EGFR and KRAS Mutations in the Non-Tumoral Lung. Prognosis in Patients with Adenocarcinoma

 , , ,
, , , 
Abstract
1. Introduction
2. Experimental Section
2.1. Patients
2.2. Data
2.3. Tumor DNA Extraction and Sequencing
2.4. DNA Extraction and Allele-Specific PCR in the NTL Tissue
2.5. Digital PCR
2.6. Definitions
2.7. Statistical Analysis
3. Results
3.1. Driver Mutations in the Tumor
3.2. Mutations in the NTL
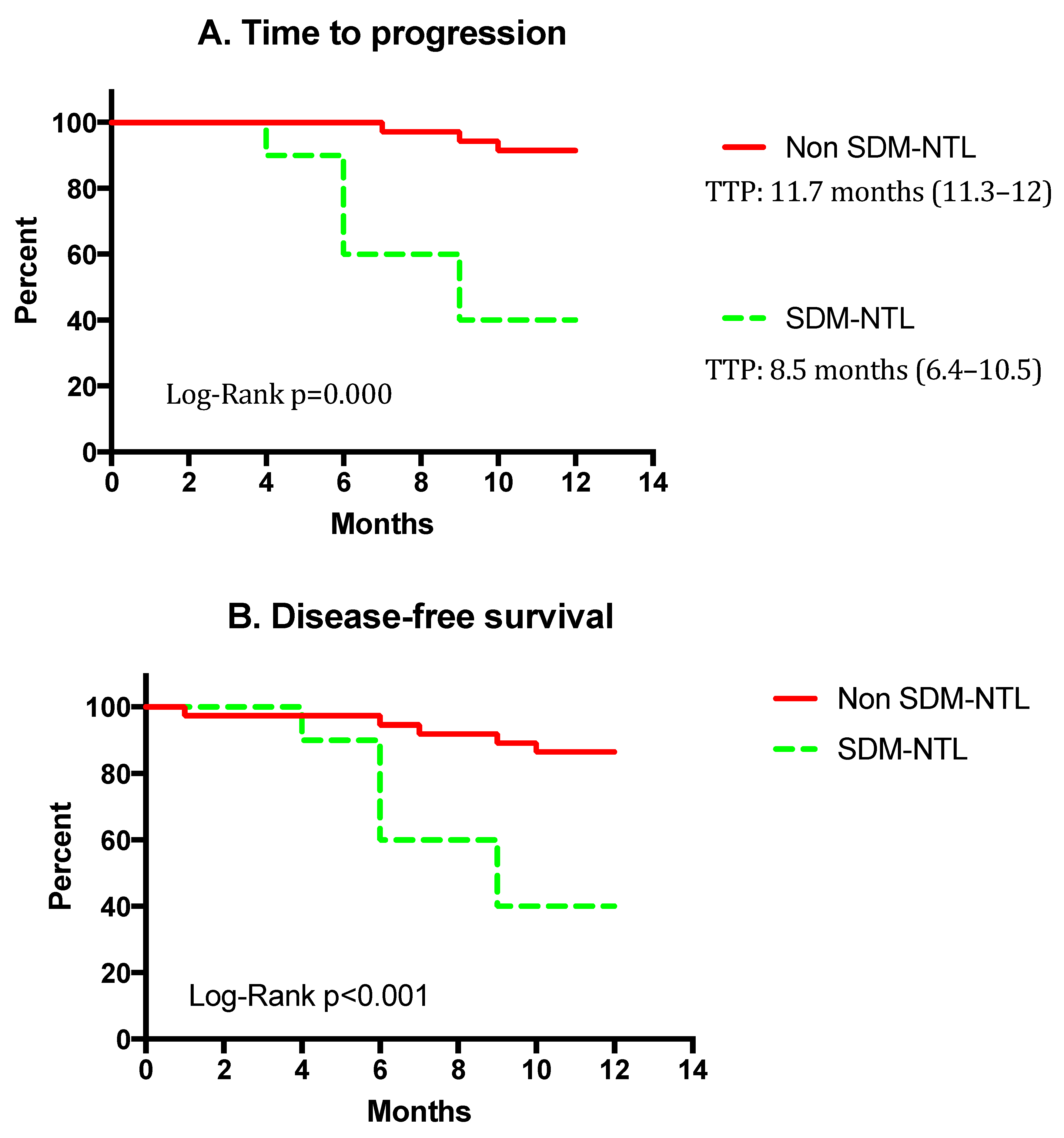
3.3. Recurrence and Survival
4. Discussion
4.1. Alternative Study Designs
4.2. Potential Limitations of the Study
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics. CA Cancer J. Clin. 2016, 66, 7–30. [Google Scholar] [CrossRef]
- American Cancer Society. Cancer Facts & Figures 2016; American Cancer Society Inc.: Atlanta, GA, USA, 2016; pp. 1–9. [Google Scholar]
- Travis, W.D.; Brambilla, E.; Müller-Hermelink, H.K.; Harris, C. World Health Organization Classification of Tumours; Tumours of Lung, Pleura, Thymus and Heart; World Health Organization: Geneva, Switzerland, 2004; pp. 9–122. [Google Scholar]
- Sugimura, H.; Nichols, F.C.; Yang, P.; Allen, M.S.; Cassivi, S.D.; Deschamps, C.; Williams, B.A.; Pairolero, P.C. Survival after recurrent nonsmall-cell lung cancer after complete pulmonary resection. Ann. Thorac. Surg. 2007, 83, 409–417. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, T.; Okumura, N.; Ohata, K.; Igai, H.; Matsuoka, T.; Kameyama, K. Postrecurrence survival in patients with stage I non-small cell lung cancer. Eur. J. Cardiothorac. Surg. 2008, 34, 499–504. [Google Scholar] [CrossRef][Green Version]
- Martini, N.; Bains, M.S.; Burt, M.E.; Zakowski, M.F.; McCormack, P.; Rusch, V.W.; Ginsberg, R.J. Incidence of local recurrence and second primary tumors in resected stage I lung cancer. J. Thorac. Cardiovasc. Surg. 1995, 109, 120–129. [Google Scholar] [CrossRef]
- Nesbitt, J.C.; Putnam, J.B.; Walsh, G.L.; Roth, J.A.; Mountain, C.F. Survival in early-stage non-small cell lung cancer. Ann. Thorac. Surg. 1995, 60, 466–472. [Google Scholar] [CrossRef]
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [PubMed]
- Gibelin, C.; Couraud, S. Somatic alterations in lung cancer: Do environmental factors matter? Lung Cancer 2016, 100, 45–52. [Google Scholar] [CrossRef]
- Goldstraw, P.; Chansky, K.; Crowley, J.; Rami-Porta, R.; Asamura, H.; Eberhardt, W.E.; Nicholson, A.G.; Groome, P.; Mitchell, A.; Bolejack, V.; et al. The IASLC lung cancer staging project: Proposals for revision of the TNM stage groupings in the forthcoming (eighth) edition of the TNM Classification for lung cancer. J. Thorac. Oncol. 2016, 11, 39–51. [Google Scholar] [CrossRef]
