Family and School Contexts as Predictors of Suicidal Behavior among Adolescents: The Role of Depression and Anxiety

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Measures
2.1.1. Suicidal Behavior
2.1.2. Depression
2.1.3. Anxiety
2.1.4. Family Function
2.1.5. School Climate
2.2. Procedure
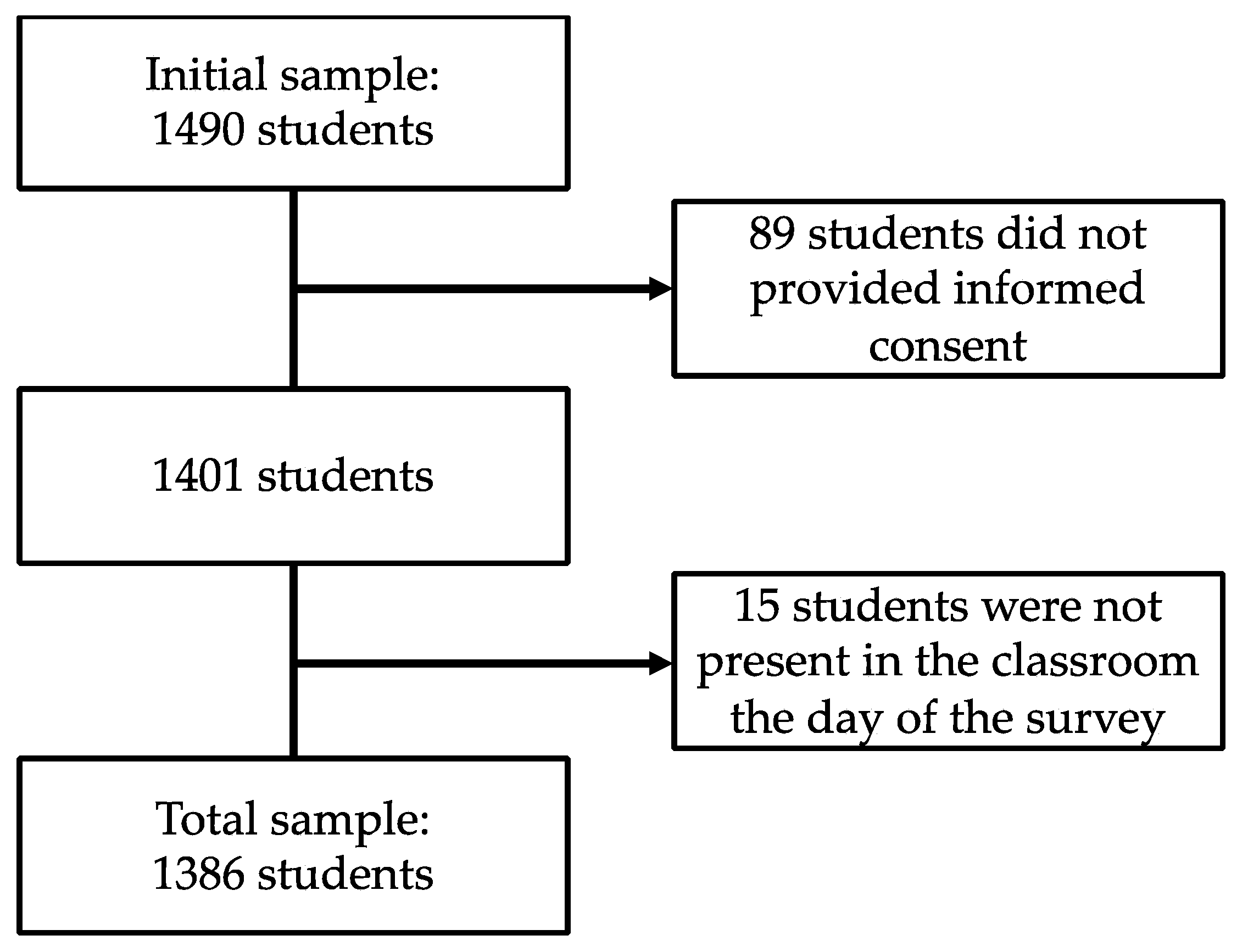
Participants Recruitment
2.3. Statistical Analyses
3. Results
3.1. Characterization of Suicide Behavior in the Study Sample
3.2. Relationships between Family Function, School Climate, Depression, Anxiety, and Suicidal Behavior
3.3. Predictive Value of Family Function and School Climate for Suicidal Behavior
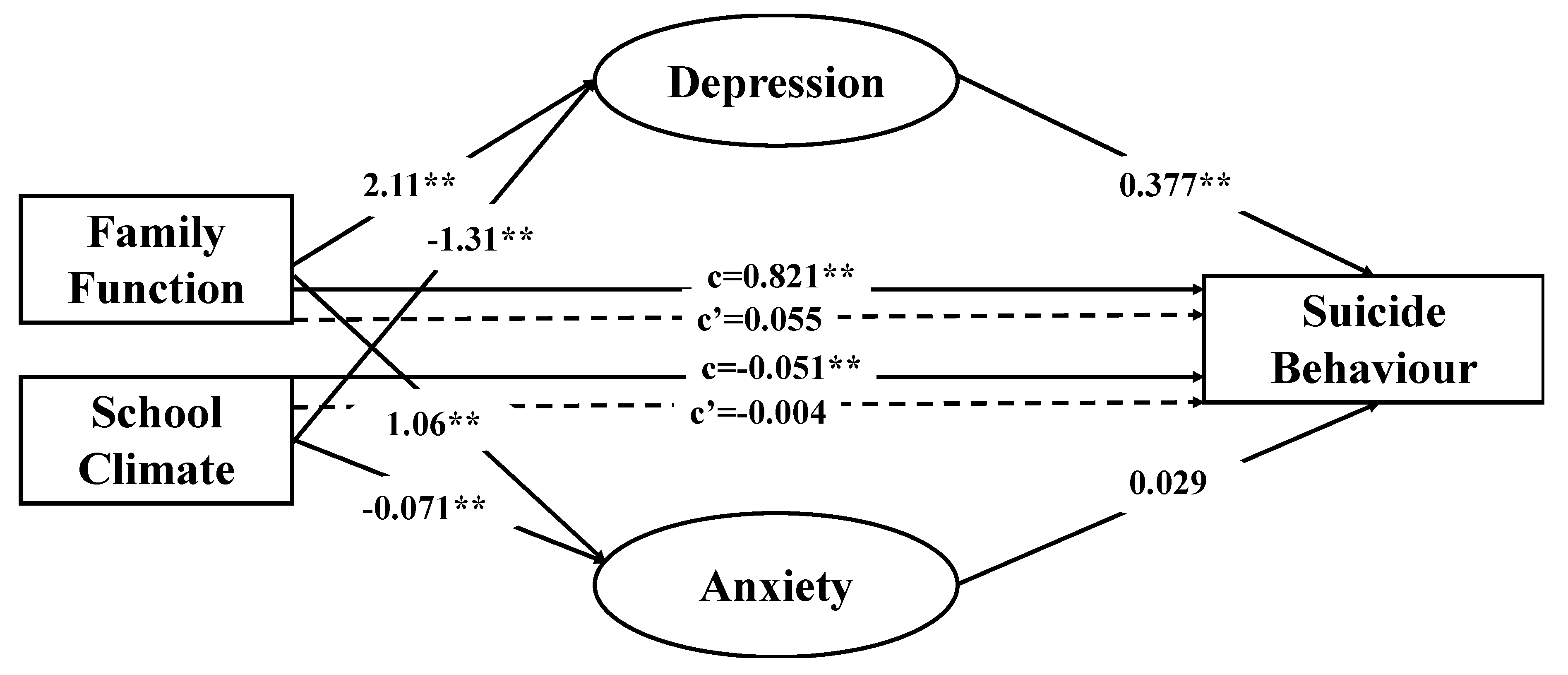
3.4. Multiple Mediating Effects of Depression and Anxiety on the Relationship of Family Function and School Climate with Suicidal Behavior
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Picazo-Zappino, J. Suicide among children and adolescents: A review. Actas Esp. Psiquiatr. 2014, 42, 125–132. [Google Scholar] [PubMed]
- Navarro-Gómez, N. El suicidio en jóvenes en España: Cifras y posibles causas. Análisis de los últimos datos disponibles. Clínica y Salud 2017, 28, 25–31. [Google Scholar]
- McLoughlin, A.B.; Gould, M.S.; Malone, K.M. Global trends in teenage suicide: 2003–2014. QJM 2015, 108, 765–780. [Google Scholar] [CrossRef] [PubMed]
- Fonseca-Pedrero, E.; Inchausti, F.; Pérez-Gutiérrez, L.; Aritio Solana, R.; Ortuño-Sierra, J.; Sánchez-García, M.Á.; Lucas-Molina, B.; Domínguez, C.; Foncea, D.; Espinosa, V.; et al. Ideación suicida en una muestra representativa de adolescentes españoles. Rev. de Psiquiatr. y Salud Ment. 2018, 11, 76–85. [Google Scholar] [CrossRef]
- La Salle, T.P.; Wang, C.; Parris, L.; Brown, J.A. Associations between school climate, suicidal thoughts, and behaviors and ethnicity among middle school students. Psychol. Sch. 2017, 54, 1294–1301. [Google Scholar] [CrossRef]
