfoot in adults: Subtalar arthroereisis. Ther. Clin. Risk Manag. 2015, 11, 1597–1602. [Google Scholar] [CrossRef] [PubMed]
- Tong, J.W.; Kong, P.W. Medial Longitudinal Arch Development of Children Aged 7 to 9 Years: Longitudinal Investigation. Phys. Ther. 2016, 96, 1216–1224. [Google Scholar] [CrossRef]
- Kubo, H.; Lipp, C.; Hufeland, M.; Ruppert, M.; Westhoff, B.; Krauspe, R.; Pilge, H. Outcome after subtalar screw arthroereisis in children with flexible flatfoot depends on time of treatment: Midterm results of 95 cases. J. Orthop. Sci. 2019. [Google Scholar] [CrossRef]
- Vulcano, E.; Maccario, C.; Myerson, M.S. How to approach the pediatric flatfoot. World J. Orthop. 2016, 7, 1–7. [Google Scholar] [CrossRef][Green Version]
- Faldini, C.; Mazzotti, A.; Panciera, A.; Perna, F.; Stefanini, N.; Giannini, S. Bioabsorbable implants for subtalar arthroereisis in pediatric flatfoot. Musculoskelet. Surg. 2018, 102, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Miao, X.D.; Wu, Y.P.; Zhang, X.F.; Zhang, Q. Therapeutic Outcomes of Kalix II in Treating Juvenile Flexible Flatfoot. Orthop. Surg. 2017, 9, 20–27. [Google Scholar] [CrossRef] [PubMed]
