Review of Systemic Antibiotic Treatments in Children with Rhinosinusitis

 ,
,  , , , ,
, , , , 
Abstract
:1. Introduction
2. Microbiological Basis
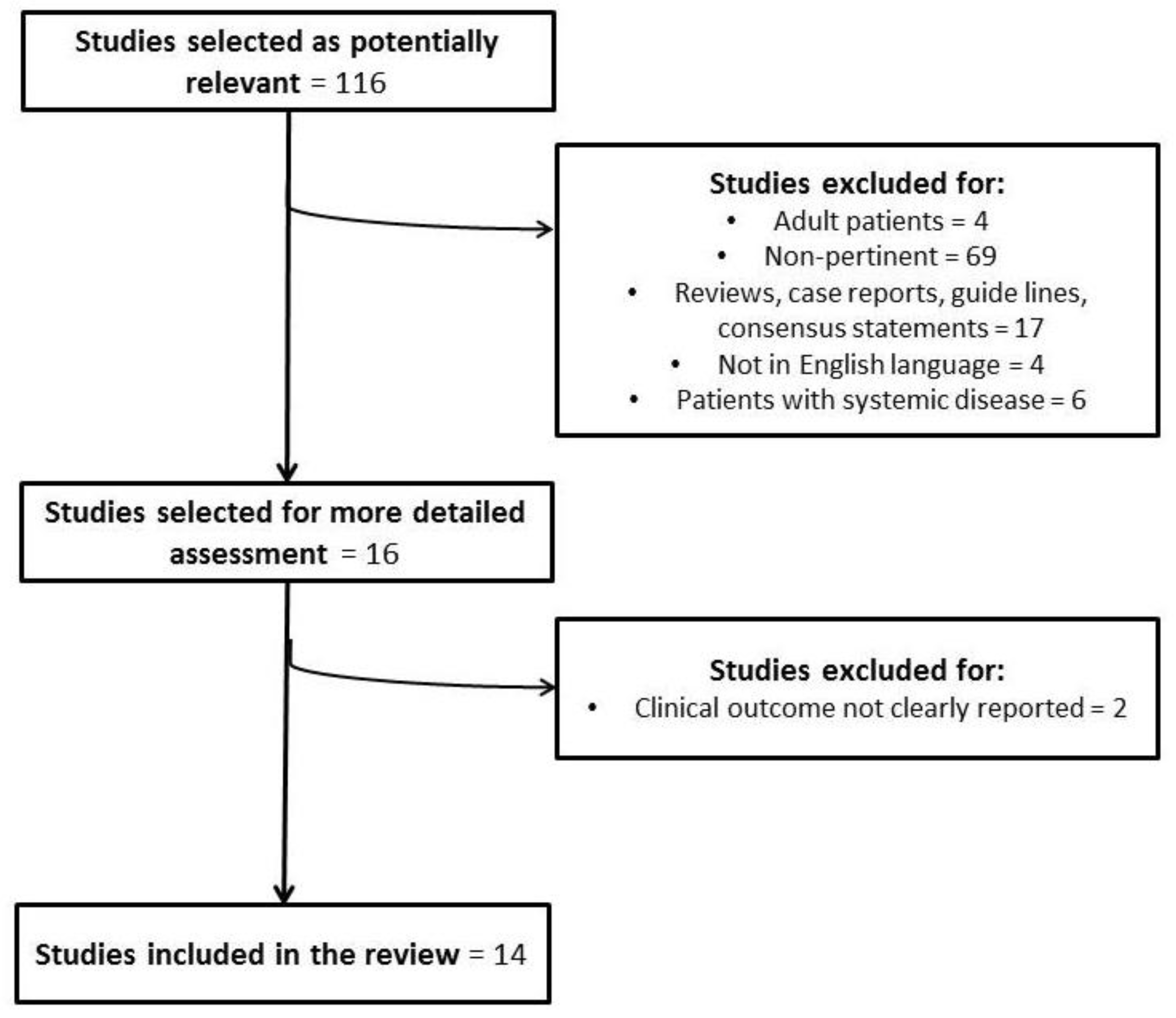
3. Aim of Study and Methods
4. Results
5. Discussion
6. Conclusions
Author Contributions
Conflicts of Interest
References
- Drago, L.; Pignataro, L.; Torretta, S. Microbiological Aspects of Acute and Chronic Pediatric Rhinosinusitis. J. Clin. Med. 2019, 28, 149. [Google Scholar] [CrossRef]
- Wald, E.R.; Nash, D.; Eickhoff, J. Effectiveness of Amoxicillin/Clavulanate Potassium in the Treatment of Acute Bacterial Sinusitis in Children. Pediatrics 2009, 124, 9–15. [Google Scholar] [CrossRef]
- Hauk, L. AAP releases guideline on diagnosis and management of acute bacterial sinusitis in children one to 18 years of age. Am. Fam. Physician 2014, 89, 676–681. [Google Scholar] [PubMed]
- Fokkens, W.J.; Lund, V.J.; Mullol, J.; Bachert, C.; Alobid, I.; Baroody, F.; Cohen, N.; Cervin, A.; Douglas, R.; Gevaert, P.; et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2012. Rhinol. Suppl. 2012, 50, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Karatzanis, A.; Kalogjera, L.; Scadding, G.; Velegrakis, S.; Kawauchi, H.; Cingi, C.; Prokopakis, E. Severe Chronic Upper Airway Disease (SCUAD) in children. Definition issues and requirements. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 965–968. [Google Scholar] [CrossRef] [PubMed]
- Akdis, C.A.; Bachert, C.; Cingi, C.; Dykewicz, M.S.; Hellings, P.W.; Naclerio, R.M.; Schleimer, R.P.; Ledford, D. Endotypes and phenotypes of chronic rhinosinusitis: A PRACTALL document of the European Academy of Allergy and Clinical Immunology and the American Academy of Allergy, Asthma & Immunology. J. Allergy Clin. Immunol. 2013, 131, 1479–1490. [Google Scholar] [PubMed] [Green Version]
- Sih, T. Correlation between respiratory alterations and respiratory diseases due to urban pollution. Int. J. Pediatr. Otorhinolaryngol. 1999, 49, S261–S267. [Google Scholar] [CrossRef]
- Torretta, S.; Drago, L.; Marchisio, P.; Ibba, T.; Pignataro, L. Role of Biofilms in Children with Chronic Adenoiditis and Middle Ear Disease. J. Clin. Med. 2019, 13, 671. [Google Scholar] [CrossRef] [PubMed]
- Nazzari, E.; Torretta, S.; Pignataro, L.; Marchisio, P.; Esposito, S. Role of biofilm in children with recurrent upper respiratory tract infections. Eur. J. Clin. Microbiol. Infect. Dis. 2015, 34, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Smart, B.A.; Slavin, R.G. Rhinosinusitis and pediatric asthma. Immunol. Allergy Clin. N. Am. 2005, 25, 67–82. [Google Scholar] [CrossRef]
- Sedaghat, A.R.; Phipatanakul, W.; Cunningham, M.J. Prevalence of and associations with allergic rhinitis in children with chronic rhinosinusitis. Int. J. Pediatr. Otorhinolaryngol. 2014, 78, 343–347. [Google Scholar] [CrossRef] [PubMed]
- Makary, C.A.; Ramadan, H.H. The role of sinus surgery in children. Laryngoscope 2013, 123, 1348–1352. [Google Scholar] [CrossRef] [PubMed]
