Differences in the Effectiveness of Long-Acting Injection and Orally Administered Antipsychotics in Reducing Rehospitalization among Patients with Schizophrenia Receiving Home Care Services


Abstract
:1. Introduction
2. Methods
2.1. Patient Selection
2.2. Statistical Methods
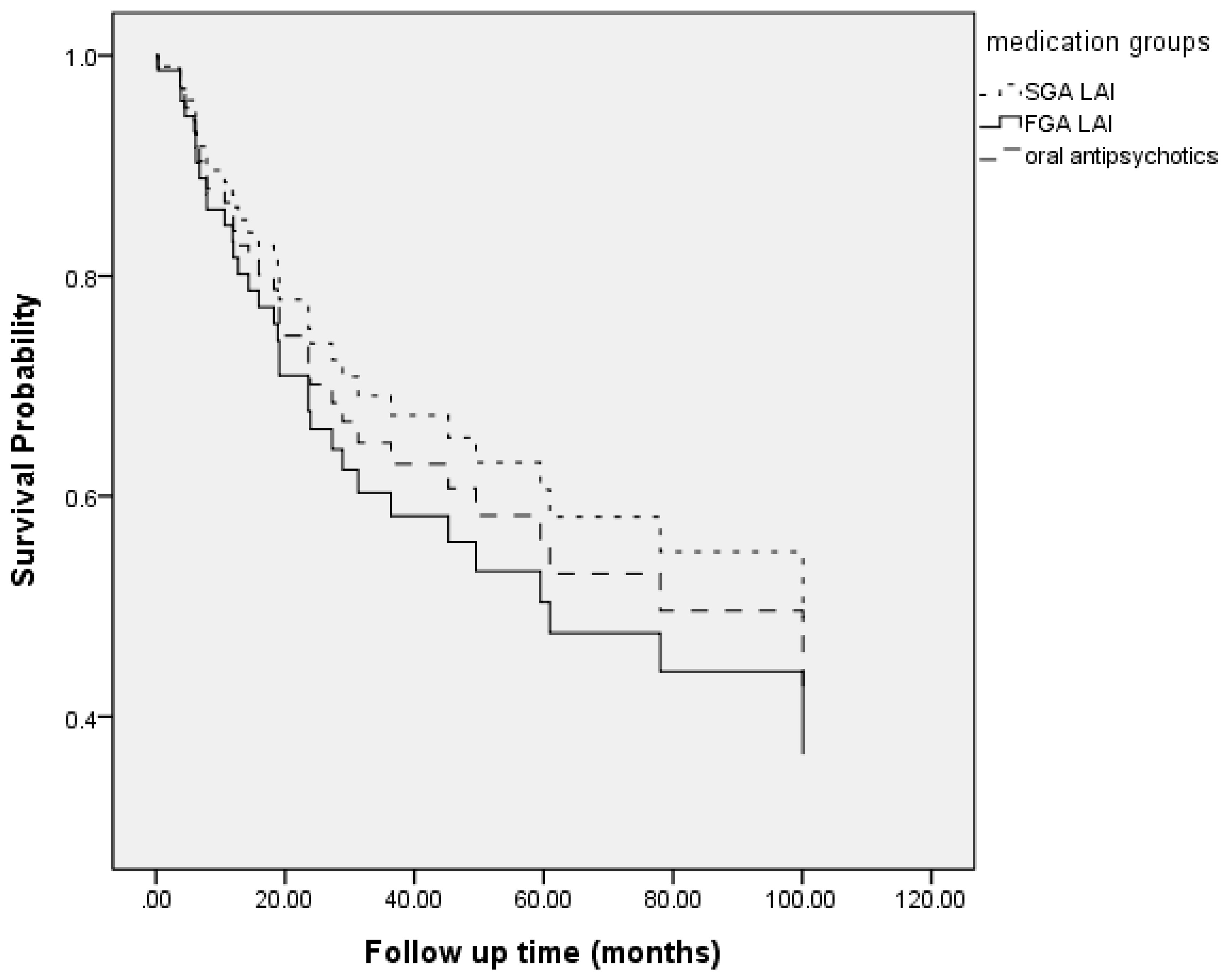
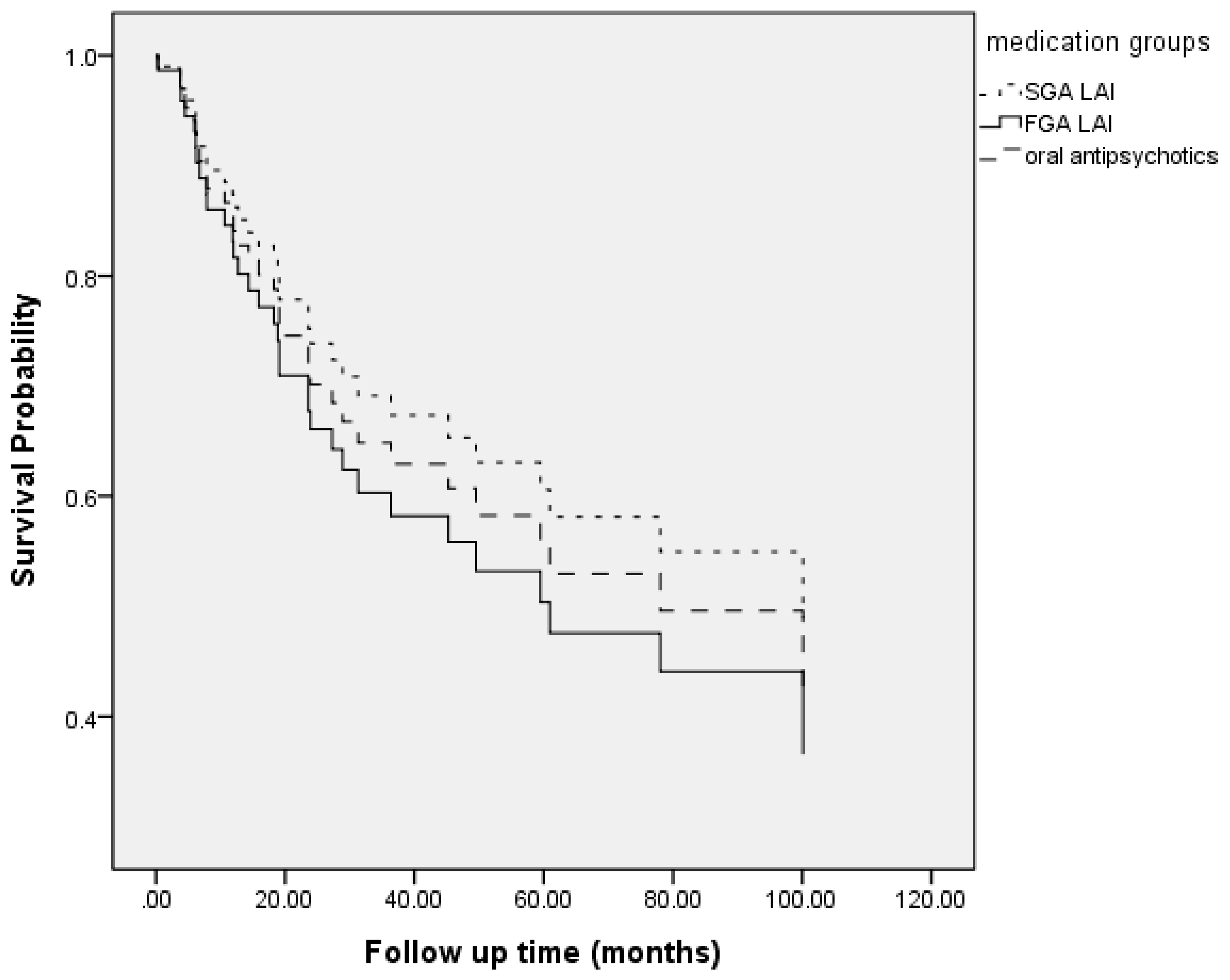
3. Results
Participant Characteristics
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Van Os, J.; Kapur, S. Schizophrenia. Lancet 2009, 374, 635–645. [Google Scholar] [CrossRef]
- Thornicroft, G.; Brohan, E.; Rose, D.; Sartorius, N.; Leese, M.; INDIGO Study Group. Global pattern of experienced and anticipated discrimination against people with schizophrenia: A cross-sectional survey. Lancet 2009, 373, 408–415. [Google Scholar] [CrossRef]
- Kane, J.M. Treatment strategies to prevent relapse and encourage remission. J. Clin. Psychiatry 2007, 68 (Suppl. 14), 27–30. [Google Scholar] [PubMed]
- Carbon, M.; Correll, C.U. Clinical predictors of therapeutic response to antipsychotics in schizophrenia. Dialogues Clin. Neurosci. 2014, 16, 505–524. [Google Scholar] [PubMed]
- Kane, J.M.; Kishimoto, T.; Correll, C.U. Non-adherence to medication in patients with psychotic disorders: Epidemiology, contributing factors and management strategies. World Psychiatry 2013, 12, 216–226. [Google Scholar] [CrossRef]
- Rosenheck, R.A.; Krystal, J.H.; Lew, R.; Barnett, P.G.; Fiore, L.; Valley, D.; Thwin, S.S.; Vertrees, J.E.; Liang, M.H.; CSP555 Research Group. Long-acting risperidone and oral antipsychotics in unstable schizophrenia. N. Engl. J. Med. 2011, 364, 842–851. [Google Scholar] [CrossRef]
- Haddad, P.M.; Brain, C.; Scott, J. Nonadherence with antipsychotic medication in schizophrenia: Challenges and management strategies. Patient Relat. Outcome Meas. 2014, 5, 43–62. [Google Scholar] [CrossRef]
- Xiao, J.; Mi, W.; Li, L.; Shi, Y.; Zhang, H. High relapse rate and poor medication adherence in the Chinese population with schizophrenia: Results from an observational survey in the People’s Republic of China. Neuropsychiatr. Dis. Treat. 2015, 11, 1161–1167. [Google Scholar] [CrossRef]
