Independent Effects of Hypertension and Obesity on Left Ventricular Mass and Geometry: Evidence from the Cardiovision 2030 Study

 ,
,  , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Physical Examination
2.3. Echocardiography
2.4. Covariates
2.5. Statistical Analyses
3. Results
3.1. Study Population
3.2. BMI and Systolic Blood Pressure Are Strong Predictors of Left Ventricular Mass Index
3.3. ECG Parameters According to BMI and Hypertension
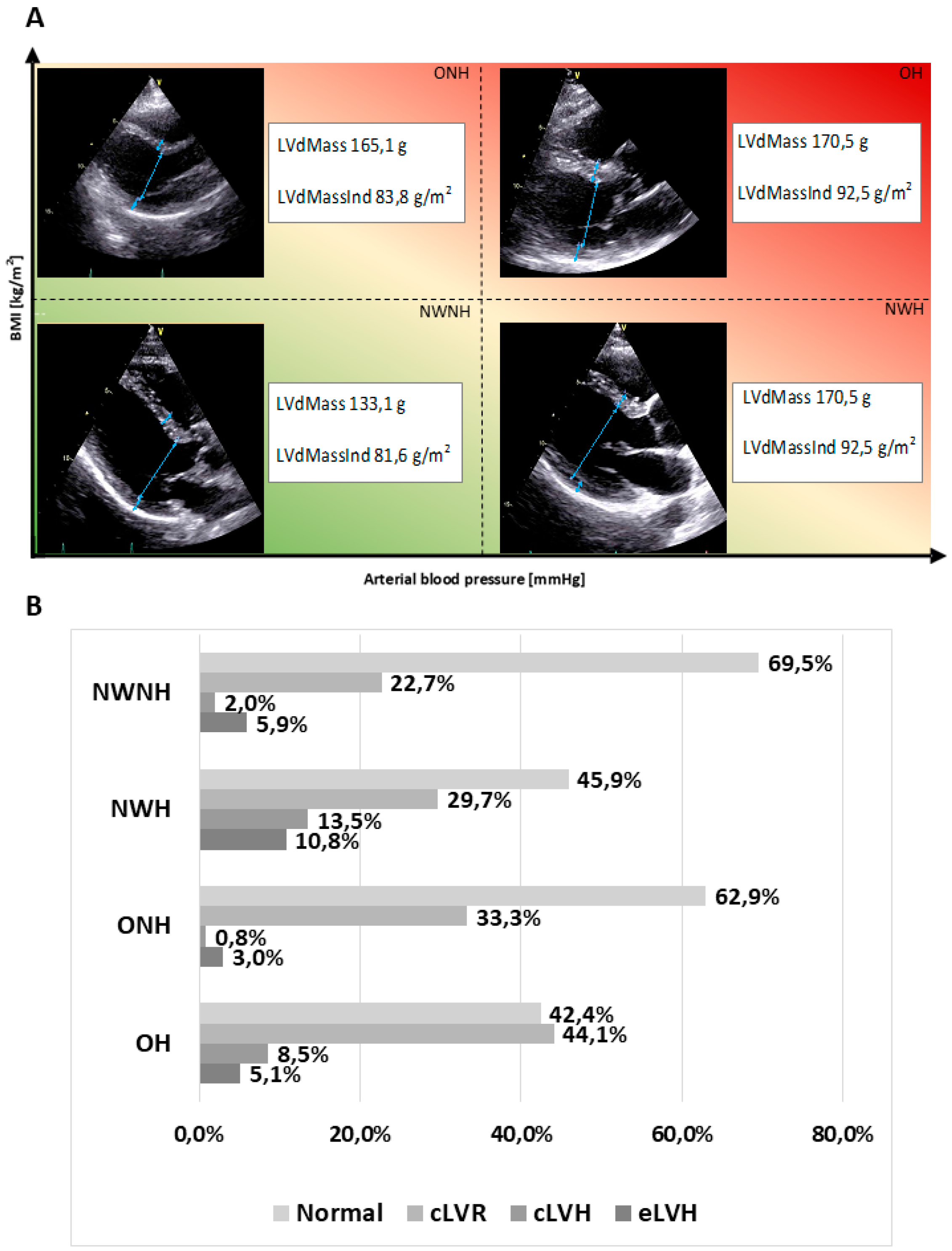
3.4. Left Ventricular Geometry According to BMI and Hypertension
3.5. Association of Hypertension and Obesity with Left Ventricular Geometry
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ganau, A.; Devereux, R.B.; Roman, M.J.; de Simone, G.; Pickering, T.G.; Saba, P.S.; Vargiu, P.; Simongini, I.; Laragh, J.H. Patterns of left ventricular hypertrophy and geometric remodeling in essential hypertension. J. Am. Coll. Cardiol. 1992, 19, 1550–1558. [Google Scholar] [CrossRef]
- De Simone, G.; Daniels, S.R.; Kimball, T.R.; Roman, M.J.; Romano, C.; Chinali, M.; Galderisi, M.; Devereux, R.B. Evaluation of concentric left ventricular geometry in humans: Evidence for age-related systematic underestimation. Hypertension 2005, 45, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Lavie, C.J.; Blair, S.N. Obesity and Cardiovascular Disease. Circ. Res. 2016, 118, 1752–1770. [Google Scholar] [CrossRef] [PubMed]
- Kjeldsen, S.E. Hypertension and cardiovascular risk: General aspects. Pharmacol. Res. 2018, 129, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Huang, F.; Chen, J.; Cai, Q.; Wang, T.; Zou, R.; Zuo, Z.; Wang, J.; Huang, H. Independent influence of overweight and obesity on the regression of left ventricular hypertrophy in hypertensive patients: A meta-analysis. Medicine 2014, 93, e130. [Google Scholar] [CrossRef] [PubMed]
- De Cleva, R.; Araujo, V.A.; Buchalla, C.C.O.; de Oliveira Costa, F.; Cardoso, A.F.; Pajecki, D.; Santo, M.A. Cardiac Remodeling Patterns in Severe Obesity According to Arterial Hypertension Grade. Obes. Surg. 2018, 28, 1047–1054. [Google Scholar] [CrossRef] [PubMed]
- Aurigemma, G.P.; de Simone, G.; Fitzgibbons, T.P. Cardiac remodeling in obesity. Circ. Cardiovasc. Imaging 2013, 6, 142–152. [Google Scholar] [CrossRef] [PubMed]
- Avelar, E.; Cloward, T.V.; Walker, J.M.; Farney, R.J.; Strong, M.; Pendleton, R.C.; Segerson, N.; Adams, T.D.; Gress, R.E.; Hunt, S.C.; et al. Left ventricular hypertrophy in severe obesity: Interactions among blood pressure, nocturnal hypoxemia, and body mass. Hypertension 2007, 49, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Rodilla, E.; Costa, J.A.; Martin, J.; Gonzalez, C.; Pascual, J.M.; Redon, J. Impact of abdominal obesity and ambulatory blood pressure in the diagnosis of left ventricular hypertrophy in never treated hypertensives. Med. Clin. 2014, 142, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Agodi, A.; Maugeri, A.; Kunzova, S.; Sochor, O.; Bauerova, H.; Kiacova, N.; Barchitta, M.; Vinciguerra, M. Association of Dietary Patterns with Metabolic Syndrome: Results from the Kardiovize Brno 2030 Study. Nutrients 2018, 10, 898. [Google Scholar] [CrossRef] [PubMed]
