Optimized Treatment for Infantile Spasms: Vigabatrin versus Prednisolone versus Combination Therapy

 and
and
Abstract
1. Introduction
2. Experimental Section
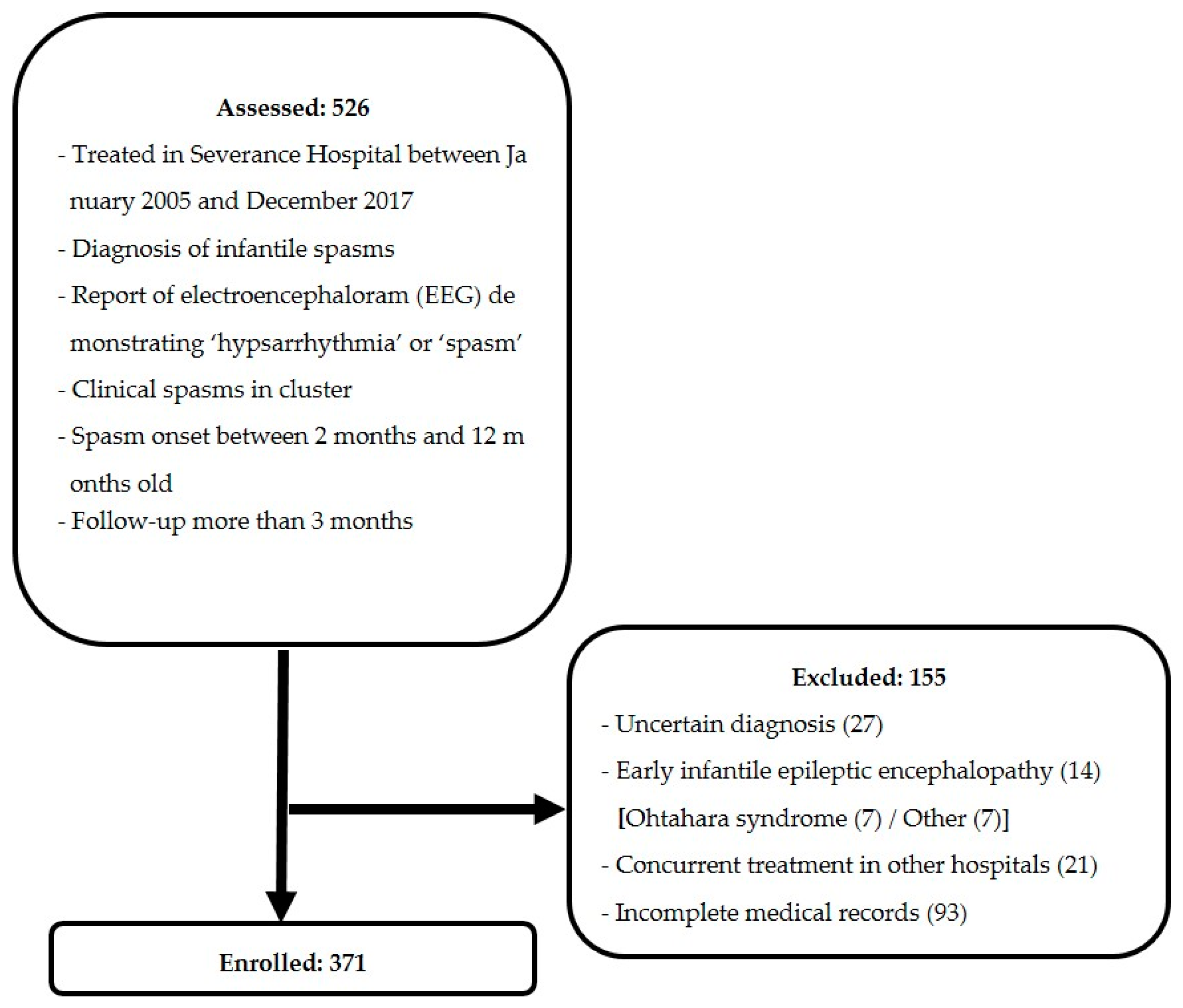
2.1. Study Design and Subjects
2.2. Outcome Measurement
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. First-Line Treatment
3.3. Second-Line Treatment
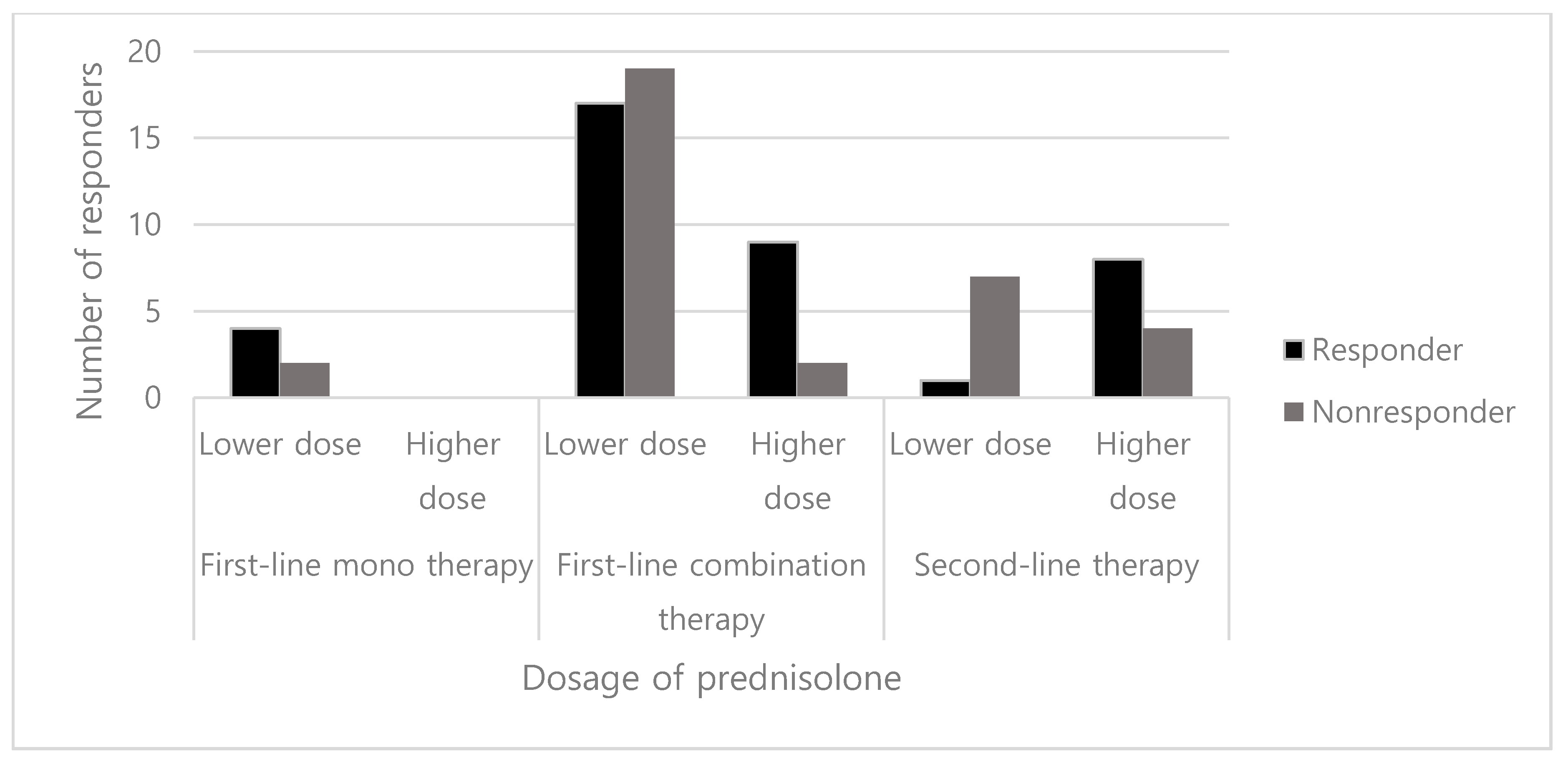
3.4. Dosage of Prednisolone
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hancock, E.C.; Osborne, J.P.; Edwards, S.W. Treatment of infantile spasms. Cochrane Database Syst. Rev. 2013, CD001770. [Google Scholar] [CrossRef] [PubMed]
- Pellock, J.M.; Hrachovy, R.; Shinnar, S.; Baram, T.Z.; Bettis, D.; Dlugos, D.J.; Gaillard, W.D.; Gibson, P.A.; Holmes, G.L.; Nordl, D.R.; et al. Infantile spasms: A U.S. consensus report. Epilepsia 2010, 51, 2175–2189. [Google Scholar] [CrossRef] [PubMed]
- D’Alonzo, R.; Rigante, D.; Mencaroni, E.; Esposito, S. West Syndrome: A Review and Guide for Paediatricians. Clin. Drug Investig. 2018, 38, 113–124. [Google Scholar] [CrossRef] [PubMed]
- O’Callaghan, F.J.; Lux, A.L.; Darke, K.; Edwards, S.W.; Hancock, E.; Johnson, A.L.; Kennedy, C.R.; Newton, R.W.; Verity, C.M.; Osborne, J.P. The effect of lead time to treatment and of age of onset on developmental outcome at 4 years in infantile spasms: Evidence from the United Kingdom Infantile Spasms Study. Epilepsia 2011, 52, 1359–1364. [Google Scholar] [CrossRef] [PubMed]
- Wilmshurst, J.M.; Gaillard, W.D.; Vinayan, K.P.; Tsuchida, T.N.; Plouin, P.; Van Bogaert, P.; Carrizosa, J.; Elia, M.; Craiu, D.; Jovic, N.J.; et al. Summary of recommendations for the management of infantile seizures: Task Force Report for the ILAE Commission of Pediatrics. Epilepsia 2015, 56, 1185–1197. [Google Scholar] [CrossRef] [PubMed]
- Tsao, C.Y. Current trends in the treatment of infantile spasms. Neuropsychiatr. Dis. Treat. 2009, 5, 289–299. [Google Scholar] [CrossRef][Green Version]
- Lerner, J.T.; Salamon, N.; Sankar, R. Clinical profile of vigabatrin as monotherapy for treatment of infantile spasms. Neuropsychiatr. Dis. Treat. 2010, 6, 731–740. [Google Scholar] [CrossRef][Green Version]
