The Combination of Different Ergonomic Supports during Dental Procedures Reduces the Muscle Activity of the Neck and Shoulder

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
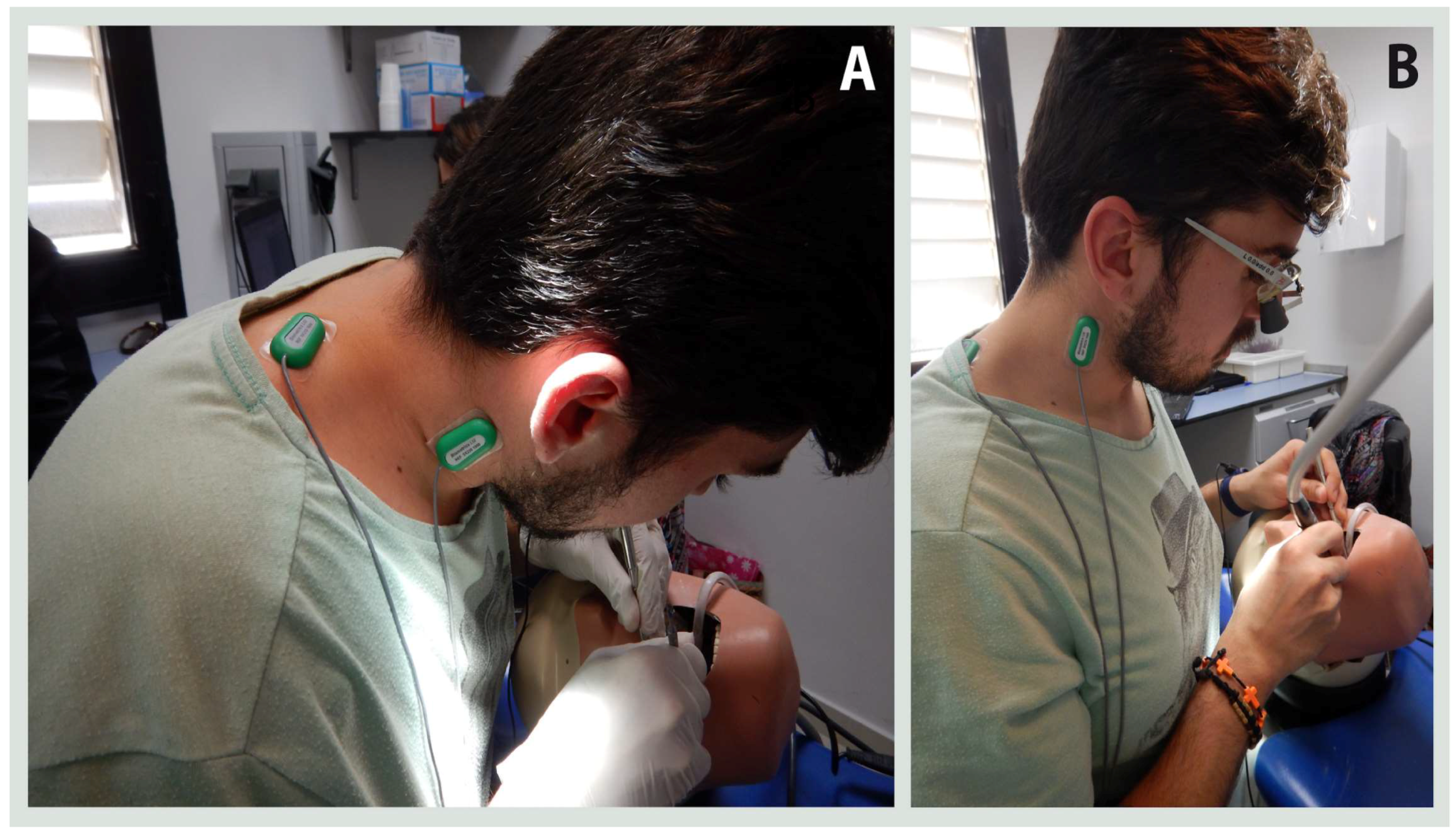
2.3. Instrumentation
2.4. Procedures
2.5. Statistical Analysis
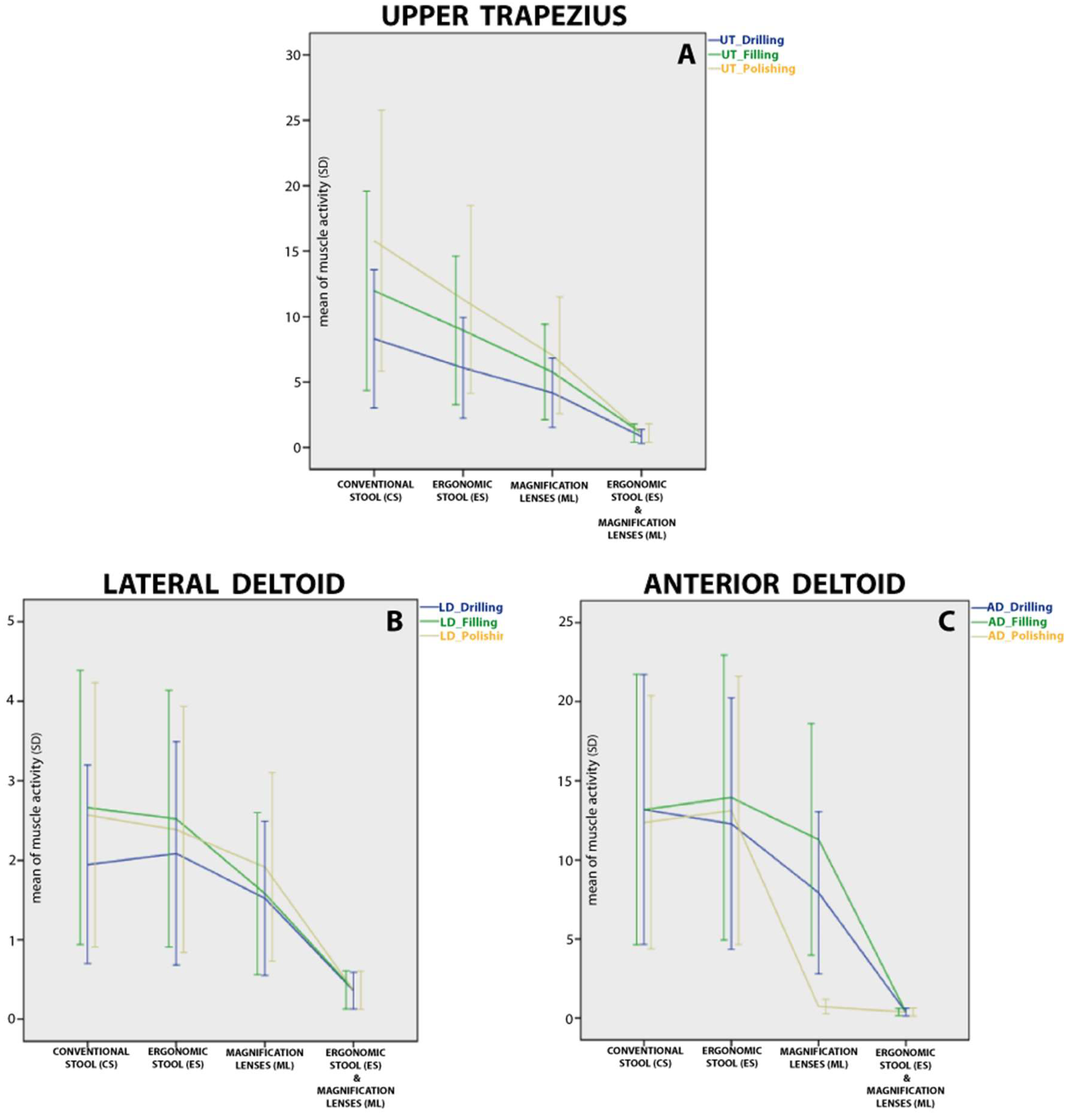
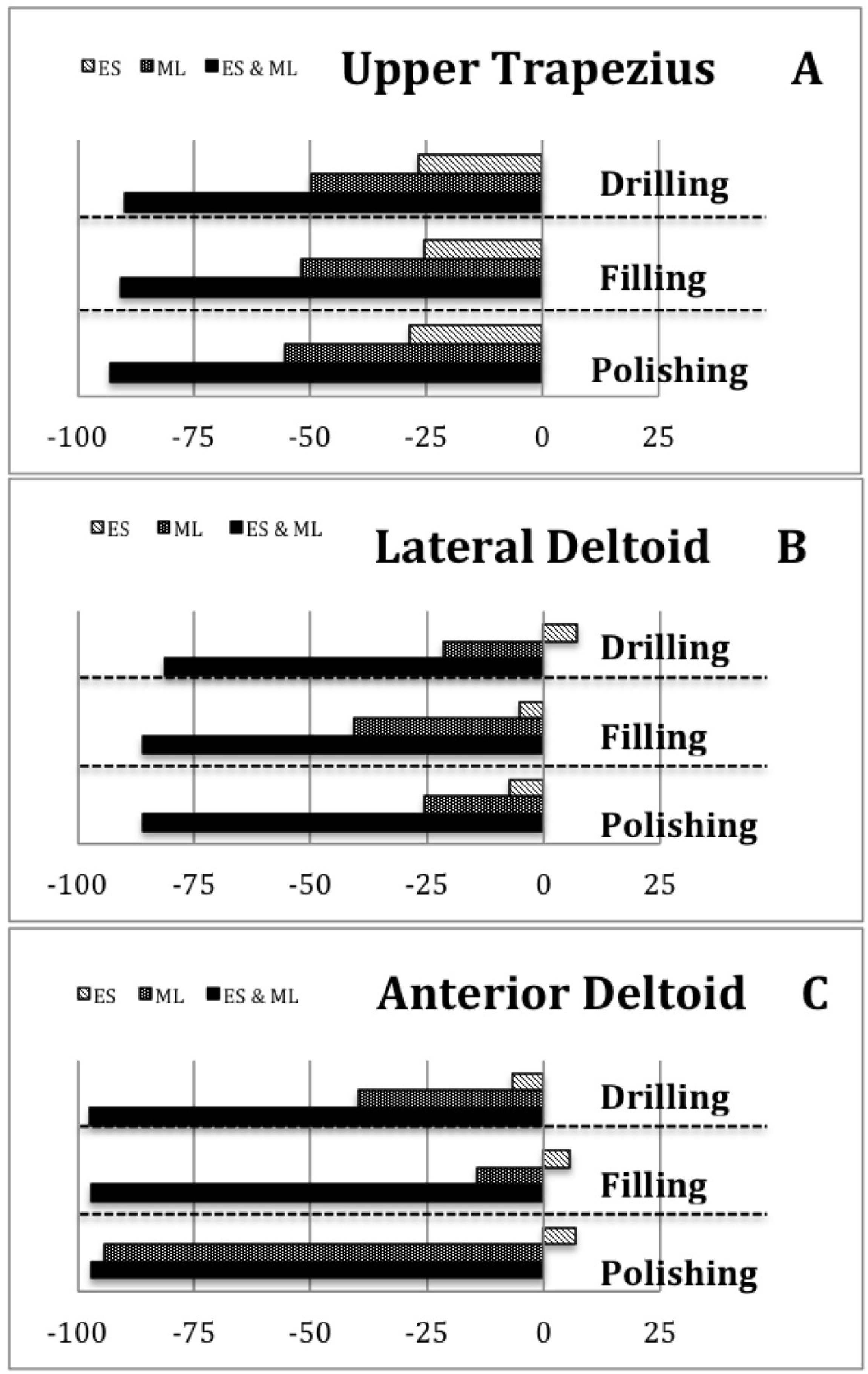
3. Results
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Pejčić, N.; Đurić-Jovičić, M.; Miljković, N.; Popović, D.B.; Petrović, V. Posture in dentists: Sitting vs. standing positions during dentistry work—An EMG study. Srp. Arh. Celok. Lek. 2016, 144, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Sommerich, C.M.; Joines, S.M.; Hermans, V.; Moon, S.D. Use of surface electromyography to estimate neck muscle activity. J. Electromyogr. Kines. 2000, 10, 3773–3798. [Google Scholar] [CrossRef]
- De Sio, S.; Traversini, V.; Rinaldo, F.; Colasanti, V.; Buomprisco, G.; Perri, R.; Mormone, F.; La Torre, G.; Guerra, F. Ergonomic risk and preventive measures of musculoskeletal disorders in the dentistry environment: An umbrella review. PeerJ 2018, 6, 41–54. [Google Scholar] [CrossRef] [PubMed]
- Valachi, B.; Valachi, K. Preventing musculoskeletal disorders in clinical dentistry: Strategies to address the mechanisms leading to musculoskeletal disorders. J. Am. Dent. Assoc. 2003, 134, 1604–1612. [Google Scholar] [CrossRef] [PubMed]
- Khalekar, Y.; Zope, A.; Chaudahari, L.; Brahmankar, U.; Gadge, H.; Deore, S. Prevention is better than cure: Ergonomics in dentistry. J. Appl. Dent. Med. Sci. 2016, 2, 209–216. [Google Scholar]
- Finsen, L.; Christensen, H.; Bakke, M. Musculoskeletal disorders among dentists and variation in dental work. Appl. Ergon. 1998, 29, 119–125. [Google Scholar] [CrossRef]