- Maugeri, A.; Kunzova, S.; Medina-Inojosa, J.R.; Agodi, A.; Barchitta, M.; Homolka, M.; Kiacova, N.; Bauerova, H.; Sochor, O.; Lopez-Jimenez, F.; et al. Association between eating time interval and frequency with ideal cardiovascular health: Results from a random sample Czech urban population. Nutr. Metab. Cardiovasc. Dis. NMCD 2018. [Google Scholar] [CrossRef] [PubMed]
- Hruskova, J.; Maugeri, A.; Podrouzkova, H.; Stipalova, T.; Jakubik, J.; Barchitta, M.; Medina-Inojosa, J.R.; Homolka, M.; Agodi, A.; Kunzova, S.; et al. Association of Cardiovascular Health with Epicardial Adipose Tissue and Intima Media Thickness: The Kardiovize Study. J. Clin. Med. 2018, 7, 113. [Google Scholar] [CrossRef] [PubMed]
- Movsisyan, N.K.; Vinciguerra, M.; Lopez-Jimenez, F.; Kunzová, Š.; Homolka, M.; Jaresova, J.; Cífková, R.; Sochor, O. Kardiovize Brno 2030, a prospective cardiovascular health study in Central Europe: Methods, baseline findings and future directions. Eur. J. Prev. Cardiol. 2017. [Google Scholar] [CrossRef] [PubMed]
- Maugeri, A.; Medina-Inojosa, J.R.; Kunzova, S.; Agodi, A.; Barchitta, M.; Sochor, O.; Lopez-Jimenez, F.; Geda, Y.E.; Vinciguerra, M. Sleep Duration and Excessive Daytime Sleepiness Are Associated with Obesity Independent of Diet and Physical Activity. Nutrients 2018, 10, 1219. [Google Scholar] [CrossRef] [PubMed]
- Maugeri, A.; Hruskova, J.; Jakubik, J.; Kunzova, S.; Sochor, O.; Barchitta, M.; Agodi, A.; Bauerova, H.; Medina-Inojosa, J.R.; Vinciguerra, M. Dietary antioxidant intake decreases carotid intima media thickness in women but not in men: A cross-sectional assessment in the Kardiovize study. Free Radic. Biol. Med. 2019, 131, 274–281. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Physical status: The use and interpretation of anthropometry. Report of a WHO Expert Committee. World Health Organ. Tech. Rep. Ser. 1995, 854, 1–452. [Google Scholar]
- WHO. Waist Circumference and Waist–Hip Ratio: Report of a WHO Expert Consultation; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [PubMed]
- Zoghbi, W.A.; Adams, D.; Bonow, R.O.; Enriquez-Sarano, M.; Foster, E.; Grayburn, P.A.; Hahn, R.T.; Han, Y.; Hung, J.; Lang, R.M.; et al. Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Magnetic Resonance. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2017, 30, 303–371. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd.; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.L.; Jones, D.W.; Materson, B.J.; Oparil, S.; Wright, J.T.; et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003, 42, 1206–1252. [Google Scholar] [CrossRef] [PubMed]
