Impact of Body Composition on the Risk of Hepatocellular Carcinoma Recurrence After Liver Transplantation

 ,
,
Abstract
1. Introduction
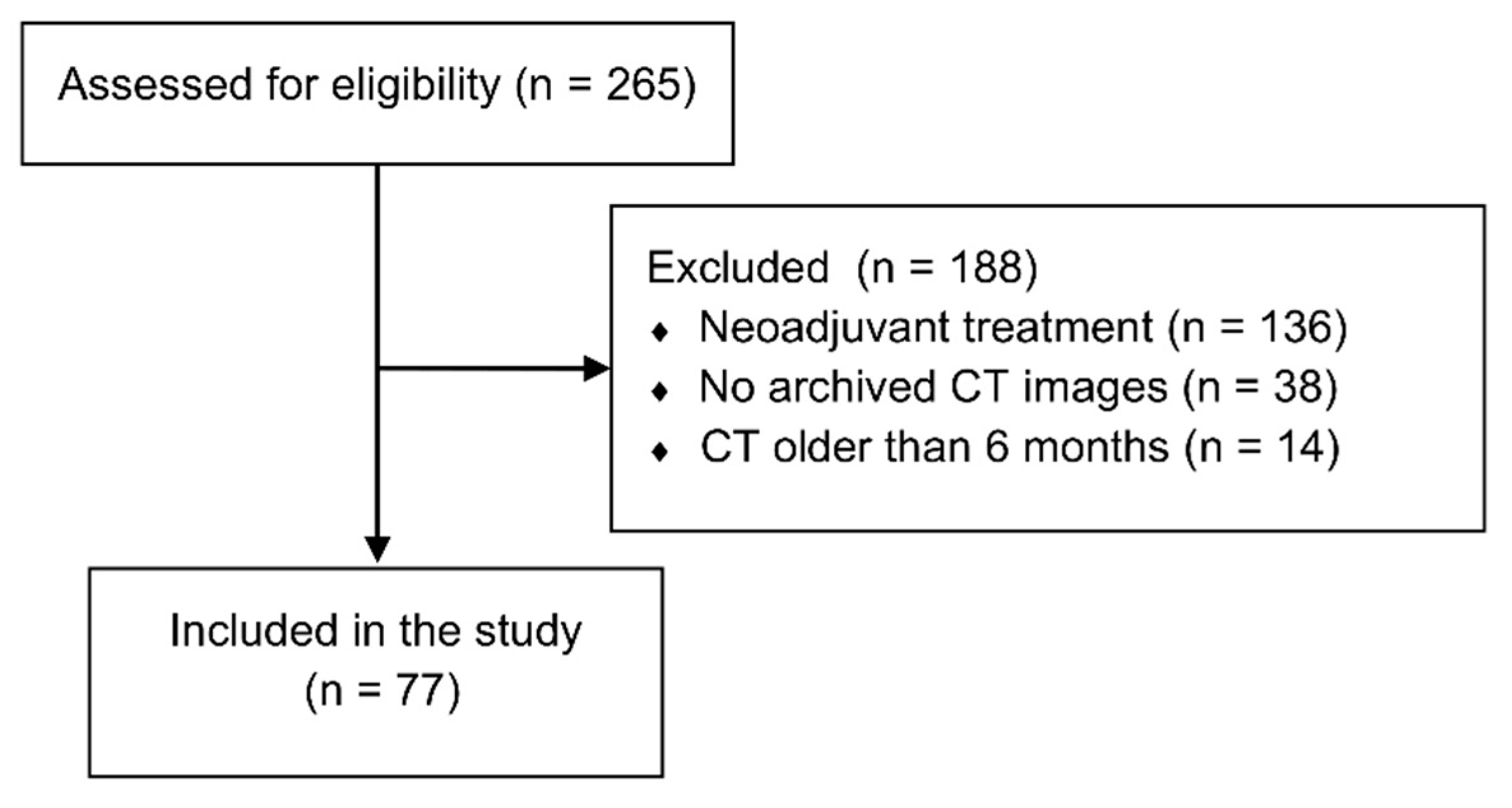
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Puigvehí, M.; Hashim, D.; Haber, P.K.; Dinani, A.; Schiano, T.D.; Asgharpour, A.; Kushner, T.; Kakked, G.; Tabrizian, P.; Schwartz, M.; et al. Liver Transplant for Hepatocellular Carcinoma in the United States: Evolving Trends over the Last Three Decades. Am. J. Transplant. 2019. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferro, V.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Montalto, F.; Ammatuna, M.; Morabito, A.; Gennari, L. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N. Engl. J. Med. 1996, 334, 693–699. [Google Scholar] [CrossRef] [PubMed]
- Grąt, M.; Wronka, K.M.; Stypułkowski, J.; Bik, E.; Krasnodębski, M.; Masior, Ł.; Lewandowski, Z.; Grąt, K.; Patkowski, W.; Krawczyk, M. The Warsaw Proposal for the Use of Extended Selection Criteria in Liver Transplantation for Hepatocellular Cancer. Ann. Surg. Oncol. 2017, 24, 526–534. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferro, V.; Sposito, C.; Zhou, J.; Pinna, A.D.; De Carlis, L.; Fan, J.; Cescon, M.; Di Sandro, S.; Yi-Feng, H.; Lauterio, A.; et al. Metroticket 2.0 Model for Analysis of Competing Risks of Death After Liver Transplantation for Hepatocellular Carcinoma. Gastroenterology 2018, 154, 128–139. [Google Scholar] [CrossRef] [PubMed]
- Duvoux, C.; Roudot-Thoraval, F.; Decaens, T.; Pessione, F.; Badran, H.; Piardi, T.; Francoz, C.; Compagnon, P.; Vanlemmens, C.; Dumortier, J.; et al. Liver transplantation for hepatocellular carcinoma: A model including α-Fetoprotein improves the performance of Milan criteria. Gastroenterology 2012, 143, 986–994. [Google Scholar] [CrossRef] [PubMed]
- Mehta, N.; Dodge, J.L.; Roberts, J.P.; Hirose, R.; Yao, F.Y. Alpha-Fetoprotein Decrease from >1000 to <500 ng/mL in Patients with Hepatocellular Carcinoma Leads to Improved Posttransplant Outcomes. Hepatology 2019, 69, 1193–1205. [Google Scholar] [PubMed]
- Halazun, K.J.; Tabrizian, P.; Najjar, M.; Florman, S.; Schwartz, M.; Michelassi, F.; Samstein, B.; Brown, R.S., Jr.; Emond, J.C.; Busuttil, R.W.; et al. Is it Time to Abandon the Milan Criteria?: Results of a Bicoastal US Collaboration to Redefine Hepatocellular Carcinoma Liver Transplantation Selection Policies. Ann. Surg. 2018, 268, 690–699. [Google Scholar] [CrossRef] [PubMed]
- Halazun, K.J.; Najjar, M.; Abdelmessih, R.M.; Samstein, B.; Griesemer, A.D.; Guarrera, J.V.; Kato, T.; Verna, E.C.; Emond, J.C.; Brown, R.S., Jr. Recurrence After Liver Transplantation for Hepatocellular Carcinoma: A New MORAL to the Story. Ann. Surg. 2017, 265, 557–564. [Google Scholar] [CrossRef]