- Thakar, S.; Shivlingesh, K.; Jayaprakash, K.; Gupta, B.; Gupta, N.; Anand, R.; Motghare, V. High levels of physical inactivity amongst dental professionals: A questionnaire based cross sectional study. J. Clin. Diagn. Res. 2015, 9, 43–46. [Google Scholar] [CrossRef]
- Custodio, R.; Silva, C.; Brandão, J. Ergonomics work analysis applied to dentistry—A Brazilian case study. Work 2012, 41, 690–697. [Google Scholar] [CrossRef]
- Pîrvu, C.; Pătraşcu, I.; Pîrvu, D.; Ionescu, C. The dentist’s operating posture—Ergonomic aspects. J. Med. Life 2014, 7, 177–182. [Google Scholar]
- Gosavi, S.S.; Gosavi, S.Y.; Jawade, R.S. Posturedontics: Reducing the stress in dentistry. World J. Dent. 2012, 3, 335–339. [Google Scholar] [CrossRef]
- Kumar, D.K.; Rathan, N.; Mohan, S.; Begum, M.; Prasad, B.; Prasad, E.R. Exercise prescription to prevent musculoskeletal disorders in dentists. J. Clin. Diagn. Res. 2014, 8, 13–16. [Google Scholar] [CrossRef]
- Carpentier, M.; Aubeux, D.; Armengol, V.; Pérez, F.; Prud’homme, T.; Gaudin, A. The effect of magnification loupes on spontaneous posture change of dental students during preclinical restorative training. J. Dent. Educ. 2019, 83, 407–415. [Google Scholar] [CrossRef]
- Haddad, O.; Sanjari, M.A.; Amirfazli, A.; Narimani, R.; Parnianpour, M. Trapezius Muscle Activity in using Ordinary and Ergonomically Designed Dentistry Chairs. Int. J. Occup. Environ. Med. 2012, 3, 76–83. [Google Scholar]
- Tran, V.; Turner, R.; MacFadden, A.; Cornish, S.M.; Esliger, D.; Komiyama, K.; Chilibeck, P.D. A dental stool with chest support reduces lower back muscle activation. Int. J. Occup. Saf. Ergon. 2016, 22, 301–304. [Google Scholar] [CrossRef]
- Branson, B.G.; Bray, K.K.; Gadbury-Amyot, C.; Holt, L.A.; Kaselyak, N.T.; Mitchell, T.V.; Williams, K.B. Effect of magnification lenses on student operator posture. J. Dent. Educ. 2004, 68, 384–389. [Google Scholar] [PubMed]