- De Simone, G.; Izzo, R.; De Luca, N.; Gerdts, E. Left ventricular geometry in obesity: Is it what we expect? Nutr. Metab. Cardiovasc. Dis. 2013, 23, 905–912. [Google Scholar] [CrossRef] [PubMed]
- De Simone, G.; Palmieri, V.; Bella, J.N.; Celentano, A.; Hong, Y.; Oberman, A.; Kitzman, D.W.; Hopkins, P.N.; Arnett, D.K.; Devereux, R.B. Association of left ventricular hypertrophy with metabolic risk factors: The HyperGEN study. J. Hypertens. 2002, 20, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Lauer, M.S.; Anderson, K.M.; Kannel, W.B.; Levy, D. The impact of obesity on left ventricular mass and geometry. The Framingham Heart Study. JAMA 1991, 266, 231–236. [Google Scholar] [CrossRef] [PubMed]
- De Simone, G.; Devereux, R.B.; Roman, M.J.; Alderman, M.H.; Laragh, J.H. Relation of obesity and gender to left ventricular hypertrophy in normotensive and hypertensive adults. Hypertension 1994, 23, 600–606. [Google Scholar] [CrossRef] [PubMed]
- Cuspidi, C.; Rescaldani, M.; Sala, C.; Grassi, G. Left-ventricular hypertrophy and obesity: A systematic review and meta-analysis of echocardiographic studies. J. Hypertens. 2014, 32, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Grossman, W.; Jones, D.; McLaurin, L.P. Wall stress and patterns of hypertrophy in the human left ventricle. J. Clin. Investig. 1975, 56, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Poirier, P.; Giles, T.D.; Bray, G.A.; Hong, Y.; Stern, J.S.; Pi-Sunyer, F.X.; Eckel, R.H.; American Heart Association; Obesity Committee of the Council on Nutrition, Physical Activity, and Metabolism. Obesity and cardiovascular disease: Pathophysiology, evaluation, and effect of weight loss: An update of the 1997 American Heart Association Scientific Statement on Obesity and Heart Disease from the Obesity Committee of the Council on Nutrition, Physical Activity, and Metabolism. Circulation 2006, 113, 898–918. [Google Scholar] [CrossRef]
- Cheng, S.; Fernandes, V.R.; Bluemke, D.A.; McClelland, R.L.; Kronmal, R.A.; Lima, J.A. Age-related left ventricular remodeling and associated risk for cardiovascular outcomes: The Multi-Ethnic Study of Atherosclerosis. Circ. Cardiovasc. Imaging 2009, 2, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Heesen, W.F.; Beltman, F.W.; May, J.F.; Smit, A.J.; de Graeff, P.A.; Havinga, T.K.; Schuurman, F.H.; van der Veur, E.; Hamer, J.P.; Meyboom-de Jong, B.; et al. High prevalence of concentric remodeling in elderly individuals with isolated systolic hypertension from a population survey. Hypertension 1997, 29, 539–543. [Google Scholar] [CrossRef] [PubMed]
- Kostkiewicz, M.; Tracz, W.; Olszowska, M.; Podolec, P.; Drop, D. Left ventricular geometry and function in patients with aortic stenosis: Gender differences. Int. J. Cardiol. 1999, 71, 57–61. [Google Scholar] [CrossRef]
- Krumholz, H.M.; Larson, M.; Levy, D. Sex differences in cardiac adaptation to isolated systolic hypertension. Am. J. Cardiol. 1993, 72, 310–313. [Google Scholar] [CrossRef]