- Grąt, M.; Stypułkowski, J.; Morawski, M.; Wronka, K.M.; Wasilewicz, M.; Lewandowski, Z.; Grąt, K.; Wójcik, Z.; Patkowski, W.; Zieniewicz, K. Shadows Behind Using Simple Risk Models in Selection of Hepatocellular Carcinoma Patients for Liver Transplantation. Ann. Surg. 2018. [Google Scholar] [CrossRef]
- Grąt, M.; Krasnodębski, M.; Krawczyk, M.; Stypułkowski, J.; Morawski, M.; Wasilewicz, M.; Lewandowski, Z.; Grąt, K.; Patkowski, W.; Zieniewicz, K. Extremes of Liver Transplantation for Hepatocellular Carcinoma. J. Clin. Med. 2019, 8, 787. [Google Scholar] [CrossRef]
- Karczewski, J.; Begier-Krasińska, B.; Staszewski, R.; Popławska, E.; Gulczynska-Elhadi, K.; Dobrowolska, A. Obesity and the Risk of Gastrointestinal Cancers. Dig. Dis. Sci. 2019, 64, 2740–2749. [Google Scholar] [CrossRef] [PubMed]
- Okumura, S.; Kaido, T.; Hamaguchi, Y.; Kobayashi, A.; Shirai, H.; Yao, S.; Yagi, S.; Kamo, N.; Hatano, E.; Okajima, H.; et al. Visceral Adiposity and Sarcopenic Visceral Obesity are Associated with Poor Prognosis After Resection of Pancreatic Cancer. Ann. Surg. Oncol. 2017, 24, 3732–3740. [Google Scholar] [CrossRef] [PubMed]
- Kambara, Y.; Yuasa, N.; Takeuchi, E.; Miyake, H.; Nagai, H.; Yoshioka, Y.; Okuno, M.; Miyata, K. Overweight or Obesity is an Unfavorable Long-Term Prognostic Factor for Patients who Underwent Gastrectomy for Stage II/III Gastric Cancer. World J. Surg. 2019, 43, 1766–1776. [Google Scholar] [CrossRef] [PubMed]
- Shiota, M.; Takeuchi, A.; Sugimoto, M.; Kashiwagi, E.; Dejima, T.; Kiyoshima, K.; Inokuchi, J.; Tatsugami, K.; Yokomizo, A.; Eto, M. The Differential Impact of Body Mass Index and the Feature of Metabolic Syndrome on Oncological Outcomes Following Different Surgical Procedures in Japanese Men with Prostate Cancer. Ann. Surg. Oncol. 2017, 24, 1443–1450. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.F.; Lu, J.; Zheng, C.H.; Li, P.; Xie, J.W.; Wang, J.B.; Lin, J.X.; Chen, Q.Y.; Lin, M.; Huang, C.M. A Novel Prognostic Scoring System Based on Preoperative Sarcopenia Predicts the Long-Term Outcome for Patients After R0 Resection for Gastric Cancer: Experiences of a High-Volume Center. Ann. Surg. Oncol. 2017, 24, 1795–1803. [Google Scholar] [CrossRef] [PubMed]
- Kudou, K.; Saeki, H.; Nakashima, Y.; Edahiro, K.; Korehisa, S.; Taniguchi, D.; Tsutsumi, R.; Nishimura, S.; Nakaji, Y.; Akiyama, S.; et al. Prognostic Significance of Sarcopenia in Patients with Esophagogastric Junction Cancer or Upper Gastric Cancer. Ann. Surg. Oncol. 2017, 24, 1804–1810. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Zheng, Z.F.; Li, P.; Xie, J.W.; Wang, J.B.; Lin, J.X.; Chen, Q.Y.; Cao, L.L.; Lin, M.; Tu, R.H.; et al. A Novel Preoperative Skeletal Muscle Measure as a Predictor of Postoperative Complications, Long-Term Survival and Tumor Recurrence for Patients with Gastric Cancer After Radical Gastrectomy. Ann. Surg. Oncol. 