- Rizzi, M.D.; Kazahaya, K. Pediatric chronic rhinosinusitis: When should we operate? Curr. Opin. Otolaryngol. Head Neck Surg. 2014, 22, 27–33. [Google Scholar] [CrossRef] [PubMed]
- Newton, L.; Kotowski, A.; Grinker, M.; Chun, R. Diagnosis and management of pediatric sinusitis: A survey of primary care, otolaryngology and urgent care providers. Int. J. Pediatr. Otorhinolaryngol. 2018, 108, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Torretta, S.; Guastella, C.; Ibba, T.; Gaffuri, M.; Pignataro, L. Surgical Treatment of Paediatric Chronic Rhinosinusitis. J. Clin. Med. 2019, 8, 684. [Google Scholar] [CrossRef] [PubMed]
- Torretta, S.; Guastella, C.; Marchisio, P.; Marom, T.; Bosis, S.; Ibba, T.; Drago, L.; Pignataro, L. Sinonasal-Related Orbital Infections in Children: A Clinical and Therapeutic Overview. J. Clin. Med. 2019, 16, 101. [Google Scholar] [CrossRef] [PubMed]
- Hauser, A.; Fogarasi, S. Periorbital and orbital cellulitis. Pediatr. Rev. 2010, 31, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Chandler, J.R.; Langenbrunner, D.J.; Stevens, E.R. The pathogenesis of orbital complications in acute sinusitis. Laryngoscope 1970, 80, 1414–1428. [Google Scholar] [CrossRef] [PubMed]
- Bedwell, J.; Bauman, N.M. Management of pediatric orbital cellulitis and abscess. Curr. Opin. Otolaryngol. Head Neck Surg. 2011, 19, 467–473. [Google Scholar] [CrossRef]
- Kinis, V.; Ozbay, M.; Bakir, S.; Yorgancilar, E.; Gun, R.; Akdag, M.; Sahin, M.; Topcu, I.; Bakır, S. Management of Orbital Complications of Sinusitis in Pediatric Patients. J. Craniofacial Surg. 2013, 24, 1706–1710. [Google Scholar] [CrossRef]
- Hongguang, P.; Lan, L.; Zebin, W.; Guowei, C. Pediatric nasal orbital cellulitis in Shenzhen (South China): Etiology, management, and outcomes. Int. J. Pediatr. Otorhinolaryngol. 2016, 87, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Coudert, A.; Ayari-Khalfallah, S.; Suy, P.; Truy, E. Microbiology and antibiotic therapy of subperiosteal orbital abscess in children with acute ethmoiditis. Int. J. Pediatr. Otorhinolaryngol. 2018, 106, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.Y.; Chiu, N.C.; Lee, K.S.; Huang, F.Y.; Hsu, C.H. Neonatal orbital abscess. Pediatr. Int. 2013, 55, 2316–2320. [Google Scholar] [CrossRef] [PubMed]
- Schlemmer, K.D.; Naidoo, S.K. Complicated sinusitis in a developing country, a retrospective review. Int. J. Pediatr. Otorhinolaryngol. 2013, 77, 1174–1178. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.K.; Saikia, B.; Sharma, R. Orbitocranial Complications of Acute Sinusitis in Children. J. Emerg. Med. 2014, 47, 282–285. [Google Scholar] [CrossRef] [PubMed]
- Ong, Y.K.; Tan, H.K.K. Suppurative intracranial complications of sinusitis in children. Int. J. Pediatr. Otorhinolaryngol. 2002, 66, 49–54. [Google Scholar] [CrossRef]
- Slack, R.; Sim, R. Complications of Rhinosinusitis. Scott Brown’s Otorhinolaryngology: Head and Neck Surgery, 7th ed.; CRC Press: Boca Raton, FL, USA, 2008; pp. 1539–1548. [Google Scholar]