- Lux, A.L.; Edwards, S.W.; Hancock, E.; Johnson, A.L.; Kennedy, C.R.; Newton, R.W.; O’Callaghan, F.J.K.; Verity, C.M.; Osborne, J.P. The United Kingdom Infantile Spasms Study comparing vigabatrin with prednisolone or tetracosactide at 14 days: A multicentre, randomised controlled trial. Lancet 2004, 364, 1773–1778. [Google Scholar] [CrossRef]
- Go, C.Y.; Mackay, M.T.; Weiss, S.K.; Stephens, D.; Adams-Webber, T.; Ashwal, S.; Snead, O.C., 3rd. Evidence-based guideline update: Medical treatment of infantile spasms. Report of the Guideline Development Subcommittee of the American Academy of Neurology and the Practice Committee of the Child Neurology Society. Neurology 2012, 78, 1974–1980. [Google Scholar] [CrossRef]
- Lux, A.L.; Edwards, S.W.; Hancock, E.; Johnson, A.L.; Kennedy, C.R.; Newton, R.W.; O’Callaghan, F.J.K.; Verity, C.M.; Osborne, J.P. The United Kingdom Infantile Spasms Study (UKISS) comparing hormone treatment with vigabatrin on developmental and epilepsy outcomes to age 14 months: A multicentre randomised trial. Lancet Neurol. 2005, 4, 712–717. [Google Scholar] [CrossRef]
- Mohamed, B.P.; Scott, R.C.; Desai, N.; Gutta, P.; Patil, S. Seizure outcome in infantile spasms—A retrospective study. Epilepsia 2011, 52, 746–752. [Google Scholar] [CrossRef]
- Hahn, J.; Lee, H.; Kang, H.-C.; Lee, J.S.; Kim, H.D.; Kim, S.H.; Chang, M.J. Clobazam as an adjunctive treatment for infantile spasms. Epilepsy & Behavior 2019, 95, 161–165. [Google Scholar]
- Knupp, K.G.; Leister, E.; Coryell, J.; Nickels, K.C.; Ryan, N.; Juarez-Colunga, E.; Gaillard, W.D.; Mytinger, J.R.; Berg, A.T.; Millichap, J.; et al. Response to second treatment after initial failed treatment in a multicenter prospective infantile spasms cohort. Epilepsia 2016, 57, 1834–1842. [Google Scholar] [CrossRef]
- Rajaraman, R.R.; Lay, J.; Alayari, A.; Anderson, K.; Sankar, R.; Hussain, S.A. Prevention of infantile spasms relapse: Zonisamide and topiramate provide no benefit. Epilepsia 2016, 57, 1280–1287. [Google Scholar] [CrossRef]
- Zhu, X.; Chen, O.; Zhang, D.; Jin, R.; Li, F.; Wang, Y.; Sun, R. A prospective study on the treatment of infantile spasms with first-line topiramate followed by low-dose ACTH. Epilepsy Res. 2011, 93, 149–154. [Google Scholar] [CrossRef]