- Orsolini, L.; Tomasetti, C.; Valchera, A.; Vecchiotti, R.; Matarazzo, I.; Vellante, F.; Iasevoli, F.; Buonaguro, E.F.; Fornaro, M.; Fiengo, A.L.; et al. An update of safety of clinically used atypical antipsychotics. Expert Opin. Drug Saf. 2016, 15, 1329–1347. [Google Scholar] [CrossRef]
- De Berardis, D.; Marini, S.; Carano, A.; Lang, A.P.; Cavuto, M.; Piersanti, M.; Fornaro, M.; Perna, G.; Valchera, A.; Mazza, M.; et al. Efficacy and safety of long acting injectable atypical antipsychotics: A review. Curr. Clin. Pharmacol. 2013, 8, 256–264. [Google Scholar] [CrossRef]
- Correll, C.U.; Citrome, L.; Haddad, P.M.; Lauriello, J.; Olfson, M.; Calloway, S.M.; Kane, J.M. The use of long-acting injectable antipsychotics in schizophrenia: evaluating the evidence. J. Clin. Psychiatry 2016, 77, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Heres, S.; Lambert, M.; Vauth, R. Treatment of early episode in patients with schizophrenia: The role of long acting antipsychotics. Eur. Psychiatry 2014, 29 (Suppl. 2), 1409–1413. [Google Scholar] [CrossRef]
- Pietrini, F.; Albert, U.; Ballerini, A.; Calo, P.; Maina, G.; Pinna, F.; Vaggi, M.; Boggian, I.; Fontana, M.; Moro, C.; et al. The modern perspective for long-acting injectables antipsychotics in the patient-centered care of schizophrenia. Neuropsychiatr. Dis. Treat. 2019, 15, 1045–1060. [Google Scholar] [CrossRef] [PubMed]
- Brissos, S.; Veguilla, M.R.; Taylor, D.; Balanza-Martinez, V. The role of long-acting injectable antipsychotics in schizophrenia: A critical appraisal. Ther. Adv. Psychopharmacol. 2014, 4, 198–219. [Google Scholar] [CrossRef] [PubMed]
- Newcomer, J.W. Second-generation (atypical) antipsychotics and metabolic effects: A comprehensive literature review. CNS Drugs 2005, 19 (Suppl. 1), 1–93. [Google Scholar] [CrossRef] [PubMed]
- Goff, D.C.; Sullivan, L.M.; McEvoy, J.P.; Meyer, J.M.; Nasrallah, H.A.; Daumit, G.L.; Lamberti, S.; D’Agostino, R.B.; Stroup, T.S.; Davis, S.; et al. A comparison of ten-year cardiac risk estimates in schizophrenia patients from the CATIE study and matched controls. Schizophr. Res. 2005, 80, 45–53. [Google Scholar] [CrossRef]