- De Bruyne, M.A.; van Renterghem, B.; Baird, A.; Palmans, T.; Danneels, L.; Dolphens, M. Influence of different stool types on muscle activity and lumbar posture among dentists during a simulated dental screening task. Appl. Ergon. 2016, 56, 220–226. [Google Scholar] [CrossRef]
- Dable, R.A.; Wasnik, P.B.; Yeshwante, B.J.; Musani, S.I.; Patil, A.K.; Nagmode, S.N. Postural assessment of students evaluating the need of ergonomic seat and magnification in dentistry. J. Indian Prosthodont. Soc. 2014, 14, 51–58. [Google Scholar] [CrossRef]
- Hayes, M.J.; Osmotherly, P.G.; Taylor, J.A.; Smith, D.R.; Ho, A. The effect of wearing loupes on upper extremity musculoskeletal disorders among dental hygienists. Int. J. Dent. Hyg. 2014, 12, 174–179. [Google Scholar] [CrossRef]
- Hayes, M.J.; Osmotherly, P.G.; Taylor, J.A.; Smith, D.R.; Ho, A. The effect of loupes on neck pain and disability among dental hygienists. Work 2016, 53, 755–762. [Google Scholar] [CrossRef]
- Rolander, B.; Jonker, D.; Karsznia, A.; Öberg, T. Evaluation of muscular activity, local muscular fatigue, and muscular rest patterns among dentists. Acta Odontol. Scand. 2005, 63, 189–195. [Google Scholar] [CrossRef]
- Ranavolo, A.; Chini, G.; Silvetti, A.; Mari, S.; Serrao, M.; Draicchio, F. Myoelectric manifestation of muscle fatigue in repetitive work detected by means of miniaturized sEMG sensors. Int. J. Occup. Saf. Ergon. 2018, 24, 464–474. [Google Scholar] [CrossRef]
- Silva, V.; Fonseca, P.; Pinho, M.E.; Góis, J.; Vaz, M.; Reis-Campos, J. Biomechanical study of dentists’ posture when using a conventional chair versus a saddle-seat chair. Rev. Port. Estomatol. Med. Dent. Cir. Maxilofac. 2017, 58, 39–45. [Google Scholar] [CrossRef][Green Version]
- Jonker, D.; Rolander, B.; Balogh, I. Relation between perceived and measured workload obtained by long-term inclinometry among dentists. Appl. Ergon. 2009, 40, 309–315. [Google Scholar] [CrossRef]
- Maillet, J.; Millar, A.; Burke, J.; Maillet, M.; Maillet, W.; Neish, N. Effect of magnification loupes on dental hygiene student posture. J. Dent. Educ. 2008, 72, 33–44. [Google Scholar]
