Dialysis Reimbursement: What Impact Do Different Models Have on Clinical Choices?

 ,
,  ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Costs and Reimbursements: Not the Same Story
3. Dialysis Reimbursement: Per Session, Per Patient, Per Bundle
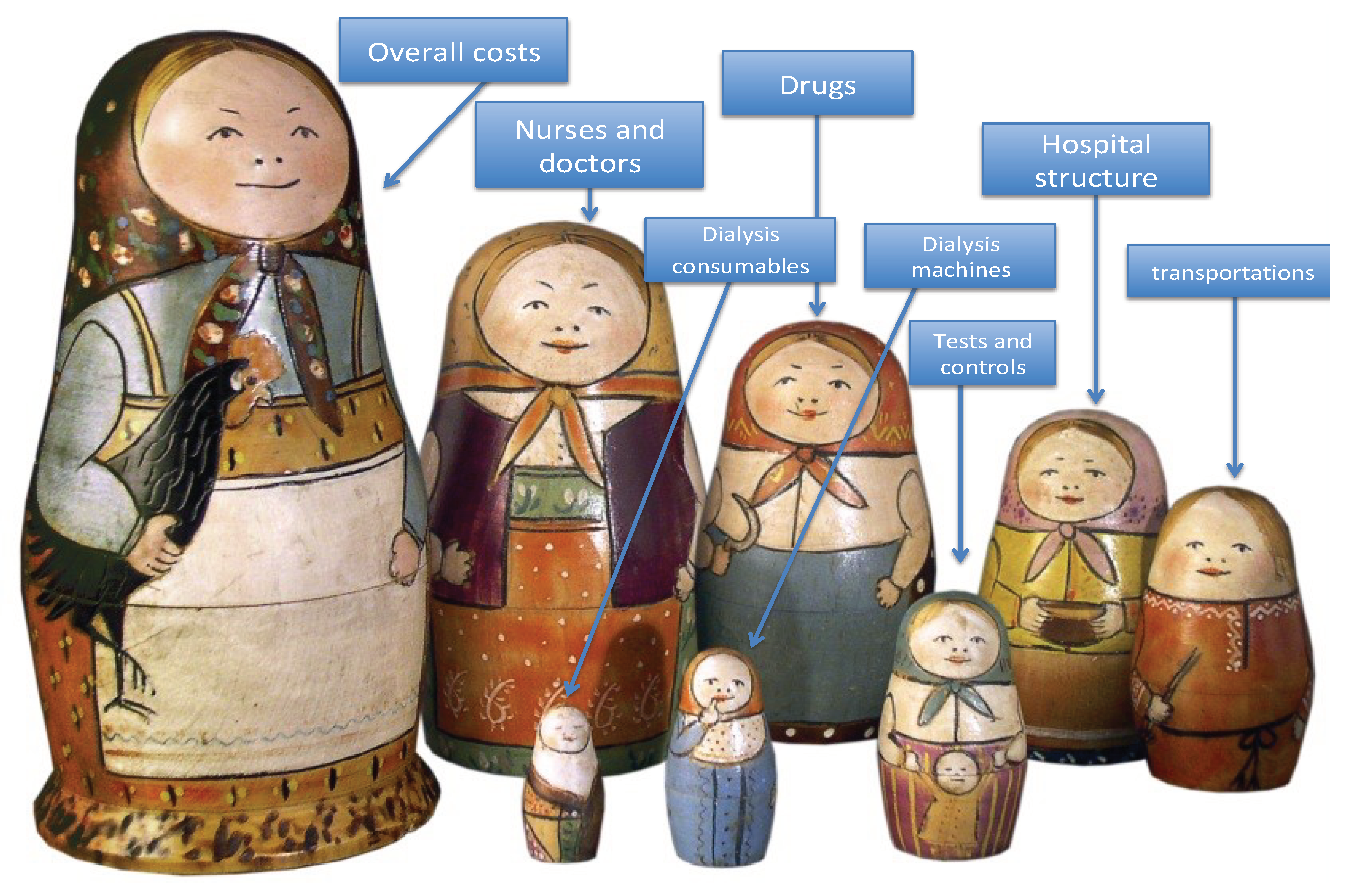
4. Reimbursement Per Separate Element: Dialysis Treatment Seen as a Matryoshka
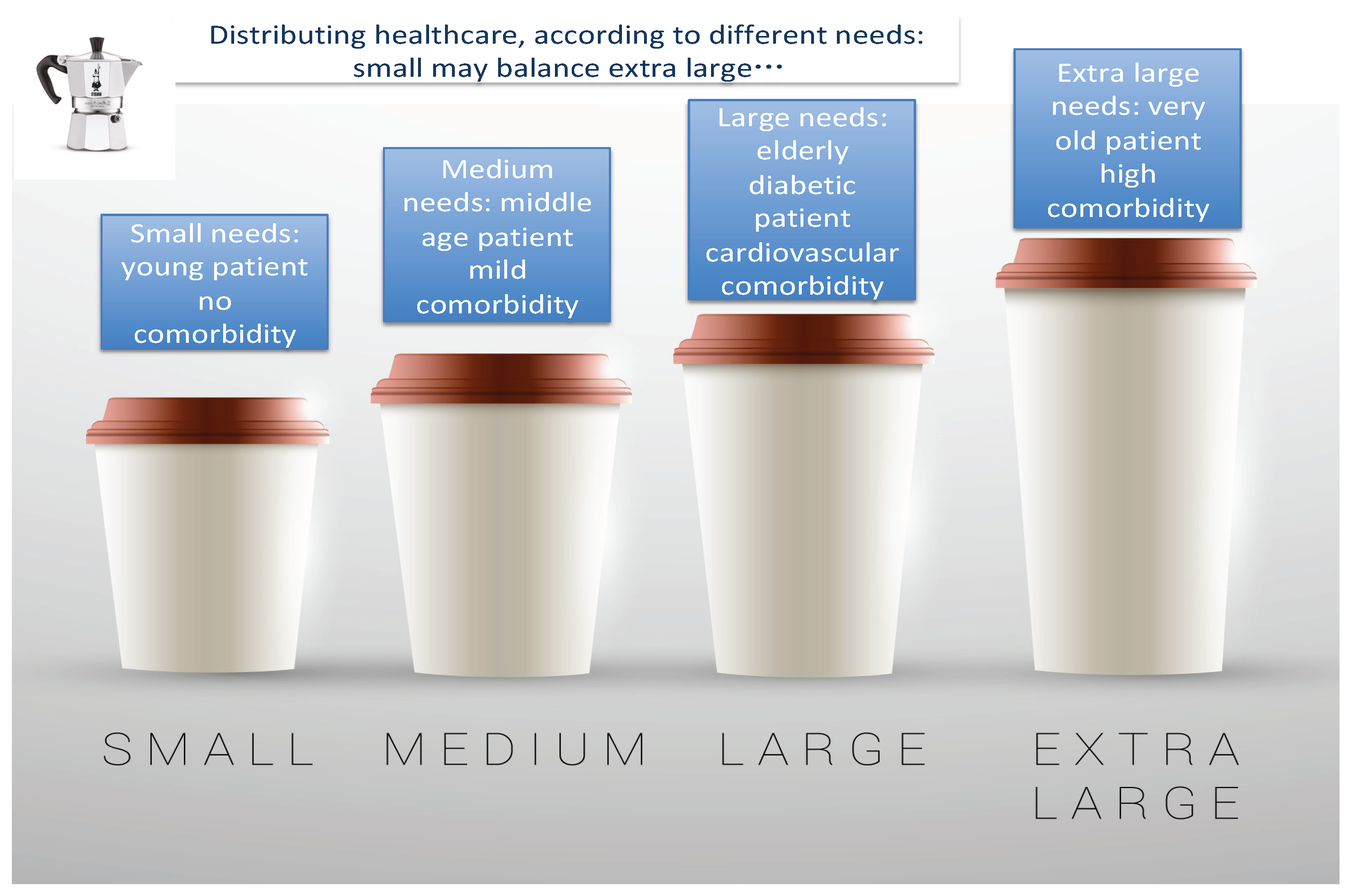
5. The “Capitation System” of Reimbursement: Dialysis Treatment Seen with a Distributive Approach
6. What Is Favourable for the Patient and for the System May Not Be Favourable for the Hospital: The Case of Incremental Dialysis