2018, 25, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Chakedis, J.; Spolverato, G.; Beal, E.W.; Woelfel, I.; Bagante, F.; Merath, K.; Sun, S.H.; Chafitz, A.; Galo, J.; Dillhoff, M.; et al. Pre-Operative Sarcopenia Identifies Patients at Risk for Poor Survival After Resection of Biliary Tract Cancers. J. Gastrointest. Surg. 2018, 22, 1697–1708. [Google Scholar] [CrossRef] [PubMed]
- Jung, A.R.; Roh, J.L.; Kim, J.S.; Kim, S.B.; Choi, S.H.; Nam, S.Y.; Kim, S.Y. Prognostic value of body composition on recurrence and survival of advanced-stage head and neck cancer. Eur. J. Cancer 2019, 116, 98–106. [Google Scholar] [CrossRef]
- Kobayashi, A.; Kaido, T.; Hamaguchi, Y.; Okumura, S.; Shirai, H.; Yao, S.; Kamo, N.; Yagi, S.; Taura, K.; Okajima, H.; et al. Impact of Sarcopenic Obesity on Outcomes in Patients Undergoing Hepatectomy for Hepatocellular Carcinoma. Ann. Surg. 2019, 269, 924–931. [Google Scholar] [CrossRef]
- Itoh, S.; Shirabe, K.; Matsumoto, Y.; Yoshiya, S.; Muto, J.; Harimoto, N.; Yamashita, Y.; Ikegami, T.; Yoshizumi, T.; Nishie, A.; et al. Effect of body composition on outcomes after hepatic resection for hepatocellular carcinoma. Ann. Surg. Oncol. 2014, 21, 3063–3068. [Google Scholar] [CrossRef] [PubMed]
- Guo, Z.; Zhang, J.; Jiang, J.H.; Li, L.Q.; Xiang, B.D. Obesity Does Not Influence Outcomes in Hepatocellular Carcinoma Patients following Curative Hepatectomy. PLoS ONE 2015, 10, e0125649. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.X.; Zhu, N.; Zhang, C.J.; Wang, Y.K.; Wu, H.T.; Li, Q.; Du, K.; Liao, D.F.; Qin, L. Friend or foe: Multiple roles of adipose tissue in cancer formation and progression. J. Cell. Physiol. 2019, 234, 21436–21449. [Google Scholar] [CrossRef] [PubMed]
- Lutz, C.T.; Quinn, L.S. Sarcopenia, obesity, and natural killer cell immune senescence in aging: Altered cytokine levels as a common mechanism. Aging 2012, 4, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Parida, S.; Siddharth, S.; Sharma, D. Adiponectin, Obesity, and Cancer: Clash of the Bigwigs in Health and Disease. Int. J. Mol. Sci. 2019, 20, 2519. [Google Scholar] [CrossRef] [PubMed]
- O’Shea, D.; Hogan, A.E. Dysregulation of Natural Killer Cells in Obesity. Cancers 2019, 11, 573. [Google Scholar] [CrossRef] [PubMed]
- Grąt, M.; Krawczyk, M.; Wronka, K.M.; Stypułkowski, J.; Lewandowski, Z.; Wasilewicz, M.; Krawczyk, P.; Grąt, K.; Patkowski, W.; Zieniewicz, K. Ischemia-Reperfusion injury and the risk of hepatocellular carcinoma recurrence after deceased donor liver transplantation. Sci. Rep. 2018, 8, 8935. [Google Scholar] [CrossRef]
