Prevention of Sudden Death Related to Sport: The Science of Basic Life Support—From Theory to Practice

 ,
,  , ,
, ,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Methodology
3. Results
3.1. Sudden Death and Sport: General Aspects and Presumed Causes
3.2. Cardiac Death and Sport: Is It Possible to Prevent It?
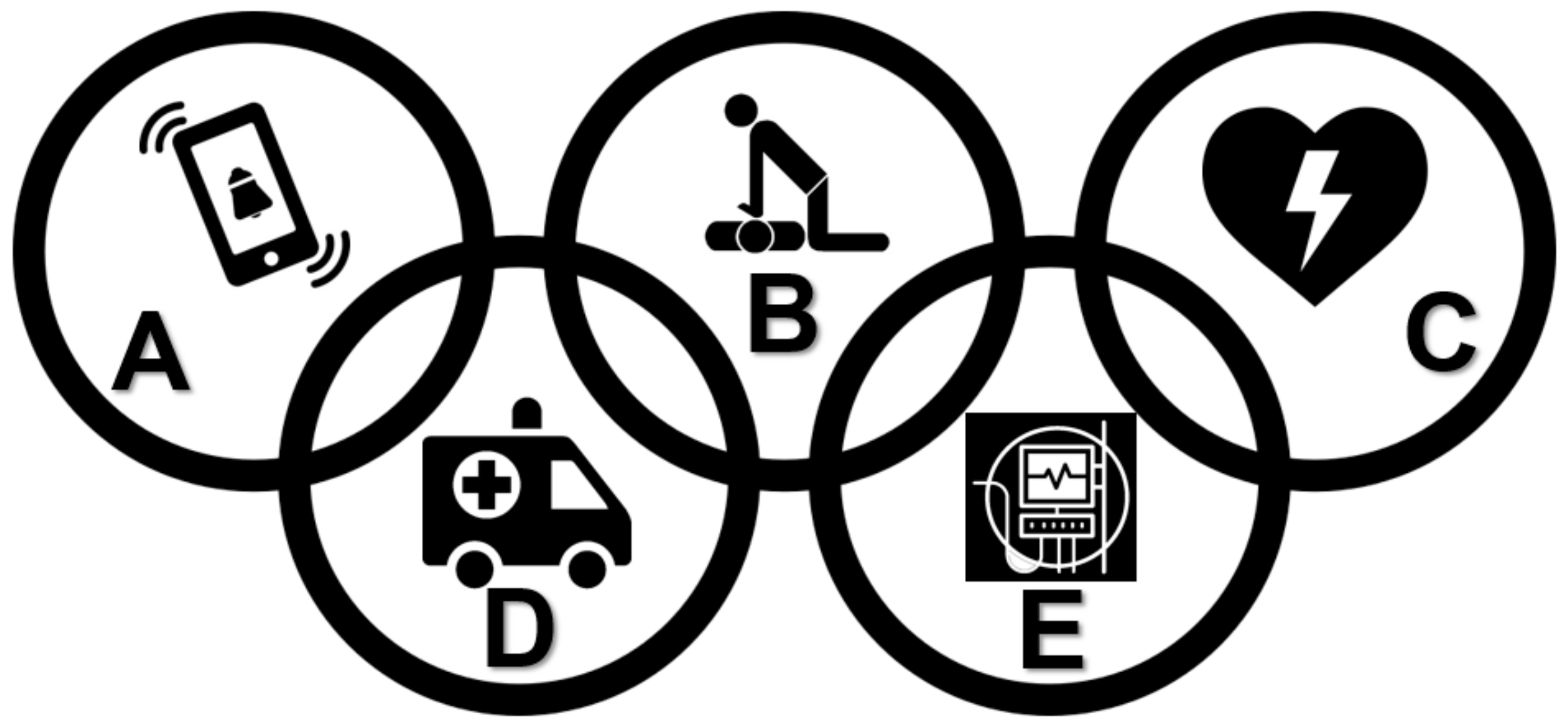
3.3. Strategies for Prevention and Treatment of Sudden Cardiac Death Related to Sport
- Assess whether the location is safe in order to ensure there is no physical risk for the rescuer and the victim;
- Evaluate if the victim is aware by touching your shoulders and asking out loud, “Are you okay?” and/or “Can you hear me?”;
- Ask for help, call the EMS, and request an AED;
- Check at the same time whether the victim has pulse and normal breathing;
- Observe for effective movement of the chest and palpate the carotid pulse for a maximum of 10 s;
- If the patient has a pulse and breathes normally, monitor the patient until the EMS arrives;
- If the victim has a pulse but abnormal breathing, initiate rescue breaths by administering one ventilation every 6 s. In this situation, reassess the victim every two minutes, until the EMS arrives;
- In the absence of pulse, initiate high-quality CPR immediately, intercalating 30 external chest compressions (ECC) cycles with two ventilations, until the arrival of the EMS and AED (Figure 3).
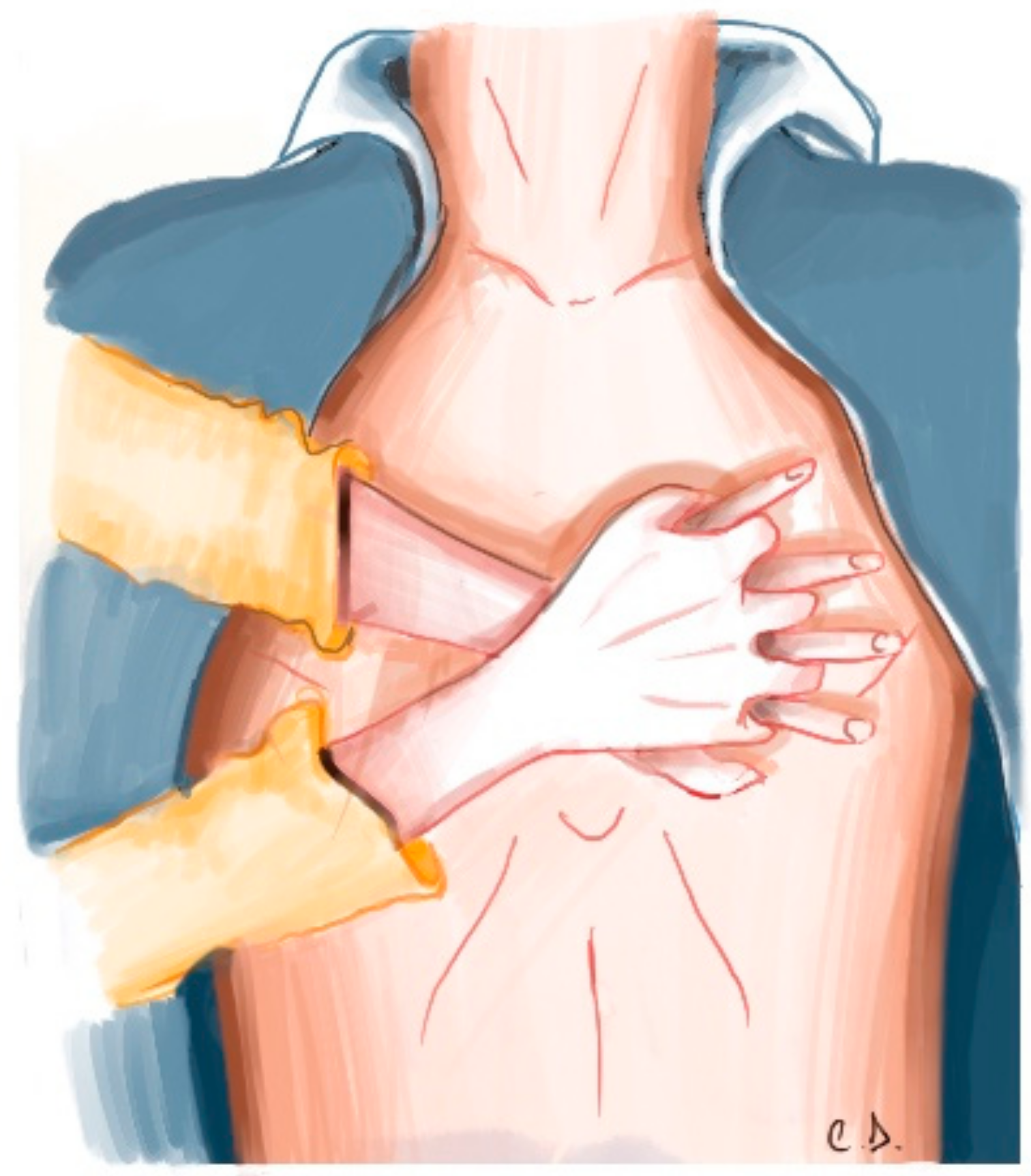
- Put the victim in the supine position and on a flat and rigid surface;
- Place the hypothenar region of the dominant hand in the lower half of the sternum of the victim and the other hand parallel to the first;
- Keep the elbows extended, forming an angle of 90° in a horizontal plane;
- Compress the chest to the depth of 5 to 6 cm in a rhythm (frequency—trained in conjunction with metronome—of 100 to 120 compressions/minute, allowing the total return of the thorax at each compression;
- After 30 ECC, perform two ventilations;
- For ventilation to be effective, open the airways before applying them and observe the elevation of the chest at each ventilation;
- The ventilations should be fast, lasting approximately 1 s and performed with the bag-valve-mask device coupled to the oxygen source (when possible);
- Relieve the rescuer who does the ECC every two minutes, thus avoiding their fatigue and decreasing the quality of the CPR.