7. Is Bundled Care the Solution? Defining the Core, Defining Comorbidity: A Difficult Mission
8. A Fundamental Question: Haemodialysis or Peritoneal Dialysis?
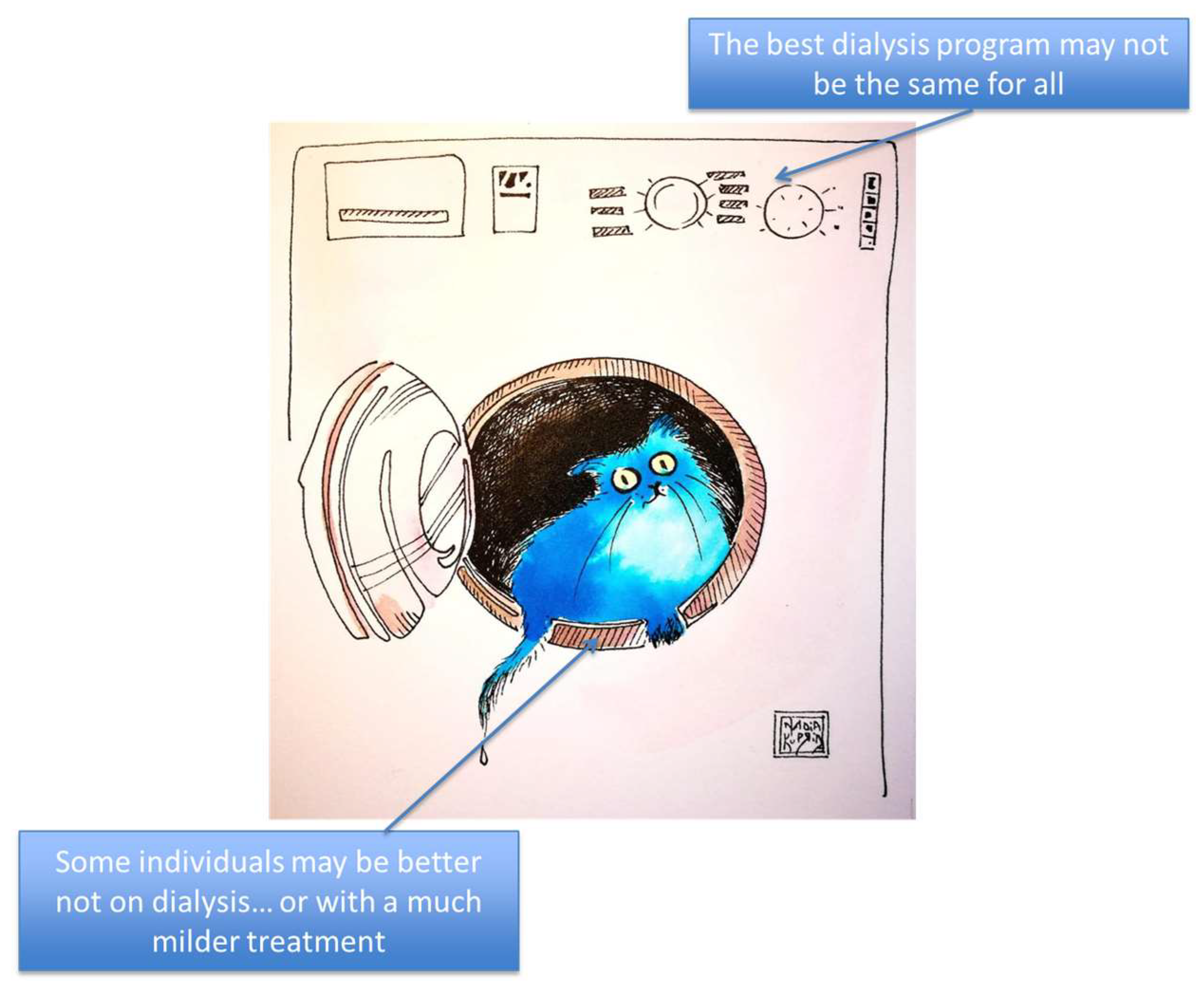
9. One-Size-Fits-All or Tailor-Made Treatments?
10. Predialysis Care May Be Good for the Patient and for the Community, but Less Rewarding for the Hospital
11. Concluding Remarks
Author Contributions
Acknowledgments
Conflicts of Interest
References
- United States Renal Data System. Chapter 1: Incidence, Prevalence, Patient Characteristics, and Treatment Modalities. Available online: https://www.usrds.org/2017/view/v2_01.aspx (accessed on 20 October 2018).
- United States Renal Data System. Chapter 11: International Comparisons. Available online: https://www.usrds.org/2017/view/v2_11.aspx (accessed on 20 October 2018).
