Diagnostic Accuracy of Radiologic Methods for Ankle Syndesmosis Injury: A Systematic Review and Meta-Analysis


 , , and
, , and
Abstract
:1. Introduction
2. Experimental Section
2.1. Searching Strategy
2.2. Data Collection and Analysis
2.3. Statistical Analyses
2.4. Assessing the Risk of Bias in the Included Studies
2.5. Synthesis of Included Studies
3. Results
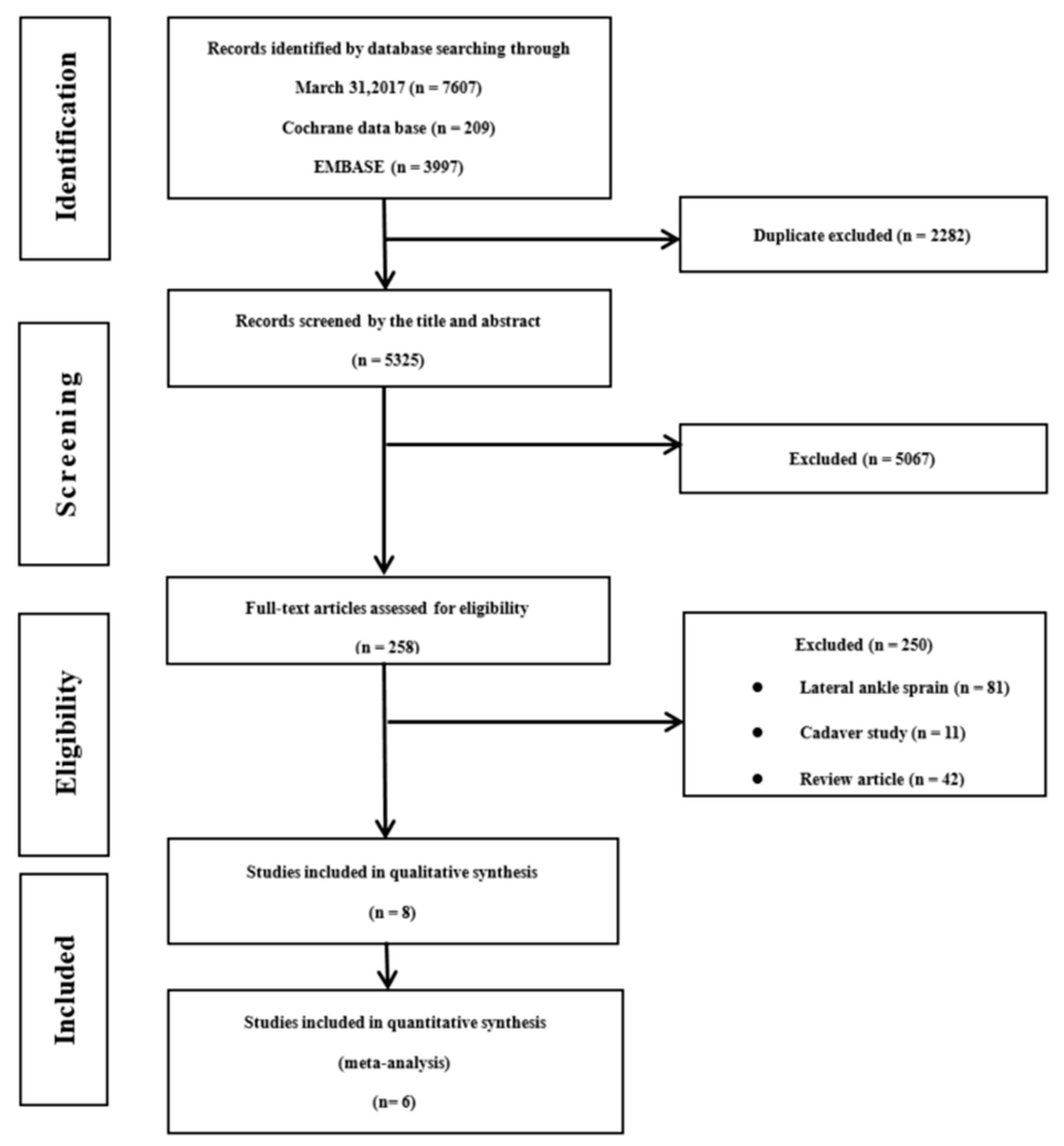
3.1. Inclusion of Studies
3.2. Quality Assessment and Reporting Bias
3.3. Outcome and Findings for Diagnostic Accuracy
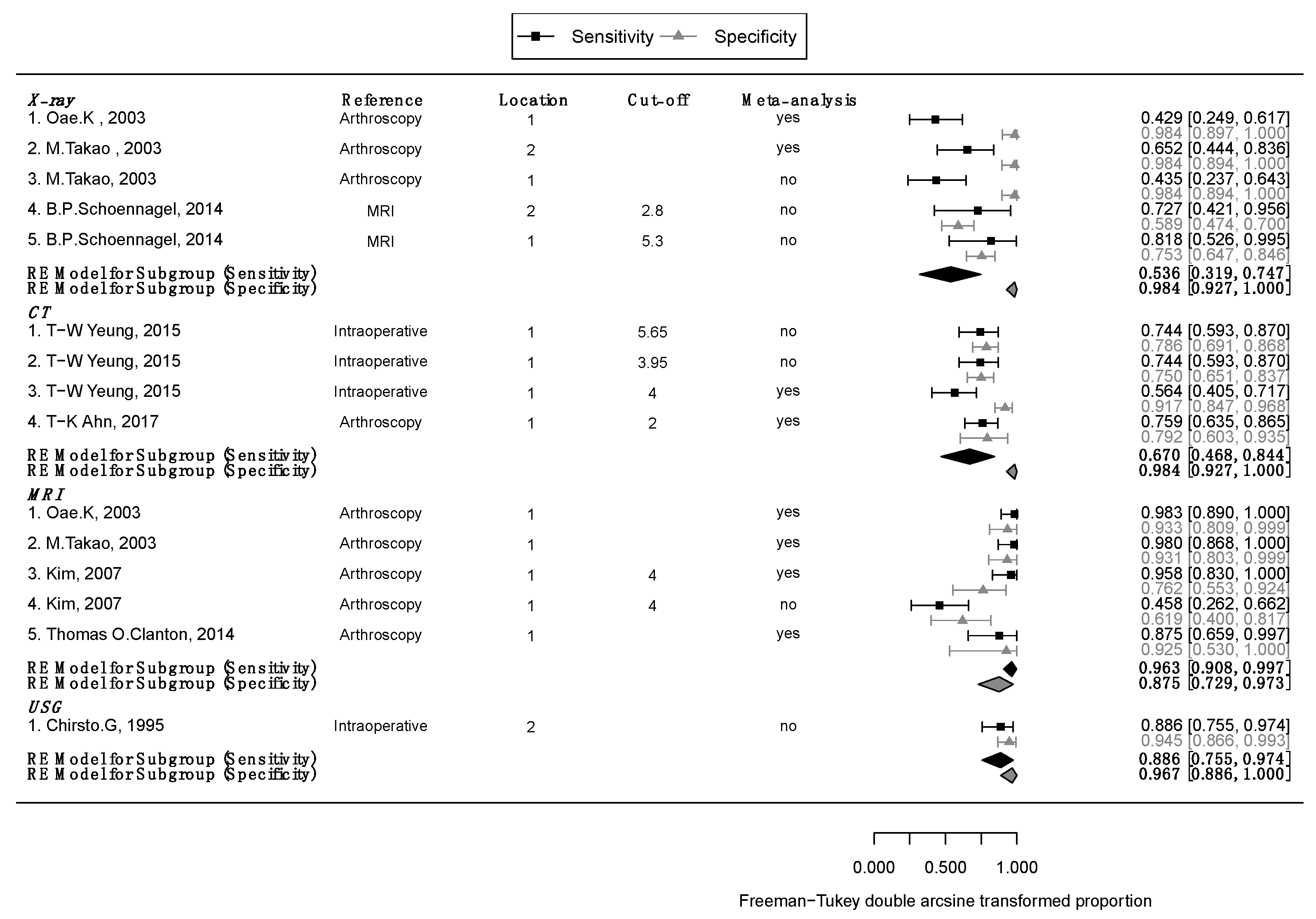
3.3.1. X-ray
3.3.2. CT
3.3.3. MRI
3.3.4. USG
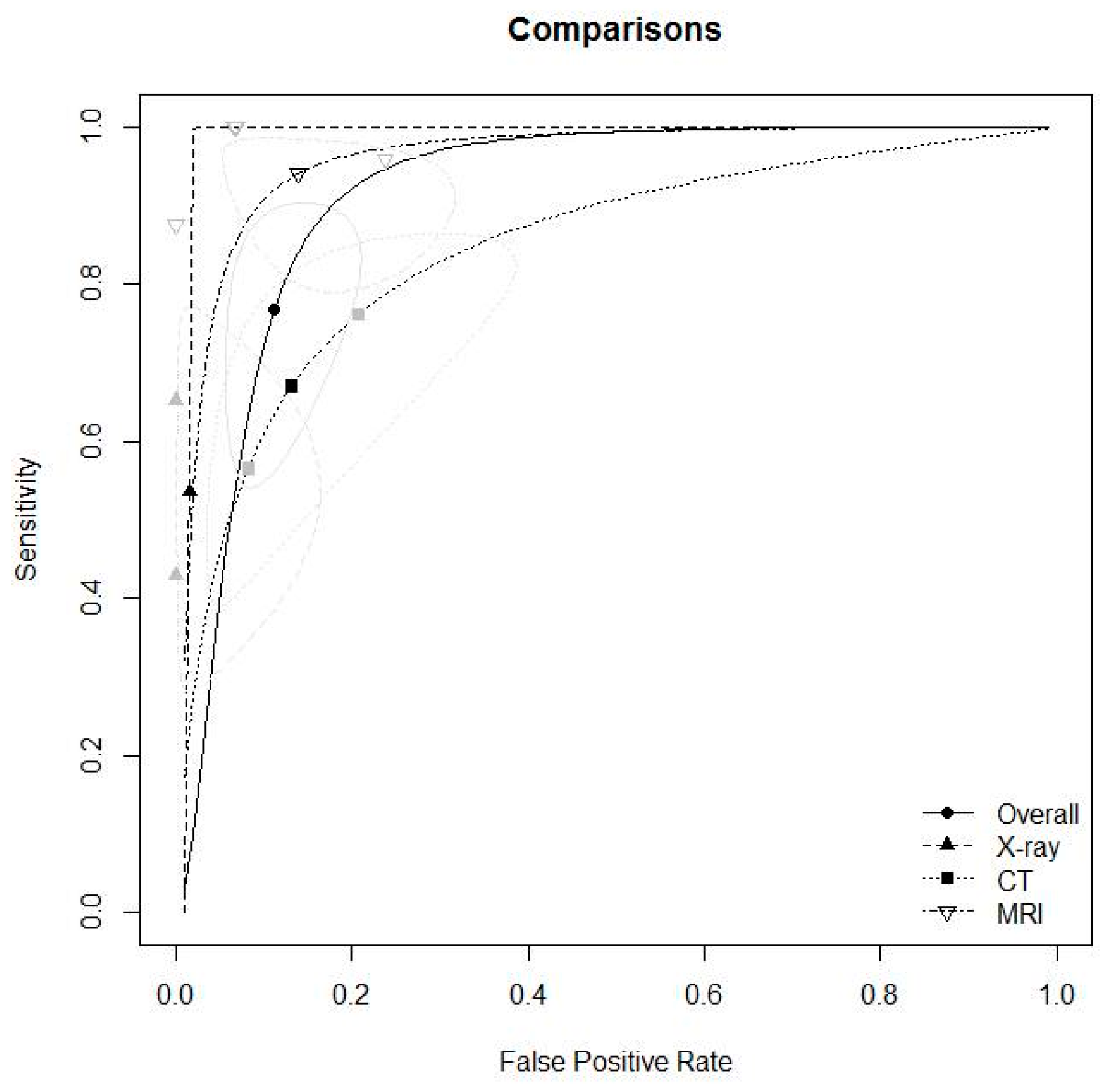
3.3.5. Diagnostic Accuracy for X-ray, CT, and MRI
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Gerber, J.P.; Williams, G.N.; Scoville, C.R.; Arciero, R.A.; Taylor, D.C. Persistent disability associated with ankle sprains: A prospective examination of an athletic population. Foot Ankle Int. 1998, 19, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Brosky, T.; Nyland, J.; Nitz, A.; Caborn, D.N. The ankle ligaments: Consideration of syndesmotic injury and implications for rehabilitation. J. Orthop. Sports Phys. Ther. 1995, 21, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Boytim, M.J.; Fischer, D.A.; Neumann, L. Syndesmotic ankle sprains. Am. J. Sports Med. 1991, 19, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Fritschy, D. An unusual ankle injury in top skiers. Am. J. Sports Med. 1989, 17, 282–285, discussion 285–286. [Google Scholar] [CrossRef] [PubMed]
- Wright, R.W.; Barile, R.J.; Surprenant, D.A.; Matava, M.J. Ankle syndesmosis sprains in national hockey league players. Am. J. Sports Med. 2004, 32, 1941–1945. [Google Scholar] [CrossRef] [PubMed]
- Hopkinson, W.J.; St Pierre, P.; Ryan, J.B.; Wheeler, J.H. Syndesmosis sprains of the ankle. Foot Ankle 1990, 10, 325–330. [Google Scholar] [CrossRef] [PubMed]
- Katznelson, A.; Lin, E.; Militiano, J. Ruptures of the ligaments about the tibio-fibular syndesmosis. Injury 1983, 15, 170–172. [Google Scholar] [CrossRef]