- Lawlor, K.M.; Devlin, A.M. Levetiracetam in the treatment of infantile spasms. Eur. J. Paediatr. Neurol. 2005, 9, 19–22. [Google Scholar] [CrossRef]
- Suzuki, Y.; Nagai, T.; Ono, J.; Imai, K.; Otani, K.; Tagawa, T.; Abe, J.; Shiomi, M.; Okada, S. Zonisamide monotherapy in newly diagnosed infantile spasms. Epilepsia 1997, 38, 1035–1038. [Google Scholar] [CrossRef]
- O’Callaghan, F.J.K.; Edwards, S.W.; Alber, F.D.; Hancock, E.; Johnson, A.L.; Kennedy, C.R.; Likeman, M.; Lux, A.L.; Mackay, M.; Mallick, A.A.; et al. Safety and effectiveness of hormonal treatment versus hormonal treatment with vigabatrin for infantile spasms (ICISS): A randomised, multicentre, open-label trial. Lancet Neurol. 2017, 16, 33–42. [Google Scholar] [CrossRef]
- Knupp, K.G. Hormonal therapy with vigabatrin is superior to hormonal therapy alone in infantile spasms. J. Pediatrics 2017, 184, 235–238. [Google Scholar] [CrossRef]
- Sakakihara, Y. Treatment of West syndrome. Brain Dev. 2011, 33, 202–206. [Google Scholar] [CrossRef]
- Lux, A.L.; Osborne, J.P. A proposal for case definitions and outcome measures in studies of infantile spasms and West syndrome: Consensus statement of the West Delphi group. Epilepsia 2004, 45, 1416–1428. [Google Scholar] [CrossRef] [PubMed]
- Kleinman, L.C.; Norton, E.C. What’s the Risk? A simple approach for estimating adjusted risk measures from nonlinear models including logistic regression. Health Serv. Res. 2009, 44, 288–302. [Google Scholar] [CrossRef] [PubMed]
- Hussain, S.A. Treatment of infantile spasms. Epilepsia Open 2018, 3, 143–154. [Google Scholar] [CrossRef]
- Ko, A.; Youn, S.E.; Chung, H.J.; Kim, S.H.; Lee, J.S.; Kim, H.D.; Kang, H.C. Vigabatrin and high-dose prednisolone therapy for patients with West syndrome. Epilepsy research 2018, 145, 127–133. [Google Scholar] [CrossRef]
- Chellamuthu, P.; Sharma, S.; Jain, P.; Kaushik, J.S.; Seth, A.; Aneja, S. High dose (4 mg/kg/day) versus usual dose (2 mg/kg/day) oral prednisolone for treatment of infantile spasms: An open-label, randomized controlled trial. Epilepsy Res. 2014, 108, 1378–1384. [Google Scholar] [CrossRef]