- Chakrabarti, A.; Denning, D.W.; Ferguson, B.J.; Ponikau, J.; Buzina, W.; Kita, H.; Marple, B.; Panda, N.; Vlaminck, S.; Kauffmann-Lacroix, C.; et al. Fungal Rhinosinusitis: A Categorization and Definitional Schema Addressing Current Controversies. Laryngoscope 2009, 119, 1809–1818. [Google Scholar] [CrossRef]
- Amat, F. Complications of bacterial rhino-sinusitis in children: A case report and a review of the literature. Arch. Pediatr. 2010, 17, 258–262. [Google Scholar] [CrossRef]
- Mortimore, S.; Wormald, P.J.; Oliver, S. Antibiotic choice in acute and complicated sinusitis. J. Laryngol. Otol. 1998, 112, 264–268. [Google Scholar] [CrossRef]
- Oxford, L.E.; McClay, J. Complications of Acute Sinusitis in Children. Otolaryngol. Head Neck Surg. 2005, 133, 32–37. [Google Scholar] [CrossRef]
- Kombogiorgas, D.; Seth, R.; Athwal, R.; Modha, J.; Singh, J. Suppurative intracranial complications of sinusitis in adolescence. Single institute experience and review of literature. Br. J. Neurosurg. 2007, 21, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Costerton, J.W.; Lewandowski, Z.; Caldwell, D.E.; Korber, D.R.; Lappin-Scott, H.M. Microbial biofilms. Annu. Rev. Microbiol. 1995, 49, 711–745. [Google Scholar] [CrossRef] [PubMed]
- Keir, J.; Pedelty, L.; Swift, A.C. Biofilms in chronic rhinosinusitis: Systematic review and suggestions for future research. J. Laryngol. Otol. 2011, 125, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Perloff, J.R.; Palmer, J.N. Evidence of Bacterial Biofilms in a Rabbit Model of Sinusitis. Am. J. Rhinol. 2005, 19, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Starner, T.D.; Zhang, N.; Kim, G.; Apicella, M.A.; McCray, P.B., Jr. Haemophilus influenza forms biofilms on airway epithelia: Implications in cystic fibrosis. Am. J. Resp. Crit. Care Med. 2006, 174, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Hall-Stoodley, L.; Costerton, J.W.; Stoodley, P. Bacterial biofilms: From the Natural environment to infectious diseases. Nat. Rev. Genet. 2004, 2, 95–108. [Google Scholar] [CrossRef] [PubMed]
- Chiu, A.G.; Antunes, M.B.; Feldman, M.; Cohen, N.A. An Animal Model for the Study of Topical Medications in Sinusitis. Am. J. Rhinol. 2007, 21, 5–9. [Google Scholar] [CrossRef]
- Sperandio, V. Novel approaches to bacterial infection therapy by interfering with bacteria-to-bacteria signaling. Expert Rev. Anti Infect. Ther. 2007, 5, 271–276. [Google Scholar] [CrossRef] [Green Version]
- De Moor, C.; Reardon, G.; McLaughlin, J.; Maiese, E.M.; Navaratnam, P. A Retrospective Comparison of Acute Rhinosinusitis Outcomes in Patients Prescribed Antibiotics, Mometasone Furoate Nasal Spray, or Both. Am. J. Rhinol. Allergy 2012, 26, 308–314. [Google Scholar] [CrossRef]
- Ragab, A.; Farahat, T.; Al-Hendawy, G.; Samaka, R.; Ragab, S.; El-Ghobashy, A. Nasal saline irrigation with or without systemic antibiotics in treatment of children with acute rhinosinusitis. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 2178–2186. [Google Scholar] [CrossRef]