- Lee, M.T.Y.; Wong, B.P.; Chow, B.W.Y.; McBride-Chang, C. Predictors of suicide ideation and depression in Hong Kong adolescents: Perceptions of academic and family climates. Suicide Life Threat. Behav. 2006, 36, 82–96. [Google Scholar] [CrossRef]
- Hatzenbuehler, M.L.; Birkett, M.; Van Wagenen, A.; Meyer, I.H. Protective School Climates and Reduced Risk for Suicide Ideation in Sexual Minority Youths. Am. J. Public Health 2013, 104, 279–286. [Google Scholar] [CrossRef]
- Li, D.; Bao, Z.; Li, X.; Wang, Y. Perceived School Climate and Chinese Adolescents’ Suicidal Ideation and Suicide Attempts: The Mediating Role of Sleep Quality. J. Sch. Health 2016, 86, 75–83. [Google Scholar] [CrossRef]
- Consoli, A.; Peyre, H.; Speranza, M.; Hassler, C.; Falissard, B.; Touchette, E.; Cohen, D.; Moro, M.-R.; Révah-Lévy, A. Suicidal behaviors in depressed adolescents: Role of perceived relationships in the family. Child Adolesc. Psychiatry Ment. Health 2013, 7, 8. [Google Scholar] [CrossRef]
- Lipschitz, J.M.; Yen, S.; Weinstock, L.M.; Spirito, A. Adolescent and caregiver perception of family functioning: Relation to suicide ideation and attempts. Psychiatry Res. 2012, 200, 400–403. [Google Scholar] [CrossRef]
- Winek, J.L. Systemic Family Therapy: From Theory to Practice; SAGE: California, CA, USA, 2009; ISBN 978-1-4129-3696-5. [Google Scholar]
- Palmer, E.; Welsh, P.; Tiffin, P.A. Perceptions of family functioning in adolescents who self-harm. J. Fam. Ther. 2016, 38, 257–273. [Google Scholar] [CrossRef]
- Brent, D.A. Risk factors for adolescent suicide and suicidal behavior: Mental and substance abuse disorders, family environmental factors, and life stress. Suicide Life Threat. Behav. 1995, 25, 52–63. [Google Scholar] [CrossRef] [PubMed]
- King, C.A.; Merchant, C.R. Social and Interpersonal Factors Relating to Adolescent Suicidality: A Review of the Literature. Arch. Suicide Res. 2008, 12, 181–196. [Google Scholar] [CrossRef] [PubMed]