- Robinson, B.M.; Akizawa, T.; Jager, K.J.; Kerr, P.G.; Saran, R.; Pisoni, R.L. Factors affecting outcomes in patients reaching end-stage kidney disease worldwide: Differences in access to renal replacement therapy, modality use, and haemodialysis practices. Lancet 2016, 388, 294–306. [Google Scholar] [CrossRef]
- Lu, J.L.; Molnar, M.Z.; Sumida, K.; Diskin, C.D.; Streja, E.; Siddiqui, O.A.; Kalantar-Zadeh, K.; Kovesdy, C.P. Association of the frequency of pre-end-stage renal disease medical care with post-end-stage renal disease mortality and hospitalization. Nephrol. Dial. Transpl. 2018, 33, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Yang, W.C.; Hwang, S.J.; Taiwan Society of Nephrology. Incidence, prevalence and mortality trends of dialysis end-stage renal disease in Taiwan from 1990 to 2001: The impact of national health insurance. Nephrol. Dial. Transpl. 2008, 23, 3977–3982. [Google Scholar] [CrossRef] [PubMed]
- Yen-Chung, L.; Chiao-Ying, H.; Chih-Chin, K.; Tzen-Wen, C.; His-Hsien, C.; Chi-Cheng, H.; Mai-Szu, W. Incidence and Prevalence of ESRD in Taiwan Renal Registry Data System (TWRDS): 2005-2012. Acta Nephrologica 2014, 28, 65–68. [Google Scholar]
- Tattersall, J.; Dekker, F.; Heimbürger, O.; Jager, K.J.; Lameire, N.; Lindley, E.; Van Biesen, W.; Vanholder, R.; Zoccali, C.; ERBP Advisory Board. When to start dialysis: Updated guidance following publication of the Initiating Dialysis Early and Late (IDEAL) study. Nephrol. Dial. Transpl. 2011, 26, 2082–2086. [Google Scholar] [CrossRef] [PubMed]
- Liberek, T.; Warzocha, A.; Galgowska, J.; Taszner, K.; Clark, W.F.; Rutkowski, B. When to initiate dialysis—Is early start always better? Nephrol. Dial. Transpl. 2011, 26, 2087–2091. [Google Scholar] [CrossRef] [PubMed]
- Nesrallah, G.E.; Mustafa, R.A.; Clark, W.F.; Bass, A.; Barnieh, L.; Hemmelgarn, B.R.; Klarenbach, S.; Quinn, R.R.; Hiremath, S.; Ravani, P.; et al. Canadian Society of Nephrology 2014 clinical practice guideline for timing the initiation of chronic dialysis. CMAJ 2014, 186, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Verberne, W.R.; Geers, A.B.; Jellema, W.T.; Vincent, H.H.; van Delden, J.J.; Bos, W.J. Comparative Survival among Older Adults with Advanced Kidney Disease Managed Conservatively Versus with Dialysis. Clin. J. Am. Soc. Nephrol. 2016, 11, 633–640. [Google Scholar] [CrossRef] [PubMed]
- Morton, R.L.; Webster, A.C.; McGeechan, K.; Howard, K.; Murtagh, F.E.; Gray, N.A.; Kerr, P.G.; Germain, M.J.; Snelling, P. Conservative Management and End-of-Life Care in an Australian Cohort with ESRD. Clin. J. Am. Soc. Nephrol. 2016, 11, 2195–2203. [Google Scholar] [CrossRef] [PubMed]
- Wongrakpanich, S.; Susantitaphong, P.; Isaranuwatchai, S.; Chenbhanich, J.; Eiam-Ong, S.; Jaber, B.L. Dialysis Therapy and Conservative Management of Advanced Chronic Kidney Disease in the Elderly: A Systematic Review. Nephron 2017, 137, 178–189. [Google Scholar] [CrossRef] [PubMed]
- Grubbs, V.; Moss, A.H.; Cohen, L.M.; Fischer, M.J.; Germain, M.J.; Jassal, S.V.; Perl, J.; Weiner, D.E.; Mehrotra, R.; Dialysis Advisory Group of the American Society of Nephrology. A palliative approach to dialysis care: A patient-centered transition to the end of life. Clin. J. Am. Soc. Nephrol. 2014, 9, 2203–2209. [Google Scholar] [CrossRef] [PubMed]
- Vanholder, R.; Annemans, L.; Brown, E.; Gansevoort, R.; Gout-Zwart, J.J.; Lameire, N.; Morton, R.L.; Oberbauer, R.; Postma, M.J.; Tonelli, M.; et al. Reducing the costs of chronic kidney disease while delivering quality health care: A call to action. Nat. Rev. Nephrol. 2017, 13, 393–409. [Google Scholar] [CrossRef] [PubMed]
- Vanholder, R.; Lameire, N.; Annemans, L.; Van Biesen, W. Cost of renal replacement: How to help as many as possible while keeping expenses reasonable? Nephrol. Dial. Transpl. 2016, 31, 1251–1261. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, J.K.; Neovius, M.; Jacobson, S.H.; Elinder, C.G.; Hylander, B. Healthcare costs in chronic kidney disease and renal replacement therapy: A population-based cohort study in Sweden. BMJ Open 2016, 6, e012062. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Garcia, G.; Jha, V.; World Kidney Day Steering Committee. CKD in disadvantaged populations. Kidney Int. 2015, 87, 251–253. [Google Scholar] [CrossRef] [PubMed]
- Teerawattananon, Y.; Luz, A.; Pilasant, S.; Tangsathitkulchai, S.; Chootipongchaivat, S.; Tritasavit, N.; Yamabhai, I.; Tantivess, S. How to meet the demand for good quality renal dialysis as part of universal health coverage in resource-limited settings? Health Res. Policy Syst. 2016, 14, 21. [Google Scholar] [CrossRef] [PubMed]
- Voelker, R. Cost of Transplant vs Dialysis. JAMA 1999, 281, 2277. [Google Scholar] [CrossRef]
- Silva, S.B.; Caulliraux, H.M.; Araújo, C.A.; Rocha, E. Cost comparison of kidney transplant versus dialysis in Brazil. Cad. Saude Publica 2016, 32. [Google Scholar] [CrossRef]