- Faldini, C.; Mazzotti, A.; Panciera, A.; Persiani, V.; Pardo, F.; Pardo, F.; Perna, F.; Giannini, S. Patient-perceived outcomes after subtalar arthroereisis with bioabsorbable implants for flexible flatfoot in growing age: A 4-year follow-up study. Eur. J. Orthop. Surg. Traumatol. 2018, 28, 707–712. [Google Scholar] [CrossRef] [PubMed]
- Metcalfe, S.A.; Bowling, F.L.; Reeves, N.D. Subtalar joint arthroereisis in the management of pediatric flexible flatfoot: A critical review of the literature. Foot Ankle Int. 2011, 32, 1127–1139. [Google Scholar] [CrossRef] [PubMed]
- Wozniacka, R.; Bac, A.; Matusik, S.; Szczygiel, E.; Ciszek, E. Body weight and the medial longitudinal foot arch: High-arched foot, a hidden problem? Eur. J. Pediatr. 2013, 172, 683–691. [Google Scholar] [CrossRef] [PubMed]
- Pavone, V.; Costarella, L.; Testa, G.; Conte, G.; Riccioli, M.; Sessa, G. Calcaneo-stop procedure in the treatment of the juvenile symptomatic flatfoot. J. Foot Ankle Surg. 2013, 52, 444–447. [Google Scholar] [CrossRef] [PubMed]