- Veskitkul, J.; Vichyanond, P.; Pacharn, P.; Visitsunthorn, N.; Jirapongsananuruk, O. Clinical characteristics of recurrent acute rhinosinusitis in children. Asian Pac. J. Allergy Immunol. 2015, 33, 276–280. [Google Scholar] [PubMed]
- Veskitkul, J.; Wongkaewpothong, P.; Thaweethamchareon, T.; Ungkanont, K.; Visitsunthorn, N.; Pacharn, P.; Vichyanond, P.; Jirapongsananuruk, O. Recurrent Acute Rhinosinusitis Prevention by Azithromycin in Children with Nonallergic Rhinitis. J. Allergy Clin. Immunol. Pract. 2017, 5, 1632–1638. [Google Scholar] [CrossRef] [PubMed]
- Poachanukoon, O.; Nanthapisal, S.; Chaumrattanakul, U. Pediatric acute and chronic rhinosinusitis: Comparison of clinical characteristics and outcome of treatment. Asian Pac. J. Allergy Immunol. 2012, 30, 146–151. [Google Scholar] [PubMed]
- Shin, Y.H.; Kim, H.S.; Lee, E.K.; Kim, Y.J.; Lee, H.-S.; Jang, P.-S.; Kim, Y.-H.; Chun, Y.H.; Yoon, J.-S.; Kim, H.H.; et al. Eosinophil related markers and total immunoglobulin E as a predictive marker for antibiotics response in chronic rhinosinusitis: A case-control study. Ann. Saudi Med. 2015, 35, 312–317. [Google Scholar] [CrossRef] [PubMed]
- Gavriel, H.; Yeheskeli, E.; Aviram, E.; Yehoshua, L.; Eviatar, E. Dimension of Subperiosteal Orbital Abscess as an Indication for Surgical Management in Children. Otolaryngol. Neck Surg. 2011, 145, 823–827. [Google Scholar] [CrossRef] [PubMed]
- Ketenci, I.; Unlü, Y.; Vural, A.; Doğan, H.; Sahin, M.I.; Tuncer, E. Approaches to subperiosteal orbital abscesses. Eur. Arch. Otorhinolaryngol. 2013, 270, 1317–1327. [Google Scholar] [CrossRef] [PubMed]
- Schupper, A.J.; Jiang, W.; Coulter, M.J.; Brigger, M.; Nation, J. Intracranial complications of pediatric sinusitis: Identifying risk factors associated with prolonged clinical course. Int. J. Pediatr. Otorhinolaryngol. 2018, 112, 10–15. [Google Scholar] [CrossRef]
- Wan, K.S.; Wu, W.F.; Chen, T.C.; Wu, C.S.; Hung, C.W.; Chang, Y.S. Comparison of amoxicillin clavulanate with or without intranasal fluticasone for the treatment of uncomplicated acute rhinosinusitis in children. Minerva Pediatr. 2015, 67, 489–494. [Google Scholar]
- Kristo, A.; Uhari, M. Timing of Rhinosinusitis Complications in Children. Pediatr. Infect. Dis. J. 2009, 28, 769–771. [Google Scholar] [CrossRef]
- Emmett Hurley, P.; Harris, G.J. Subperiosteal abscess of the orbit: Duration of intravenous antibiotic therapy in nonsurgical cases. Ophthalmic Plast. Reconstr. Surg. 2012, 28, 22–26. [Google Scholar] [CrossRef]
- Chow, A.W.; Benninger, M.S.; Brook, I.; Brozek, J.L.; Goldstein, E.J.; Hicks, L.A.; Pankey, G.A.; Seleznick, M.; Volturo, G.; Wald, E.R.; et al. Infectious Diseases Society of America. IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clin. Infect. Dis. 2012, 54, e72–e112. [Google Scholar] [CrossRef] [PubMed]
- Wald, E.R.; Applegate, K.E.; Bordley, C.; Darrow, D.H.; Glode, M.P.; Marcy, S.M.; Nelson, C.E.; Rosenfeld, R.M.; Shaikh, N.; Smith, M.J.; et al. Clinical practice guideline for the diagnosis and management of acute bacterial sinusitis in children aged 1 to 18 years. Pediatrics 2013, 132, 262–280. [Google Scholar]