- Ferguson, T.W.; Tangri, N.; Rigatto, C.; Komenda, P. Cost-effective treatment modalities for reducing morbidity associated with chronic kidney disease. Expert Rev. Pharmacoecon Outcomes Res. 2015, 15, 243–252. [Google Scholar] [CrossRef] [PubMed]
- Jensen, C.E.; Sørensen, P.; Petersen, K.D. In Denmark kidney transplantation is more cost-effective than dialysis. Dan Med. J. 2014, 61, A4796. [Google Scholar] [PubMed]
- Blotière, P.O.; Tuppin, P.; Weill, A.; Ricordeau, P.; Allemand, H. The cost of dialysis and kidney transplantation in France in 2007, impact of an increase of peritoneal dialysis and transplantation. Nephrol. Ther. 2010, 6, 240–247. [Google Scholar] [CrossRef] [PubMed]
- Howard, K.; Salkeld, G.; White, S.; McDonald, S.; Chadban, S.; Craig, J.C.; Cass, A. The cost-effectiveness of increasing kidney transplantation and home-based dialysis. Nephrology 2009, 14, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Tonelli, M.; Wiebe, N.; Knoll, G.; Bello, A.; Browne, S.; Jadhav, D.; Klarenbach, S.; Gill, J. Systematic review: Kidney transplantation compared with dialysis in clinically relevant outcomes. Am. J. Transpl. 2011, 11, 2093–2109. [Google Scholar] [CrossRef] [PubMed]
- McDonald, S.P.; Russ, G.R. Survival of recipients of cadaveric kidney transplants compared with those receiving dialysis treatment in Australia and New Zealand, 1991–2001. Nephrol. Dial. Transpl. 2002, 17, 2212–2219. [Google Scholar] [CrossRef]
- Ruck, J.M.; Segev, D.L. Expanding deceased donor kidney transplantation: Medical risk, infectious risk, hepatitis C. virus, and HIV. Curr. Opin. Nephrol. Hypertens. 2018, 27, 445–453. [Google Scholar] [CrossRef] [PubMed]
- Sypek, M.P.; Clayton, P.A.; Lim, W.; Hughes, P.; Kanellis, J.; Wright, J.; Chapman, J.; McDonald, S.P. Access to waitlisting for deceased donor kidney transplantation in Australia. Nephrology 2018. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.B.; Eddinger, K.C.; Locke, J.E.; Forde, K.A.; Reese, P.P.; Sawinski, D.L. Survival Benefit of Transplantation with a Deceased Diabetic Donor Kidney Compared with Remaining on the Waitlist. Clin. J. Am. Soc. Nephrol. 2017, 12, 974–982. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.statista.com/statistics/628386/kidney-transplant-waiting-time-from-dialysis-europe/ (accessed on 20 October 2018).
- Oniscu, G.C.; Brown, H.; Forsythe, J.L. How old is old for transplantation? Am. J. Transpl. 2004, 4, 2067–2074. [Google Scholar] [CrossRef] [PubMed]
- Bastani, B. The worsening transplant organ shortage in USA; desperate times demand innovative solutions. J. Nephropathol. 2015, 4, 105–109. [Google Scholar] [PubMed]
- Heldal, K.; Hartmann, A.; Lønning, K.; Leivestad, T.; Reisæter, A.V.; Line, P.D.; Holdaas, H.; Midtvedt, K. Should patients older than 65 years be offered a second kidney transplant? BMC Nephrol. 2017, 18, 13. [Google Scholar] [CrossRef] [PubMed]
- Hippen, B. Debating Organ Procurement Policy Without Illusions. Am. J. Kidney Dis. 2015, 66, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Shrestha, B.M. Strategies for reducing the renal transplant waiting list: A review. Exp. Clin. Transpl. 2009, 7, 173–179. [Google Scholar]
- Barnieh, L.; Klarenbach, S.; Gill, J.S.; Caulfield, T.; Manns, B. Attitudes toward strategies to increase organ donation: Views of the general public and health professionals. Clin. J. Am. Soc. Nephrol. 2012, 7, 1956–1963. [Google Scholar] [CrossRef] [PubMed]
- Gordon, E.J.; Patel, C.H.; Sohn, M.W.; Hippen, B.; Sherman, L.A. Does financial compensation for living kidney donation change willingness to donate? Am. J. Transpl. 2015, 15, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Cairns, J.A.; Fotheringham, J.; Tomson, C.R.; Forsythe, J.L.; Watson, C.; Metcalfe, W.; Fogarty, D.G.; Draper, H.; Oniscu, G.C.; et al. Understanding cost of care for patients on renal replacement therapy: Looking beyond fixed tariffs. Nephrol. Dial. Transpl. 2015, 30, 1726–1734. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.K.; Hsu, C.C.; Chen, P.C.; Chen, Y.S.; Hwang, S.J.; Li, T.C.; Huang, C.C.; Li, C.Y.; Sung, F.C. Trends of cost and mortality of patients on haemodialysis with end stage renal disease. Nephrology 2015, 20, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Rocha, M.J.; Ferreira, S.; Martins, L.S.; Almeida, M.; Dias, L.; Pedroso, S.; Henriques, A.C.; Almeida, R.; Cabrita, A. Cost analysis of renal replacement therapy by transplant in a system of bundled payment of dialysis. Clin. Transpl. 2012, 26, 529–531. [Google Scholar] [CrossRef] [PubMed]
- Vanholder, R.; Davenport, A.; Hannedouche, T.; Kooman, J.; Kribben, A.; Lameire, N.; Lonnemann, G.; Magner, P.; Mendelssohn, D.; Saggi, S.J.; et al. Reimbursement of dialysis: A comparison of seven countries. J. Am. Soc. Nephrol. 2012, 23, 1291–1298. [Google Scholar] [CrossRef] [PubMed]
- Chow, K.M.; Li, P.K. Dialysis: Choice of dialysis--what to do with economic incentives. Nat. Rev. Nephrol. 2012, 8, 495–496. [Google Scholar] [CrossRef] [PubMed]