- Leucht, S.; Corves, C.; Arbter, D.; Engel, R.R.; Li, C.; Davis, J.M. Second-generation versus first-generation antipsychotic drugs for schizophrenia: A meta-analysis. Lancet 2009, 373, 31–41. [Google Scholar] [CrossRef]
- Rosenheck, R.; Lin, H. Noninferiority of perphenazine vs. three second-generation antipsychotics in chronic schizophrenia. J. Nerv. Ment. Dis. 2014, 202, 18–24. [Google Scholar] [CrossRef]
- McEvoy, J.P.; Byerly, M.; Hamer, R.M.; Dominik, R.; Swartz, M.S.; Rosenheck, R.A.; Ray, N.; Lamberti, J.S.; Buckley, P.F.; Wilkins, T.M.; et al. Effectiveness of paliperidone palmitate vs haloperidol decanoate for maintenance treatment of schizophrenia: A randomized clinical trial. JAMA 2014, 311, 1978–1987. [Google Scholar] [CrossRef]
- Dieterich, M.; Irving, C.B.; Park, B.; Marshall, M. Intensive case management for severe mental illness. Cochrane Database Syst. Rev. 2010, CD007906. [Google Scholar] [CrossRef]
- Ju, P.C.; Chou, F.H.; Lai, T.J.; Chuang, P.Y.; Lin, Y.J.; Yang, C.W.; Tang, C.H. Long-acting injectables and risk for rehospitalization among patients with schizophrenia in the home care program in Taiwan. J. Clin. Psychopharmacol. 2014, 34, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Tham, X.C.; Xie, H.; Chng, C.M.; Seah, X.Y.; Lopez, V.; Klainin-Yobas, P. Factors affecting medication adherence among adults with schizophrenia: A literature review. Arch. Psychiatr. Nurs. 2016, 30, 797–809. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| FGA Depot | SGA Depot | Oral Medication | F or χ2 | p | Post Hoc | |
|---|---|---|---|---|---|---|
| n | 19 | 42 | 17 | |||
| Sex (male/female) (n) | 9/10 | 20/22 | 2/15 | 7.1 | 0.029 * | SGA = FGA ≠ Oral |
| Age (years) | 47.4 ± 11.9 | 47.9 ± 10.5 | 57.9 ± 17.2 | 4.6 | 0.013 * | FGA = SGA ≠ Oral |
| Onset age (years) | 29.8 ± 8.9 | 32.5 ± 11.2 | 35.4 ± 14.4 | 1.0 | 0.36 | |
| Education (≤9 years, >9 years) (n) | 5/14 | 11/31 | 10/7 | 6.4 | 0.042 * | SGA = FGA > Oral |
| Marital status (single/married divorced) (n) | 9/9/1 | 25/12/5 | 5/11/1 | 7.2 | 0.12 | |
| Job (yes/no) (n) | 1/18 | 7/35 | 1/16 | 2.35 | 0.31 | |
| Hospitalization times before home care service (n) | 5 ± 3.5 | 2.2 ± 1.5 | 2.1 ± 1.4 | 12.3 | <0.001 * | SGA = Oral < FGA |