- Wald, E.R.; DeMuri, G.P. Antibiotic Recommendations for Acute Otitis Media and Acute Bacterial Sinusitis: Conundrum No More. Pediatr. Infect. Dis. J. 2018, 37, 1255–1257. [Google Scholar] [CrossRef] [PubMed]
- Brietzke, S.E.; Shin, J.J.; Choi, S.; Lee, J.T.; Parikh, S.R.; Pena, M.; Prager, J.D.; Ramadan, H.; Veling, M.; Corrigan, M.; et al. Clinical consensus statement: Pediatric chronic rhinosinusitis. Otolaryngol. Head Neck Surg. 2014, 151, 542–553. [Google Scholar] [CrossRef] [PubMed]
- Brook, I. The role of antibiotics in pediatric chronic rhinosinusitis. Laryngoscope 2017, 2, 104–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Author, Year | Pts Category | No. of Pts; Age (Years) | Study Design | Interventions | Outcomes | Failures and Side Effects | |
|---|---|---|---|---|---|---|---|
| Wald et al., 2009 [2] | 56; 66 ± 30 months | Prospective randomised | Amoxicillin (90 mg/kg/day) with potassium clavulanate (6.4 mg/kg/day) in two doses (50%) vs. placebo | Children receiving antibiotics were more likely to be cured (50% vs. 14%; p = 0.010) and less likely to have treatment failure (14% vs. 68%; p < 0.001) compared to placebo | Adverse events * more frequently occurred in treatment compared to placebo group (44% vs. 14%; p = 0.014); * self-limiting diarrhoea | ||
| De Moor et al., 2012 [40] | 12679; 12–75 | Retrospective | Mometasone furoato nasal spray (MNS) vs. MNS plus antibiotic vs. antibiotic | MNS (alone or in combination with antibiotic) significantly reduced the risk of rhinosinusitis-related medical encounters compared to antibiotic alone | |||
| Poachanukoon et al., 2012 [44] | ARS (103) and CRS (51) | 154; 5.9 ± 3.3 | Prospective non-randomised | Amoxicillin-clavulanic acid (54.5%), cefditoren pivoxil (33.8%) for 14.6 ± 3.8 days (ARS) or 22.3 ± 5.0 days (CRS); intravenous antibiotic in 5.8% of cases (77.8% with ARS) | Symptomatic improvement in ARS group after 14.6 days of treatment on average and in CRS group after 22.3 days of treatment on average; no one underwent surgery | ||
| Wan et al., 2015 [49] | Allergic rhinitis in 50% | 100; 15 ± 1.7 | Retrospective | Amoxicillin-clavulanic acid vs. amoxicillin-clavulanic acid plus intranasal corticosteroid vs. placebo | Symptom improvement in 92% and 88% of patients receiving amoxicillin-clavulanic acid with and without allergic rhinitis, respectively, compared to symptom improvement in 84% and 96% of patients receiving amoxicillin-clavulanic acid plus intranasal corticosteroid with and without allergic rhinitis, respectively; symptomatic improvement in 30% of placebo group | ||
| Ragab et al., 2015 [41] | 62; 5.4 ± 2.3 and 4.6 ± 2.0 | Prospective randomised | Amoxicillin 100 mg/kg/day, three times a day, plus nasal saline irrigations vs. placebo plus nasal saline irrigations | Clinical recovery in 83.9% and 71% of patients respectively belonging to study and control group (not significant); clinical improvement in 3% and 6% of patients respectively belonging to study and control group | Adverse events in 58.1% * and 25.8% of patients respectively belonging to study and control group (p = 0.005); * including diarrhoea (29.0%), abdominal pain (16.1%), and nausea (6.0%) |