- Place the adhesive pads on the patient’s chest—below the right clavicle and at the apex from heart;
- Attach the blade connector to the unit;
- Evaluate the heart rhythm. During the analysis of the rhythm and application of the shock, make sure that you and others are away from the victim;
- After the shock, immediately start CPR for two minutes.
- For children, if two rescuers are available to do CPR, the compression to breaths ratio is 15:2; if only one rescuer is available, the ratio is 30:2 for all age groups.
- For very small children, you can use one-handed chest compressions.
- The depth of compression may be different. For a child, compress the chest at least one-third the depth of the chest. This may be less than two inches for small children but will be approximately two inches for larger children.
- If you are the only person at the scene and find an unresponsive child, perform CPR for two minutes BEFORE you call EMS or go and look for an AED.
- In children, primary cardiac events are not common. Cardiac arrest is most commonly preceded by respiratory problems. Survival rates improve with early intervention for respiratory problems. Remember that prevention is the first link in the pediatric chain of survival!
- If you witness a cardiac arrest in a child, call EMS and get an AED just as you would in the adult BLS sequence
4. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Vancini-Campanharo, C.R.; Vancini, R.L.; de Lira, C.A.B.; Andrade, M.S.; Teixeira Lopes, M.C.B.; Okuno, M.F.P.; Batista, R.E.A.; Atallah, Á.N.; de Góis, A.F.T. Characterization of cardiac arrest in the emergency department of a brazilian university reference hospital: A prospective study. Indian J. Med Res. 2016, 144, 552–559. [Google Scholar]
- Marijon, E.; Uy-Evanado, A.; Reinier, K.; Teodorescu, C.; Narayanan, K.; Jouven, X.; Gunson, K.; Jui, J.; Chugh, S.S. Sudden cardiac arrest during sports activity in middle age. Circulation 2015, 131, 1384–1391. [Google Scholar] [CrossRef]
- Mosterd, A. Pre-participation screening of asymptomatic athletes: “Don’t do stupid stuff”. Neth. Heart J. 2018, 26, 123–126. [Google Scholar] [CrossRef]
- Sheppard, M.N. Aetiology of sudden cardiac death in sport: A histopathologist’s perspective. Br. J. Sports Med. 2012, 46, i15–i21. [Google Scholar] [CrossRef] [PubMed]
- Liberthson, R.R. Sudden death from cardiac causes in children and young adults. N. Engl. J. Med. 1996, 334, 1039–1044. [Google Scholar] [CrossRef]
- Lippi, G.; Favaloro, E.J.; Sanchis-Gomar, F. Sudden cardiac and noncardiac death in sports: Epidemiology, causes, pathogenesis, and prevention. Semin. Thromb. Hemost. 2018, 44, 780–786. [Google Scholar]
- Maron, B.J.; Shirani, J.; Poliac, L.C.; Mathenge, R.; Roberts, W.C.; Mueller, F.O. Sudden death in young competitive athletes: Clinical, demographic, and pathological profiles. J. Am. Med. Assoc. 1996, 276, 199–204. [Google Scholar] [CrossRef]
- Harris, K.M.; Creswell, L.L.; Haas, T.S.; Thomas, T.; Tung, M.; Isaacson, E.; Garberich, R.F.; Maron, B.J. Death and cardiac arrest in U.S. Triathlon participants, 1985 to 2016: A case series. Ann. Intern. Med. 2017, 167, 529–536. [Google Scholar] [CrossRef]
- Knechtle, B.; Nikolaidis, P.T. Physiology and pathophysiology in ultra-marathon running. Front. Physiol. 2018, 9, 634. [Google Scholar] [CrossRef] [PubMed]
- Strachan, A.F.; Noakes, T.D.; Kotzenberg, G.; Nel, A.E.; de Beer, F.C. C reactive protein concentrations during long distance running. Br. Med. J. 1984, 289, 1249–1251. [Google Scholar] [CrossRef]
- Leal, A.G.F.; Vancini, R.L.; Gentil, P.; Benedito-Silva, A.A.; da Silva, A.C.; Campos, M.H.; Andrade, M.S.; de Lira, C.A.B. Knowledge about sport and exercise science: A cross-sectional survey among health professionals in brazil. Health Educ. 2018, 118, 250–261. [Google Scholar] [CrossRef]
- Vora, A.; Burkule, N.; Contractor, A.; Bhargava, K. Prevention of sudden cardiac death in athletes, sportspersons and marathoners in India. Indian Heart J. 2018, 70, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Ransone, J.; Dunn-Bennett, L.R. Assessment of first-aid knowledge and decision making of high school athletic coaches. J. Athl. Train. 1999, 34, 267–271. [Google Scholar]
- Peterson, D.F.; Siebert, D.M.; Kucera, K.L.; Thomas, L.C.; Maleszewski, J.J.; Lopez-Anderson, M.; Suchsland, M.Z.; Harmon, K.G.; Drezner, J.A. Etiology of sudden cardiac arrest and death in us competitive athletes: A 2-year prospective surveillance study. Clin. J. Sport Med. 2018. [Google Scholar] [CrossRef] [PubMed]
- Eckart, R.E.; Scoville, S.L.; Campbell, C.L.; Shry, E.A.; Stajduhar, K.C.; Potter, R.N.; Pearse, L.A.; Virmani, R. Sudden death in young adults: A 25-year review of autopsies in military recruits. Ann. Intern. Med. 2004, 141, 829–834. [Google Scholar] [CrossRef]
- Lobo, S.W.; Pant, S.; Kharoshah, M.A.; Senthilkumaran, S.; Riaz, N.; Menezes, R.G. Can rhabdomyolysis be a cause of sudden death in young athletes? Med. Hypotheses 2011, 77, 935. [Google Scholar] [CrossRef]
- Maron, B.J. Clinical course and management of hypertrophic cardiomyopathy. N. Engl. J. Med. 2018, 379, 655–668. [Google Scholar] [CrossRef] [PubMed]
- Montagnana, M.; Lippi, G.; Franchini, M.; Banfi, G.; Guidi, G.C. Sudden cardiac death in young athletes. Intern. Med. 2008, 47, 1373–1378. [Google Scholar] [CrossRef][Green Version]
- Montagnana, M.; Lippi, G.; Franchini, M.; Targher, G.; Cesare Guidi, G. Sudden cardiac death: Prevalence, pathogenesis, and prevention. Ann. Med. 2008, 40, 360–375. [Google Scholar] [CrossRef]
- Palmieri, V.; Gervasi, S.; Bianco, M.; Cogliani, R.; Poscolieri, B.; Cuccaro, F.; Marano, R.; Mazzari, M.; Basso, C.; Zeppilli, P. Anomalous origin of coronary arteries from the “wrong” sinus in athletes: Diagnosis and management strategies. Int. J. Cardiol. 2018, 252, 13–20. [Google Scholar] [CrossRef]
- Maron, B.J. Sudden death in young athletes. N. Engl. J. Med. 2003, 349, 1064–1075. [Google Scholar] [CrossRef]