- Taylor, D.C.; Englehardt, D.L.; Bassett, F.H., 3rd. Syndesmosis sprains of the ankle. The influence of heterotopic ossification. Am. J. Sports Med. 1992, 20, 146–150. [Google Scholar] [CrossRef]
- Nussbaum, E.D.; Hosea, T.M.; Sieler, S.D.; Incremona, B.R.; Kessler, D.E. Prospective evaluation of syndesmotic ankle sprains without diastasis. Am. J. Sports Med. 2001, 29, 31–35. [Google Scholar] [CrossRef]
- Mullins, J.F.; Sallis, J.G. Recurrent sprain of the ankle joint with diastasis. J. Bone Jt. Surg. Br. 1958, 40, 270–273. [Google Scholar] [CrossRef]
- Ogilvie-Harris, D.J.; Reed, S.C. Disruption of the ankle syndesmosis: Diagnosis and treatment by arthroscopic surgery. Arthroscopy 1994, 10, 561–568. [Google Scholar] [CrossRef]
- Kiter, E.; Bozkurt, M. The crossed-leg test for examination of ankle syndesmosis injuries. Foot Ankle Int. 2005, 26, 187–188. [Google Scholar] [CrossRef] [PubMed]
- Beumer, A.; Swierstra, B.A.; Mulder, P.G. Clinical diagnosis of syndesmotic ankle instability: Evaluation of stress tests behind the curtains. Acta Orthop. Scand. 2002, 73, 667–669. [Google Scholar] [CrossRef] [PubMed]
- Teitz, C.C.; Harrington, R.M. A biochemical analysis of the squeeze test for sprains of the syndesmotic ligaments of the ankle. Foot Ankle Int. 1998, 19, 489–492. [Google Scholar] [CrossRef] [PubMed]
- Takao, M.; Ochi, M.; Naito, K.; Iwata, A.; Kawasaki, K.; Tobita, M.; Miyamoto, W.; Oae, K. Arthroscopic diagnosis of tibiofibular syndesmosis disruption. Arthroscopy 2001, 17, 836–843. [Google Scholar] [CrossRef]
- Takao, M.; Ochi, M.; Oae, K.; Naito, K.; Uchio, Y. Diagnosis of a tear of the tibiofibular syndesmosis. The role of arthroscopy of the ankle. J. Bone Jt. Surg. Br. 2003, 85, 324–329. [Google Scholar] [CrossRef]
- Miyamoto, W.; Takao, M. Management of chronic disruption of the distal tibiofibular syndesmosis. World J. Orthop. 2011, 2, 1–6. [Google Scholar] [CrossRef]