- Sheftall, A.H.; Mathias, C.W.; Furr, R.M.; Dougherty, D.M. Adolescent attachment security, family functioning, and suicide attempts. Attach. Hum. Dev. 2013, 15, 368–383. [Google Scholar] [CrossRef]
- Marraccini, M.E.; Brier, Z.M.F. School connectedness and suicidal thoughts and behaviors: A systematic meta-analysis. Sch. Psychol. Q. 2017, 32, 5–21. [Google Scholar] [CrossRef]
- Wang, M.-T.; Degol, J.L. School Climate: A Review of the Construct, Measurement, and Impact on Student Outcomes. Educ. Psychol. Rev. 2016, 28, 315–352. [Google Scholar] [CrossRef]
- Côté-Lussier, C.; Fitzpatrick, C. Feelings of Safety at School, Socioemotional Functioning, and Classroom Engagement. J. Adolesc. Health 2016, 58, 543–550. [Google Scholar] [CrossRef]
- Kidger, J.; Araya, R.; Donovan, J.; Gunnell, D. The effect of the school environment on the emotional health of adolescents: A systematic review. Pediatrics 2012, 129, 925–949. [Google Scholar] [CrossRef]
- Bosworth, K. (Ed.) Prevention Science in School Settings: Complex Relationships and Processes; Springer: New York, NY, USA, 2015; ISBN 978-1-4939-3154-5. [Google Scholar]
- Kuramoto-Crawford, S.J.; Ali, M.M.; Wilcox, H.C. Parent–Child Connectedness and Long-Term Risk for Suicidal Ideation in a Nationally Representative Sample of US Adolescents. Crisis 2016, 38, 309–318. [Google Scholar] [CrossRef]
- Stewart, S.M.; Eaddy, M.; Horton, S.E.; Hughes, J.; Kennard, B. The Validity of the Interpersonal Theory of Suicide in Adolescence: A Review. J. Clin. Child Adolesc. Psychol. 2017, 46, 437–449. [Google Scholar] [CrossRef]
- Maslow, G.R.; Dunlap, K.; Chung, R.J. Depression and Suicide in Children and Adolescents. Pediatr. Rev. 2015, 36, 299–308. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hill, R.M.; Castellanos, D.; Pettit, J.W. Suicide-related behaviors and anxiety in children and adolescents: A review. Clin. Psychol. Rev. 2011, 31, 1133–1144. [Google Scholar] [CrossRef] [PubMed]