- Maron, B.J.; Ommen, S.R.; Semsarian, C.; Spirito, P.; Olivotto, I.; Maron, M.S. Hypertrophic cardiomyopathy: Present and future, with translation into contemporary cardiovascular medicine. J. Am. Coll. Cardiol. 2014, 64, 83–99. [Google Scholar] [CrossRef] [PubMed]
- Sweeting, J.; Semsarian, C. Sudden cardiac death in athletes. Heart Lung Circ. 2018, 27, 1072–1077. [Google Scholar] [CrossRef] [PubMed]
- Fiuza-Luces, C.; Garatachea, N.; Berger, N.A.; Lucia, A. Exercise is the real polypill. Physiology 2013, 28, 330–358. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Saltin, B. Exercise as medicine—Evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sports 2015, 25, 1–72. [Google Scholar] [CrossRef]
- Elliott, P.; Andersson, B.; Arbustini, E.; Bilinska, Z.; Cecchi, F.; Charron, P.; Dubourg, O.; Kühl, U.; Maisch, B.; McKenna, W.J.; et al. Classification of the cardiomyopathies: A position statement from the european society of cardiology working group on myocardial and pericardial diseases. Eur. Heart J. 2008, 29, 270–276. [Google Scholar] [CrossRef]
- Elliott, P.M.; Anastasakis, A.; Borger, M.A.; Borggrefe, M.; Cecchi, F.; Charron, P.; Hagege, A.A.; Lafont, A.; Limongelli, G.; Mahrholdt, H.; et al. 2014 esc guidelines on diagnosis and management of hypertrophic cardiomyopathy: The task force for the diagnosis and management of hypertrophic cardiomyopathy of the european society of cardiology (esc). Eur. Heart J. 2014, 35, 2733–2779. [Google Scholar]
- Villa, A.D.; Sammut, E.; Nair, A.; Rajani, R.; Bonamini, R.; Chiribiri, A. Coronary artery anomalies overview: The normal and the abnormal. World J. Radiol. 2016, 8, 537–555. [Google Scholar] [CrossRef]
- American Heart Association. Heart Attack or Sudden Cardiac Arrest: How Are They Different? Available online: www.heart.org/en/health-topics/heart-attack/about-heart-attacks/heart-attack-or-sudden-cardiac-arrest-how-are-they-different.
- Tarasoutchi, F.; Montera, M.W.; Grinberg, M.; Pineiro, D.J.; Sanchez, C.R.; Bacelar, A.C.; Lopes, A.S.; Fernandes, J.R.; Pires, L.J.; Moraes, R.C.; et al. Brazilian guidelines for valve disease—sbc 2011/i guideline inter-american valve disease—2011 siac. Arq. Bras. Cardiol. 2011, 97, 1–67. [Google Scholar] [CrossRef]
- Schultz, J.C.; Hilliard, A.A.; Cooper, L.T., Jr.; Rihal, C.S. Diagnosis and treatment of viral myocarditis. Mayo Clin. Proc. 2009, 84, 1001–1009. [Google Scholar] [CrossRef]
- Mayo Clinic Staff. Coronary Artery Disease: Symptoms and Causes. Available online: https://www.mayoclinic.org/diseases-conditions/coronary-artery-disease/symptoms-causes/syc-20350613 (accessed on 12 December 2018).
- Hepburn-Brown, M.; Darvall, J.; Hammerschlag, G. Acute pulmonary embolism: A concise review of diagnosis and management. Intern. Med. J. 2019, 49, 15–27. [Google Scholar] [CrossRef]
- Mayo Clinic Staff. Stroke: Symptoms and Causes. Available online: https://www.mayoclinic.org/diseases-conditions/stroke/symptoms-causes/syc-20350113 (accessed on 12 December 2018).
- Koźniewska, E.; Podlecka, A.; Rafałowska, J. Hyponatremic encephalopathy—Some experimental and clinical findings. Folia Neuropathol. 2003, 41, 41–45. [Google Scholar]
- Achinger, S.G.; Ayus, J.C. Treatment of hyponatremic encephalopathy in the critically ill. Crit. Care Med. 2017, 45, 1762–1771. [Google Scholar] [CrossRef]
- Desforges, J.F.; Simon, H.B. Hyperthermia. N. Engl. J. Med. 1993, 329, 483–487. [Google Scholar] [CrossRef]
- Zimmerman, J.L.; Shen, M.C. Rhabdomyolysis. Chest 2013, 144, 1058–1065. [Google Scholar] [CrossRef]
- National Heart, Lung, and Blood Institute (NHLBI). Respiratory Failure. Available online: https://www.nhlbi.nih.gov/health-topics/respiratory-failure (accessed on 12 December 2018).
- Sadiq, U.; Grossman, S.A. Rhythm, pulseless electrical activity. In Statpearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2019. [Google Scholar]
- Gangadharan, S.; Nawathe, P.; Schleien, C.L. 40 cardiopulmonary resuscitation. In A Practice of Anesthesia for Infants and Children, 6th ed.; Coté, C.J., Lerman, J., Anderson, B.J., Eds.; Elsevier: Philadelphia, PA, USA, 2019; pp. 908–920.e904. [Google Scholar]
- Ferreira, M.; Santos-Silva, P.R.; de Abreu, L.C.; Valenti, V.E.; Crispim, V.; Imaizumi, C.; Filho, C.F.; Murad, N.; Meneghini, A.; Riera, A.R.; et al. Sudden cardiac death athletes: A systematic review. Sports Med. Arthrosc. Rehabil. Ther. Technol. 2010, 2, 19. [Google Scholar] [CrossRef]
- Asif, I.M.; Harmon, K.G. Incidence and etiology of sudden cardiac death: New updates for athletic departments. Sports Health 2017, 9, 268–279. [Google Scholar] [CrossRef] [PubMed]
- Bohm, P.; Scharhag, J.; Meyer, T. Data from a nationwide registry on sports-related sudden cardiac deaths in Germany. Eur. J. Prev. Cardiol. 2016, 23, 649–656. [Google Scholar] [CrossRef]
- Wasfy, M.M.; Hutter, A.M.; Weiner, R.B. Sudden cardiac death in athletes. Methodist Debakey Cardiovasc. J. 2016, 12, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. Heart disease and stroke statistics-2013 update: A report from the american heart association. Circulation 2013, 127, e6–e245. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez, M.M.; Timerman, S.; de Oliveira, R.G.; Polastri, T.F.; Dallan, L.A.P.; Araújo, S.; Lage, S.G.; Schmidt, A.; de Bernoche, C.S.M.; Canesin, M.F.; et al. I guideline for cardiopulmonary resuscitation and emergency cardiovascular care—Brazilian society of cardiology: Executive summary. Arq. Bras. Cardiol. 2013, 100, 105–113. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart disease and stroke statistics—2018 update: A report from the american heart association. Circulation 2018, 137, E67–E492. [Google Scholar] [CrossRef]
- Heart Rhythm Society. Sudden Cardiac Arrest (sca). Available online: www.hrsonline.org/Patient-Resources/Heart-Diseases-Disorders/Sudden-Cardiac-Arrest-SCA (accessed on 12 December 2018).