- Grąt, M.; Kornasiewicz, O.; Lewandowski, Z.; Skalski, M.; Zieniewicz, K.; Pączek, L.; Krawczyk, M. The impact of surgical technique on the results of liver transplantation in patients with hepatocellular carcinoma. Ann. Transplant. 2013, 18, 448–459. [Google Scholar]
- Krawczyk, M.; Grąt, M.; Barski, K.; Ligocka, J.; Antczak, A.; Kornasiewicz, O.; Skalski, M.; Patkowski, W.; Nyckowski, P.; Zieniewicz, K.; et al. 1000 liver transplantations at the Department of General, Transplant and Liver Surgery, Medical University of Warsaw—Analysis of indications and results. Pol. Przegl. Chir. 2012, 84, 304–312. [Google Scholar] [CrossRef]
- Montano-Loza, A.J.; Mazurak, V.C.; Ebadi, M.; Meza-Junco, J.; Sawyer, M.B.; Baracos, V.E.; Kneteman, N. Visceral adiposity increases risk for hepatocellular carcinoma in male patients with cirrhosis and recurrence after liver transplant. Hepatology 2018, 67, 914–923. [Google Scholar] [CrossRef]
- Hamaguchi, Y.; Kaido, T.; Okumura, S.; Kobayashi, A.; Shirai, H.; Yao, S.; Yagi, S.; Kamo, N.; Seo, S.; Taura, K.; et al. Preoperative Visceral Adiposity and Muscularity Predict Poor Outcomes after Hepatectomy for Hepatocellular Carcinoma. Liver Cancer 2019, 8, 92–109. [Google Scholar] [CrossRef] [PubMed]
- Higashi, T.; Hayashi, H.; Kaida, T.; Arima, K.; Takeyama, H.; Taki, K.; Izumi, D.; Tokunaga, R.; Kosumi, K.; Nakagawa, S.; et al. Prognostic Impact of Visceral Fat Amount and Branched-Chain Amino Acids (BCAA) in Hepatocellular Carcinoma. Ann. Surg. Oncol. 2015, 22, S1041–S1047. [Google Scholar] [CrossRef] [PubMed]
- Fujihara, S.; Mori, H.; Kobara, H.; Nishiyama, N.; Kobayashi, M.; Oryu, M.; Masaki, T. Metabolic syndrome, obesity, and gastrointestinal cancer. Gastroenterol. Res. Pract. 2012, 2012, 483623. [Google Scholar] [CrossRef] [PubMed]
- McDonald, A.M.; Fiveash, J.B.; Kirkland, R.S.; Cardan, R.A.; Jacob, R.; Kim, R.Y.; Dobelbower, M.C.; Yang, E.S. Subcutaneous adipose tissue characteristics and the risk of biochemical recurrence in men with High-Risk prostate cancer. Urol. Oncol. 2017, 35, e15–e663. [Google Scholar] [CrossRef] [PubMed]
- Delouya, G.; Tiberi, D.; Bhatnagar, S.R.; Campeau, S.; Saad, F.; Taussky, D. Impact of adipose tissue on prostate cancer aggressiveness—Analysis of a high-risk population. Horm. Mol. Biol. Clin. Investig. 2018, 36. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Norheim, F.; Langleite, T.M.; Gulseth, H.L.; Birkeland, K.I.; Drevon, C.A. Effects of Long-Term exercise on plasma adipokine levels and inflammation-related gene expression in subcutaneous adipose tissue in sedentary dysglycaemic, overweight men and sedentary normoglycaemic men of healthy weight. Diabetologia 2019, 62, 1048–1064. [Google Scholar] [CrossRef] [PubMed]