- Manandhar, D.N.; Chhetri, P.K.; Tiwari, R.; Lamichhane, S. Evaluation of dialysis adequacy in patients under hemodialysis and effectiveness of dialysers reuses. Nepal Med. Coll. J. 2009, 11, 107–110. [Google Scholar] [PubMed]
- Brown, C. Current opinion and controversies of dialyser reuse. Saudi J. Kidney Dis. Transpl. 2001, 12, 352–363. [Google Scholar] [PubMed]
- Robinson, B.M.; Feldman, H.I. Dialyzer reuse and patient outcomes: What do we know now? Semin. Dial. 2005, 18, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Locatelli, F.; Andrulli, S.; D’Amico, M. Evaluation of dialysis outcomes: Experimental versus observational evidence. J. Nephrol. 2001, 14, S101–S108. [Google Scholar] [PubMed]
- Goodkin, D.A.; Mapes, D.L.; Held, P.J. The dialysis outcomes and practice patterns study (DOPPS): How can we improve the care of hemodialysis patients? Semin. Dial. 2001, 14, 157–159. [Google Scholar] [CrossRef] [PubMed]
- Pisoni, R.L.; Young, E.W.; Dykstra, D.M.; Greenwood, R.N.; Hecking, E.; Gillespie, B.; Wolfe, R.A.; Goodkin, D.A.; Held, P.J. Vascular access use in Europe and the United States: Results from the DOPPS. Kidney Int. 2002, 61, 305–316. [Google Scholar] [CrossRef] [PubMed]
- Pisoni, R.L.; Bragg-Gresham, J.L.; Young, E.W.; Akizawa, T.; Asano, Y.; Locatelli, F.; Bommer, J.; Cruz, J.M.; Kerr, P.G.; Mendelssohn, D.C.; et al. Anemia management and outcomes from 12 countries in the Dialysis Outcomes and Practice Patterns Study (DOPPS). Am. J. Kidney Dis. 2004, 44, 94–111. [Google Scholar] [CrossRef] [PubMed]
- Hirth, R.A. International economics of dialysis: Lessons from the DOPPS. Semin. Dial. 2010, 23, 16–18. [Google Scholar] [CrossRef] [PubMed]
- Rhee, C.M.; Obi, Y.; Mathew, A.T.; Kalantar-Zadeh, K. Precision Medicine in the Transition to Dialysis and Personalized Renal Replacement Therapy. Semin. Nephrol. 2018, 38, 325–335. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Nielsen, L.; Gendrot, L.; Fois, A.; Cataldo, E.; Cabiddu, G. Prescribing Hemodialysis or Hemodiafiltration: When One Size Does Not Fit All the Proposal of a Personalized Approach Based on Comorbidity and Nutritional Status. J. Clin. Med. 2018, 7, 331. [Google Scholar] [CrossRef] [PubMed]
- Gedney, N.; Kalantar-Zadeh, K. Dialysis Patient-Centeredness and Precision Medicine: Focus on Incremental Home Hemodialysis and Preserving Residual Kidney Function. Semin. Nephrol. 2018, 38, 426–432. [Google Scholar] [CrossRef] [PubMed]
- Pauly, R.P. Survival comparison between intensive hemodialysis and transplantation in the context of the existing literature surrounding nocturnal and short-daily hemodialysis. Nephrol. Dial. Transpl. 2013, 28, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B. The never-ending search for the perfect dialysis. Should we move from the best treatment to the best system? Nephrol. Dial. Transpl. 2011, 26, 1128–1131. [Google Scholar] [CrossRef] [PubMed]
- Kleophas, W.; Karaboyas, A.; Li, Y.; Bommer, J.; Reichel, H.; Walter, A.; Icks, A.; Rump, L.C.; Pisoni, R.L.; Robinson, B.M.; et al. Changes in dialysis treatment modalities during institution of flat rate reimbursement and quality assurance programs. Kidney Int. 2013, 84, 578–584. [Google Scholar] [CrossRef] [PubMed]
- Marcelli, D.; Grassmann, A.; Ponce, P. Changes in dialysis treatment modalities during institution of flat-rate reimbursement and quality assurance programs. Kidney Int. 2013, 84, 1051. [Google Scholar] [CrossRef] [PubMed]
- Alquist, M.; Bosch, J.P.; Barth, C.; Combe, C.; Daugirdas, J.T.; Hegbrant, J.B.; Martin, G.; McIntyre, C.W.; O’Donoghue, D.J.; Rodriguez, H.J.; et al. Knowing what we do and doing what we should: Quality assurance in hemodialysis. Nephron Clin. Pract. 2014, 126, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Vaccaro, C.M.; Sopranzi, F. A comparison between the costs of dialysis treatments in Marche Region, Italy: Macerata and Tolentino hospitals. Ann. Ist. Super. Sanita 2017, 53, 344–349. [Google Scholar] [CrossRef] [PubMed]
- Available online: http://www.centresdedialyse.com/wp-content/uploads/2015/03/rapport_dialyse_chronique_France_2016_SFNDT.pdf (accessed on 20 December 2018).
- Available online: http://documenti.sinitaly.org/wp-content/uploads/sites/7/2017/03/rete_nefrologica.pdf (accessed on 20 December 2018).
- Available online: https://www.sigaps.fr (accessed on 20 December 2018).
- Piccoli, G.B.; Nazha, M.; Ferraresi, M.; Vigotti, F.N.; Pereno, A.; Barbero, S. Eco-dialysis: The financial and ecological costs of dialysis waste products: Is a ‘cradle-to-cradle’ model feasible for planet-friendly haemodialysis waste management? Nephrol. Dial. Transpl. 2015, 30, 1018–1027. [Google Scholar] [CrossRef] [PubMed]
- Ponce, P.; Marcelli, D.; Guerreiro, A.; Grassmann, A.; Gonçalves, C.; Scatizzi, L.; Bayh, I.; Stopper, A.; Da Silva, R. Converting to a capitation system for dialysis payment—The Portuguese experience. Blood Purif. 2012, 34, 313–324. [Google Scholar] [CrossRef] [PubMed]
- Available online: http://dialisiperitoneale.org/wp-content/uploads/sites/18/2017/07/Piemonte_DGR_8-12316_12.10.2009-legge.pdf (accessed on 20 October 2018).