- Woodiwiss, A.J.; Norton, G.R. Obesity and left ventricular hypertrophy: The hypertension connection. Curr. Hypertens. Rep. 2015, 17, 539. [Google Scholar] [CrossRef] [PubMed]
- De Simone, G.; Kizer, J.R.; Chinali, M.; Roman, M.J.; Bella, J.N.; Best, L.G.; Lee, E.T.; Devereux, R.B.; Investigators, S.H.S. Normalization for body size and population-attributable risk of left ventricular hypertrophy: The Strong Heart Study. Am. J. Hypertens. 2005, 18, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Alessandro Gondoni, L.; Titon, A.M.; Montano, M.; Nibbio, F.; Bertone, G. The importance of a shared definition of left ventricular hypertrophy: The case of obese women. Int. J. Cardiol. 2017, 227, 404–406. [Google Scholar] [CrossRef] [PubMed]
- Schmieder, R.E.; Martus, P.; Klingbeil, A. Reversal of left ventricular hypertrophy in essential hypertension. A meta-analysis of randomized double-blind studies. JAMA 1996, 275, 1507–1513. [Google Scholar] [CrossRef] [PubMed]
- Schmieder, R.E.; Schlaich, M.P.; Klingbeil, A.U.; Martus, P. Update on reversal of left ventricular hypertrophy in essential hypertension (a meta-analysis of all randomized double-blind studies until December 1996). Nephrol. Dial. Transpl. 1998, 13, 564–569. [Google Scholar] [CrossRef]

{kind=link}
| Characteristics | NWNH (n = 204) | NWH (n = 37) | p-Value | ONH (n = 132) | p-Value | OH (n = 60) | p-Value |
|---|---|---|---|---|---|---|---|
| Age, years | 42.0 (16.0) | 49.0 (19.0) | 0.028 | 44.5 (16.3) | 0.244 | 52.0 (17.5) | <0.001 |
| Sex (% male) | 38.2% | 48.6% | 0.234 | 64.4% | <0.001 | 60.0% | 0.003 |
| Education level (% low) | 7.8% | 5.4% | 0.138 | 11.5% | 0.002 | 11.7% | 0.567 |
| Marital status (% living alone) | 41.2% | 37.8% | 0.704 | 35.1% | 0.267 | 26.7% | 0.042 |
| Employment (% unemployed) | 12.5% | 13.5% | 0.895 | 8.5% | 0.056 | 13.6% | 0.266 |
| Smoking (% current smokers) | 21.6% | 35.1% | 0.310 | 15.9% | 0.238 | 11.7% | 0.128 |
| Physical activity, MET-min/week | 2983 (3363) | 34485 (5731) | 0.523 | 3555 (5593) | 0.355 | 3297 (3736) | 0.637 |
| Weight, Kg | 66.0 (14.0) | 68.0 (10.0) | 0.135 | 88.0 (14.0) | <0.001 | 88.0 (21.0) | <0.001 |
| BMI, Kg/m2 | 21.9 (2.8) | 23.0 (2.3) | 0.034 | 27.4 (2.8) | <0.001 | 27.9 (4.2) | <0.001 |
| Waist circumference, cm | 78.0 (11.0) | 82.9 (12.0) | 0.012 | 95.0 (10.0) | <0.001 | 99.0 (17.0) | <0.001 |
| Fat mass (%) | 20.3 (10.8) | 21.8 (9.3) | 0.285 | 25.0 (13.8) | <0.001 | 28.0 (13.5) | <0.001 |
| Central Obesity (%) | 0.0% | 0.0% | - | 34.8% | <0.001 | 48.3% | <0.001 |
| Systolic Blood Pressure, mmHg | 111.0 (13.0) | 131.0 (21.0) | <0.001 | 115.0 (10.5) | <0.001 | 138.3 (18.4) | <0.001 |
| Diastolic Blood Pressure, mmHg | 74.0 (11.0) | 87.5 (11.5) | <0.001 | 77.5 (10.0) | <0.001 | 91.0 (7.4) | <0.001 |
| Fasting Glucose, mmol/L | 4.7 (0.7) | 4.8 (056) | 0.014 | 4.9 (0.6) | <0.001 | 4.9 (0.6) | <0.001 |
| Triglycerides, mmol/L | 0.85 (0.40) | 0.86 (0.70) | 0.141 | 1.21 (1.0) | <0.001 | 1.24 (0.9) | <0.001 |