- Kossoff, E.H.; Hartman, A.L.; Rubenstein, J.E.; Vining, E.P. High-dose oral prednisolone for infantile spasms: An effective and less expensive alternative to ACTH. Epilepsy Behav. 2009, 14, 674–676. [Google Scholar] [CrossRef]
- Kelley, S.A.; Knupp, K.G. Infantile Spasms-Have We Made Progress? Curr. Neurol. Neurosci. Rep. 2018, 18, 27. [Google Scholar] [CrossRef]
- Pavone, P.; Striano, P.; Falsaperla, R.; Pavone, L.; Ruggieri, M. Infantile spasms syndrome, West syndrome and related phenotypes: What we know in 2013. Brain Dev. 2014, 36, 739–751. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristic | Treatment Group a | p Value | ||||
|---|---|---|---|---|---|---|
| Vigabatrin n = 271 | Prednisolone n = 6 | Vigabatrin + Prednisolone n = 47 | Non-Standard n = 47 | Total n = 371 | ||
| Sex Male Female | 163 (60.1) 108 (39.9) | 1 (16.7) 5 (83.3) | 21 (44.7) 26 (55.3) | 30 (63.8) 17 (36.2) | 215 (58.0) 156 (42.0) | 0.032 †,* |
| Presence of seizure history | 97 (35.8) | 0 (0.0) | 16 (34.0) | 15 (31.9) | 128 (34.5) | 0.320 † |
| Age at spasm onset, mo. | 5.8 (4.4, 7.3) | 7.7 (5.1, 8.7) | 5.7 (4.4, 6.7) | 5.7 (4.4, 7.4) | 5.8 (4.4, 7.3) | 0.719 ‡ |
| Age at treatment, mo. | 6.6 (5.3, 8.1) | 8.1 (5.4, 8.9) | 6.6 (5.5, 8.0) | 7.1 (5.3, 8.8) | 6.6 (5.3, 8.2) | 0.804 ‡ |
| Lag time from spasm onset to treatment, days | 12.0 (5.0, 29.0) | 7.0 (4.3, 19.5) | 20.0 (11.5, 43.0) | 20.0 (7.0, 56.0) | 14.0 (5.0, 32.0) | 0.012 ‡,* |
| Etiology Structural Metabolic Infection Genetic Unknown | 87 (32.1) 23 (8.5) 6 (2.2) 7 (2.6) 148 (54.6) | 1 (16.7) 0 (0) 0 (0) 0 (0) 5 (83.3) | 15 (31.9) 2 (4.3) 0 (0) 1 (2.1) 29 (61.7) | 12 (25.5) 2 (4.3) 1 (2.1) 1 (2.1) 31 (66.0) | 115 (31.0) 27 (7.3) 7 (1.9) 9 (2.4) 213 (57.4) | 0.938 § |
| Response to Initial treatment a | Time to Cessation of Spasms (days) b | Relapse Rate a | ||
|---|---|---|---|---|
| Treatment | Response n = 141 | Non-Response n = 230 | ||
| Vigabatrin | 106 (39.1) | 165 (60.9) | 5 (3, 9) | 8 (7.5) |
| Prednisolone | 4 (66.7) | 2 (33.3) | 4 (3, 7) | 1 (25.0) |
| Vigabatrin + prednisolone | 26 (55.3) | 21 (44.7) | 5 (2, 9) | 3 (11.5) |
| Non-standard | 5 (10.6) | 42 (89.4) | 4 (2, 7) | 2 (40.0) |
| Characteristic | Responders n (%) | p value † | Crude Risk Ratio (95% CI) | Adjusted a Risk Ratio (95% CI) | Adjusted b Risk Ratio (95% CI) |