- Marinangeli, G.; Cabiddu, G.; Neri, L.; Viglino, G.; Russo, R.; Teatini, U.; Italian Society of Nephrology Peritoneal Dialysis Study Group. Old and new perspectives on peritoneal dialysis in Italy emerging from the Peritoneal Dialysis Study Group Census. Perit. Dial. Int. 2012, 32, 558–565. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.X.; Walton, S.M.; Leipold, R.; Isbell, D.; Golper, T.A. Financial implications to Medicare from changing the dialysis modality mix under the bundled prospective payment system. Perit. Dial. Int. 2014, 34, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Lin, E.; Cheng, X.S.; Chin, K.K.; Zubair, T.; Chertow, G.M.; Bendavid, E.; Bhattacharya, J. Home Dialysis in the Prospective Payment System Era. J. Am. Soc. Nephrol. 2017, 28, 2993–3004. [Google Scholar] [CrossRef] [PubMed]
- Devereaux, P.J.; Schünemann, H.J.; Ravindran, N.; Bhandari, M.; Garg, A.X.; Choi, P.T.; Grant, B.J.; Haines, T.; Lacchetti, C.; Weaver, B.; et al. Comparison of mortality between private for-profit and private not-for-profit hemodialysis centers: A systematic review and meta-analysis. JAMA 2002, 288, 2449–2457. [Google Scholar] [CrossRef] [PubMed]
- Dalrymple, L.S.; Johansen, K.L.; Romano, P.S.; Chertow, G.M.; Mu, Y.; Ishida, J.H.; Grimes, B.; Kaysen, G.A.; Nguyen, D.V. Comparison of hospitalization rates among for-profit and nonprofit dialysis facilities. Clin. J. Am. Soc. Nephrol. 2014, 9, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Johansen, K.L. The Frail Dialysis Population: A Growing Burden for the Dialysis Community. Blood Purif. 2015, 40, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Perneger, T.V.; Leski, M.; Chopard-Stoermann, C.; Martin, P.Y. Assessment of health status in chronic hemodialysis patients. J. Nephrol. 2003, 16, 252–259. [Google Scholar] [PubMed]
- Spatola, L.; Finazzi, S.; Calvetta, A.; Angelini, C.; Badalamenti, S. Subjective Global Assessment-Dialysis Malnutrition Score and arteriovenous fistula outcome: A comparison with Charlson Comorbidity Index. J. Vasc. Access. 2018. [Google Scholar] [CrossRef] [PubMed]
- Miskulin, D. Characterizing comorbidity in dialysis patients: Principles of measurement and applications in risk adjustment and patient care. Perit. Dial. Int. 2005, 25, 320–332. [Google Scholar] [PubMed]
- Miskulin, D.C.; Martin, A.A.; Brown, R.; Fink, N.E.; Coresh, J.; Powe, N.R.; Zager, P.G.; Meyer, K.B.; Levey, A.S.; Medical Directors of Dialysis Clinic, Inc. Predicting 1 year mortality in an outpatient haemodialysis population: A comparison of comorbidity instruments. Nephrol. Dial. Transpl. 2004, 19, 413–420. [Google Scholar] [CrossRef]
- McArthur, E.; Bota, S.E.; Sood, M.M.; Nesrallah, G.E.; Kim, S.J.; Garg, A.X.; Dixon, S.N. Comparing Five Comorbidity Indices to Predict Mortality in Chronic Kidney Disease: A Retrospective Cohort Study. Can. J. Kidney Health Dis. 2018, 5. [Google Scholar] [CrossRef] [PubMed]
- Floege, J.; Gillespie, I.A.; Kronenberg, F.; Anker, S.D.; Gioni, I.; Richards, S.; Pisoni, R.L.; Robinson, B.M.; Marcelli, D.; Froissart, M.; et al. Development and validation of a predictive mortality risk score from a European hemodialysis cohort. Kidney Int. 2015, 87, 996–1008. [Google Scholar] [CrossRef] [PubMed]
- Steenkamp, R.; Caskey, F.J. ‘How long have I got doctor?’ The development and validation of a new prognostic model. Kidney Int. 2015, 87, 879–882. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Cabiddu, G.; Moio, M.R.; Fois, A.; Cao, R.; Molfino, I.; Kaniassi, A.; Lippi, F.; Froger, L.; Pani, A.; et al. Efficiency and nutritional parameters in an elderly high risk population on hemodialysis and hemodiafiltration in Italy and France: Different treatments with similar names? BMC Nephrol. 2018, 19, 171. [Google Scholar] [CrossRef] [PubMed]
- Gencer, F.; Yıldıran, H.; Erten, Y. Association of Malnutrition Inflammation Score With Anthropometric Parameters, Depression, and Quality of Life in Hemodialysis Patients. J. Am. Coll. Nutr. 2018, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Obi, Y.; Kalantar-Zadeh, K. Incremental and Once- to Twice-Weekly Hemodialysis: From Experience to Evidence. Kidney Int. Rep. 2017, 2, 781–784. [Google Scholar] [CrossRef] [PubMed]
- Chin, A.I.; Appasamy, S.; Carey, R.J.; Madan, N. Feasibility of Incremental 2-Times Weekly Hemodialysis in Incident Patients with Residual Kidney Function. Kidney Int. Rep. 2017, 2, 933–942. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Zou, W.; Wu, J.; Liu, L.; He, Q. Comparison between incremental and thrice-Weekly hemodialysis: A systematic review and meta-analysis. Nephrology 2018. [Google Scholar] [CrossRef] [PubMed]
- Himmelfarb, J.; Chertow, G.M. Medicare ESRD prospective payment system: Weighing the evidence. J. Am. Soc. Nephrol. 2005, 16, 1164–1165. [Google Scholar] [CrossRef] [PubMed]
- Deoreo, P.B. How dialysis is paid for: What the dialysis medical director should know, and why. Semin. Dial. 2008, 21, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Kane, R.; Levenson, M.; Kelman, J.; Wernecke, M.; Lee, J.Y.; Kozlowski, S.; Dekmezian, C.; Zhang, Z.; Thompson, A.; et al. Association Between Changes in CMS Reimbursement Policy and Drug Labels for Erythrocyte-Stimulating Agents With Outcomes for Older Patients Undergoing Hemodialysis Covered by Fee-for-Service Medicare. JAMA Intern. Med. 2016, 176, 1818–1825. [Google Scholar] [CrossRef] [PubMed]
- Coyne, D.W. Managing anemia in for-profit dialysis chains: When ethics and business conflict. Semin. Dial. 2009, 22, 18–21. [Google Scholar] [CrossRef] [PubMed]
- Charytan, C. Bundled-rate legislation for Medicare reimbursement for dialysis services: Implications for anemia management with ESAs. Clin. J. Am. Soc. Nephrol. 2010, 5, 2355–2362. [Google Scholar] [CrossRef] [PubMed]