- Giannini, B.S.; Ceccarelli, F.; Benedetti, M.G.; Catani, F.; Faldini, C. Surgical treatment of flexible flatfoot in children a four-year follow-up study. J. Bone Joint Surg. Am. 2001, 83, 73–79. [Google Scholar] [CrossRef] [PubMed]
- Viladot Voegeli, A.; Fontecilla Cornejo, N.; Serra Sandoval, J.A.; Alvarez Goenaga, F.; Viladot Perice, R. Results of subtalar arthroereisis for posterior tibial tendon dysfunction stage IIA1. Based on 35 patients. Foot Ankle Surg. 2018, 24, 28–33. [Google Scholar] [CrossRef] [PubMed]
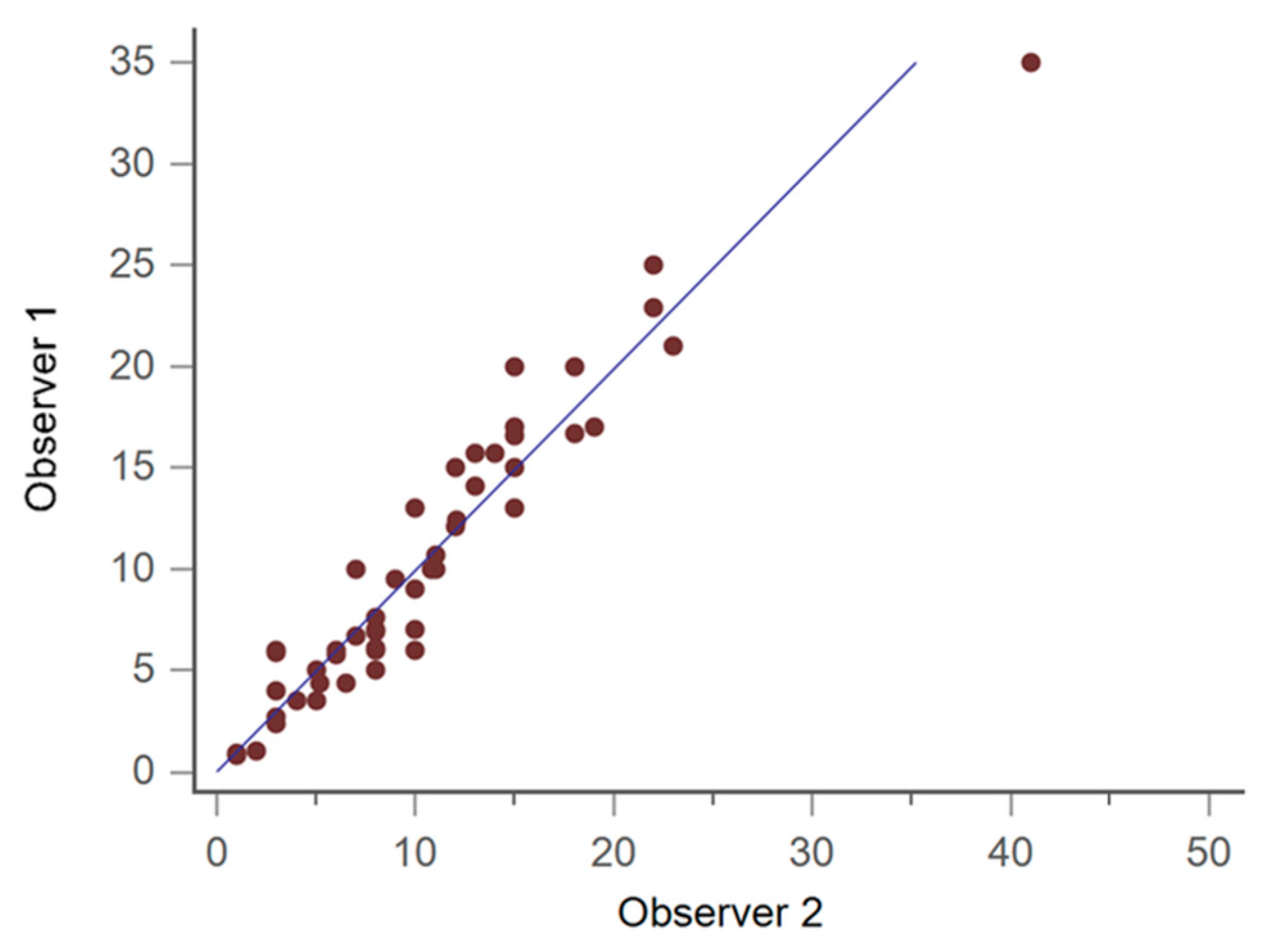
- Bock, P.; Pittermann, M.; Chraim, M.; Rois, S. The inter- and intraobserver reliability for the radiological parameters of flatfoot, before and after surgery. Bone Joint J. 2018, 100, 596–602. [Google Scholar] [CrossRef] [PubMed]
- De Pellegrin, M.; Moharamzadeh, D.; Strobl, W.M.; Biedermann, R.; Tschauner, C.; Wirth, T. Subtalar extra-articular screw arthroereisis (SESA) for the treatment of flexible flatfoot in children. J. Child. Orthop. 2014, 8, 479–487. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Data | In Situ | Extrusion | p Value |