- Nielson, J.H.; Gardner, M.J.; Peterson, M.G.; Sallis, J.G.; Potter, H.G.; Helfet, D.L.; Lorich, D.G. Radiographic measurements do not predict syndesmotic injury in ankle fractures: An MRI study. Clin. Orthop. Relat. Res. 2005, 436, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Ebraheim, N.A.; Lu, J.; Yang, H.; Mekhail, A.O.; Yeasting, R.A. Radiographic and CT evaluation of tibiofibular syndesmotic diastasis: A cadaver study. Foot Ankle Int. 1997, 18, 693–698. [Google Scholar] [CrossRef]
- Vogl, T.J.; Hochmuth, K.; Diebold, T.; Lubrich, J.; Hofmann, R.; Stockle, U.; Sollner, O.; Bisson, S.; Sudkamp, N.; Maeurer, J.; et al. Magnetic resonance imaging in the diagnosis of acute injured distal tibiofibular syndesmosis. Investig. Radiol. 1997, 32, 401–409. [Google Scholar] [CrossRef]
- Oae, K.; Takao, M.; Naito, K.; Uchio, Y.; Kono, T.; Ishida, J.; Ochi, M. Injury of the tibiofibular syndesmosis: Value of MR imaging for diagnosis. Radiology 2003, 227, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Han, S.H.; Lee, J.W.; Kim, S.; Suh, J.S.; Choi, Y.R. Chronic tibiofibular syndesmosis injury: The diagnostic efficiency of magnetic resonance imaging and comparative analysis of operative treatment. Foot Ankle Int. 2007, 28, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Sman, A.D.; Hiller, C.E.; Refshauge, K.M. Diagnostic accuracy of clinical tests for diagnosis of ankle syndesmosis injury: A systematic review. Br. J. Sports Med. 2013, 47, 620–628. [Google Scholar] [CrossRef] [PubMed]
- Christodoulou, G.; Korovessis, P.; Giarmenitis, S.; Dimopoulos, P.; Sdougos, G. The use of sonography for evaluation of the integrity and healing process of the tibiofibular interosseous membrane in ankle fractures. J. Orthop. Trauma 1995, 9, 98–106. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Huh, Y.M.; Song, H.T.; Lee, S.A.; Lee, J.W.; Lee, J.E.; Chung, I.H.; Suh, J.S. Chronic tibiofibular syndesmosis injury of ankle: Evaluation with contrast-enhanced fat-suppressed 3D fast spoiled gradient-recalled acquisition in the steady state MR imaging. Radiology 2007, 242, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Schoennagel, B.P.; Karul, M.; Avanesov, M.; Bannas, P.; Gold, G.; Grossterlinden, L.G.; Rupprecht, M.; Adam, G.; Yamamura, J. Isolated syndesmotic injury in acute ankle trauma: Comparison of plain film radiography with 3T MRI. Eur. J. Radiol. 2014, 83, 1856–1861. [Google Scholar] [CrossRef]