| Hospitalization duration before home care service (months) | 7.1 ± 6.4 | 3.1 ± 2.5 | 2.4 ± 1.7 | 9.3 | <0.001 * | SGA = Oral < FGA |
| FGA Depot | SGA Depot | Oral Medication | F or χ2 | p | Post hoc | |
|---|---|---|---|---|---|---|
| n = 19 | n = 42 | n = 17 | ||||
| Follow up period under home care service (months) | 44.4 ± 39.4 | 37.8 ± 32.3 | 40.5 ± 34.4 | 0.24 | 0.79 | |
| Rehospitalization rate after home service care (%) | 36.8 | 47.6 | 35.3 | 1.06 | 0.59 |
| Exp(B) | 95%CI | p | |
|---|---|---|---|
| Treatment Groups | |||
| Oral medication | 1 | ||
| FGA | 0.77 | 0.22–2.62 | 0.61 |
| SGA | 1.17 | 0.43–3.18 | 0.76 |
| Sex | 1.38 | 0.67–2.86 | 0.38 |
| Age | 0.98 | 0.95–1.02 | 0.30 |
| Education | 1.22 | 0.53–2.77 | 0.64 |
| Hospitalization times before home care service | 1.04 | 0.89–1.20 | 1.04 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, H.-F.; Kao, C.-C.; Lu, T.; Ying, J.C.; Lee, S.-Y. Differences in the Effectiveness of Long-Acting Injection and Orally Administered Antipsychotics in Reducing Rehospitalization among Patients with Schizophrenia Receiving Home Care Services. J. Clin. Med. 2019, 8, 823. https://doi.org/10.3390/jcm8060823
Hsu H-F, Kao C-C, Lu T, Ying JC, Lee S-Y. Differences in the Effectiveness of Long-Acting Injection and Orally Administered Antipsychotics in Reducing Rehospitalization among Patients with Schizophrenia Receiving Home Care Services. Journal of Clinical Medicine. 2019; 8(6):823. https://doi.org/10.3390/jcm8060823
Chicago/Turabian StyleHsu, Hsiao-Fen, Chia-Chan Kao, Ti Lu, Jeremy C. Ying, and Sheng-Yu Lee. 2019. "Differences in the Effectiveness of Long-Acting Injection and Orally Administered Antipsychotics in Reducing Rehospitalization among Patients with Schizophrenia Receiving Home Care Services" Journal of Clinical Medicine 8, no. 6: 823. https://doi.org/10.3390/jcm8060823
APA StyleHsu, H.-F., Kao, C.-C., Lu, T., Ying, J. C., & Lee, S.-Y. (2019). Differences in the Effectiveness of Long-Acting Injection and Orally Administered Antipsychotics in Reducing Rehospitalization among Patients with Schizophrenia Receiving Home Care Services. Journal of Clinical Medicine, 8(6), 823. https://doi.org/10.3390/jcm8060823