- Stratton, M.R.; Campbell, P.J.; Futreal, P.A.A. The cancer genome. Nature 2009, 458, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Siravegna, G.; Mussolin, B.; Buscarino, M.; Corti, G.; Cassingena, A.; Crisafulli, G.; Ponzetti, A.; Cremolini, C.; Amatu, A.; Lauricella, C.; et al. Clonal evolution and resistance to EGFR blockade in the blood of colorectal cancer patients. Nat. Med. 2015, 21, 795–801. [Google Scholar] [CrossRef]
- Chalela, R.; Curull, V.; Enríquez, C.; Pijuan, L.; Bellosillo, B.; Gea, J. Lung adenocarcinoma: From molecular basis to genome-guided therapy and immunotherapy. J. Thorac. Dis. 2017, 9, 2142–2158. [Google Scholar] [CrossRef] [PubMed]
- Tamborero, D.; Gonzalez-Perez, A.; Perez-Llamas, C.; Deu-Pons, J.; Kandoth, C.; Reimand, J.; Lawrence, M.S.; Getz, G.; Bader, G.D.; Ding, L.; et al. Comprehensive identification of mutational cancer driver genes across 12 tumor types. Sci. Rep. 2013, 3, 2650. [Google Scholar] [CrossRef]
- Collisson, E.A.; Campbell, J.D.; Brooks, A.N.; Berger, A.H.; Lee, W.; Chmielecki, J.; Beer, D.G.; Cope, L.; Creighton, C.J.; Danilova, L.; et al. Comprehensive molecular profiling of lung adenocarcinoma. Nature 2014, 511, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, F.R.; Scagliotti, G.V.; Mulshine, J.L.; Kwon, R.; Curran, W.J.; Wu, Y.-L.; Paz-Ares, L. Lung cancer: Current therapies and new targeted treatments. Lancet (Lond. Engl.) 2017, 389, 299–311. [Google Scholar] [CrossRef]
- Travis, W.D.; Brambilla, E.; Noguchi, M.; Nicholson, A.G.; Geisinger, K.R.; Yatabe, Y.; Beer, D.G.; Powell, C.A.; Riely, G.J.; Van Schil, P.E.; et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J. Thorac. Oncol. 2011, 6, 244–285. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, D.R.; Ost, D.E. How and when to use genetic markers for nonsmall cell lung cancer. Curr. Opin. Pulm. Med. [Internet] 2013, 19, 331–339. [Google Scholar] [CrossRef]
- Nishii, T.; Yokose, T.; Miyagi, Y.; Daigo, Y.; Isaka, T.; Furumoto, H.; Ito, H.; Murakami, S.; Kondo, T.; Saito, H.; et al. Prognostic value of EGFR mutations in surgically resected pathological stage I lung adenocarcinoma. Asia Pac. J. Clin. Oncol. 2016, 13, e204–e211. [Google Scholar] [CrossRef] [PubMed]
- Kadota, K.; Sima, C.S.; Arcila, M.E.; Hedvat, C.; Kris, M.G.; Jones, D.R.; Adusumilli, P.S.; Travis, W.D. KRAS Mutation Is a Significant Prognostic Factor in Early-stage Lung Adenocarcinoma. Am. J. Surg. Pathol. 2016, 40, 1579–1590. [Google Scholar] [CrossRef]
