Prognostic Implication of Metastatic Lymph Node Ratio in Colorectal Cancers: Comparison Depending on Tumor Location



Abstract
1. Introduction
2. Materials and Methods
2.1. Patients and Evaluation of Pathological Features
2.2. Definition and Evaluation of Metastatic Lymph Node Ratio
2.3. Statistical Analysis
3. Results
3.1. Clinicopathological Significance of Lymph Node Metastasis in Colorectal Cancers
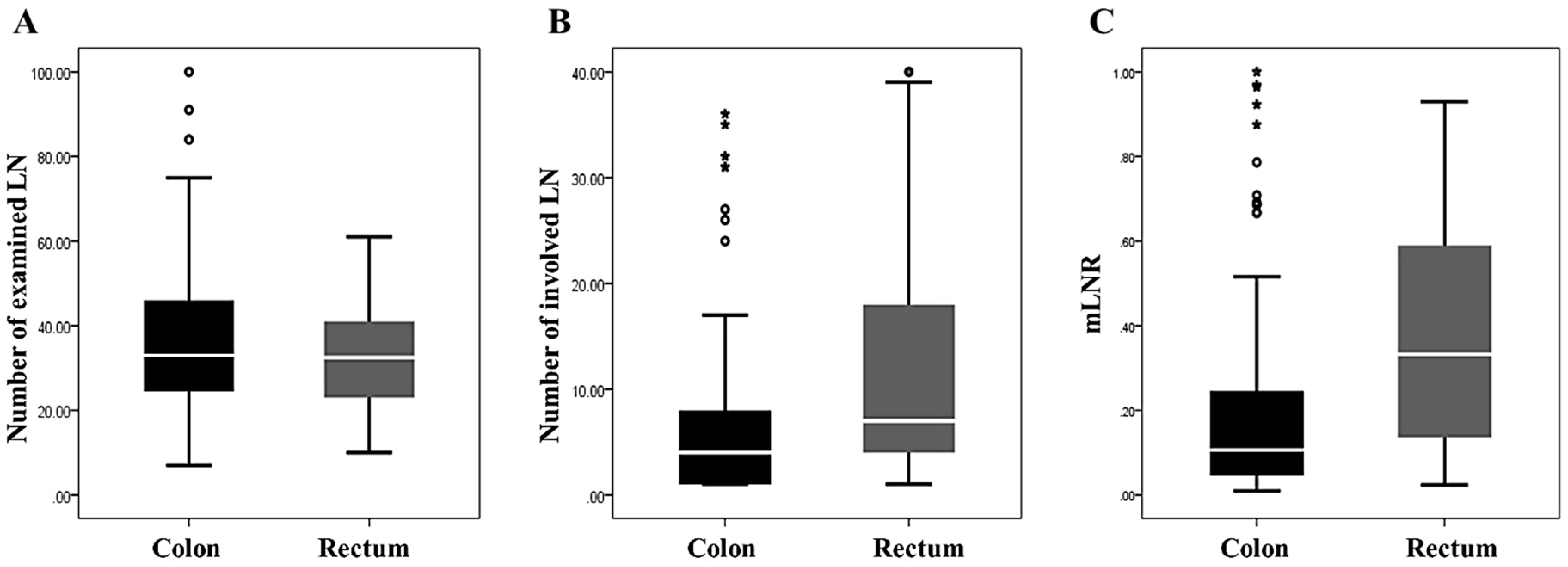
3.2. Characteristics of Nodal Status in Colorectal Cancers
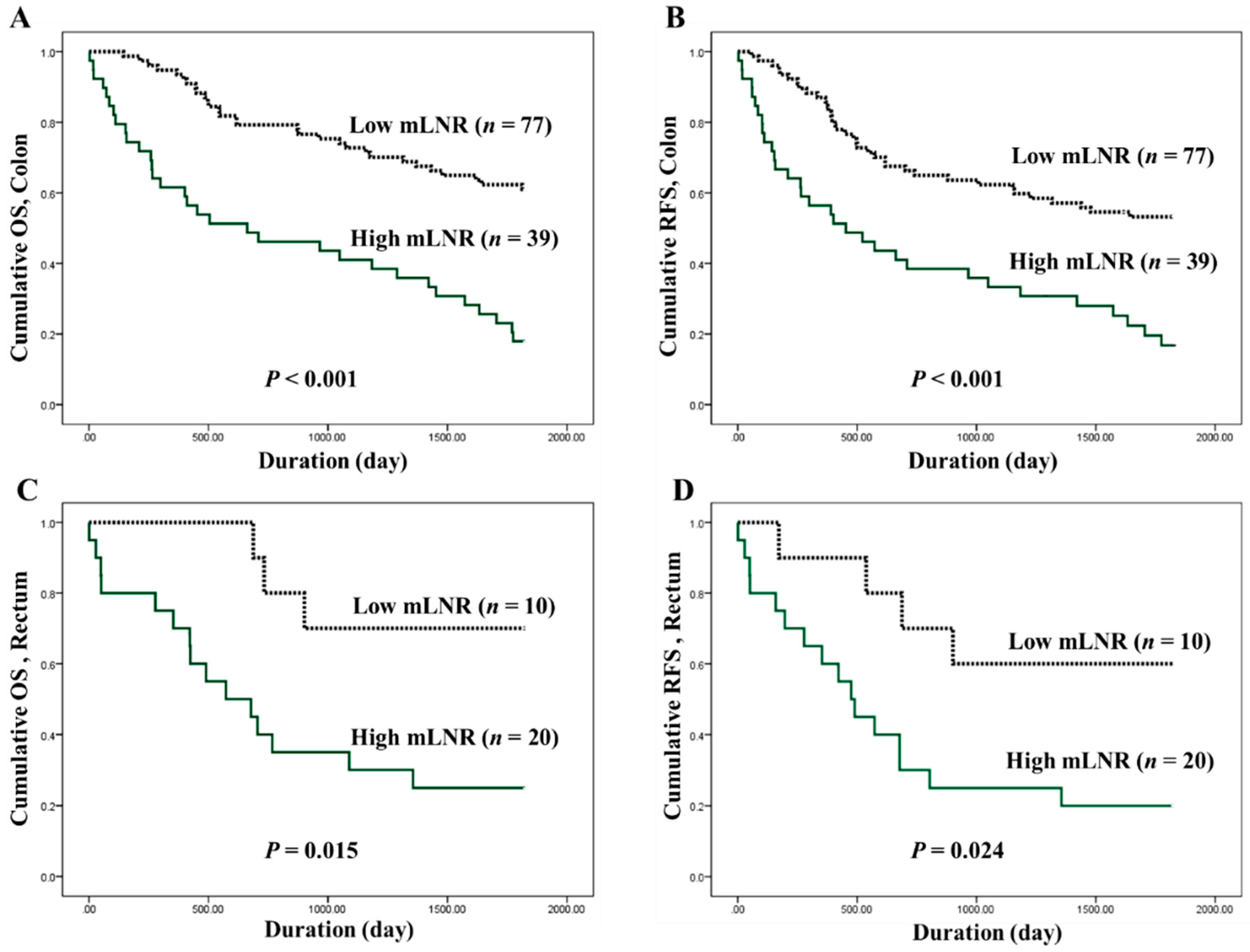
3.3. Correlation between High Metastatic Lymph Node Ratio and Survival Rates in Colorectal Cancers
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Byrd, D.R. The Eighth Edition AJCC Cancer Staging Manual; Springer: New York, NY, USA, 2016. [Google Scholar]
- Märkl, B.; Olbrich, G.; Schenkirsch, G.; Kretsinger, H.; Kriening, B.; Anthuber, M. Clinical Significance of International Union Against Cancer pN Staging and Lymph Node Ratio in Node-Positive Colorectal Cancer after Advanced Lymph Node Dissection. Dis. Colon Rectum 2016, 59, 386–395. [Google Scholar] [CrossRef] [PubMed]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Cederquist, L.; Chen, Y.J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Engstrom, P.F.; et al. NCCN Guidelines Insights: Colon Cancer, Version 2.2018. J. Natl. Compr. Cancer Netw. 2018, 16, 359–369. [Google Scholar] [CrossRef] [PubMed]
- Baxter, N.N.; Virnig, D.J.; Rothenberger, D.A.; Morris, A.M.; Jessurun, J.; Virnig, B.A. Lymph node evaluation in colorectal cancer patients: A population-based study. J. Natl. Cancer Inst. 2005, 97, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Chang, G.J.; Rodriguez-Bigas, M.A.; Skibber, J.M.; Moyer, V.A. Lymph node evaluation and survival after curative resection of colon cancer: Systematic review. J. Natl. Cancer Inst. 2007, 99, 433–441. [Google Scholar] [CrossRef]
- Le Voyer, T.E.; Sigurdson, E.R.; Hanlon, A.L.; Mayer, R.J.; Macdonald, J.S.; Catalano, P.J.; Haller, D.G. Colon cancer survival is associated with increasing number of lymph nodes analyzed: A secondary survey of intergroup trial INT-0089. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2003, 21, 2912–2919. [Google Scholar] [CrossRef]