- Hornberger, J.; Hirth, R.A. Financial implications of choice of dialysis type of the revised Medicare payment system: An economic analysis. Am. J. Kidney Dis. 2012, 60, 280–287. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.; Bernardini, J.; Piraino, B. Charlson comorbidity index as a predictor of outcomes in incident peritoneal dialysis patients. Am. J. Kidney Dis. 2001, 37, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Kan, W.C.; Wang, J.J.; Wang, S.Y.; Sun, Y.M.; Hung, C.Y.; Chu, C.C.; Lu, C.L.; Weng, S.F.; Chio, C.C.; Chien, C.C. The new comorbidity index for predicting survival in elderly dialysis patients: A long-term population-based study. PLoS ONE 2013, 8, e68748. [Google Scholar] [CrossRef] [PubMed]
- Rigler, S.K.; Wetmore, J.B.; Mahnken, J.D.; Dong, L.; Ellerbeck, E.F.; Shireman, T.I. Impact of a modified data capture period on Liu comorbidity index scores in Medicare enrollees initiating chronic dialysis. BMC Nephrol. 2013, 14, 51. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Huang, Z.; Gilbertson, D.T.; Foley, R.N.; Collins, A.J. An improved comorbidity index for outcome analyses among dialysis patients. Kidney Int. 2010, 77, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Fernandez Lucas, M.; Teruel, J.L.; Zamora, J.; Lopez Mateos, M.; Rivera, M.; Ortuno, J. A Mediterranean age-comorbidity prognostic index for survival in dialysis populations. J. Nephrol. 2007, 20, 696–702. [Google Scholar] [PubMed]
- Li, P.K.; Chow, K.M.; Van de Luijtgaarden, M.W.; Johnson, D.W.; Jager, K.J.; Mehrotra, R.; Naicker, S.; Pecoits-Filho, R.; Yu, X.Q.; Lameire, N. Changes in the worldwide epidemiology of peritoneal dialysis. Nat. Rev. Nephrol. 2017, 13, 90–103. [Google Scholar] [CrossRef] [PubMed]
- Davies, S.J. Peritoneal dialysis—Current status and future challenges. Nat. Rev. Nephrol. 2013, 9, 399–408. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.K.; Blake, P.; Cordy, P.; Garg, A.X. Global trends in rates of peritoneal dialysis. J. Am. Soc. Nephrol. 2012, 23, 533–544. [Google Scholar] [CrossRef] [PubMed]
- Wauters, J.P.; Uehlinger, D. Non-medical factors influencing peritoneal dialysis utilization: The Swiss experience. Nephrol. Dial. Transpl. 2004, 19, 1363–1367. [Google Scholar] [CrossRef] [PubMed]
- Burnier, M.; Martin, P.Y. Dialyse à domicile: Retour vers le future. Rev. Med. Suisse 2017, 13, 443–444. [Google Scholar] [PubMed]
- Marinangeli, G.; Neri, L.; Viglino, G.; Rocca, A.R.; Laudon, A.; Ragusa, A.; Cabiddu, G.; Peritoneal Dialysis Study Group of Italian Society of Nephrology. PD in Italy: The 5th GSDP-SIN Census 2014. G. Ital. Nefrol. 2018, 35. [Google Scholar]
- Karopadi, A.N.; Mason, G.; Rettore, E.; Ronco, C. Cost of peritoneal dialysis and haemodialysis across the world. Nephrol. Dial. Transpl. 2013, 28, 2553–2569. [Google Scholar] [CrossRef] [PubMed]
- Machowska, A.; Rutherford, P. Peritoneal dialysis use within the context of the population and healthcare systems of Europe - differences, trends and future challenges. Int. J. Artif. Organs 2016, 39, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.; Kafle, M.; Sud, K.; Lee, V. Predictors and outcomes of patients switching from maintenance hemodialysis to peritoneal dialysis in Australia and New Zealand—Strengthening the argument for “Peritoneal Dialysis First” policy. Nephrology 2018. [Google Scholar] [CrossRef] [PubMed]
- Changsirikulchai, S.; Sriprach, S.; Thokanit, N.S.; Janma, J.; Chuengsaman, P.; Sirivongs, D. Survival Analysis and Associated Factors in Thai Patients on Peritoneal Dialysis Under the PD-First Policy. Perit. Dial. Int. 2018, 38, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H.; Hoshi, H.; Inoue, T.; Kikuta, T.; Tsuda, M.; Takenaka, T. New modality of dialysis therapy: Peritoneal dialysis first and transition to home hemodialysis. Adv. Perit. Dial. 2012, 28, 106–111. [Google Scholar] [PubMed]
- Walker, R.C.; Morton, R.L.; Tong, A.; Marshall, M.R.; Palmer, S.; Howard, K. Patient and caregiver preferences for home dialysis-the home first study: A protocol for qualitative interviews and discrete choice experiments. BMJ Open 2015, 5, e007405. [Google Scholar] [CrossRef] [PubMed]
- Benaroia, M.; Mendelssohn, D.C. The home dialysis first paradigm: Suitability and transitioning. Int. Urol. Nephrol. 2010, 42, 715–717. [Google Scholar] [CrossRef] [PubMed]
- Link, D.K.; Saxena, R. The right patient, the right treatment, the right access and the right time. Adv. Chronic Kidney Dis. 2014, 21, 360–364. [Google Scholar] [CrossRef] [PubMed]
- Port, F.K.; Morgenstern, H.; Bieber, B.A.; Karaboyas, A.; McCullough, K.P.; Tentori, F.; Pisoni, R.L.; Robinson, B.M. Understanding associations of hemodialysis practices with clinical and patient-reported outcomes: Examples from the DOPPS. Nephrol. Dial. Transpl. 2017, 32, ii106–ii112. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.Y.; Kalantar-Zadeh, K.; Fouque, D.; Wee, P.T.; Kovesdy, C.P.; Price, S.R.; Kopple, J.D. Precision Medicine for Nutritional Management in End-Stage Kidney Disease and Transition to Dialysis. Semin. Nephrol. 2018, 38, 383–396. [Google Scholar] [CrossRef] [PubMed]
- Cabrera, V.J.; Hansson, J.; Kliger, A.S.; Finkelstein, F.O. Symptom Management of the Patient with CKD: The Role of Dialysis. Clin. J. Am. Soc. Nephrol. 2017, 12, 687–693. [Google Scholar] [CrossRef] [PubMed]
- Feely, M.A.; Swetz, K.M.; Zavaleta, K.; Thorsteinsdottir, B.; Albright, R.C.; Williams, A.W. Reengineering Dialysis: The Role of Palliative Medicine. J. Palliat. Med. 2016, 19, 652–655. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.A.; Collett, G.K.; Josland, E.A.; Foote, C.; Li, Q.; Brennan, F.P. CKD in elderly patients managed without dialysis: Survival, symptoms, and quality of life. Clin. J. Am. Soc. Nephrol. 2015, 10, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Combs, S.A.; Davison, S.N. Palliative and end-of-life care issues in chronic kidney disease. Curr. Opin. Support. Palliat. Care. 2015, 9, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Watnick, S. Financial and medico-legal implications of late-start dialysis: Understanding the present policies through a window of past performance. Semin. Dial. 2013, 26, 702–705. [Google Scholar] [CrossRef] [PubMed]