- Camidge, D.R.; Kono, S.A.; Flacco, A.; Tan, A.-C.; Doebele, R.C.; Zhou, Q.; Crino, L.; Franklin, W.A.; Varella-Garcia, M. Optimizing the Detection of Lung Cancer Patients Harboring Anaplastic Lymphoma Kinase (ALK) Gene Rearrangements Potentially Suitable for ALK Inhibitor Treatment. Clin. Cancer Res. 2010, 16, 5581–5590. [Google Scholar] [CrossRef]
- Kapp, J.R.; Diss, T.; Spicer, J.; Gandy, M.; Schrijver, I.; Jennings, L.J.; Li, M.M.; Tsongalis, G.J.; de Castro, D.G.; Bridge, J.A.; et al. Variation in pre-PCR processing of FFPE samples leads to discrepancies in BRAF and EGFR mutation detection: A diagnostic RING trial. J. Clin. Pathol. 2015, 68, 111–118. [Google Scholar] [CrossRef]
- Kokkat, T.J.; Patel, M.S.; McGarvey, D.; LiVolsi, V.A.; Baloch, Z.W. Archived formalin-fixed paraffin-embedded (FFPE) blocks: A valuable underexploited resource for extraction of DNA, RNA, and protein. Biopreserv. Biobank. 2013, 11, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Cavallo, F.; De Giovanni, C.; Nanni, P.; Forni, G.; Lollini, P.L. 2011: The immune hallmarks of cancer. Cancer Immunol. Immunother. 2011, 60, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Mateu-Jimenez, M.; Fermoselle, C.; Rojo, F.; Mateu, J.; Peña, R.; Urtreger, A.J.; Diament, M.J.; Joffé, E.D.; Pijuan, L.; Herreros, A.G.; et al. Pharmacological Approaches in an Experimental Model of Non-Small Cell Lung Cancer: Effects on Tumor Biology. Curr. Pharm. Des. 2016, 22, 5300–5310. [Google Scholar] [CrossRef][Green Version]
- Soria, J.-C.; Mok, T.S.; Cappuzzo, F.; Jänne, P.A. EGFR-mutated oncogene-addicted non-small cell lung cancer: Current trends and future prospects. Cancer Treat. Rev. 2012, 38, 416–430. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.; Lee, T.; Lee, S.; Choi, Y.; Han, J. Clinicopathologic characteristics of EGFR, KRAS, and ALK alterations in 6,595 lung cancers. Oncotarget 2016, 7, 23874–23884. [Google Scholar] [CrossRef]
- Sánchez-Font, A.; Chalela, R.; Martín-Ontiyuelo, C.; Albero-González, R.; Dalmases, A.; Longarón, R.; Alonso-Espinaco, V.; Curull, V.; Bellosillo, B.; Pijuan, L.; et al. Molecular analysis of peripheral lung adenocarcinoma in brush cytology obtained by EBUS plus fluoroscopy-guided bronchoscopy. Cancer Cytopathol. 2018, 126, 860–871. [Google Scholar] [CrossRef] [PubMed]
- Wilson, D.O.; Weissfeld, J.L.; Balkan, A.; Schragin, J.G.; Fuhrman, C.R.; Fisher, S.N.; Wilson, J.; Leader, J.K.; Siegfried, J.M.; Shapiro, S.D.; et al. Association of radiographic emphysema and airflow obstruction with lung cancer. Am. J. Respir. Crit. Care Med. 2008, 178, 738–744. [Google Scholar] [CrossRef] [PubMed]