- Kim, M.J.; Jeong, S.Y.; Choi, S.J.; Ryoo, S.B.; Park, J.W.; Park, K.J.; Oh, J.H.; Kang, S.B.; Park, H.C.; Heo, S.C.; et al. Survival paradox between stage IIB/C (T4N0) and stage IIIA (T1-2N1) colon cancer. Ann. Surg. Oncol. 2015, 22, 505–512. [Google Scholar] [CrossRef]
- Rodriguez Santiago, J.M.; Munoz, E.; Marti, M.; Quintana, S.; Veloso, E.; Marco, C. Metastatic lymph node ratio as a prognostic factor in gastric cancer. Eur. J. Surg. Oncol. 2005, 31, 59–66. [Google Scholar] [CrossRef]
- Bando, E.; Yonemura, Y.; Taniguchi, K.; Fushida, S.; Fujimura, T.; Miwa, K. Outcome of ratio of lymph node metastasis in gastric carcinoma. Ann. Surg. Oncol. 2002, 9, 775–784. [Google Scholar] [CrossRef]
- Bilici, A.; Selcukbiricik, F.; Seker, M.; Oven, B.B.; Olmez, O.F.; Yildiz, O.; Olmuscelik, O.; Hamdard, J.; Acikgoz, O.; Cakir, A.; et al. Prognostic Significance of Metastatic Lymph Node Ratio in Patients with pN3 Gastric Cancer Who Underwent Curative Gastrectomy. Oncol. Res. Treat. 2019, 42, 209–216. [Google Scholar] [CrossRef]
- Berger, A.C.; Watson, J.C.; Ross, E.A.; Hoffman, J.P. The metastatic/examined lymph node ratio is an important prognostic factor after pancreaticoduodenectomy for pancreatic adenocarcinoma. Am. Surg. 2004, 70, 235–240, discussion 240. [Google Scholar]
- van der Wal, B.C.; Butzelaar, R.M.; van der Meij, S.; Boermeester, M.A. Axillary lymph node ratio and total number of removed lymph nodes: Predictors of survival in stage I and II breast cancer. Eur. J. Surg. Oncol. 2002, 28, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Pyo, J.S.; Sohn, J.H.; Chang, K. Prognostic Role of Metastatic Lymph Node Ratio in Papillary Thyroid Carcinoma. J. Pathol. Transl. Med. 2018, 52, 331–338. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Liu, W.; Cheng, Y. Prognostic significance of metastatic lymph node ratio in squamous cell carcinoma of the cervix. Oncotargets Ther. 2016, 9, 3791–3797. [Google Scholar] [CrossRef]
- Lei, B.W.; Hu, J.Q.; Yu, P.C.; Wang, Y.L.; Wei, W.J.; Zhu, J.; Shi, X.; Qu, N.; Lu, Z.W.; Ji, Q.H. Lymph node ratio (LNR) as a complementary staging system to TNM staging in salivary gland cancer. Eur. Arch. Oto-Rhino-Laryngol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Berger, A.C.; Sigurdson, E.R.; LeVoyer, T.; Hanlon, A.; Mayer, R.J.; Macdonald, J.S.; Catalano, P.J.; Haller, D.G. Colon cancer survival is associated with decreasing ratio of metastatic to examined lymph nodes. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2005, 23, 8706–8712. [Google Scholar] [CrossRef] [PubMed]