- Osman, A.; Bagge, C.L.; Gutierrez, P.M.; Konick, L.C.; Kopper, B.A.; Barrios, F.X. The Suicidal Behaviors Questionnaire-Revised (SBQ-R): Validation with clinical and nonclinical samples. Assessment 2001, 8, 443–454. [Google Scholar] [CrossRef] [PubMed]
- Wulsin, L.; Somoza, E.; Heck, J. The Feasibility of Using the Spanish PHQ-9 to Screen for Depression in Primary Care in Honduras. Prim. Care Companion J. Clin Psychiatry 2002, 4, 191–195. [Google Scholar] [CrossRef] [PubMed]
- Diez-Quevedo, C.; Rangil, T.; Sanchez-Planell, L.; Kroenke, K.; Spitzer, R.L. Validation and utility of the patient health questionnaire in diagnosing mental disorders in 1003 general hospital Spanish inpatients. Psychosom. Med. 2001, 63, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B. Validation and utility of a self-report version of PRIME-MD: The PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA 1999, 282, 1737–1744. [Google Scholar] [CrossRef]
- García-Campayo, J.; Zamorano, E.; Ruiz, M.A.; Pardo, A.; Pérez-Páramo, M.; López-Gómez, V.; Freire, O.; Rejas, J. Cultural adaptation into Spanish of the generalized anxiety disorder-7 (GAD-7) scale as a screening tool. Health Qual Life Outcomes 2010, 8, 8. [Google Scholar] [CrossRef]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Stratton, P.; Lask, J.; Bland, J.; Nowotny, E.; Evans, C.; Singh, R.; Janes, E.; Peppiatt, A. Detecting therapeutic improvement early in therapy: Validation of the SCORE-15 index of family functioning and change. J. Fam. Ther. 2014, 36, 3–19. [Google Scholar] [CrossRef]
- Rivas, G.; Pereira, R. Score 15: Escala de Evaluación Familiar en Español. Available online: https://www.featf.org/score-15/ (accessed on 17 September 2019).
- Díaz-Aguado, M.J.; Martínez, R.; Martín, J. Estudio Estatal Sobre la Convivencia Escolar en la Educación Secundaria Obligatoria; Ministerio de Educación: Madrid, Spain, 2010.