|---|---|---|---|
| (n = 118 Feet of 59 Patients) | (n = 86 Feet of 43 Patients) | ||
| Age | 8.6 ± 0.2 | 9.7 ± 0.3 | 0.021 * |
| Sex | |||
| Male | 42 (71%) | 30 (70%) | |
| Female | 17 (29%) | 13 (30%) | |
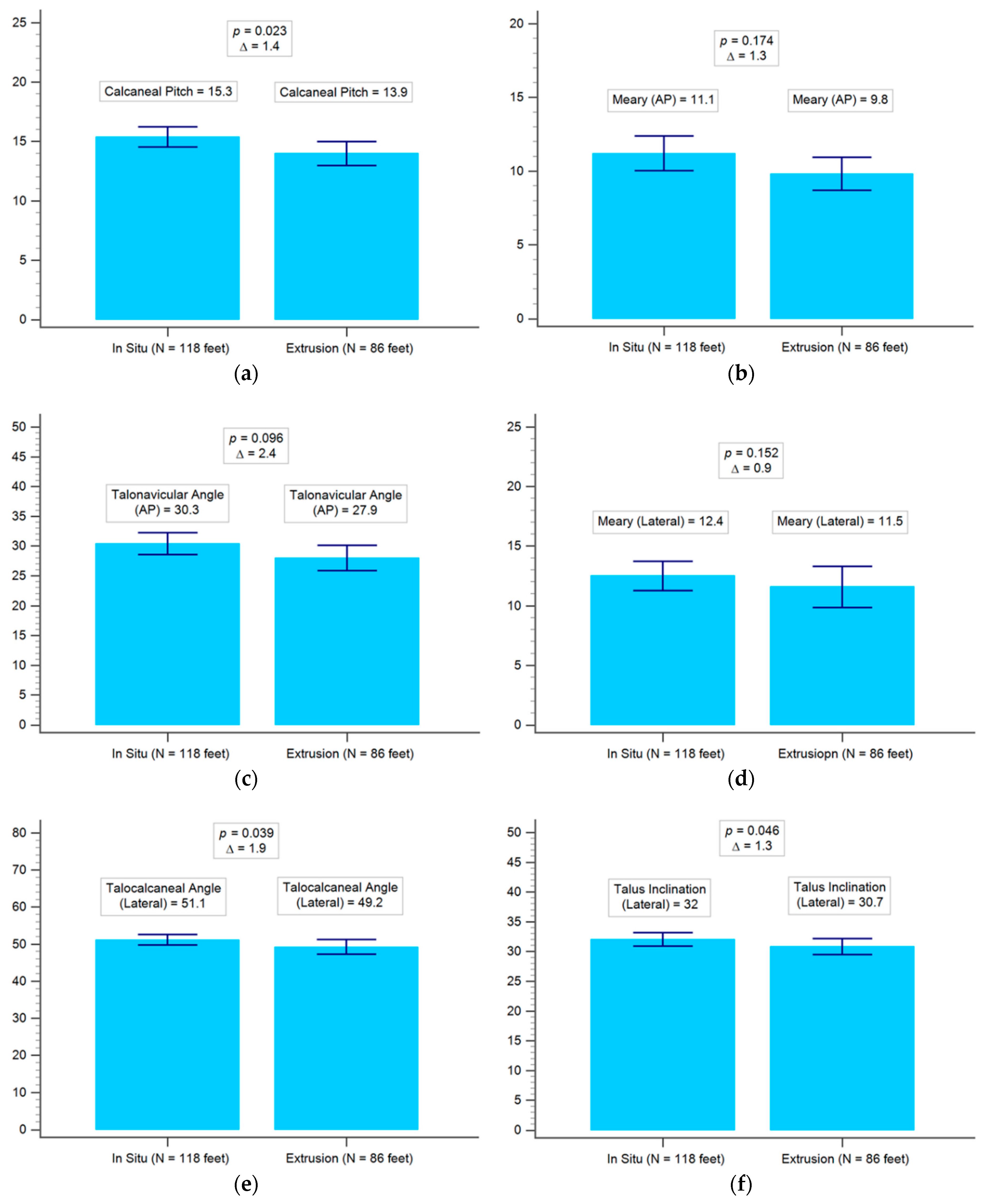
| Calcaneal pitch | 15.3 | 13.9 | 0.023 * |
| Meary (AP) | 11.1 | 9.8 | 0.174 |
| Talonavicular angle (AP) | 30.3 | 27.9 | 0.096 |
| Meary (lateral) | 12.4 | 11.5 | 0.152 |
| Talocalcaneal angle (lateral) | 51.1 | 49.2 | 0.039 * |
| Talus inclination (lateral) | 32.0 | 30.7 | 0.046 * |
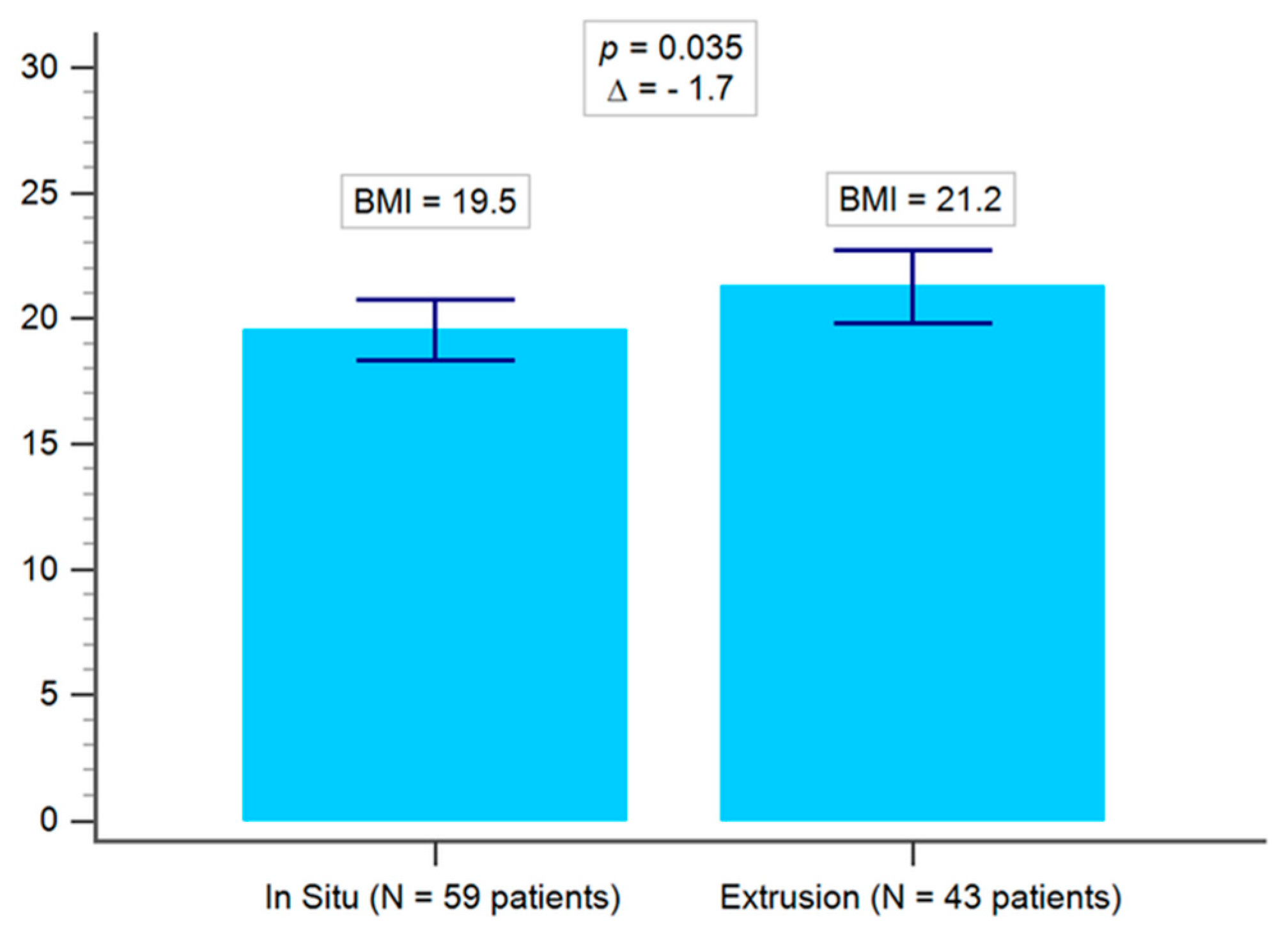
| Demographic Data | Overweight (BMI ≥ 24) | Low Body Weight (BMI ≤ 18.5) | p Value |
|---|---|---|---|
| (n = 56 Feet of 28 Patients) | (n = 112 Feet of 56 Patients) | ||
| Age | 10.1 ± 0.4 | 8.3 ± 0.2 | 0.0005 * |
| Sex | |||
| Male | 24 (86%) | 35 (62.5%) | |
| Female | 4 (14%) | 21 (37.5%) | |
| Calcaneal pitch | 13.7 | 15.2 | 0.018 * |
| Meary (AP) | 9.1 | 11.4 | 0.019 * |