- Dedavid e Silva, T.L.; Damin, D.C. Lymph node ratio predicts tumor recurrence in stage III colon cancer. Rev. Col. Bras. Cir. 2013, 40, 463–470. [Google Scholar] [PubMed]
- Greenberg, R.; Itah, R.; Ghinea, R.; Sacham-Shmueli, E.; Inbar, R.; Avital, S. Metastatic lymph node ratio (LNR) as a prognostic variable in colorectal cancer patients undergoing laparoscopic resection. Tech. Coloproctol. 2011, 15, 273–279. [Google Scholar] [CrossRef]
- Leonard, D.; Remue, C.; Abbes Orabi, N.; van Maanen, A.; Danse, E.; Dragean, A.; Debetancourt, D.; Humblet, Y.; Jouret-Mourin, A.; Maddalena, F.; et al. Lymph node ratio and surgical quality are strong prognostic factors of rectal cancer: Results from a single referral centre. Colorectal Dis. Off. J. Assoc. Coloproctol. Great Br. Irel. 2016, 18, O175–O184. [Google Scholar] [CrossRef]
- Lu, Y.J.; Lin, P.C.; Lin, C.C.; Wang, H.S.; Yang, S.H.; Jiang, J.K.; Lan, Y.T.; Lin, T.C.; Liang, W.Y.; Chen, W.S.; et al. The impact of the lymph node ratio is greater than traditional lymph node status in stage III colorectal cancer patients. World J. Surg. 2013, 37, 1927–1933. [Google Scholar] [CrossRef]
- Park, I.J.; Yu, C.S.; Lim, S.B.; Yoon, Y.S.; Kim, C.W.; Kim, T.W.; Kim, J.H.; Kim, J.C. Ratio of metastatic lymph nodes is more important for rectal cancer patients treated with preoperative chemoradiotherapy. World J. Gastroenterol. 2015, 21, 3274–3281. [Google Scholar] [CrossRef]
- Ramos-Esquivel, A.; Juarez, M.; Gonzalez, I.; Porras, J.; Rodriguez, L. Prognosis impact of the lymph node ratio in patients with colon adenocarcinoma: A single-centre experience. J. Gastrointest. Cancer 2014, 45, 133–136. [Google Scholar] [CrossRef] [PubMed]
- Rao, A.; Dadras, M.; Razzak, M.A.; Ahmad, K.; Vijayasekar, C. Effect of Lymph Node Retrieval and Ratio on the Long-Term Survival and Recurrence of Colon Cancer. J. Coll. Physicians Surg. Pak. 2016, 26, 467–470. [Google Scholar] [PubMed]