- Anglesio, M.S.; Papadopoulos, N.; Ayhan, A.; Nazeran, T.M.; Noë, M.; Horlings, H.M.; Lum, A.; Jones, S.; Senz, J.; Seckin, T.; et al. Cancer-Associated Mutations in Endometriosis without Cancer. N. Engl. J. Med. 2017, 376, 1835–1848. [Google Scholar] [CrossRef]
- Nikolaev, S.I.; Vetiska, S.; Bonilla, X.; Boudreau, E.; Jauhiainen, S.; Rezai Jahromi, B.; Khyzha, N.; DiStefano, P.V.; Suutarinen, S.; Kiehl, T.R.; et al. Somatic Activating KRAS Mutations in Arteriovenous Malformations of the Brain. N. Engl. J. Med. 2018, 378, 250–261. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| SM n = 10 | Non-SM n = 37 | p Value | |
|---|---|---|---|
| Age, mean (SD), yrs. | 62.9 (8.7) | 66.9 (9.9) | 0.25 |
| Smoking status, current or former, n (%) | 6 (60) | 24 (64.9) | 0.77 |
| Smoking index, mean (SD), pack-year | 62.1 (27) | 41.2 (20) | 0.04 |
| Sex, n (%) | |||
| Male | 5 (50) | 21 (56.8) | 0.70 |
| Female | 5 (50) | 16 (43.2) | |
| Comorbidities, n (%) | |||
| Diabetes mellitus | 1 (10) | 4 (10.8) | 0.94 |
| Chronic kidney disease | 1 (10) | 0 (0) | 0.06 |
| Cardiovascular disease | 2 (20) | 5 (13.5) | 0.60 |
| Dyslipidemia | 2 (20) | 18 (48.6) | 0.10 |
| Hypertension | 4 (40) | 21 (56.8) | 0.34 |
| COPD | 3 (30) | 8 (21.6) | 0.57 |
| Asthma | 1 (10) | 2 (5.4) | 0.59 |
| Previous cancer | 2 (20) | 10 (27) | 0.65 |
| Lung function tests, mean (SD) | |||
| FEV1, % ref. | 78.3 (19.1) | 79.1 (20) | 0.92 |
| FVC, % ref. | 85.2 (17.9) | 83 (17.4) | 0.75 |
| TLC, % ref. | 98.2 (13.6) | 96.9 (14.7) | 0.82 |
| RV/TLC, % | 48.5 (9.3) | 47.4 (12.4) | 0.77 |
| DLCO, % ref. | 66.7 (15.1) | 82.9 (19.5) | 0.04 |
| Karnofsky Performance Scale, mean (SD) | 88 (6.3) | 88.6 (3.4) | 0.66 |
| Pre-operative tumor characteristics | |||
| SUV by PET, mean (SD), cm | 9.0 (5.7) | 4.4 (4.7) | 0.01 |
| T (tumor size), mean (SD), cm | 3.3 (16) | 2.6 (17) | 0.75 |
| N (nodal infiltration), n (%) | 1 (10) | 1 (2.7) | 0.31 |
| M (metastasis), n (%) | 0 (0) | 0 (0) | |
| Post-operative Stage Groups, n (%) | 0.43 | ||
| I | 6 (60) | 29 (78.4) | 0.21 |
| II | 3 (30) | 5 (13.5) | 0.34 |
| III | 1 (10) | 3 (8.1) | 1.00 |
| IV | 0 (0) | 0 (0) | -- |
| Post-operative Treatment, n (%) | |||
| Chemoradiotherapy | 4 (40) | 10 (27) | 0.42 |
| Radiotherapy | 4 (40) | 7 (18.9) | 0.16 |
| Genomic guided treatment or immunotherapy | 4 (40) | 1 (2.7) | 0.001 |
| EGFR Mutations (24 Patients *; Total Mutations = 28) | ||||
|---|---|---|---|---|
| Site | Alteration | Amino Acid Variation | Patients, n | Group (n+) |
| Exon 19 | Deletion | E746-A750 | 9 | SM (3) |