- Yeung, T.W.; Chan, C.Y.G.; Chan, W.C.S.; Yeung, Y.N.; Yuen, M.K. Can pre-operative axial CT imaging predict syndesmosis instability in patients sustaining ankle fractures? Seven years’ experience in a tertiary trauma center. Skelet. Radiol. 2015, 44, 823–829. [Google Scholar] [CrossRef] [PubMed]
- Clanton, T.O.; Ho, C.P.; Williams, B.T.; Surowiec, R.K.; Gatlin, C.C.; Haytmanek, C.T.; LaPrade, R.F. Magnetic resonance imaging characterization of individual ankle syndesmosis structures in asymptomatic and surgically treated cohorts. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 2089–2102. [Google Scholar] [CrossRef] [PubMed]
- Ahn, T.K.; Choi, S.M.; Kim, J.Y.; Lee, W.C. Isolated Syndesmosis Diastasis: Computed Tomography Scan Assessment With Arthroscopic Correlation. Arthrosc. J. Arthrosc. Relat. Surg. 2017, 33, 828–834. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author (year) | Location | No. of Samples | Median Age (Range) | Test | Fracture | Reference | |
|---|---|---|---|---|---|---|---|
| B.P.Schoennagel (2014) | Germany | 84 | 32.8 ± 9.9 | X-ray | no | MRI | |
| M.Takao (2003) | Japan | 52 | 35 (14–67) | X-ray | yes | Arthroscopy | |
| Oae.K (2003) | Japan | 58 | 37.4 (12–79) | X-ray | yes | Arthroscopy | |
| T-K Ahn (2017) | Korea | 78 | 34.2 (15–64) | CT | no | Arthroscopy | |
| T-W Yeung (2015) | Hongkong | 123 | 43.2 (11–82) | CT | yes | Intraoperative findings | |
| S.J.Kim (2007) | Korea | 45 | 32.1 (18–58) | MRI | no | Arthroscopy | |
| M.Takao (2003) | Japan | 52 | 35 (14–67) | MRI | yes | Arthroscopy | |
| Oae.K (2003) | Japan | 58 | 37.4 (12–79) | MRI | yes | Arthroscopy | |
| T.Clanton (2014) | USA | 21 | 35 (16–60) | MRI | no | Arthroscopy | |
| Chirsto.G (1995) | Greece | 90 | 36.5 (18–80) | USG | yes | Intraoperative findings |