- Pyo, J.S.; Kim, J.H.; Lee, S.Y.; Baek, T.H.; Kang, D.W. Metastatic Lymph Node Ratio (mLNR) is a Useful Parameter in the Prognosis of Colorectal Cancer; A Meta-Analysis for the Prognostic Role of mLNR. Medicina 2019, 55, 673. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.; Wang, F.; Guo, G.; Dong, J.; Liu, S.; He, W.; Zhang, B.; Xia, L. Metastatic lymph node ratio as a prognostic indicator in patients with stage IV colon cancer undergoing resection. J. Cancer 2019, 10, 2534–2540. [Google Scholar] [CrossRef]
- Lv, Y.; Feng, Q.Y.; Lin, S.B.; Mao, Y.H.; Xu, Y.Q.; Zheng, P.; Yang, L.L.; He, G.D.; Xu, J.M. Exploration of exact significance of lymph node ratio and construction of a novel stage in colon cancer with no distant metastasis. Cancer Manag. Res. 2019, 11, 6841–6854. [Google Scholar] [CrossRef]
- Elsamany, S.A.; Alzahrani, A.S.; Mohamed, M.M.; Elmorsy, S.A.; Zekri, J.E.; Al-Shehri, A.S.; Haggag, R.M.; Alnagar, A.A.; El Taani, H.A. Clinico-pathological patterns and survival outcome of colorectal cancer in young patients: Western Saudi Arabia experience. Asian Pac. J. Cancer Prev. 2014, 15, 5239–5243. [Google Scholar] [CrossRef]
- Hong, K.D.; Lee, S.I.; Moon, H.Y. Lymph node ratio as determined by the 7th edition of the American Joint Committee on Cancer staging system predicts survival in stage III colon cancer. J. Surg. Oncol. 2011, 103, 406–410. [Google Scholar] [CrossRef]
- Schiffmann, L.; Eiken, A.K.; Gock, M.; Klar, E. Is the lymph node ratio superior to the Union for International Cancer Control (UICC) TNM system in prognosis of colon cancer? World J. Surg. Oncol. 2013, 11, 79. [Google Scholar] [CrossRef]
- Sugimoto, K.; Sakamoto, K.; Tomiki, Y.; Goto, M.; Kojima, Y.; Komiyama, H. The validity of predicting prognosis by the lymph node ratio in node-positive colon cancer. Dig. Surg. 2013, 30, 368–374. [Google Scholar] [CrossRef]
- Sugimoto, K.; Sakamoto, K.; Tomiki, Y.; Goto, M.; Kotake, K.; Sugihara, K. Proposal of new classification for stage III colon cancer based on the lymph node ratio: Analysis of 4,172 patients from multi-institutional database in Japan. Ann. Surg. Oncol. 2015, 22, 528–534. [Google Scholar] [CrossRef]
- Vaccaro, C.A.; Im, V.; Rossi, G.L.; Quintana, G.O.; Benati, M.L.; Perez de Arenaza, D.; Bonadeo, F.A. Lymph node ratio as prognosis factor for colon cancer treated by colorectal surgeons. Dis. Colon Rectum 2009, 52, 1244–1250. [Google Scholar] [CrossRef]