| Talonavicular angle (AP) | 28.6 | 29.9 | 0.405 |
| Meary (lateral) | 9.5 | 12.4 | 0.002 * |
| Talocalcaneal angle (lateral) | 53.1 | 51.7 | 0.004 * |
| Talus inclination (lateral) | 29.7 | 32.6 | 0.005 * |
| Demographic Data | Overweight (BMI ≥ 24) | Low Body Weight (BMI ≤ 18.5) |
|---|---|---|
| Age | 10.1 ± 0.4 | 8.3 ± 0.2 |
| Sex | ||
| Male | 24 (86%) | 36 (63%) |
| Female | 4 (14%) | 21 (37%) |
| Both feet in situ | 8 (29%) | 32 (56%) |
| Both feet extrusion | 11 (39%) | 13 (23%) |
| One foot extrusion | 9 (32%) | 12 (21%) |
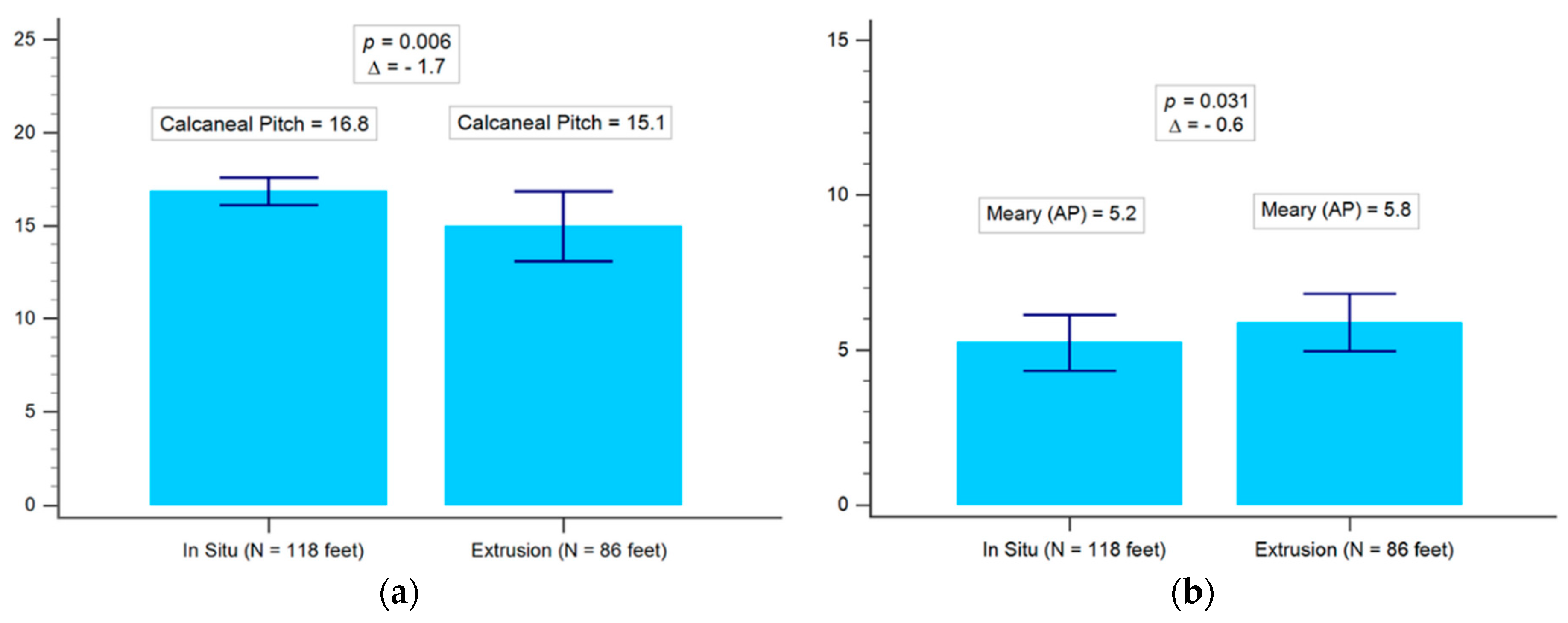
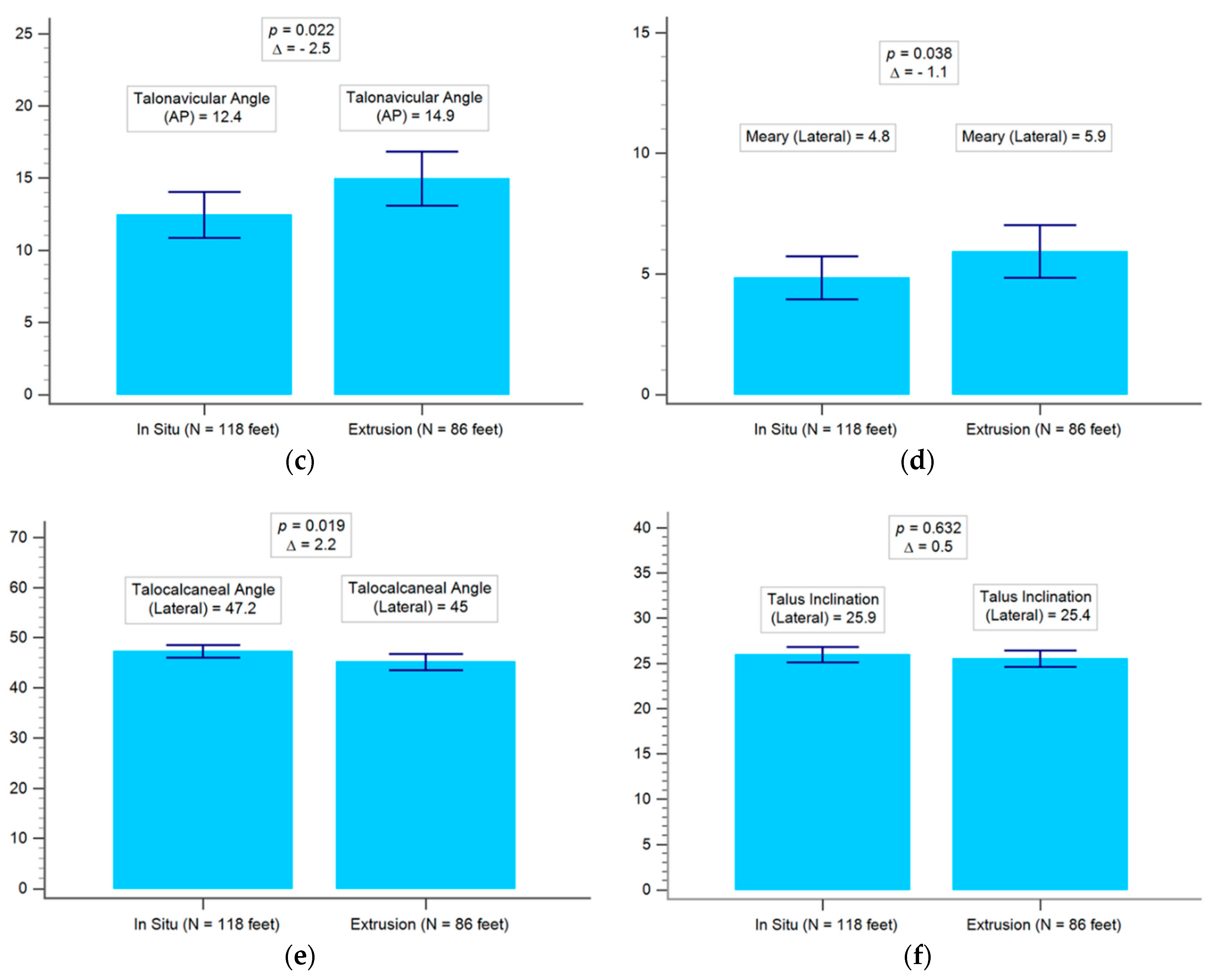
| Radiographic Data | In Situ | Extrusion | p Value |
|---|---|---|---|
| (n = 118 Feet of 59 Patients) | (n = 86 Feet of 43 Patients) | ||
| Calcaneal pitch | 16.8 | 15.1 | 0.006 * |
| Meary angle (AP) | 5.2 | 5.8 | 0.031 * |
| Talonavicular angle (AP) | 12.4 | 14.9 | 0.022 * |
| Meary angle (lateral) | 4.8 | 5.9 | 0.038 * |
| Talocalcaneal angle (lateral) | 47.2 | 45.0 | 0.019 * |
| Talus inclination (lateral) | 25.9 | 25.4 | 0.632 |