| Author (Year) | Location | Detailed Reasons for Selected Population | Detailed Description of Sampling and Measurement Method | Study Participation | Outcome Measurement |
|---|---|---|---|---|---|
| B.P. Schoennagel, 2014 | Germany | Adult patients with acute ankle trauma that presented in our emergency unit | Yes | low 5 | low 3 |
| M.Takao,2003 | Japan | Patients with acute injuries of the ankle which were treated surgically | Yes | moderate 4 | low 3 |
| Oaek,2003 | Japan | Patients with ankle sprains and distal fibular fractures underwent surgery and ankle arthroscopy | Yes | moderate 4 | low3 |
| T.K. Ahn,2017 | Korea | Who underwent an arthroscopic examination for the syndesmosis injury | Yes | low 6 | low 3 |
| T.W.Yeung, 2015 | Hongkong | Patients who received CT scan for preoperative assessment with subsequent operation performed were in | Yes | low 5 | low 3 |
| S.J. Kim,2007 | Korea | Who had a history of repeated ankle sprain and who had undergone MRI and arthroscope surgery | Yes | moderate 4 | low 3 |
| M.Takao,2003 | Japan | Patients with acute injuries of the ankle which were treated surgically | Yes | moderate 4 | low 3 |
| Oae K,2003 | Japan | Patients with ankle sprains and distal fibular fractures underwent surgery and ankle arthroscopy | Yes | moderate 4 | low 3 |
| T. Clanton, 2014 | USA | Who underwent arthroscopically assisted surgery for ankle pathology and suspected syndesmosis injury | Yes | low 6 | moderate 2 |
| Chirsto.G,1995 | Greece | Who had Weber type B and C ankle fracture | Yes | low 5 | low 3 |
| Author | Test | Location | Method | Reference | Unit | Cut-off | TP | FN | FP | TN |
|---|---|---|---|---|---|---|---|---|---|---|
| B.P. Schoennaqel, 2014 | X-ray | 1 | T-F clear | MRI | mm | 5.3 mm | 9 | 2 | 18 | 55 |
| B.P. Schoennaqel, 2014 | X-ray | 2 | Med. clear | MRI | mm | 2.8 mm | 8 | 3 | 30 | 43 |
| M.Takao, 2003† | X-ray | 1 | T-F clear, T-F overlap | Arthroscopy | mm | 10 | 13 | 0 | 29 | |
| M.Takao, 2003† | X-ray | 2 | talar tilt, med. clear space | Arthroscopy | degree, mm | 15 | 8 | 0 | 29 | |