| Author, Year | Pts Category | No. of Pts; Age (Years) | Study Design | Interventions | Outcomes | Failures and Side Effects |
|---|---|---|---|---|---|---|
| Poachanukoon et al., 2012 [44] | ARS (103) and CRS (51) | 154; 5.9 ± 3.3 | Prospective non-randomised | Amoxicillin-clavulanic acid (54.5%), cefditoren pivoxil (33.8%) for 14.6 ± 3.8 days (ARS) or 22.3 ± 5.0 days (CRS); intravenous antibiotic in 5.8% of cases (77.8% with ARS) | Symptomatic improvement in ARS group after 14.6 days of treatment on average and in CRS group after 22.3 days of treatment on average; no one underwent surgery | |
| Shin et al., 2015 [45] | CRS (62.1% non-respondents and 37.9% respondents) | 58 with CRS; 5.8 ± 3.0 and 5.6 ± 2.7 | Prospective non-randomised | Amoxicillin (90 mg/kg/day) with clavulanic acid (6.4 mg/kg/day), second-or third-generation cephalosporines for 12 weeks | Symptomatic, clinical, or radiological recovery in 62.1% | Lack of response to antibiotic treatment was significantly related to increased total eosinophilic count and serum eosinophilic cationic protein levels |
| Veskitkul et al., 2015 [42] | RARS (IgG subclass deficiency in 78.7%) | 94; 7.7 ± 2.6 | Retrospective | Oral antibiotic prophylaxis in 61.5% * (± adenotonsillectomy, allergen immunotherapy, gentamicin nasal irrigations, intravenous immunoglobulins); * amoxicillin or azithromycin | Symptomatic improvement in 80% of patients receiving antibiotic | |
| Veskitkul et al., 2017 [43] | RARS | 60; 5–15 | Prospective randomised | Azithromycin 5 mg/kg/day for 3 days a week for 12 months | Number of acute episodes significantly reduced in children receiving antibiotic compared to controls with a number needed to treat = 2; subjective improvement and reduced adjunctive medication in study but not control group |
| Author, Year | Pts Category | No. of Pts; Age (Years) | Study Design | Interventions | Outcomes | Failures and Side Effects | ||
|---|---|---|---|---|---|---|---|---|
| Kristo et al., 2009 [50] | Orbital complications | 20; 6.4 (8.0–12.4) | Retrospective | Parenteral antibiotic * (surgery in 10%); * cefuroxime (80.0%), clindamycin (10.0%), combined (10.0%) | Complete recovery in 100% | |||
| Hurley et al., 2011 [51] | SPA | 42; <9 years | Retrospective | Parenteral antibiotic: combined therapy with either amoxicillin-sulbactam or a third-generation cephalosporin, and either clindamycin or vancomycin for 2–8 days, followed by amoxicillin-clavulanate for 2–3 weeks | Complete recovery in 97.6% | One patient readmitted and underwent surgery | ||
| Gavriel et al., 2011 [46] | SPA | 48; 4.0 ± 3.5 | Retrospective | Parenteral antibiotic * (surgery in 47.6%); *amoxicillin-clavulanic acid (83.3%), ceftriaxone (10.0%), clindamycin plus metronidazole (8.3%), cefuroxime (2%) | Children with an abscess >0.5 mL should be candidates for surgery; conservative treatment can be considered only in those with smaller abscess without visual impairment | |||