- Vather, R.; Sammour, T.; Kahokehr, A.; Connolly, A.B.; Hill, A.G. Lymph node evaluation and long-term survival in Stage II and Stage III colon cancer: A national study. Ann. Surg. Oncol. 2009, 16, 585–593. [Google Scholar] [CrossRef] [PubMed]
- Johnson, P.M.; Malatjalian, D.; Porter, G.A. Adequacy of nodal harvest in colorectal cancer: A consecutive cohort study. J. Gastrointest. Surg. Off. J. Soc. Surg. Aliment. Tract 2002, 6, 883–888, discussion 889–890. [Google Scholar] [CrossRef]
- Miller, E.D.; Robb, B.W.; Cummings, O.W.; Johnstone, P.A. The effects of preoperative chemoradiotherapy on lymph node sampling in rectal cancer. Dis. Colon Rectum 2012, 55, 1002–1007. [Google Scholar] [CrossRef] [PubMed]
- Lykke, J.; Roikjaer, O.; Jess, P. Tumour stage and preoperative chemoradiotherapy influence the lymph node yield in stages I-III rectal cancer: Results from a prospective nationwide cohort study. Colorectal Dis. Off. J. Assoc. Coloproctology Great Br. Irel. 2014, 16, O144-9. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Lymph Node Metastasis | P-Value | ||
|---|---|---|---|
| Present | Absent | ||
| Total (n = 266) | 146 (54.9) | 120 (45.1) | |
| Age (mean ± SD, years) | 64.03 ± 13.42 | 63.04 ± 12.30 | 0.534 |
| Sex | 0.313 | ||
| Male (n = 135) | 70 (47.9) | 65 (54.2) | |
| Female (n = 131) | 76 (52.1) | 55 (45.8) | |
| Tumor maximum diameter | 0.192 | ||
| ≤5 cm | 53 (36.3) | 53 (44.2) | |
| >5 cm | 93 (63.7) | 67 (55.8) | |
| Tumor size (mean ± SD, cm) | 5.69 ± 2.07 | 5.18 ± 2.05 | 0.044 |
| Location of tumor | 0.422 | ||
| right colon | 67 (45.9) | 61 (50.8) | |
| left colon | 79 (54.1) | 59 (49.2) | |
| Tumor differentiation | 108 (74.0) | 103 (85.8) | 0.017 |
| Well or Moderate | 38 (26.0) | 17 (14.2) | |
| Poorly | |||
| Vascular invasion | <0.001+ | ||
| Present | 22 (15.1) | 2 (1.7) | |
| Absent | 124 (84.9) | 118 (98.3) | |
| Lymphatic invasion | <0.001 | ||
| Present | 57 (39.0) | 13 (10.8) | |
| Absent | 89 (61.0) | 107 (89.2) | |
| Perineural invasion | <0.001 | ||
| Present | 35 (24.0) | 9 (7.5) | |
| Absent | 111 (76.0) | 111 (92.5) | |
| Number of examined lymph node (mean ± SD) | 35.64 ± 17.15 | 33.38 ± 19.38 | 0.316 |
| pT stage | <0.001 | ||
| pT1-2 | 9 (6.2) | 32 (26.7) | |
| pT3-4 | 137 (93.8) | 88 (73.3) | |
| Distant metastasis | 0.001 | ||
| Present | 24 (16.4) | 5 (4.2) | |
| Absent | 122 (83.6) | 115 (95.8) | |