| Radiographic Data | In Situ | p Value | Extrusion | p Value | ||
|---|---|---|---|---|---|---|
| (n = 118 Feet of 59 Patients) | (n = 86 Feet of 43 Patients) | |||||
| Pre-op | Post-op | Pre-op | Post-op | |||
| Calcaneal pitch | 15.3 | 16.8 | <0.0001 * | 13.9 | 15.1 | <0.0006 * |
| Meary angle (AP) | 11.1 | 5.2 | <0.0001 * | 9.8 | 5.8 | <0.0001 * |
| Talonavicular angle (AP) | 30.3 | 12.4 | <0.0001 * | 27.9 | 14.9 | <0.0001 * |
| Meary angle (lateral) | 12.4 | 4.8 | <0.0001 * | 11.5 | 5.9 | <0.0001 * |
| Talocalcaneal angle (lateral) | 51.1 | 47.2 | <0.0001 * | 49.2 | 45.0 | <0.0001 * |
| Talus inclination (lateral) | 32.0 | 25.9 | <0.0001 * | 30.7 | 25.4 | <0.0001 * |
| Radiographic Data | In Situ | Extrusion | p Value |
|---|---|---|---|
| (n = 118 Feet of 59 Patients) | (n = 86 Feet of 43 Patients) | ||
| Improved Angle (Degree) | Improved Angle (Degree) | ||
| Calcaneal pitch | 2.7 | 2.6 | 0.732 |
| Meary angle (AP) | 7.8 | 5.9 | 0.008 * |
| Talonavicular angle (AP) | 18.0 | 14.4 | 0.016 * |
| Meary angle (lateral) | 7.9 | 7.0 | 0.096 |