- Ptaszkowski, K.; Zdrojowy, R.; Ptaszkowska, L.; Bartnicki, J.; Taradaj, J.; Paprocka-Borowicz, M. Electromyographic evaluation of synergist muscles of the pelvic floor muscle depending on the pelvis setting in menopausal women: A prospective observational study. Gait Posture 2019, 71, 170–176. [Google Scholar] [CrossRef]
- Daliri, S.; Forogh, B.; Emami Razavi, S.; Ahadi, T.; Madjlesi, F.; Ansari, N. A single blind, clinical trial to investigate the effects of a single session extracorporeal shock wave therapy on wrist flexor spasticity after stroke. NeuroRehabilitation 2015, 36, 67–72. [Google Scholar] [CrossRef]
- Lovell, R.; Knox, M.; Weston, M.; Siegler, J.; Brennan, S.; Marshall, P. Hamstring injury prevention in soccer: Before or after training? Scand. J. Med. Sci. Spor. 2018, 28, 658–666. [Google Scholar] [CrossRef]
- Pope-Ford, R.; Jiang, Z. Neck and shoulder muscle activation patterns among dentists during common dental procedures. Work 2015, 51, 391–399. [Google Scholar] [CrossRef]
- Åkesson, I.; Hansson, G.Å.; Balogh, I.; Moritz, U.; Skerfving, S. Quantifying work load in neck, shoulders and wrists in female dentists. Int. Arch. Occup. Environ. Health 1997, 69, 461–474. [Google Scholar]
- Blanc, D.; Farre, P.; Hamel, O. Variability of musculoskeletal strain on dentists: An electromyographic and goniometric study. Int. J. Occup. Saf. Ergon. 2014, 20, 295–307. [Google Scholar] [CrossRef]
- Motmans, R.; Tomlow, S.; Vissers, D. Trunk muscle activity in different modes of carrying schoolbags. Ergonomics 2006, 49, 127–138. [Google Scholar] [CrossRef]
- Lindegård, A.; Gustafsson, M.; Hansson, G. Effects of prismatic glasses including optometric correction on head and neck kinematics, perceived exertion and comfort during dental work in the oral cavity—A randomised controlled intervention. Appl. Ergon. 2012, 43, 246–253. [Google Scholar] [CrossRef]