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process. Analysis, Second Edition: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2017; ISBN 978-1-4625-3466-1. [Google Scholar]
- Miranda, R.; Ortin, A.; Scott, M.; Shaffer, D. Characteristics of suicidal ideation that predict the transition to future suicide attempts in adolescents. J. Child Psychol. Psychiatry 2014, 55, 1288–1296. [Google Scholar] [CrossRef]
- Miranda-Mendizabal, A.; Castellví, P.; Parés-Badell, O.; Alayo, I.; Almenara, J.; Alonso, I.; Blasco, M.J.; Cebrià, A.; Gabilondo, A.; Gili, M.; et al. Gender differences in suicidal behavior in adolescents and young adults: Systematic review and meta-analysis of longitudinal studies. Int. J. Public Health 2019, 64, 265–283. [Google Scholar] [CrossRef] [PubMed]
- Van Orden, K.A.; Witte, T.K.; Cukrowicz, K.C.; Braithwaite, S.; Selby, E.A.; Joiner, T.E. The Interpersonal Theory of Suicide. Psychol. Rev. 2010, 117, 575–600. [Google Scholar] [CrossRef] [PubMed]
- Shim-Pelayo, H.; De Pedro, K.T. The role of school climate in rates of depression and suicidal ideation among school-attending foster youth in California public schools. Child. Youth Serv. Rev. 2018, 88, 149–155. [Google Scholar] [CrossRef]
- Thapa, A.; Cohen, J.; Guffey, S.; Higgins-D’Alessandro, A. A Review of School Climate Research. Rev. Educ. Res. 2013, 83, 357–385. [Google Scholar] [CrossRef]
- Barzilay, S.; Feldman, D.; Snir, A.; Apter, A.; Carli, V.; Hoven, C.W.; Wasserman, C.; Sarchiapone, M.; Wasserman, D. The interpersonal theory of suicide and adolescent suicidal behavior. J. Affect. Disord. 2015, 183, 68–74. [Google Scholar] [CrossRef]
- Jellinek, M.S.; Snyder, J.B. Depression and suicide in children and adolescents. Pediatr. Rev. 1998, 19, 255–264. [Google Scholar] [CrossRef]
- Hawton, K.; Casañas, I.; Comabella, C.; Haw, C.; Saunders, K. Risk factors for suicide in individuals with depression: A systematic review. J. Affect. Disord. 2013, 147, 17–28. [Google Scholar] [CrossRef]
- Polanczyk, G.V.; Salum, G.A.; Sugaya, L.S.; Caye, A.; Rohde, L.A. Annual Research Review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J. Child Psychol. Psychiatry 2015, 56, 345–365. [Google Scholar] [CrossRef]
- Boden, J.M.; Fergusson, D.M.; Horwood, L.J. Anxiety disorders and suicidal behaviours in adolescence and young adulthood: Findings from a longitudinal study. Psychol. Med. 2007, 37, 431–440. [Google Scholar] [CrossRef]
- Kosky, R.; Silburn, S.; Zubrick, S.R. Are Children and Adolescents Who Have Suicidal Thoughts Different from Those Who Attempt Suicide? J. Nerv. Ment. Dis. 1990, 178, 38. [Google Scholar] [CrossRef]
- D’Eramo, K.S.; Prinstein, M.J.; Freeman, J.; Grapentine, W.L.; Spirito, A. Psychiatric diagnoses and comorbidity in relation to suicidal behavior among psychiatrically hospitalized adolescents. Child Psychiatry Hum. Dev. 2004, 35, 21–35. [Google Scholar] [CrossRef] [PubMed]
- Myers, K.; McCauley, E.; Calderon, R.; Mitchell, J.; Burke, P.; Schloredt, K. Risks for suicidality in major depressive disorder. J. Am. Acad. Child Adolesc. Psychiatry 1991, 30, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Beautrais, A.L. Suicide and serious suicide attempts in youth: A multiple-group comparison study. Am. J. Psychiatry 2003, 160, 1093–1099. [Google Scholar] [CrossRef] [PubMed]