| Total Cholesterol, mmol/L | 4.9 (1.4) | 5.0 (1.5) | 0.457 | 5.4 (1.6) | <0.001 | 5.2 (1.3) | 0.004 |
| HDL Cholesterol, mmol/L | 1.6 (0.5) | 1.6 (0.5) | 0.946 | 1.3 (0.5) | <0.001 | 1.4 (0.5) | <0.001 |
| LDL Cholesterol, mmol/L | 2.9 (1.1) | 2.8 (1.2) | 0.754 | 3.4 (1.4) | <0.001 | 3.3 (1.2) | <0.001 |
| Characteristics | Bivariate Correlation | Linear Regression | ||
|---|---|---|---|---|
| Spearman Correlation Coefficient | p-Value | Standardized Coefficient (β) | p-Value | |
| Age, years | 0.097 | 0.043 | 0.040 | 0.353 |
| BMI, Kg/m2 | 0.207 | <0.001 | 0.171 | 0.037 |
| Waist circumference, cm | 0.292 | <0.001 | 0.167 | 0.087 |
| Systolic Blood Pressure, mmHg | 0.253 | <0.001 | 0.153 | 0.023 |
| Diastolic Blood Pressure, mmHg | 0.242 | <0.001 | −0.027 | 0.676 |
| Fasting Glucose, mmol/L | 0.120 | 0.013 | −0.006 | 0.883 |
| Triglycerides, mmol/L | 0.128 | 0.008 | −0.026 | 0.533 |
| HDL Cholesterol, mmol/L | −0.246 | <0.001 | −0.041 | 0.344 |
| LDL Cholesterol, mmol/L | −0.004 | 0.928 | - | - |
| Characteristics | NWNH (n = 204) | NWH (n = 37) | p-Value | ONH (n = 132) | p-Value | OH (n = 60) | p-Value |
|---|---|---|---|---|---|---|---|
| LVM | 133.1 (51.9) | 145.0 (55.8) | 0.015 | 165.1 (44.1) | <0.001 | 170.5 (59.9) | <0.001 |
| LVMIe | 81.6 (24.3) | 82.7 (31.3) | 0.048 | 83.8 (19.6) | 0.017 | 92.5 (22.5) | 0.001 |
| RWT | 0.37 (0.08) | 0.42 (0.08) | 0.002 | 0.40 (0.09) | 0.012 | 0.43 (0.09) | 0.003 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maugeri, A.; Hruskova, J.; Jakubik, J.; Barchitta, M.; Lo Re, O.; Kunzova, S.; Medina-Inojosa, J.R.; Agodi, A.; Sciacca, S.; Vinciguerra, M. Independent Effects of Hypertension and Obesity on Left Ventricular Mass and Geometry: Evidence from the Cardiovision 2030 Study. J. Clin. Med. 2019, 8, 370. https://doi.org/10.3390/jcm8030370
Maugeri A, Hruskova J, Jakubik J, Barchitta M, Lo Re O, Kunzova S, Medina-Inojosa JR, Agodi A, Sciacca S, Vinciguerra M. Independent Effects of Hypertension and Obesity on Left Ventricular Mass and Geometry: Evidence from the Cardiovision 2030 Study. Journal of Clinical Medicine. 2019; 8(3):370. https://doi.org/10.3390/jcm8030370
Chicago/Turabian StyleMaugeri, Andrea, Jana Hruskova, Juraj Jakubik, Martina Barchitta, Oriana Lo Re, Sarka Kunzova, Jose R. Medina-Inojosa, Antonella Agodi, Sergio Sciacca, and Manlio Vinciguerra. 2019. "Independent Effects of Hypertension and Obesity on Left Ventricular Mass and Geometry: Evidence from the Cardiovision 2030 Study" Journal of Clinical Medicine 8, no. 3: 370. https://doi.org/10.3390/jcm8030370
APA StyleMaugeri, A., Hruskova, J., Jakubik, J., Barchitta, M., Lo Re, O., Kunzova, S., Medina-Inojosa, J. R., Agodi, A., Sciacca, S., & Vinciguerra, M. (2019). Independent Effects of Hypertension and Obesity on Left Ventricular Mass and Geometry: Evidence from the Cardiovision 2030 Study. Journal of Clinical Medicine, 8(3), 370. https://doi.org/10.3390/jcm8030370