| Exon 21 | Substitution | L858R | 9 | SM (1) |
| Exon 20 | Substitution | T790M | 4 | SM (3) |
| Exon 19 | Deletion | L747-P752 | 3 | SM (1) |
| Exon 19 | Deletion | L747-P753 | 2 | Non-SM |
| Exon 18 | Substitution | G719A | 1 | Non-SM |
| KRAS mutations (24 patients *; total mutations = 24) | ||||
| Site | Alteration | Amino acid variation | Patients, n | Group |
| Codon 12 | Substitution | Gly12Cys | 12 | SM (3) |
| Codon 12 | Substitution | Gly12Val | 4 | SM (1) |
| Codon 12 | Substitution | Gly12Asp | 4 | Non-SM |
| Codon 13 | Substitution | Gly13Cys | 2 | SM (1) |
| Codon 12 | Substitution | Gly12Ala | 1 | Non-SM |
| Codon 12 | Substitution | Gly12Arg | 1 | Non-SM |
| SM | Non-SM | p Value | |
|---|---|---|---|
| n = 10 | n = 37 | ||
| Recurrence, n (%) * | 6 (60) | 3 (8.1) | |
| Pattern of recurrence Local | 0 (0) | 1 (2.7) | p = 0.59 |
| Distance | 6 (60) | 2 (5.4) | p < 0.001 |
| Organ site of metastases | |||
| Multiple organs affected | 3 (30) | 0 (0) | p = 0.001 |
| Brain | 5 (50) | 0 (0) | p < 0.001 |
| Hepatic | 1 (10) | 0 (0) | p = 0.55 |
| Suprarenal | 0 (0) | 1 (2.7) | p = 0.59 |
| Contralateral lung | 1 (10) | 0 (0) | p = 0.55 |
| Bone | 1 (10) | 0 (0) | p = 0.55 |
| Lymph node | 2 (10) | 1 (2.7) | p = 0.47 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chalela, R.; Bellosillo, B.; Curull, V.; Longarón, R.; Pascual-Guardia, S.; Badenes-Bonet, D.; Arriola, E.; Sánchez-Font, A.; Pijuan, L.; Gea, J. EGFR and KRAS Mutations in the Non-Tumoral Lung. Prognosis in Patients with Adenocarcinoma. J. Clin. Med. 2019, 8, 529. https://doi.org/10.3390/jcm8040529
Chalela R, Bellosillo B, Curull V, Longarón R, Pascual-Guardia S, Badenes-Bonet D, Arriola E, Sánchez-Font A, Pijuan L, Gea J. EGFR and KRAS Mutations in the Non-Tumoral Lung. Prognosis in Patients with Adenocarcinoma. Journal of Clinical Medicine. 2019; 8(4):529. https://doi.org/10.3390/jcm8040529
Chicago/Turabian StyleChalela, Roberto, Beatriz Bellosillo, Víctor Curull, Raquel Longarón, Sergi Pascual-Guardia, Diana Badenes-Bonet, Edurne Arriola, Albert Sánchez-Font, Lara Pijuan, and Joaquim Gea. 2019. "EGFR and KRAS Mutations in the Non-Tumoral Lung. Prognosis in Patients with Adenocarcinoma" Journal of Clinical Medicine 8, no. 4: 529. https://doi.org/10.3390/jcm8040529
APA StyleChalela, R., Bellosillo, B., Curull, V., Longarón, R., Pascual-Guardia, S., Badenes-Bonet, D., Arriola, E., Sánchez-Font, A., Pijuan, L., & Gea, J. (2019). EGFR and KRAS Mutations in the Non-Tumoral Lung. Prognosis in Patients with Adenocarcinoma. Journal of Clinical Medicine, 8(4), 529. https://doi.org/10.3390/jcm8040529