| pTNM stage | <0.001 | ||
| I–II | 0 (0.0) | 115 (95.8) | |
| III-IV | 146 (100.0) | 5 (4.2) | |
| Location of Tumor | P-Value | ||
|---|---|---|---|
| Colon | Rectum | ||
| Total (n = 146) | 116 (79.5) | 30 (20.5) | |
| Number of examined lymph nodes (mean ± SD) | 36.60 ± 18.11 | 31.90 ± 12.28 | 0.181 |
| Number of involved lymph nodes (mean ± SD) | 6.37 ± 7.78 | 11.83 ± 10.92 | 0.014 |
| Metastatic lymph node ratio (mean ± SD) | 0.21 ± 0.24 | 0.38 ± 0.28 | 0.003 |
| Location of Tumor | R2 | P-Value |
|---|---|---|
| Overall | 0.030 | 0.037 |
| Colon | 0.029 | 0.068 |
| Rectum | 0.172 | 0.023 |
| Metastatic Lymph Node Ratio | Overall Survival | Recurrence-Free Survival | ||
|---|---|---|---|---|
| Hazard Ratio | P-Value | Hazard Ratio | P-Value | |
| Overall | ||||
| ≥0.1 vs. <0.1 | 3.074 (1.864–5.069) | <0.001 | 2.559 (1.616–4.053) | <0.001 |
| ≥0.2 vs. <0.2 | 3.423 (2.186–5.361) | <0.001 | 2.751 (1.803–4.197) | <0.001 |
| ≥0.3 vs. <0.3 | 3.345 (2.136–5.237) | <0.001 | 2.822 (1.828–4.356) | <0.001 |
| ≥0.4 vs. <0.4 | 3.836 (2.375–6.195) | <0.001 | 3.233 (2.027–5.156) | <0.001 |
| Colon | ||||
| ≥0.1 vs. <0.1 | 2.972 (1.741–5.074) | <0.001 | 2.333 (1.423–3.826) | 0.001 |
| ≥0.2 vs. <0.2 | 3.420 (2.071–5.649) | <0.001 | 2.701 (1.673–4.361) | <0.001 |
| ≥0.3 vs. <0.3 | 3.765 (2.221–6.382) | <0.001 | 3.395 (2.022–5.701) | <0.001 |
| ≥0.4 vs. <0.4 | 5.679 (3.131–10.302) | <0.001 | 5.141 (2.846–9.284) | <0.001 |
| Rectum | ||||
| ≥0.1 vs. <0.1 | 5.005 (0.664–37.706) | 0.118 | 6.577 (0.876–49.385) | 0.067 |
| ≥0.2 vs. <0.2 | 4.181 (1.203–14.533) | 0.024 | 3.304 (1.095–9.968) | 0.034 |
| ≥0.3 vs. <0.3 | 2.792 (1.040–7.497) | 0.042 | 1.938 (0.789–4.764) | 0.149 |
| ≥0.4 vs. <0.4 | 2.275 (0.890–5.814) | 0.086 | 1.746 (0.723–4.219) | 0.216 |
| Overall Survival | Recurrence-Free Survival | |||
|---|---|---|---|---|
| Hazard Ratio | P-Value | Hazard Ratio | P-Value | |
| Lymph node metastasis | 2.045 (1.398–2.990) | <0.001 | 2.193 (1.522–3.162) | <0.001 |
| Lymphatic invasion | 1.987 (1.367–2.889) | <0.001 | 1.775 (1.237–2.549) | 0.002 |
| pN stage (pN1/2 vs. pN0) | 1.804 (1.457–2.233) | <0.001 | 1.849 (1.507–2.269) | <0.001 |
| Metastatic Lymph Node Ratio | P-Value | ||
|---|---|---|---|
| High | Low | ||
| Total (n = 146) | 60 (41.1) | 86 (58.9) | |