| Ketenci et al., 2013 [47] | SPA | 36; 3–76 (47.2% < 10 years) | Retrospective | Ampicillin with or without metronidazole or clindamycin as first choice (ampicillin in 64.0%, multiple antibiotics* in 36.0%); * ampicillin-sulbactam, clindamycin, sulperazone, metronidazole; 3–9 days for medial, 6–10 days for superior, and 3–4 days for inferior SPA location | Visual recovery in 47.21%; partial visual recovery in 5.5% | Unilateral blindness in 5.5%. Early recurrences in 5.5% (second surgery); late recurrence in 2.8% (first surgery); intracranial abscess with fatal outcome in 2.8% (repeated surgery) | ||
| Schupper et al., 2018 [48] | Intracranial complications | 16; 5–17 | Retrospective | Parenteral antibiotic (vancomycin, meropenem, and ceftriaxone) with sinus surgery (plus craniotomy in 68.0%) | Abscess reaccumulation in 37.5%. Allergic reaction (12.0% to ceftriaxone, vamcomycin), meropenem-induced neutropenia (6.0%) |
| Author, Year | Document | Recommendation |
|---|---|---|
| Chow et al., 2012 [52] | IDSA guideline | Amoxicillin-clavulanate. In patients with risk factors *, amoxicillin-clavulanate (90 mg/kg/day in two doses) or third-generation cephalosporin plus clindamycin for 10–14 days. In the case of non-type I hypersensitivity, third-generation cephalosporin plus clindamycin, doxycycline |
| Wald et al., 2013 [53] | AAP guidelines | Amoxicillin or amoxicillin-clavulanate in children with severe onset or worsening for 10–28 days. Intravenous or intramuscular ceftriaxone (50 mg/kg) if oral therapy is not possible. In the case of non-type I hypersensitivity cefdinir, cefuroxime; in the case of type-I hypersensitivity, cefdinir, cefuroxime or cefixime plus clindamycin |
| Wald and de Muri, 2018 [54] | Expert opinion | Amoxicillin-clavulanate (45 mg/kg/day) in two doses |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torretta, S.; Drago, L.; Marchisio, P.; Gaini, L.; Guastella, C.; Moffa, A.; Rinaldi, V.; Casale, M.; Pignataro, L. Review of Systemic Antibiotic Treatments in Children with Rhinosinusitis. J. Clin. Med. 2019, 8, 1162. https://doi.org/10.3390/jcm8081162
Torretta S, Drago L, Marchisio P, Gaini L, Guastella C, Moffa A, Rinaldi V, Casale M, Pignataro L. Review of Systemic Antibiotic Treatments in Children with Rhinosinusitis. Journal of Clinical Medicine. 2019; 8(8):1162. https://doi.org/10.3390/jcm8081162
Chicago/Turabian StyleTorretta, Sara, Lorenzo Drago, Paola Marchisio, Lorenzo Gaini, Claudio Guastella, Antonio Moffa, Vittorio Rinaldi, Manuel Casale, and Lorenzo Pignataro. 2019. "Review of Systemic Antibiotic Treatments in Children with Rhinosinusitis" Journal of Clinical Medicine 8, no. 8: 1162. https://doi.org/10.3390/jcm8081162
APA StyleTorretta, S., Drago, L., Marchisio, P., Gaini, L., Guastella, C., Moffa, A., Rinaldi, V., Casale, M., & Pignataro, L. (2019). Review of Systemic Antibiotic Treatments in Children with Rhinosinusitis. Journal of Clinical Medicine, 8(8), 1162. https://doi.org/10.3390/jcm8081162