| Talocalcaneal angle (lateral) | 5.1 | 5.5 | 0.355 |
| Talus inclination (lateral) | 7.3 | 5.5 | 0.005 * |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsieh, C.-H.; Lee, C.-C.; Tseng, T.-H.; Wu, K.-W.; Chang, J.-F.; Wang, T.-M. Body Weight Effects on Extra-Osseous Subtalar Arthroereisis. J. Clin. Med. 2019, 8, 1273. https://doi.org/10.3390/jcm8091273
Hsieh C-H, Lee C-C, Tseng T-H, Wu K-W, Chang J-F, Wang T-M. Body Weight Effects on Extra-Osseous Subtalar Arthroereisis. Journal of Clinical Medicine. 2019; 8(9):1273. https://doi.org/10.3390/jcm8091273
Chicago/Turabian StyleHsieh, Chiun-Hua, Chia-Che Lee, Tzu-Hao Tseng, Kuan-Wen Wu, Jia-Feng Chang, and Ting-Ming Wang. 2019. "Body Weight Effects on Extra-Osseous Subtalar Arthroereisis" Journal of Clinical Medicine 8, no. 9: 1273. https://doi.org/10.3390/jcm8091273
APA StyleHsieh, C.-H., Lee, C.-C., Tseng, T.-H., Wu, K.-W., Chang, J.-F., & Wang, T.-M. (2019). Body Weight Effects on Extra-Osseous Subtalar Arthroereisis. Journal of Clinical Medicine, 8(9), 1273. https://doi.org/10.3390/jcm8091273