- Aehlert, B. Acls, Suporte Avançado de Vida em Cardiologia: Emergências em Cardiologia, 4th ed.; Elsevier: Rio de Janeiro, Brazil, 2013. [Google Scholar]
- Prech, M.; Bartela, E.; Szymak-Pawełczyk, B. An amateur marathon runner after sudden cardiac arrest. Whether and when can he return to sport competition? Pol. Merkur. Lek. Organ Pol. Tow. Lek. 2018, 45, 71–74. [Google Scholar]
- Landry, C.H.; Allan, K.S.; Connelly, K.A.; Cunningham, K.; Morrison, L.J.; Dorian, P. Sudden cardiac arrest during participation in competitive sports. N. Engl. J. Med. 2017, 377, 1943–1953. [Google Scholar] [CrossRef] [PubMed]
- Zorzi, A.; Susana, A.; Spadotto, V.; Cacciavillani, L.; Corrado, D. Sudden cardiac arrest in italian sports facilities in 2015: Possible epidemiological implications of the application of the “balduzzi decree”. G. Ital. Cardiol. 2016, 17, 903–907. [Google Scholar]
- Harmon, K.G.; Asif, I.M.; Maleszewski, J.J.; Owens, D.S.; Prutkin, J.M.; Salerno, J.C.; Zigman, M.L.; Ellenbogen, R.; Rao, A.L.; Ackerman, M.J.; et al. Incidence and etiology of sudden cardiac arrest and death in high school athletes in the united states. Mayo Clin. Proc. 2016, 91, 1493–1502. [Google Scholar] [CrossRef] [PubMed]
- Solberg, E.E.; Borjesson, M.; Sharma, S.; Papadakis, M.; Wilhelm, M.; Drezner, J.A.; Harmon, K.G.; Alonso, J.M.; Heidbuchel, H.; Dugmore, D.; et al. Sudden cardiac arrest in sports—Need for uniform registration: A position paper from the sport cardiology section of the european association for cardiovascular prevention and rehabilitation. Eur. J. Prev. Cardiol. 2016, 23, 657–667. [Google Scholar] [CrossRef] [PubMed]
- Cronin, O.; Jordan, J.; Quigley, F.; Molloy, M.G. Prepared for sudden cardiac arrest? A cross-sectional study of automated external defibrillators in amateur sport. Br. J. Sports Med. 2013, 47, 1171–1174. [Google Scholar] [CrossRef] [PubMed]
- Marijon, E.; Bougouin, W.; Celermajer, D.S.; Périer, M.C.; Dumas, F.; Benameur, N.; Karam, N.; Lamhaut, L.; Tafflet, M.; Mustafic, H.; et al. Characteristics and outcomes of sudden cardiac arrest during sports in women. Circ. Arrhythmia Electrophysiol. 2013, 6, 1185–1191. [Google Scholar] [CrossRef]
- Enright, K.; Turner, C.; Roberts, P.; Cheng, N.; Browne, G. Primary cardiac arrest following sport or exertion in children presenting to an emergency department: Chest compressions and early defibrillation can save lives, but is intravenous epinephrine always appropriate? Pediatr. Emerg. Care 2012, 28, 336–339. [Google Scholar] [CrossRef] [PubMed]
- Kramer, E.; Dvorak, J.; Kloeck, W. Review of the management of sudden cardiac arrest on the football field. Br. J. Sports Med. 2010, 44, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Cappato, R.; Furlanello, F.; Giovinazzo, V.; Infusino, T.; Lupo, P.; Pittalis, M.; Foresti, S.; De Ambroggi, G.; Ali, H.; Bianco, E.; et al. J wave, qrs slurring, and st elevation in athletes with cardiac arrest in the absence of heart disease marker of risk or innocent bystander? Circ. Arrhythmia Electrophysiol. 2010, 3, 305–311. [Google Scholar] [CrossRef]
- Furlanello, F.; Bertoldi, A.; Dallago, M.; Furlanello, C.; Fernando, F.; Inama, G.; Pappone, C.; Chierchia, S. Cardiac arrest and sudden death in competitive athletes with arrhythmogenic right ventricular dysplasia. Pace Pacing Clin. Electrophysiol. 1998, 21, 331–335. [Google Scholar] [CrossRef]
- Maron, B.J.; Poliac, L.C.; Kaplan, J.A.; Mueller, F.O. Blunt impact to the chest leading to sudden death from cardiac arrest during sports activities. N. Engl. J. Med. 1995, 333, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Peters, S.; Reil, G.H. Risk factors of cardiac arrest in arrhythmogenic right ventricular dysplasia. Eur. Heart J. 1995, 16, 77–80. [Google Scholar] [CrossRef]
- Dietlen, H.; Mies, M.; Stormer, A. Acute cardiac arrest in sport exercise and work. Münch. Med. Wochensch. 1953, 95, 755–756. [Google Scholar]
- Karam, N.; Narayanan, K.; Bougouin, W.; Benameur, N.; Beganton, F.; Jost, D.; Lamhaut, L.; Perier, M.C.; Cariou, A.; Celermajer, D.S.; et al. Major regional differences in automated external defibrillator placement and basic life support training in france: Further needs for coordinated implementation. Resuscitation 2017, 118, 49–54. [Google Scholar] [CrossRef]
- Gonzalez, M.M.; Marques, F.R.B.; Vianna, C.B.; Eid, C.A.; Feitosa-Filho, G.S.; Timerman, S. Ventricular fibrillation during sport activity successfully treated. Arq. Bras. Cardiol. 2009, 93, e26–e29. [Google Scholar] [CrossRef]
- Mills, J.D.; Moore, G.E.; Thompson, P.D. The athlete’s heart. Clin. Sports Med. 1997, 16, 725–737. [Google Scholar] [CrossRef]
- Schneider, K.; Meeteer, W.; Nolan, J.A.; Campbell, H.D. Health care in high school athletics in west virginia. Rural Remote Health 2017, 17, 1–11. [Google Scholar] [CrossRef]
- Lear, A.; Hoang, M.H.; Zyzanski, S.J. Preventing sudden cardiac death: Automated external defibrillators in ohio high schools. J. Athl. Train. 2015, 50, 1054–1058. [Google Scholar] [CrossRef] [PubMed]
- Kramer, E.B.; Dvorak, J.; Shmied, C.; Meyer, T. F-marc: Promoting the prevention and management of sudden cardiac arrest in football. Br. J. Sports Med. 2015, 49, 597–598. [Google Scholar] [CrossRef] [PubMed]
- Marijon, E.; Tafflet, M.; Celermajer, D.S.; Dumas, F.; Perier, M.C.; Mustafic, H.; Toussaint, J.F.; Desnos, M.; Rieu, M.; Benameur, N.; et al. Sports-related sudden death in the general population. Circulation 2011, 124, 672–681. [Google Scholar] [CrossRef] [PubMed]
- Brion, R. Sport-related sudden death and its prevention. Bull. L’academie Natl. Med. 2010, 194, 1237–1247. [Google Scholar]
- Rich, B.S.E. Sudden death screening. Med. Clin. N. Am. 1994, 78, 267–288. [Google Scholar] [CrossRef]
- Kassanoff, I.; Whaley, W.; Walter, W.H.; Burge, D.; Harrison, C.; Hurst, J.W.; Wenger, N.K. Stadium coronary care: A concept in emergency health care delivery. JAMA J. Am. Med. Assoc. 1972, 221, 397–399. [Google Scholar] [CrossRef]
- Kinoshi, T.; Tanaka, S.; Sagisaka, R.; Hara, T.; Shirakawa, T.; Sone, E.; Takahashi, H.; Sakurai, M.; Maki, A. Mobile automated external defibrillator response system during road races. N. Engl. J. Med. 2018, 379. [Google Scholar] [CrossRef]
- Fortington, L.V.; Bekker, S.; Morgan, D.; Finch, C.F. “It doesn’t make sense for us not to have one”-understanding reasons why community sports organizations chose to participate in a funded automated external defibrillator program. Clin. J. Sport Med. 2017. [Google Scholar] [CrossRef] [PubMed]
- Luther, V.; Sikkel, M.B.; Wright, I.; Faulkner, M.; Qureshi, N.; Lefroy, D.C. A collapsed sportsman with a shock advised in sinus rhythm: The importance of automated external defibrillator rhythm strip retrieval prior to defibrillator implantation. Circ. Arrhythm. Electrophysiol. 2016, 9, e003914. [Google Scholar] [CrossRef] [PubMed]
- Kramer, E.B. Automated external defibrillator in sport: Absolutely always available. Br. J. Sports Med. 2013, 47, 1138. [Google Scholar] [CrossRef]
- Toresdahl, B.G.; Harmon, K.G.; Drezner, J.A. High school automated external defibrillator programs as markers of emergency preparedness for sudden cardiac arrest. J. Athl. Train. 2013, 48, 242–247. [Google Scholar] [CrossRef]
- Smith, D.; Hoogenboom, B. The use of cardiopulmonary resuscitation and the automated external defibrillator in the practice of sports physical therapy. Int. J. Sports Phys. Ther. 2011, 6, 267–270. [Google Scholar]