- Anderson, M.R.; Udupa, J.K.; Edwin, E.; Diamond, J.M.; Singer, J.P.; Kukreja, J.; Hays, S.R.; Greenland, J.R.; Ferrante, A.; Lippel, M.; et al. Adipose tissue quantification and primary graft dysfunction after lung transplantation: The Lung Transplant Body Composition study. J. Heart Lung Transplant. 2019, 10, S1053–S2498. [Google Scholar] [CrossRef] [PubMed]
- Duan, X.F.; Tang, P.; Li, Q.; Yu, Z.T. Obesity, adipokines and hepatocellular carcinoma. Int. J. Cancer 2013, 133, 1776–1783. [Google Scholar] [CrossRef]
- Saxena, N.K.; Sharma, D.; Ding, X.; Lin, S.; Marra, F.; Merlin, D.; Anania, F.A. Concomitant activation of the JAK/STAT, PI3K/AKT, and ERK signaling is involved in Leptin-Mediated promotion of invasion and migration of hepatocellular carcinoma cells. Cancer Res. 2007, 67, 2497–2507. [Google Scholar] [CrossRef]
- Ribatti, D.; Belloni, A.S.; Nico, B.; Di Comite, M.; Crivellato, E.; Vacca, A. Leptin-Leptin receptor are involved in angiogenesis in human hepatocellular carcinoma. Peptides 2008, 29, 1596–1602. [Google Scholar] [CrossRef]
- Stefanou, N.; Papanikolaou, V.; Furukawa, Y.; Nakamura, Y.; Tsezou, A. Leptin as a critical regulator of hepatocellular carcinoma development through modulation of human telomerase reverse transcriptase. BMC Cancer 2010, 10, 442. [Google Scholar] [CrossRef] [PubMed]
- Sharma, D.; Wang, J.; Fu, P.P.; Sharma, S.; Nagalingam, A.; Mells, J.; Handy, J.; Page, A.J.; Cohen, C.; Anania, F.A.; et al. Adiponectin antagonizes the oncogenic actions of leptin in hepatocellular carcinogenesis. Hepatology 2010, 52, 1713–1722. [Google Scholar] [CrossRef] [PubMed]
- Corrêa, L.H.; Heyn, G.S.; Magalhaes, K.G. The Impact of the Adipose Organ Plasticity on Inflammation and Cancer Progression. Cells 2019, 8, E662. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.R.; Park, S.; Han, S.; Ahn, J.H.; Kim, S.; Sinn, D.H.; Jeong, W.K.; Ko, J.S.; Gwak, M.S.; Kim, G.S. Sarcopenia as a predictor of post-transplant tumor recurrence after living donor liver transplantation for hepatocellular carcinoma beyond the Milan criteria. Sci. Rep. 2018, 8, 7157. [Google Scholar] [CrossRef] [PubMed]
- Itoh, S.; Yoshizumi, T.; Kimura, K.; Okabe, H.; Harimoto, N.; Ikegami, T.; Uchiyama, H.; Shirabe, K.; Nishie, A.; Maehara, Y. Effect of Sarcopenic Obesity on Outcomes of Living-Donor Liver Transplantation for Hepatocellular Carcinoma. Anticancer Res 2016, 36, 3029–3034. [Google Scholar] [PubMed]
- Yabusaki, N.; Fujii, T.; Yamada, S.; Suzuki, K.; Sugimoto, H.; Kanda, M.; Nakayama, G.; Koike, M.; Fujiwara, M.; Kodera, Y. Adverse impact of low skeletal muscle index on the prognosis of hepatocellular carcinoma after hepatic resection. Int. J. Surg. 2016, 30, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Voron, T.; Tselikas, L.; Pietrasz, D.; Pigneur, F.; Laurent, A.; Compagnon, P.; Salloum, C.; Luciani, A.; Azoulay, D. Sarcopenia Impacts on Short- and Long-Term Results of Hepatectomy for Hepatocellular Carcinoma. Ann. Surg. 2015, 261, 1173–1183. [Google Scholar] [CrossRef]