| Oae.K, 2003† | X-ray | 1 | T-F clear | Arthroscopy | mm | 12 | 16 | 0 | 30 | |
| T-K Ahn, 2017 | CT | 1 | Narrowest T-F distance at joint | Arthroscopy | mm | 2 mm | 41 | 13 | 5 | 19 |
| T-W Yeung, 2015 | CT | 1 | Ant. T-F distance | Intraoperative findings | mm | 4 mm | 22 | 17 | 7 | 77 |
| T-W Yeung, 2015 | CT | 1 | Mid T-F distance | Intraoperative findings | mm | 3.95 mm | 29 | 10 | 21 | 63 |
| T-W Yeung, 2015 | CT | 1 | Max T-F distance | Intraoperative findings | mm | 5.65 mm | 29 | 10 | 18 | 66 |
| S.J.Kim, 2007 | MRI | 1 | 1: AITFL was definitely not injured, 2: AITFL was probably not injured, 3: AITFL was possibly injured, 4: AITFL was probably injured, 5, that the AITFL was definitely injured. Thickening, wavy contour, redundancy, discontinuity, or absence of the ligament | Arthroscopy | Signal intensity, score | 4 | 11 | 13 | 8 | 13 |
| S.J.Kim, 2007 | MRI | 1 | 1: AITFL was definitely not injured, 2: AITFL was probably not injured, 3: AITFL was possibly injured, 4: AITFL was probably injured, 5, that the AITFL was definitely injured.Thickening, wavy contour, redundancy, discontinuity, or absence of the ligament | Arthroscopy | Signal intensity, score | 4 | 23 | 1 | 5 | 16 |
| M.Takao, 2003 † | MRI | 1 | Discontinuity, decrease of tension, abnormal course of the ligament | Arthroscopy | Signal intensity | 23 | 0 | 2 | 27 | |
| Oae.K, 2003 † | MRI | 1 | Ligament discontinuity, wavy, curved ligament contour, no visualization of ligament | Arthroscopy | Signal intensity | 28 | 0 | 2 | 28 | |
| Thomas O.Clanton, 2014 † | MRI | 1 | Ligament tear, sprain, scarring | Arthroscopy | Signal intensity | 14 | 2 | 0 | 5 | |
| Chirsto.G, 1995 | USG | 2 | Interosseous membrane | Intraoperative findings | hyperechogenic | 31 | 4 | 3 | 52 |
| DOR | posLR | negLR | PPV | NPV | meta | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Estimate | 95% CI | Estimate | 95% CI | Estimate | 95% CI | Estimate | 95% CI | Estimate | 95% CI | ||||||