|---|---|---|---|---|---|
| Treatment | |||||
| Vigabatrin | 106 (39.1) | REF | REF | REF | |
| Prednisolone | 4 (66.7) | 0.219 | 3.113 (0.560, 17.296) | 2.602 (0.465, 14.560) | 2.980 (0.523, 16.975) |
| Vigabatrin + prednisolone | 26 (55.3) | 0.037 * | 1.927 (1.032, 3.599) | 1.929 (1.028, 3.620) | 2.139 (1.124, 4.069) |
| Non-standard | 5 (10.6) | <0.001 * | 0.185 (0.071, 0.483) | 0.179 (0.068, 0.468) | 0.205 (0.078, 0.539) |
| Seizure history | |||||
| No | 102 (42.0) | 0.030 * | REF | REF | - |
| Yes | 39 (30.5) | 0.606 (0.385, 0.954) | 0.593 (0.371, 0.949) | - | |
| Lag time | |||||
| ≤4 weeks | 116 (43.8) | <0.001 * | REF | - | REF |
| >4 weeks | 25 (23.6) | 0.396 (0.238, 0.660) | - | 0.406 (0.239, 0.689) |
| Second-Line Treatment | Vigabatrin | Prednisolone | Non-Standard | |
|---|---|---|---|---|
| First-Line Treatment | ||||
| Vigabatrin | 5/5, 100% (up-titration) | 9/20, 45% | 24/140, 17% | |
| Prednisolone | 2/2, 100% | - | - | |
| Vigabatrin + prednisolone | 1/1, 100% (up-titration) | - | 2/20, 10% | |
| Non-standard | 13/31, 42% | 0/1, 0% | 2/10, 20% | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hahn, J.; Park, G.; Kang, H.-C.; Lee, J.S.; Kim, H.D.; Kim, S.H.; Chang, M.J. Optimized Treatment for Infantile Spasms: Vigabatrin versus Prednisolone versus Combination Therapy. J. Clin. Med. 2019, 8, 1591. https://doi.org/10.3390/jcm8101591
Hahn J, Park G, Kang H-C, Lee JS, Kim HD, Kim SH, Chang MJ. Optimized Treatment for Infantile Spasms: Vigabatrin versus Prednisolone versus Combination Therapy. Journal of Clinical Medicine. 2019; 8(10):1591. https://doi.org/10.3390/jcm8101591
Chicago/Turabian StyleHahn, Jongsung, Gyunam Park, Hoon-Chul Kang, Joon Soo Lee, Heung Dong Kim, Se Hee Kim, and Min Jung Chang. 2019. "Optimized Treatment for Infantile Spasms: Vigabatrin versus Prednisolone versus Combination Therapy" Journal of Clinical Medicine 8, no. 10: 1591. https://doi.org/10.3390/jcm8101591
APA StyleHahn, J., Park, G., Kang, H.-C., Lee, J. S., Kim, H. D., Kim, S. H., & Chang, M. J. (2019). Optimized Treatment for Infantile Spasms: Vigabatrin versus Prednisolone versus Combination Therapy. Journal of Clinical Medicine, 8(10), 1591. https://doi.org/10.3390/jcm8101591