- Harimoto, N.; Shirabe, K.; Yamashita, Y.I.; Ikegami, T.; Yoshizumi, T.; Soejima, Y.; Ikeda, T.; Maehara, Y.; Nishie, A.; Yamanaka, T. Sarcopenia as a predictor of prognosis in patients following hepatectomy for hepatocellular carcinoma. Br. J. Surg. 2013, 100, 1523–1530. [Google Scholar] [CrossRef]
- Hiraoka, A.; Otsuka, Y.; Kawasaki, H.; Izumoto, H.; Ueki, H.; Kitahata, S.; Aibiki, T.; Okudaira, T.; Yamago, H.; Miyamoto, Y.; et al. Impact of muscle volume and muscle function decline in patients undergoing surgical resection for hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2018, 33, 1271–1276. [Google Scholar] [CrossRef]
- Kamachi, S.; Mizuta, T.; Otsuka, T.; Nakashita, S.; Ide, Y.; Miyoshi, A.; Kitahara, K.; Eguchi, Y.; Ozaki, I.; Anzai, K. Sarcopenia is a risk factor for the recurrence of hepatocellular carcinoma after curative treatment. Hepatol. Res. 2016, 46, 201–208. [Google Scholar] [CrossRef]
- Ata, N.; Ayloo, S.; Tsung, A.; Molinari, M. Recipient obesity does not affect survival after deceased donor liver transplantation for hepatocellular carcinoma. A national retrospective cohort study in the United States. HPB 2019, 21, 67–76. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Medians and IQRs or Numbers and % | |
|---|---|
| Age (years) | 56 (52–61) |
| Sex | |
| Male | 59 (76.6%) |
| Female | 18 (23.4%) |
| HCV | 58 (75.3%) |
| BMI (kg/m2) | 25.20 (23.3–28.3) |
| Serum AFP (ng/ml) | 13.1 (5.0–112.8) |
| Adipose tissue (cm2/m2) | |
| subcutaneous | 51.7 (37.3–72.3) |
| visceral | 27.8 (20.3–46.6) |
| total | 83.4 (58.7–110.9) |
| Muscular tissue (cm2/m2) | |
| psoas major | 6.2 (5.1–7.3) |
| total | 50.1 (43.1–56.4) |
| Time between LT and the last CT scan (days) | 51 (26–95) |
| Tumor characteristic | |
| number of tumors | 1 (1–2) |
| size of the largest tumor | 25 (15–35) |
| microinvasion | 14 (18.67%) |
| poor tumor differentiation | 9 (11.69%) |
| fulfillment of Milan criteria | 53 (68.83%) |
| R | p | |
|---|---|---|
| Subcutaneous Fat Area (SFA) | ||
| whole group | 0.735 | p < 0.001 |
| males | 0.756 | p < 0.001 |
| females | 0.803 | p < 0.001 |
| Visceral Fat Area (VFA) | ||
| whole group | 0.569 | p < 0.001 |
| males | 0.509 | p < 0.001 |
| females | 0.576 | p = 0.012 |
| Total Fat Area (TFA) | ||
| whole group | 0.710 | p < 0.001 |
| males | 0.700 | p < 0.001 |
| females | 0.803 | p < 0.001 |
| Psoas Muscle Area (PMA) | ||
| whole group | 0.453 | p < 0.001 |
| males | 0.344 | p = 0.008 |