| Age (mean ± SD, years) | 64.32 ± 13.51 | 63.84 ± 13.43 | 0.832 |
| Sex | 0.923 | ||
| Male (n = 70) | 28 (47.5) | 42 (48.3) | |
| Female (n = 76) | 31 (52.5) | 45 (51.7) | |
| Tumor maximum diameter | 0.209 | ||
| ≤5 cm | 25 (42.4) | 28 (32.2) | |
| >5 cm | 34 (57.6) | 59 (67.8) | |
| Tumor size (mean ± SD, cm) | 5.42 ± 2.01 | 5.88 ± 2.10 | 0.183 |
| Location of tumor | <0.001 | ||
| Right colon | 16 (27.1) | 51 (58.6) | |
| Left colon and rectum | 43 (72.9) | 36 (41.4) | |
| Tumor differentiation | 0.074 | ||
| Well or Moderate | 39 (66.1) | 69 (79.3) | |
| Poorly | 20 (33.9) | 18 (20.7) | |
| Vascular invasion | <0.001 | ||
| Present | 17 (28.8) | 5 (5.7) | |
| Absent | 42 (71.2) | 82 (94.3) | |
| Lymphatic invasion | <0.001 | ||
| Present | 38 (64.4) | 19 (21.8) | |
| Absent | 21 (35.6) | 68 (78.2) | |
| Perineural invasion | 0.007 | ||
| Present | 21 (35.6) | 14 (16.1) | |
| Absent | 38 (64.4) | 73 (83.9) | |
| Number of examined lymph node (mean ± SD) | 30.60 ± 15.41 | 39.15 ± 17.50 | 0.003 |
| Number of involved lymph node (mean ± SD) | 14.30 ± 10.11 | 2.74 ± 2.12 | <0.001 |
| pT stage | 0.655 + | ||
| pT1-2 | 3 (5.1) | 6 (6.9) | |
| pT3-4 | 56 (94.9) | 81 (93.1) | |
| Distant metastasis | 0.295 | ||
| Present | 12 (20.3) | 12 (13.8) | |
| Absent | 47 (79.7) | 75 (86.2) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pyo, J.-S.; Shin, Y.-M.; Kang, D.-W. Prognostic Implication of Metastatic Lymph Node Ratio in Colorectal Cancers: Comparison Depending on Tumor Location. J. Clin. Med. 2019, 8, 1812. https://doi.org/10.3390/jcm8111812
Pyo J-S, Shin Y-M, Kang D-W. Prognostic Implication of Metastatic Lymph Node Ratio in Colorectal Cancers: Comparison Depending on Tumor Location. Journal of Clinical Medicine. 2019; 8(11):1812. https://doi.org/10.3390/jcm8111812
Chicago/Turabian StylePyo, Jung-Soo, Young-Min Shin, and Dong-Wook Kang. 2019. "Prognostic Implication of Metastatic Lymph Node Ratio in Colorectal Cancers: Comparison Depending on Tumor Location" Journal of Clinical Medicine 8, no. 11: 1812. https://doi.org/10.3390/jcm8111812
APA StylePyo, J.-S., Shin, Y.-M., & Kang, D.-W. (2019). Prognostic Implication of Metastatic Lymph Node Ratio in Colorectal Cancers: Comparison Depending on Tumor Location. Journal of Clinical Medicine, 8(11), 1812. https://doi.org/10.3390/jcm8111812