- Drezner, J.A.; Rogers, K.J.; Horneff, J.G. Automated external defibrillator use at ncaa division ii and iii universities. Br. J. Sports Med. 2011, 45, 1174–1178. [Google Scholar] [CrossRef] [PubMed]
- Ngai, K.Y.; Chan, H.Y.; Ng, F. A patient with commotio cordis successfully resuscitated by bystander cardiopulmonary resuscitation and automated external defibrillator. Hong Kong Med. J. 2010, 16, 403–405. [Google Scholar]
- Coris, E.E.; Miller, E.; Sahebzamani, F. Sudden cardiac death in division I collegiate athletics: Analysis of automated external defibrillator utilization in national collegiate athletic association division I athletic programs. Clin. J. Sport Med. 2005, 15, 87–91. [Google Scholar] [CrossRef]
- Hevia, A.C.; Fernández, M.M.; Alacio, J.M.A.P.; Martín, E.H.; Castro, M.G.; Reguero, J.J.R. Ecg as a part of the preparticipation screening programme: An old and still present international dilemma. Br. J. Sports Med. 2011, 45, 776–779. [Google Scholar] [CrossRef] [PubMed]
- Chatard, J.C.; Mujika, I.; Goiriena, J.J.; Carré, F. Screening young athletes for prevention of sudden cardiac death: Practical recommendations for sports physicians. Scand. J. Med. Sci. Sports 2016, 26, 362–374. [Google Scholar] [CrossRef] [PubMed]
- American Heart Association. Highlights of the 2017 American Heart Association Focused Updates on Adult and Pediatric Basic Life Support and Cardiopulmonary Resuscitation Quality. Available online: https://eccguidelines.heart.org/wp-content/uploads/2017/11/2017-Focused-Updates_Highlights.pdf (accessed on 12 December 2018).
- Kleinman, M.E.; Brennan, E.E.; Goldberger, Z.D.; Swor, R.A.; Terry, M.; Bobrow, B.J.; Gazmuri, R.J.; Travers, A.H.; Rea, T. Part 5: Adult basic life support and cardiopulmonary resuscitation quality: 2015 american heart association guidelines update for cardiopulmonary resuscitation and emergency cardiovascular care. Circulation 2015, 132, S414–S435. [Google Scholar] [CrossRef]
- Lear, S.A.; Ignaszewski, A. Cardiac rehabilitation: A comprehensive review. Trials 2001, 2, 221. [Google Scholar] [CrossRef]
- Available online: https://nhcps.com/lesson/bls-for-children-1-8-years-old/ (accessed on 12 December 2018).
- Vitti, A.; Nikolaidis, P.T.; Villiger, E.; Onywera, V.; Knechtle, B. The “New York City Marathon”: Participation and performance trends of 1.2M runners during half-century. Res. Sports Med. 2019. [Google Scholar] [CrossRef]
- Knechtle, B.; Di Gangi, S.; Rüst, C.A.; Rosemann, T.; Nikolaidis, P.T. Men’s participation and performance in the Boston marathon from 1897 to 2017. Int. J. Sports Med. 2018, 39, 1018–1027. [Google Scholar] [CrossRef] [PubMed]
- Fragakis, N.; Pagourelias, E.D.; Koskinas, K.C.; Vassilikos, V. Arrhythmias in athletes: Evidence-based strategies and challenges for diagnosis, management, and sports eligibility. Cardiol. Rev. 2013, 21, 229–238. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Cause | Literal Definition | Reference |
|---|---|---|
| Cardiomyopathies | Defined by structural and functional abnormalities of the ventricular myocardium those are unexplained by flow-limiting coronary artery disease or abnormal loading conditions. | [26] |
| Hypertrophic cardiomyopathy | Defined by the presence of increased left ventricular wall thickness that is not solely explained by abnormal loading conditions. | [27] |
| Coronary artery anomalies | Can be classified as anomalies with obligatory ischemia, without ischemia or with exceptional ischemia. The clinical symptoms may include chest pain, dyspnea, palpitations, syncope, cardiomyopathy, and arrhythmia. | [28] |
| Arrhythmia (the main is ventricular fibrillation) | Electrical malfunction in the heart that causes an irregular heartbeat. | [29] |
| Valvulopathies | Changes in the heart valves, which cause stenosis or insufficiency, and may result in hemodynamic problems. | [30] |
| Myocarditis | Defined as inflammation of the heart muscle that may be identified by clinical or histopathologic criteria and an important cause of dilated cardiomyopathy. Viral infection is an important cause. | [31] |
| Coronary atherosclerotic disease | Develops when the major blood vessels that supply heart with blood, oxygen, and nutrients (coronary arteries) become damaged or diseased. Cholesterol-containing deposits in arteries (plaque, accumulate at the site of injury in a process called atherosclerosis) and inflammation are usually to blame for disease. | [32] |
| Heart attack | Occurs when a blocked artery prevents oxygen-rich blood from reaching a section of the heart. If the blocked artery is not reopened quickly, the part of the heart normally nourished by that artery begins to die. The longer a person goes without treatment, the greater the damage. | [29] |
| Cardiac arrest | Occurs suddenly and often without warning. It is triggered by an electrical malfunction in the heart. With its pumping action disrupted, the heart cannot pump blood to the brain, lungs, and other organs. Seconds later, a person loses consciousness and has no pulse. Death occurs within minutes if the victim does not receive treatment. | [29] |
| Pulmonary embolism | Characterized by occlusion of one or more pulmonary arteries. Physiological disturbance may be minimal, but often cardiac output decreases as the right ventricle attempts to overcome increased afterload. Additionally, ventilation-perfusion mismatches can develop in affected vascular beds, reducing systemic oxygenation. | [33] |
| Stroke | Occurs when the blood supply to part of your brain is interrupted or reduced, depriving brain tissue of oxygen and nutrients. Within minutes, brain cells begin to die. | [34] |
| Hyponatremic encephalopathy | Symptomatic cerebral edema due to a low osmolar state. Hyponatremia is a common electrolyte disturbance occurring in a broad spectrum of patients, from asymptomatic to critically ill. The disease is defined as a decrease in serum sodium concentration to a level below 136 mmol per liter. The brain damage from hyponatremia can be associated with either hyponatremic encephalopathy or improper therapy of symptomatic hyponatremia. | [35,36] |
| Hyperthermia | May be caused by excessive heat production, diminished heat dissipation, or malfunction of the hypothalamic thermostat. | [37] |
| Rhabdomyolysis | Defined as injury of the skeletal muscle, which results in the release of intracellular contents into the circulation. Skeletal muscle comprises 40% of body mass, and a large insult can result in the accumulation of cellular contents in the extracellular space such that elimination mechanisms are overwhelmed. The resulting effects are recognized as a clinical syndrome of muscle injury that is associated with the development of myoglobinuria, electrolyte abnormalities, and often acute kidney injury | [38] |
| Respiratory failure | Condition in which not enough oxygen passes from your lungs into your blood. When respiratory failure causes a low level of oxygen in the blood, it is called hypoxemic respiratory failure. When respiratory failure causes a high level of carbon dioxide in the blood, it is called hypercapnic respiratory failure. | [39] |
| Pulseless electrical activity | Also known as electromechanical dissociation is a clinical condition characterized by unresponsiveness and impalpable pulse in the presence of sufficient electrical discharge. Electrical activity is a pertinent, but not sufficient, condition for contraction. Also defined as organized ECG activity, excluding ventricular tachycardia and fibrillation, without clinical evidence of a palpable pulse or myocardial contractions | [40,41] |