| females | 0.606 | p = 0.008 |
| Total Skeletal Muscle Area (TSMA) | ||
| whole group | 0.529 | p < 0.001 |
| males | 0.491 | p < 0.001 |
| females | 0.667 | p < 0.002 |
| Factor | HR | 95% CI | p |
|---|---|---|---|
| Area of: | |||
| subcutaneous fat a | 1.026 | 1.005–1.047 | 0.013 |
| visceral fat a | 1.025 | 0.982–1.070 | 0.264 |
| total fat tissue a | 1.026 | 1.005–1.049 | 0.017 |
| psoas major a | 1.409 | 0.893–2.225 | 0.141 |
| total skeletal muscle a | 1.024 | 0.934–1.122 | 0.618 |
| Age b | 0.997 | 0.901–1.103 | 0.952 |
| BMI c | 1.183 | 0.956–1.463 | 0.122 |
| Tumor characteristics: | |||
| number of tumors d | 1.254 | 0.983–1.599 | 0.068 |
| size of the largest tumor e | 1.069 | 1.020–1.119 | 0.005 |
| microvascular invasion | 5.780 | 1.284–25.641 | 0.022 |
| poor tumor differentiation | 3.534 | 0.685–18.182 | 0.132 |
| fulfillment of Milan criteria | 100% vs. 53.3% * | p < 0.001 * | |
| Donor age b | 0.999 | 0.938–1.063 | 0.965 |
| MELD points f | 0.995 | 0.846–1.170 | 0.949 |
| Serum AFP g | 1.428 | 1.106–1.843 | 0.006 |
| Female sex | 0.627 | 0.075–5.217 | 0.666 |
| HCV | 0.903 | 0.100–2.041 | 0.301 |
| Body Mass Index (BMI) (kg/m2) | Subcutaneous Fat Area (SFA) | Total Fat Area (TFA) | ||
|---|---|---|---|---|
| Value (cm2/m2) | Number of Patients | Value (cm2/m2) | Number of Patients | |
| 18.50–24.99 | <71.5 ≥71.5 | 30 (90.9%) 3 (9.1%) | <90.5 ≥90.5 | 26 (78.8%) 7 (21.2%) |
| 25.00–29.99 | <71.5 ≥71.5 | 25 (71.4%) 10 (28.6%) | <90.5 ≥90.5 | 14 (40.0%) 21 (60.0%) |
| ≥ 30.00 | <71.5 ≥71.5 | 1 (11.1%) 8 (88.9%) | <90.5 ≥90.5 | 0 (0.0%) 9 (100.0%) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grąt, K.; Pacho, R.; Grąt, M.; Krawczyk, M.; Zieniewicz, K.; Rowiński, O. Impact of Body Composition on the Risk of Hepatocellular Carcinoma Recurrence After Liver Transplantation. J. Clin. Med. 2019, 8, 1672. https://doi.org/10.3390/jcm8101672
Grąt K, Pacho R, Grąt M, Krawczyk M, Zieniewicz K, Rowiński O. Impact of Body Composition on the Risk of Hepatocellular Carcinoma Recurrence After Liver Transplantation. Journal of Clinical Medicine. 2019; 8(10):1672. https://doi.org/10.3390/jcm8101672
Chicago/Turabian StyleGrąt, Karolina, Ryszard Pacho, Michał Grąt, Marek Krawczyk, Krzysztof Zieniewicz, and Olgierd Rowiński. 2019. "Impact of Body Composition on the Risk of Hepatocellular Carcinoma Recurrence After Liver Transplantation" Journal of Clinical Medicine 8, no. 10: 1672. https://doi.org/10.3390/jcm8101672
APA StyleGrąt, K., Pacho, R., Grąt, M., Krawczyk, M., Zieniewicz, K., & Rowiński, O. (2019). Impact of Body Composition on the Risk of Hepatocellular Carcinoma Recurrence After Liver Transplantation. Journal of Clinical Medicine, 8(10), 1672. https://doi.org/10.3390/jcm8101672