| lower | upper | lower | upper | lower | upper | lower | upper | lower | upper | ||||||
| 11.400 | 2.571 | 50.544 | 3.167 | 1.940 | 5.168 | 0.278 | 0.091 | 0.844 | 0.333 | 0.250 | 0.417 | 0.965 | 0.956 | 0.974 | No |
| 3.464 | 0.918 | 13.071 | 1.719 | 1.092 | 2.705 | 0.496 | 0.201 | 1.223 | 0.211 | 0.158 | 0.263 | 0.935 | 0.917 | 0.952 | No |
| 45.889 | 2.502 | 841.714 | 26.250 | 1.619 | 425.584 | 0.572 | 0.401 | 0.817 | 0.955 | 0.929 | 0.980 | 0.686 | 0.622 | 0.750 | No |
| 107.588 | 5.816 | 1990.220 | 38.750 | 2.441 | 615.026 | 0.360 | 0.209 | 0.619 | 0.969 | 0.954 | 0.984 | 0.776 | 0.721 | 0.832 | Yes |
| 46.212 | 2.570 | 831.063 | 26.724 | 1.656 | 431.189 | 0.578 | 0.420 | 0.796 | 0.962 | 0.941 | 0.982 | 0.649 | 0.584 | 0.714 | Yes |
| 11.985 | 3.734 | 38.462 | 3.644 | 1.647 | 8.064 | 0.304 | 0.181 | 0.510 | 0.891 | 0.863 | 0.919 | 0.594 | 0.510 | 0.677 | Yes |
| 14.235 | 5.239 | 38.681 | 6.769 | 3.162 | 14.489 | 0.476 | 0.331 | 0.683 | 0.759 | 0.692 | 0.825 | 0.819 | 0.789 | 0.849 | Yes |
| 8.700 | 3.637 | 20.809 | 2.974 | 1.967 | 4.498 | 0.342 | 0.198 | 0.592 | 0.580 | 0.512 | 0.648 | 0.863 | 0.836 | 0.890 | No |
| 10.633 | 4.376 | 25.837 | 3.470 | 2.215 | 5.437 | 0.326 | 0.189 | 0.563 | 0.617 | 0.549 | 0.685 | 0.868 | 0.843 | 0.894 | No |
| 1.353 | 0.422 | 4.333 | 1.191 | 0.605 | 2.342 | 0.880 | 0.539 | 1.438 | 0.579 | 0.469 | 0.689 | 0.500 | 0.404 | 0.596 | No |
| 47.000 | 6.946 | 318.027 | 3.760 | 1.811 | 7.806 | 0.080 | 0.017 | 0.385 | 0.821 | 0.767 | 0.876 | 0.941 | 0.915 | 0.967 | Yes |
| 517.000 | 23.622 | 11315.436 | 11.750 | 3.581 | 38.556 | 0.023 | 0.001 | 0.354 | 0.904 | 0.870 | 0.937 | 0.982 | 0.976 | 0.989 | Yes |
| 649.800 | 29.851 | 14144.756 | 12.186 | 3.709 | 40.038 | 0.019 | 0.001 | 0.293 | 0.919 | 0.893 | 0.945 | 0.983 | 0.977 | 0.989 | Yes |
| 63.800 | 2.624 | 1551.248 | 10.235 | 0.715 | 146.493 | 0.160 | 0.050 | 0.517 | 0.967 | 0.950 | 0.983 | 0.688 | 0.539 | 0.836 | Yes |
| 134.333 | 28.183 | 640.302 | 16.238 | 5.369 | 49.110 | 0.121 | 0.048 | 0.305 | 0.912 | 0.885 | 0.939 | 0.929 | 0.911 | 0.946 | No |