| Coronary artery anomaly | 1:100 |
| Bicuspid aortic valve | 1:100 |
| Hypertrophic cardiomyopathy | 1:500 |
| Wolff-Parkinson-White | 1:750 |
| Short QT syndrome | 1:2000 |
| Arrhythmogenic right ventricular cardiomyopathy | 1:2000 to 1:5000 |
| Brugada syndrome | 1:2000 to 1:5000 |
| Long QT syndrome | 1:2500 |
| Dilated cardiomyopathy | 1:2500 |
| Marfan syndrome | 1:5000 |
| Catecholaminergic polymorphic ventricular tachycardia | 1:10,000 |
| Author | Year | Study Type | Title | Journal | Country | Main Findings and Conclusions |
|---|---|---|---|---|---|---|
| Prech et al. [51] | 2018 | Case report | An amateur marathon runner after sudden cardiac arrest. Whether and when can he return to sport competition? | Polski Merkuriusz Lekarski | Poland | A case of an amateur runner has been presented, competitor in 50 marathons, who underwent a sudden CA. Reports on the possible dangers of overdosing extreme endurance exercises are necessary. |
| Landry et al. [52] | 2017 | Original | Sudden cardiac arrest during participation in competitive sports | The New England Journal of Medicine | Canada | Incidence of sudden CA during participation in competitive sports was 0.76 cases per 100,000 athlete-years within a specific region of Canada, with 43.8% of the athletes surviving until they were discharged from the hospital. Two deaths were attributed to hypertrophic cardiomyopathy. The occurrence of sudden CA due to structural heart disease was uncommon during participation in competitive sports |
| Zorzi et al. [53] | 2016 | Original | Sudden cardiac arrest in Italian sports facilities in 2015: epidemiological implications of the so-called “Balduzzi decree” | Giornale Italiano di Cardiologia (Rome) | Italy | After the sudden cardiac death of elite athletes in 2012, the presence of an AED and professionals trained to perform CPR must be available in Italian sports facilities. In 2015, it was reported 123 cases of sudden CA in Italian sports facilities. The majority victims were males (93%) and >35 years old (88%). The rate of return of spontaneous circulation was 62% when an AED was used before electromyostimulation arrival vs. 9% when no bystander CPR or AED use by lay rescuers was mentioned. |
| Harmon et al. [54] | 2016 | Original | Incidence and etiology of sudden cardiac arrest and death in high school athletes in the United States. | Mayo Clinic Proceedings | USA | The rate of sudden CA and death in male high school athletes was 1:44,832 athletes per year, with almost half due to possible or confirmed cardiomyopathy disease. |
| Solberg et al. [55] | 2016 | Original | Sudden cardiac arrest in sports—need for uniform registration: A position paper from the Sport Cardiology Section of the European Association for cardiovascular prevention and rehabilitation | European Journal of Preventive Cardiology | European position | Rational decisions about cardiac pre-participation screening and cardiac safety at sport facilities requires increased data quality concerning incidence, etiology, and management of sudden CA/sudden death in sports. |
| Cronin et al. [56] | 2013 | Original | Prepared for sudden cardiac arrest? A cross-sectional study of automated external defibrillators in amateur sport | British Journal of Sports Medicine | Ireland | A total of 81.3% of amateur clubs owns an AED. Many clubs engage in regular maintenance and storage of AEDs. However, this study identifies several areas for improvement in facilitating a secure survival chain for players in the event of a sudden CA. |
| Marijon et al. [57] | 2013 | Original | Characteristics and outcomes of sudden cardiac arrest during sports in women | Circulation: Arrhythmia and Electrophysiology | France | Compared with men, the incidence of sudden cardiac death in women was lower. Despite similar circumstances of occurrence, survival at hospital admission (46.5%) was significantly higher than that for men (30.0%). Favorable neurological outcomes were similar (80%). Cause of death seemed less likely to be associated with structural heart disease in women compared with men (58.3% vs. 95.8%). |
| Enright et al. [58] | 2012 | Original | Primary cardiac arrest following sport or exertion in children presenting to an emergency department: chest compressions and early defibrillation can save lives, but is intravenous epinephrine always appropriate? | Pediatric Emergency Care | Australia | The importance of early CPR and defibrillation in collapsed young athletes (with cardiac disorders that suffer CA) is fundamental. These interventions could result in full long-term neurological recovery. |
| Kramer et al. [59] | 2010 | Review | Review of the management of sudden cardiac arrest on the football field | British Journal of Sports Medicine | South Africa | Trained medical professionals must be allowed to respond, ideally with a defibrillator, to a player who suddenly and unexpectedly collapses on the field. Immediate defibrillation of a pulseless ventricular tachycardia or ventricular fibrillation has a successful cardioversion rate exceeding 90%. Medical professionals should be well trained and rehearsed in the recognition of sudden CA. Prompt initiation of CPR together with early defibrillation, will result in many athletes’ lives being saved. |
| Cappato et al. [60] | 2010 | Original | J wave, QRS slurring, and ST elevation in athletes with cardiac arrest in the absence of heart disease: marker of risk or innocent bystander? | Circulation: Arrhythmia and Electrophysiology | Italy | J wave and/or QRS slurring was found more frequently among athletes with CA/sudden death than in control athletes. Nevertheless, the presence of this ECG pattern appears not to confer a higher risk for recurrent malignant ventricular arrhythmias. |
| Furlanello et al. [61] | 1998 | Original | Cardiac arrest and sudden death in competitive athletes with ARVD | Pacing and Clinical Electrophysiology | Italy | ARVD is a predisposing factor for sport-related CA. Prevalence of ARVD among athletes with CA is high, confirming the observation that ARVD is one of the major causes of sudden death. All CA were athletic activity related, indicating the potentiality of exercise as a cause of electrical destabilization in subjects with ARVD. |
| Maron et al. [62] | 1995 | Original | Blunt impact to the chest leading to sudden death from cardiac arrest during sports activities | The New England Journal of Medicine | USA | Sudden death from CA in a young person may occur during sports play after a blunt blow to the chest in the absence of structural cardiovascular disease or traumatic injury (commotio cordis). The authors identified 25 cases (people of 3–19 years) from the registries. Incidents took place during organized competitive sports in 16 cases and in recreational settings in 9. Twelve victims collapsed virtually instantaneously on impact, whereas 13 remained conscious and physically active for a brief time before CA. CPR was administered within about 3 min to 19 victims, but normal cardiac rhythm could be restored in only 2. The authors concluded that most sudden deaths related to impact to the chest are due to ventricular dysrhythmia induced by an abrupt, blunt precordial blow, presumably delivered at an electrically vulnerable phase of ventricular excitability. |