- Apter, A.; Horesh, N.; Gothelf, D.; Zalsman, G.; Erlich, Z.; Soreni, N.; Weizman, A. Depression and suicidal behavior in adolescent inpatients with obsessive compulsive disorder. J. Affect. Disord. 2003, 75, 181–189. [Google Scholar] [CrossRef]
- Pawlak, C.; Pascual-Sanchez, T.; Raë, P.; Fischer, W.; Ladame, F. Anxiety disorders, comorbidity, and suicide attempts in adolescence: A preliminary investigation. Eur. Psychiatry 1999, 14, 132–136. [Google Scholar] [CrossRef]
- WHO Calls for Stronger Focus on Adolescent Health. Road traffic injuries, HIV/AIDS, suicide are top causes of death; depression is number 1 cause of illness and disability. Cent. Eur. J. Public Health 2014, 22, 139. [Google Scholar]



{kind=link}
{kind=link}
| Lifetime Suicide Ideation and/or Suicide Attempts | ||||||||
| Non-Suicidal Subgroup | Suicide Risk Ideation Subgroup | Suicide Plan Subgroup | Suicide Attempt Subgroup | |||||
| Total sample n = 1386 | 1149 (82.9%) | 114 (8.2%) | 72 (5.2%) | 51 (3.7%) | ||||
| Sex | Female n = 688 | 558 (81.1%) | 61 (8.9%) | 39 (5.7%) | 30 (4.4%) | |||
| Male n = 698 | 591 (84.7%) | 53 (7.6%) | 33 (4.7%) | 21 (3%) | ||||
| Age | 11–13 n = 666 | 556 (83.5%) | 57 (8.6%) | 35 (5.3%) | 18 (2.7%) | |||
| 14–19 n = 720 | 593 (82.4%) | 57 (7.9%) | 37 (5.1%) | 33 (4.6%) | ||||
| Frequency of Suicide Ideation over the Past 12 Months | ||||||||
| Never | Rarely (Once) | Sometimes (Twice) | Often (3-4 Times) | Very Often (5 or More Times) | ||||
| Total sample n = 1386 | 1203 (86.8%) | 90 (6.5%) | 36 (2.6%) | 30 (2.2%) | 27 (1.9%) | |||
| Sex | Female n = 688 | 587 (85.3%) | 49 (7.1%) | 18 (2.6%) | 15 (2.2%) | 19 (2.8%) | ||
| Male n = 698 | 616 (88.3%) | 41 (5.9%) | 18 (2.6%) | 15 (2.1%) | 8 (1.1%) | |||
| Age | 11–13 n = 666 | 585 (87.8%) | 40 (6%) | 17 (2.6%) | 13 (2%) | 11 (1.7%) | ||
| 14–19 n = 720 | 618 (85.8%) | 50 (6.9%) | 19 (2.6%) | 17 (2.4%) | 16 (2.2%) | |||
| Threat of Suicide Attempt | ||||||||
| No | Yes, on One Occasion | Yes, More Than Once | ||||||
| Total sample n = 1386 | 1242 (89.6%) | 71 (5.1%) | 73 (5.3%) | |||||
| Sex | Female n = 688 | 605 (87.9%) | 43 (6.3%) | 40 (5.8%) | ||||
| Male n = 698 | 637 (91.3%) | 28 (4%) | 33 (4.7%) | |||||
| Age | 11–13 n = 666 | 598 (89.8%) | 36 (5.4%) | 32 (4.8%) | ||||
| 14–19 n = 720 | 644 (89.4%) | 35 (4.9%) | 41 (5.7%) | |||||
| Self-Reported Likelihood of Suicidal Behavior in the Future | ||||||||
| Never | No Chance at all | Rather Unlikely | Unlikely | Likely | Rather Likely | Very Likely | ||
| Total sample n = 1386 | 1084 (78.2%) | 143 (10.3%) | 65 (4.7%) | 31 (2.2%) | 29 (2.1%) | 12 (0.9%) | 22 (1.6%) | |
| Sex | Female n = 688 | 522 (75.9%) | 75 (10.9%) | 34 (4.9%) | 17 (2.5%) | 19 (2.8%) | 8 (1.2%) | 13 (1.9%) |
| Male n = 698 | 562 (80.5%) | 68 (9.7%) | 31 (4.4%) | 14 (2%) | 10 (1.4%) | 4 (0.6%) | 9 (1.3%) | |
| Age | 11–13 n = 666 | 536 (80.5%) | 65 (9.8%) | 28 (4.2%) | 12 (1.8%) | 10 (1.5%) | 3 (0.5%) | 12 (1.8%) |