- Plessas, A.; Bernardes, M. The role of ergonomic saddle seats and magnification loupes in the prevention of musculoskeletal disorders. A systematic review. Int. J. Dent. hyg. 2018, 16, 430–440. [Google Scholar] [CrossRef]
- Chaikumarn, M.; Nakphet, N.; Janwantanakul, P. Repeatability of electromyography normalization of the neck and shoulder muscles in symptomatic office workers. Int. J. Occup. Saf. Ergon. 2018, 24, 422–430. [Google Scholar] [CrossRef]
- Cid, M.; Januario, L.; Zanca, G.; Mattiello, S.; Oliveira, A. Normalization of the trapezius sEMG signal—A reliability study on women with and without neck-shoulder pain. Braz. J. Phys. Ther. 2018, 22, 110–119. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Muscle | Task | ICC (IC 95%) | SEM | %SEM |
|---|---|---|---|---|
| UT | Drilling | 0.992 (0.982; 0.996) | 0.14 | 2.3 |
| Filling | 0.972 (0.938; 0.987) | 0.59 | 6.4 | |
| Polishing | 0.990 (0.977; 0.995) | 0.32 | 2.6 | |
| LD | Drilling | 0.966 (0.925; 0.984) | 0.06 | 4.6 |
| Filling | 0.992 (0.982; 0.996) | 0.04 | 2.2 | |
| Polishing | 0.977 (0.950; 0.990) | 0.07 | 3.8 | |
| AD | Drilling | 0.994 (0.986; 0.997) | 0.27 | 2.7 |
| Filling | 0.999 (0.998; 1.000) | 0.07 | 0.7 | |
| Polishing | 0.977 (0.950; 0.990) | 0.33 | 3.5 |
| Muscle | Task | CS Mean (SD) | ES Mean (SD) | ML Mean (SD) | ES & ML Mean (SD) | Significance | ||
|---|---|---|---|---|---|---|---|---|
| Wilks’ Lambda | F Statistic | p-Value | ||||||
| UT | D | 8.30 (5.28) | 6.08 (3.8) | 4.17 (2.64) | 0.84 (0.53) | 0.235 | F3.33 = 35.82 | <0.001 |
| F | 11.97 (7.61) | 8.94 (5.66) | 5.76 (3.64) | 1.09 (0.68) | 0.268 | F3.33 = 30.06 | <0.001 | |
| P | 15.80 (9.96) | 11.31 (7.17) | 7.04 (4.46) | 1.10 (0.69) | 0.277 | F3.33 = 28.72 | <0.001 | |
| LD | D | 1.94 (1.24) | 2.08 (1.40) | 1.52 (0.97) | 0.36 (0.23) | 0.280 | F3.33 = 28.32 | <0.001 |