| Peters and Reil [63] | 1995 | Original | Risk factors of cardiac arrest in arrhythmogenic right ventricular dysplasia | European Heart Journal | Germany | Arrhythmogenic right ventricular dysplasia is an important cause of ventricular arrhythmia with a potential risk of sudden cardiac death. People with structural alterations and a low level of right ventricular function is at a high risk of CA and strenuous exercise and sport remain most important risk factors. |
| Dietlen et al. [64] | 1953 | Not available | Acute cardiac arrest in sport exercise and work | Münchner Medizinische Wochenschrift | Germany | Not available |
| Author | Year | Study Type | Title | Journal | Country | Main Findings and Conclusions |
|---|---|---|---|---|---|---|
| Karam et al. [65] | 2017 | Original | Major regional differences in Automated External Defibrillator placement and Basic Life Support training in France: Further needs for coordinated implementation | Resuscitation | France | There is great heterogeneity in public AEDs programs. Population education on BLS offers an important benefit, regardless of the density of AEDs implanted, which should be taken into account when planning public health policies to improve the survival of sudden CA outside the hospital setting. |
| Gonzalez et al. [66] | 2009 | Case report | Ventricular fibrillation during sport activity successfully treated | Brazilian Archives of Cardiology | Brazil | Public access programs to the AED may increase survival from ventricular fibrillation in the out-of-hospital setting. It is necessary to stimulate the training of lay people for the use of AED and BLS and to disseminate these behaviors in places with great circulation of people and those with high risk of sudden death (sports centers and arenas). |
| Mills et al. [67] | 1997 | Review | The athlete’s heart | Clinics in Sports Medicine | USA | Coaches and other sports professionals should learn BLS measures such as CPR. Such efforts may prevent heart deaths related to physical exercise. |
| Author | Year | Study Type | Title | Journal | Country | Main Findings and Conclusions |
|---|---|---|---|---|---|---|
| Schneider et al. [68] | 2017 | Original | Health care in high school athletics in West Virginia | Rural Remote Health | USA | In order to avoid a potentially fatal emergency or possibly sudden cardiac death, emergency planning should be an essential part of high school sports programs. The requirement for first aid, CPR certification, and an emergency action plan are steps that can improve the health care of athletes from rural areas and non-rural areas. |
| Lear et al. [69] | 2015 | Original | Preventing sudden cardiac death: automated external defibrillators in Ohio high schools | Journal of Athletic Training | USA | Emergency action plans in secondary schools should emphasize the management of sudden CA in sports facilities and the placement of AEDs. Over a period of 11 years, 25 episodes of AED use were recorded in 22 secondary schools, of which 20 occurred in or near sports facilities. |
| Kramer et al. [70] | 2015 | Review | F-MARC: promoting the prevention and management of sudden cardiac arrest in football | British Journal of Sports Medicine | Switzerland | To prevent and administer sudden CA in soccer, the FIFA Medical and Research Center is establishing a program of research, education, and practical standardization. This strategy detected players at medical risk during mandatory pre-competitive assessments. In addition, FIFA disseminated accepted guidelines for the interpretation of athletes’ electrocardiogram, developed field-specific protocols for recognition, response, CPR, and removal of a player who underwent sudden CA. |
| Marijon et al. [71] | 2011 | Original | Sports-related sudden death in the general population | Circulation | France | Sudden sport-related death in the general population is more common than previously thought. Most cases are witnessed, but CPR by “lay” viewers was initiated in only one third of cases. Immediate interventions were significantly associated with improved survival and prognosis. |
| Brion [72] | 2010 | Review | Sport-related sudden death and its prevention | Bulletin de L’AcadémieNationale de Médecine | France | The immediate causes of sudden sports-related death are age dependent. Prevention begins with screening. Before 35 years, the most frequent causes are hypertrophic cardiomyopathy and arithmogenic right ventricular cardiomyopathy. People with cardiovascular diseases at risk of sudden death should adapt their sports activities. Knowledge of first aid procedures by those who supervise sports activities may improve prognosis. |
| Rich [73] | 1994 | Review | Sudden death screening | Medical Clinics of North America | USA | Emergency plans need to be established by physicians and sports coaches. The recognition of cardiac symptoms associated with sudden CA is a key point. Appropriate education, which includes information and training in first aid, BLS and CPR, should be encouraged for those working with athletes. The emergency plan should include on-site treatment, the way to contact Emergency medical services, and transportation to a qualified health care facility. |
| Kassanoff et al. [74] | 1972 | Original | Stadium coronary care. A concept in emergency health care delivery | JAMA | USA | BLS and emergency stations were established at sports stadiums as part of a research program to elucidate the precipitating mechanisms and/or events of sudden CA and thereby suggest appropriate therapeutic intervention through a well-equipped and prepared emergency team. During the study period there were 20 episodes of myocardial infarction. It was verified the occurrence of 1 acute event in most sports events with participation of 30,000 to 40,000 people. |
| Author | Year | Study Type | Title | Journal | Country | Main Findings and Conclusions |
|---|---|---|---|---|---|---|
| Kinoshi et al. [75] | 2018 | Correspondence | Mobile automated external defibrillator response system during road races | The New England Journal of Medicine | Japan | Between 2005 and 2017, of 1,965,265 runners in 251 road races (of 10.0 to 42.2 km), 30 CA were attended. Shocks were delivered to 23 runners who had ventricular fibrillation, and another 5 runners (4 with pulseless electrical activity and 1 with ventricular fibrillation) recovered with basic CPR only. The median interval between collapse and the return of spontaneous circulation was 5.5 min. All these runners had return of spontaneous circulation in the field and had a favorable neurologic outcome. |
| Fortington et al. [76] | 2017 | Original | “It doesn’t make sense for us not to have one”—understanding reasons why community sports organizations chose to participate in a funded automated external defibrillator program | Clinical Journal of Sport Medicine | Australia | Implementation of AEDs in community sports settings is an important component of emergency medical planning. Two overarching themes emerged: Awareness of the program and decision to apply. |
| Luther et al. [77] | 2016 | Original | A collapsed sportsman with a shock advised in sinus rhythm: the importance of automated external defibrillator rhythm strip retrieval prior to defibrillator implantation. | Circulation: Arrhythmia and Electrophysiology | England | AEDs rely on rhythm detection algorithms with high specificity for recognizing ventricular arrhythmia when used appropriately. AED diagnostics can be difficult to retrieve once the patient has arrived in hospital, with patient management decisions often made in their absence. |