| Comparison Results | Total (n = 8) | X-ray (n = 2) | CT (n = 2) | MRI (n = 4) | p-value₭ | post-hoc₤ | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Estimate | 95% CI | Estimate | 95% CI | Estimate | 95% CI | Estimate | 95% CI | |||||||
| Lower | Upper | Lower | Upper | Lower | Upper | Lower | Upper | |||||||
| Heterogeneity Test, Higgins’ I2(p value) † | 16.8% (p = 0.274) | 0% (p = 0.897) | 0% (p = 0.906) | 0% (p = 0.592) | ||||||||||
| Sensitivity ‡ | 0.745 | 0.592 | 0.854 | 0.528 | 0.380 | 0.672 | 0.669 | 0.506 | 0.800 | 0.929 | 0.837 | 0.971 | 0.004 | X-ray = CT<MRI |
| Specificity ‡ | 0.882 | 0.815 | 0.927 | 0.984 | 0.893 | 0.998 | 0.870 | 0.739 | 0.941 | 0.865 | 0.753 | 0.931 | MRI=CT =X-ray | |
| AUC ₮ | 0.922 | 0.907 | 0.938 | 0.877 | 0.798 | 0.974 | 0.834 | 0.716 | 0.999 | 0.995 | 0.957 | 1.000 | ||
| pAUC ₮ | 0.817 | 0.783 | 0.854 | N/A | 0.678 | 0.463 | 0.997 | 0.988 | 0.898 | 1.000 | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chun, D.-i.; Cho, J.-h.; Min, T.-H.; Yi, Y.; Park, S.Y.; Kim, K.-H.; Kim, J.H.; Won, S.H. Diagnostic Accuracy of Radiologic Methods for Ankle Syndesmosis Injury: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 968. https://doi.org/10.3390/jcm8070968
Chun D-i, Cho J-h, Min T-H, Yi Y, Park SY, Kim K-H, Kim JH, Won SH. Diagnostic Accuracy of Radiologic Methods for Ankle Syndesmosis Injury: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2019; 8(7):968. https://doi.org/10.3390/jcm8070968
Chicago/Turabian StyleChun, Dong-il, Jae-ho Cho, Tae-Hong Min, Young Yi, Su Yeon Park, Kwang-Hyun Kim, Jae Heon Kim, and Sung Hun Won. 2019. "Diagnostic Accuracy of Radiologic Methods for Ankle Syndesmosis Injury: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 8, no. 7: 968. https://doi.org/10.3390/jcm8070968
APA StyleChun, D.-i., Cho, J.-h., Min, T.-H., Yi, Y., Park, S. Y., Kim, K.-H., Kim, J. H., & Won, S. H. (2019). Diagnostic Accuracy of Radiologic Methods for Ankle Syndesmosis Injury: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 8(7), 968. https://doi.org/10.3390/jcm8070968