| 14–19 n = 720 | 548 (76.1%) | 78 (10.8%) | 37 (5.1%) | 19 (2.6%) | 19 (2.6%) | 9 (1.3%) | 10 (1.4%) | |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Family Function | 1.Strengths and Adaptability | - | 0.248 ** | 0.173 ** | 0.585 ** | −0.249 ** | −0.296 ** | −0.197 ** | −0.184 ** | −0.262 ** | −0.326 ** | 0.310 ** | 0.179 ** | 0.223 ** |
| 2.Overwhelmed by Difficulties | - | 0.649 ** | 0.846 ** | −0.209 ** | −0.252 ** | −0.241 ** | −0.142 ** | −0.265 ** | −0.299 ** | 0.293 ** | 0.152 ** | 0.167 ** | ||
| 3.Disrupted Communication | - | 0.833 ** | −0.200 ** | −0.172 ** | −0.196 ** | −0.088 ** | −0.200 ** | −0.237 ** | 0.196 ** | 0.109 ** | 0.106 ** | |||
| 4.Total Family Function | - | −0.285 ** | −0.309 ** | −0.277 ** | −0.176 ** | −0.315 ** | −0.373 ** | 0.345 ** | 0.189 ** | 0.211 ** | ||||
| School Climate | 5.Satisfaction | - | 0.428 ** | 0.467 ** | 0.532 ** | 0.568 ** | 0.865 ** | −0.265 ** | −0.171 ** | −0.146 ** | ||||
| 6.Sense of Belonging | - | 0.261 ** | 0.264 ** | 0.372 ** | 0.652 ** | −0.252 ** | −0.164 ** | −0.189 ** | ||||||
| 7.Integration | - | 0.566 ** | 0.412 ** | 0.656 ** | −0.326 ** | −0.214 ** | −0.229 ** | |||||||
| 8.Cooperation | - | 0.493 ** | 0.708 ** | −0.286 ** | −0.189 ** | −0.173 ** | ||||||||
| 9. Communication betweenFamily and School | - | 0.785 ** | −0.230 ** | −0.112 ** | −0.118 ** | |||||||||
| 10.Total School Climate | - | −0.352 ** | −0.218 ** | −0.216 ** | ||||||||||
| 11.Depression | - | 0.599 ** | 0.574 ** | |||||||||||
| 12.Anxiety | - | 0.316 | ||||||||||||
| 13.Suicide Behavior | - |
| Step 1 | Step 2 | Step 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|
| β | R2 | ΔR2 | β | R2 | ΔR2 | β | R2 | ΔR2 | |
| Age | 0.066 * | 0.022 | −0.006 | ||||||
| Sex | −0.061 * | −0.066 * | 0.001 | ||||||
| F(2,1379) = 5.313, p = 0.005 | 0.008 | 0.008 ** | |||||||
| Total Family Functioning | 0.157 ** | 0.010 | |||||||
| Total School Climate | −0.152 ** | −0.015 | |||||||
| F(4,1379) = 26.327, p = 0.0001 | 0.071 | 0.063 ** | |||||||
| Depression | 0.591 ** | ||||||||
| Anxiety | −0.042 | ||||||||
| F(6,1379) = 113.226, p = 0.0001 | 0.328 | 0.260 ** | |||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruiz-Robledillo, N.; Ferrer-Cascales, R.; Albaladejo-Blázquez, N.; Sánchez-SanSegundo, M. Family and School Contexts as Predictors of Suicidal Behavior among Adolescents: The Role of Depression and Anxiety. J. Clin. Med. 2019, 8, 2066. https://doi.org/10.3390/jcm8122066
Ruiz-Robledillo N, Ferrer-Cascales R, Albaladejo-Blázquez N, Sánchez-SanSegundo M. Family and School Contexts as Predictors of Suicidal Behavior among Adolescents: The Role of Depression and Anxiety. Journal of Clinical Medicine. 2019; 8(12):2066. https://doi.org/10.3390/jcm8122066
Chicago/Turabian StyleRuiz-Robledillo, Nicolás, Rosario Ferrer-Cascales, Natalia Albaladejo-Blázquez, and Miriam Sánchez-SanSegundo. 2019. "Family and School Contexts as Predictors of Suicidal Behavior among Adolescents: The Role of Depression and Anxiety" Journal of Clinical Medicine 8, no. 12: 2066. https://doi.org/10.3390/jcm8122066
APA StyleRuiz-Robledillo, N., Ferrer-Cascales, R., Albaladejo-Blázquez, N., & Sánchez-SanSegundo, M. (2019). Family and School Contexts as Predictors of Suicidal Behavior among Adolescents: The Role of Depression and Anxiety. Journal of Clinical Medicine, 8(12), 2066. https://doi.org/10.3390/jcm8122066