| Kramer [78] | 2013 | Editorial | Automated external defibrillator in sport: absolutely always available | British Journal of Sports Medicine | South Africa | Sudden CA remains the leading cause of death in sports. Whenever its prevention has failed, for whatever reason, its immediate medical management becomes paramount if the life under acute threat is to be saved. In many circumstances, this can only be effectively and efficiently achieved by the presence of a fully functional AED which is activated while CPR is being undertaken. It is no longer a question of whether an AED is necessary in any mass gathering sport environment but how many are necessary and where they should be located |
| Toresdahl et al. [79] | 2013 | Original | High school automated external defibrillator programs as markers of emergency preparedness for sudden cardiac arrest | Journal of Athletic Training | USA | A total of 2784 schools (82.6%) reported having 1 or more AEDs on campus, with an average of 2.8 AEDs per school; 587 schools (17.4%) had no AEDs. Schools with an enrollment of more than 500 students were more likely to have an AED. Suburban schools were more likely to have an AED than were rural, urban, or inner-city schools. Schools with 1 or more AEDs were more likely to ensure access to early defibrillation, establish an emergency action plan for sudden CA, review the emergency action plan at least annually, consult EMS to develop the emergency action plan, and establish a communication system to activate emergency responders. High schools with AED programs were more likely to establish a comprehensive emergency response plan for sudden CA. |
| Smith and Hoogenboom [80] | 2011 | Review | The use of cardiopulmonary resuscitation and the automated external defibrillator in the practice of sports physical therapy | International Journal of Sports Physical Therapy | USA | During the initial assessment of the injured athlete, the sports physical therapist must first be concerned with life-threatening emergencies such as absence of breathing and pulse. The sports physical therapist must also be aware of the possibility of sudden CA that could occur in others, including coaches, officials, and fans. Therefore, skills and ongoing certification in CPR techniques and the use of an AED are a basic necessity. These skills are required as part of the specialty practice of sports physical therapist and are mandatory for being qualified. |
| Drezner et al. [81] | 2011 | Original | Automated external defibrillator use at NCAA Division II and III universities | British Journal of Sports Medicine | USA | 81% of institutions had at least one AED in the university athletic setting. Athletic training rooms (75%) were the most likely location to place an AED. Twelve cases of AED use for sudden CA were reported with 67% occurring in older non-students, 16% in intercollegiate athletes, and 16% in students (non-intercollegiate athletes). The AED deployed a shock in eight cases. Eight of 12 (66%) victims were immediately resuscitated, but only 4 survived to hospital discharge (overall survival 33%). None of the intercollegiate athletes or students survived. Although no benefit was demonstrated in a small number of intercollegiate athletes, AEDs were successfully used in older individuals on campus with CA. |
| Ngai et al. [82] | 2010 | Case report | A patient with commotio cordis successfully resuscitated by bystander cardiopulmonary resuscitation and automated external defibrillator | Hong Kong Medical Journal | Hong Kong | Sudden deaths of young people during competitive sports are usually due to congenital heart diseases. Ventricular fibrillation, however, may also occur in individuals with no underlying cardiac disease who have sustained a low-impact chest wall blow (commotio cordis). Successful resuscitation can be achieved by prompt CPR and early defibrillation. Accessible CPR-trained personnel and AEDs should be present at all organized sporting events. |
| Coris et al. [83] | 2005 | Original | Sudden cardiac death in division I collegiate athletics: analysis of automated external defibrillator utilization in National Collegiate Athletic Association division I athletic programs | Clinical Journal of Sport Medicine | USA | Sixteen departments that previously reported having had a sudden cardiac death event at their institution responded to this follow-up telephone survey. 20% of AED uses were attributed to student athletes, with 33% of utilizations for athletic department staff and 47% for fans. Defibrillation was actually administered in 53% of AED unit applications. Time to shock was an average of 3.4 min, with average EMS response time of 8.2 min for those events without EMS on site. Reported survival to hospital discharge in this university athletic department setting for sudden cardiac death was 0% for students, 75% for staff, 57% for fans, and 61% overall. Athletic department AED programs were extremely successfully at increasing survival of sudden cardiac death far above national prehospital standards, mainly in the nonathletic population. |
| Short Title | Link | |
|---|---|---|
| England | Plan to teach all children first aid | https://www.bbc.com/news/education-44883708 |
| Australia | First aid in schools program | https://www.stjohnvic.com.au/first-aid-in-schools.asp |
| Ireland | First aid for schools | https://pulse8.ie/first-aid-for-schools/ |
| USA | Teaching CPR in middle schools and high schools | https://aha.channing-bete.com/school.html |
| France | Teach first aid to children younger than 6 years | https://bmjopen.bmj.com/content/bmjopen/4/9/e005848.full.pdf |
| Scotland | Call for every school to teach pupils CPR and first aid | https://www.sundaypost.com/news/scottish-news/call-every-school-teach-pupils-cpr-first-aid/ |
| Israel | Teach first aid to Bedouin high school students | https://msih.bgu.ac.il/volunteer-opportunities-in-medical-school/ |
| Canada | School programs | http://www.calgary.ca/CSPS/Recreation/Pages/Teacher-resources/First-Aid-grades-7-to-12.aspx |
| Brazil | Social project: mass training | http://www.socesp2015.com.br/treinamentoemmassa/ |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vancini, R.L.; Nikolaidis, P.T.; de Lira, C.A.B.; Vancini-Campanharo, C.R.; Viana, R.B.; Andrade, M.d.S.; Rosemann, T.; Knechtle, B. Prevention of Sudden Death Related to Sport: The Science of Basic Life Support—From Theory to Practice. J. Clin. Med. 2019, 8, 556. https://doi.org/10.3390/jcm8040556
Vancini RL, Nikolaidis PT, de Lira CAB, Vancini-Campanharo CR, Viana RB, Andrade MdS, Rosemann T, Knechtle B. Prevention of Sudden Death Related to Sport: The Science of Basic Life Support—From Theory to Practice. Journal of Clinical Medicine. 2019; 8(4):556. https://doi.org/10.3390/jcm8040556
Chicago/Turabian StyleVancini, Rodrigo Luiz, Pantelis Theodoros Nikolaidis, Claudio Andre Barbosa de Lira, Cássia Regina Vancini-Campanharo, Ricardo Borges Viana, Marilia dos Santos Andrade, Thomas Rosemann, and Beat Knechtle. 2019. "Prevention of Sudden Death Related to Sport: The Science of Basic Life Support—From Theory to Practice" Journal of Clinical Medicine 8, no. 4: 556. https://doi.org/10.3390/jcm8040556
APA StyleVancini, R. L., Nikolaidis, P. T., de Lira, C. A. B., Vancini-Campanharo, C. R., Viana, R. B., Andrade, M. d. S., Rosemann, T., & Knechtle, B. (2019). Prevention of Sudden Death Related to Sport: The Science of Basic Life Support—From Theory to Practice. Journal of Clinical Medicine, 8(4), 556. https://doi.org/10.3390/jcm8040556