| F | 2.66 (1.72) | 2.52 (1.61) | 1.58 (1.01) | 0.37 (0.24) | 0.235 | F3.33 = 35.87 | <0.001 | |
| P | 2.57 (1.66) | 2.38 (1.54) | 1.91 (1.18) | 0.36 (0.24) | 0.225 | F3.33 = 37.88 | <0.001 | |
| AD | D | 13.18 (8.53) | 12.29 (7.95) | 7.92 (5.13) | 0.35 (0.23) | 0.284 | F3.33 = 27.68 | <0.001 |
| F | 13.17 (8.54) | 13.93 (9.01) | 11.29 (7.31) | 0.36 (0.22) | 0.272 | F3.33 = 29.38 | <0.001 | |
| P | 12.37 (8.00) | 13.12 (8.48) | 0.71 (0.46) | 0.36 (0.24) | 0.276 | F3.33 = 28.90 | <0.001 | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
García-Vidal, J.A.; López-Nicolás, M.; Sánchez-Sobrado, A.C.; Escolar-Reina, M.P.; Medina-Mirapeix, F.; Bernabeu-Mora, R. The Combination of Different Ergonomic Supports during Dental Procedures Reduces the Muscle Activity of the Neck and Shoulder. J. Clin. Med. 2019, 8, 1230. https://doi.org/10.3390/jcm8081230
García-Vidal JA, López-Nicolás M, Sánchez-Sobrado AC, Escolar-Reina MP, Medina-Mirapeix F, Bernabeu-Mora R. The Combination of Different Ergonomic Supports during Dental Procedures Reduces the Muscle Activity of the Neck and Shoulder. Journal of Clinical Medicine. 2019; 8(8):1230. https://doi.org/10.3390/jcm8081230
Chicago/Turabian StyleGarcía-Vidal, José A., Manuel López-Nicolás, Ana C. Sánchez-Sobrado, María P. Escolar-Reina, Francesc Medina-Mirapeix, and Roberto Bernabeu-Mora. 2019. "The Combination of Different Ergonomic Supports during Dental Procedures Reduces the Muscle Activity of the Neck and Shoulder" Journal of Clinical Medicine 8, no. 8: 1230. https://doi.org/10.3390/jcm8081230
APA StyleGarcía-Vidal, J. A., López-Nicolás, M., Sánchez-Sobrado, A. C., Escolar-Reina, M. P., Medina-Mirapeix, F., & Bernabeu-Mora, R. (2019). The Combination of Different Ergonomic Supports during Dental Procedures Reduces the Muscle Activity of the Neck and Shoulder. Journal of Clinical Medicine, 8(8), 1230. https://doi.org/10.3390/jcm8081230