- Rosansky, S.J.; Cancarini, G.; Clark, W.F.; Eggers, P.; Germaine, M.; Glassock, R.; Goldfarb, D.S.; Harris, D.; Hwang, S.J.; Imperial, E.B.; et al. Dialysis initiation: what’s the rush? Semin. Dial. 2013, 26, 650–657. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.W.; Wong, M.G.; Cooper, B.A.; Branley, P.; Bulfone, L.; Collins, J.F.; Craig, J.C.; Fraenkel, M.B.; Harris, A.; Kesselhut, J.; et al. Effect of timing of dialysis commencement on clinical outcomes of patients with planned initiation of peritoneal dialysis in the IDEAL trial. Perit. Dial. Int. 2012, 32, 595–604. [Google Scholar] [CrossRef] [PubMed]
- Cooper, B.A.; Branley, P.; Bulfone, L.; Collins, J.F.; Craig, J.C.; Fraenkel, M.B.; Harris, A.; Johnson, D.W.; Kesselhut, J.; Li, J.J.; et al. A randomized, controlled trial of early versus late initiation of dialysis. N. Engl. J. Med. 2010, 363, 609–619. [Google Scholar] [CrossRef] [PubMed]
- Tattersall, J.; Farrington, K.; Gentile, G.; Kooman, J.; Macias Núñez, J.F.; Nistor, I.; Van Biesen, W.; Covic, A.; European Renal Best Practice Guidelines Group and the European Union of Geriatric Medicine Societies (EUGMS) Collaborative Group for the Production of Guidelines on the Management of Older Patients with CKD. Is Kt/V useful in elderly dialysis patients? Pro and Con arguments. Nephrol. Dial. Transpl. 2018, 33, 742–750. [Google Scholar] [CrossRef] [PubMed]
- Tattersall, J. Hemodialysis Time and Kt/V: Less May Be Better. Semin. Dial. 2017, 30, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Raj, D.S.; Charra, B.; Pierratos, A.; Work, J. In search of ideal hemodialysis: Is prolonged frequent dialysis the answer? Am. J. Kidney Dis. 1999, 34, 597–610. [Google Scholar] [CrossRef]
- Macías, N.; Vega, A.; Abad, S.; Santos, A.; Cedeño, S.; Linares, T.; García-Prieto, A.M.; Aragoncillo, I.; Yuste, C.; López-Gómez, J.M. Is High-Volume Online Hemodiafiltration Associated with Malnutrition? Ther. Apher. Dial. 2017, 21, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Sirich, T.L.; Fong, K.; Larive, B.; Beck, G.J.; Chertow, G.M.; Levin, N.W.; Kliger, A.S.; Plummer, N.S.; Meyer, T.W.; Frequent Hemodialysis Network (FHN) Trial Group. Limited reduction in uremic solute concentrations with increased dialysis frequency and time in the Frequent Hemodialysis Network Daily Trial. Kidney Int. 2017, 91, 1186–1192. [Google Scholar] [CrossRef] [PubMed]
- Vega, A.; Sequí, M.J.; Abad, S.; Yuste, C.; Santos, A.; Macías, N.; López-Gómez, J.M. Daily Home Hemodialysis Is an Available Option for Renal Replacement Therapy in Spain. Ther. Apher. Dial. 2016, 20, 408–412. [Google Scholar] [CrossRef] [PubMed]
- Kraus, M.A.; Fluck, R.J.; Weinhandl, E.D.; Kansal, S.; Copland, M.; Komenda, P.; Finkelstein, F.O. Intensive Hemodialysis and Health-Related Quality of Life. Am. J. Kidney Dis. 2016, 68, S33–S42. [Google Scholar] [CrossRef] [PubMed]
- Tangren, J.; Nadel, M.; Hladunewich, M.A. Pregnancy and End-Stage Renal Disease. Blood Purif. 2018, 45, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Minelli, F.; Versino, E.; Cabiddu, G.; Attini, R.; Vigotti, F.N.; Rolfo, A.; Giuffrida, D.; Colombi, N.; Pani, A.; et al. Pregnancy in dialysis patients in the new millennium: A systematic review and meta-regression analysis correlating dialysis schedules and pregnancy outcomes. Nephrol. Dial. Transpl. 2016, 31, 1915–1934. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Grassi, G.; Mezza, E.; Gai, M.; Iacuzzo, C.; Bechis, F.; Biancone, L.; Jeantet, A.; Dani, F.; Perin, P.C.; et al. Early referral of Type 2 diabetic patients: Are we ready for the assault? Nephrol. Dial. Transpl. 2002, 17, 1241–1247. [Google Scholar] [CrossRef]
- Hahn, D.; Hodson, E.M.; Fouque, D. Low protein diets for non-diabetic adults with chronic kidney disease. Cochrane Database Syst. Rev. 2018, 10, CD001892. [Google Scholar] [CrossRef] [PubMed]
- Bellizzi, V.; Calella, P.; Carrero, J.J.; Fouque, D. Very low-protein diet to postpone renal failure: Pathophysiology and clinical applications in chronic kidney disease. Chronic Dis. Transl. Med. 2018, 4, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Kalantar-Zadeh, K.; Fouque, D. Nutritional Management of Chronic Kidney Disease. N. Engl. J. Med. 2017, 377, 1765–1776. [Google Scholar] [CrossRef] [PubMed]
- Garneata, L.; Stancu, A.; Dragomir, D.; Stefan, G.; Mircescu, G. Ketoanalogue-Supplemented Vegetarian Very Low-Protein Diet and CKD Progression. J. Am. Soc. Nephrol. 2016, 27, 2164–2176. [Google Scholar] [CrossRef] [PubMed]
- Piccoli, G.B.; Nazha, M.; Capizzi, I.; Vigotti, F.N.; Mongilardi, E.; Bilocati, M.; Avagnina, P.; Versino, E. Patient Survival and Costs on Moderately Restricted Low-Protein Diets in Advanced CKD: Equivalent Survival at Lower Costs? Nutrients 2016, 8, 758. [Google Scholar] [CrossRef] [PubMed]




© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piccoli, G.B.; Cabiddu, G.; Breuer, C.; Jadeau, C.; Testa, A.; Brunori, G. Dialysis Reimbursement: What Impact Do Different Models Have on Clinical Choices? J. Clin. Med. 2019, 8, 276. https://doi.org/10.3390/jcm8020276
Piccoli GB, Cabiddu G, Breuer C, Jadeau C, Testa A, Brunori G. Dialysis Reimbursement: What Impact Do Different Models Have on Clinical Choices? Journal of Clinical Medicine. 2019; 8(2):276. https://doi.org/10.3390/jcm8020276
Chicago/Turabian StylePiccoli, Giorgina Barbara, Gianfranca Cabiddu, Conrad Breuer, Christelle Jadeau, Angelo Testa, and Giuliano Brunori. 2019. "Dialysis Reimbursement: What Impact Do Different Models Have on Clinical Choices?" Journal of Clinical Medicine 8, no. 2: 276. https://doi.org/10.3390/jcm8020276
APA StylePiccoli, G. B., Cabiddu, G., Breuer, C., Jadeau, C., Testa, A., & Brunori, G. (2019). Dialysis Reimbursement: What Impact Do Different Models Have on Clinical Choices? Journal of Clinical Medicine, 8(2), 276. https://doi.org/10.3390/jcm8020276