Effort Oxygen Saturation and Effort Heart Rate to Detect Exacerbations of Chronic Obstructive Pulmonary Disease or Congestive Heart Failure

 , , , ,
, , , ,
Abstract
1. Introduction
2. Experimental Section
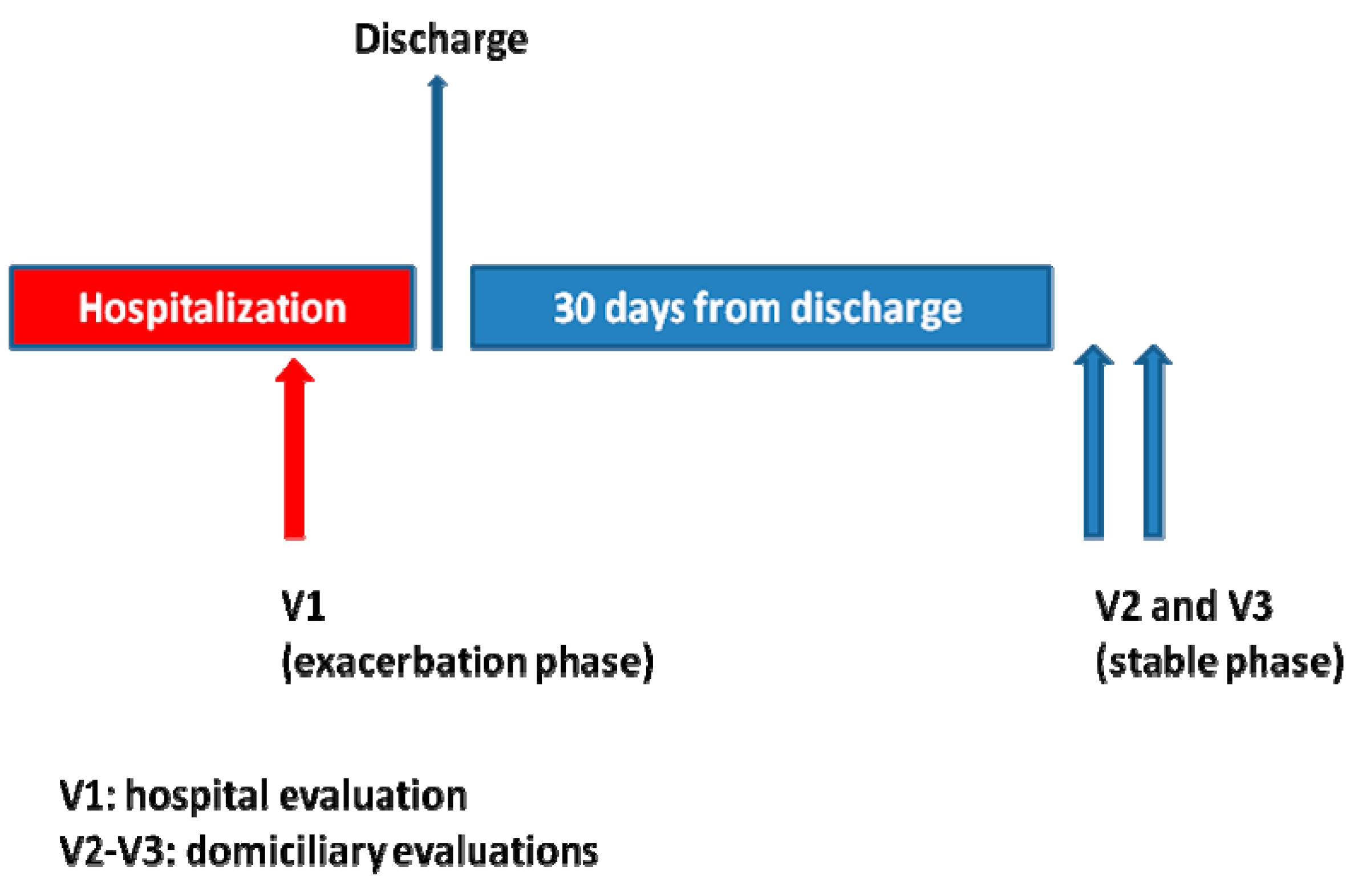
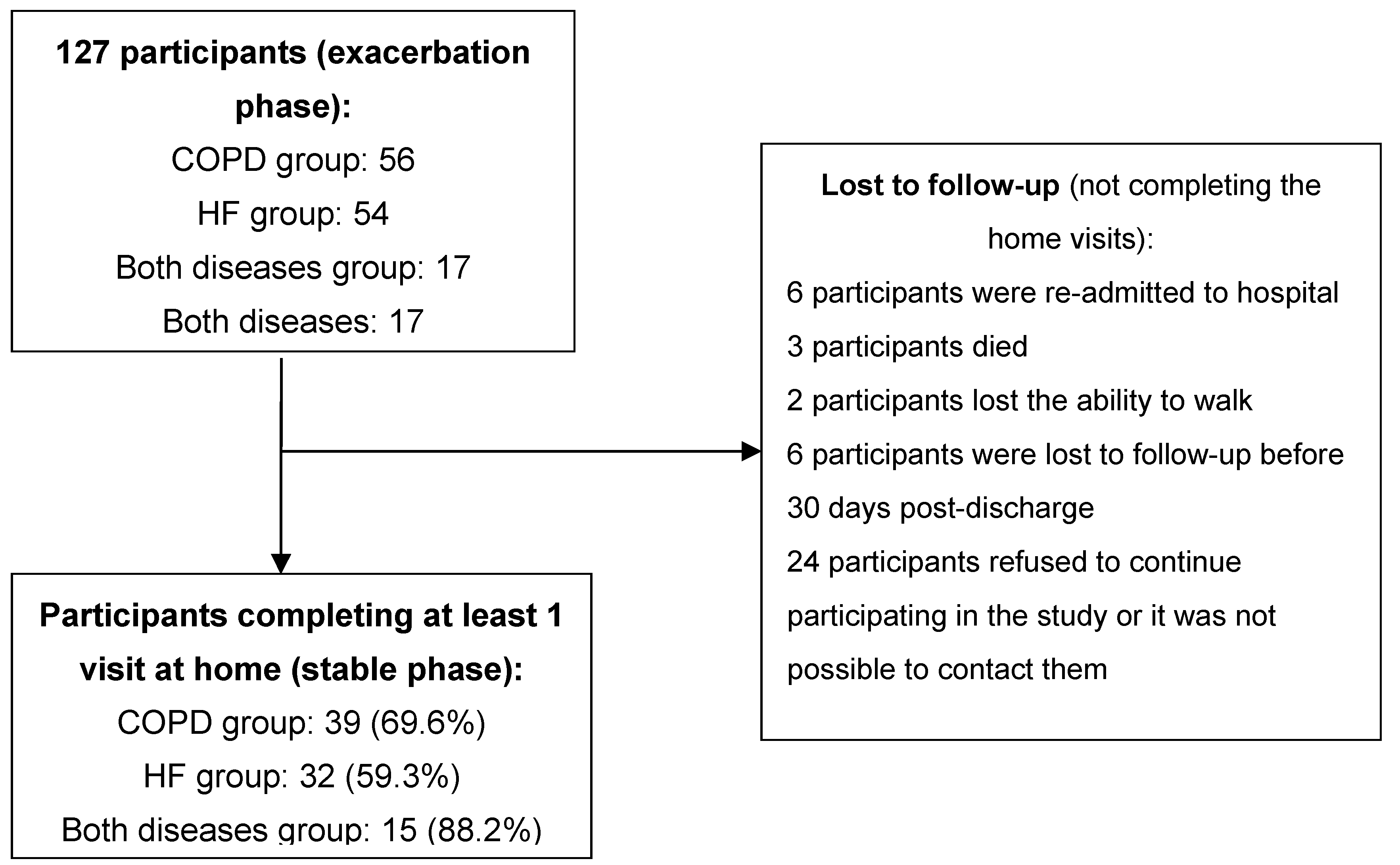
2.1. Design and Sample
2.2. Participants’ Evaluation and Variables
2.3. Statistical Analysis
3. Results
3.1. Demographics
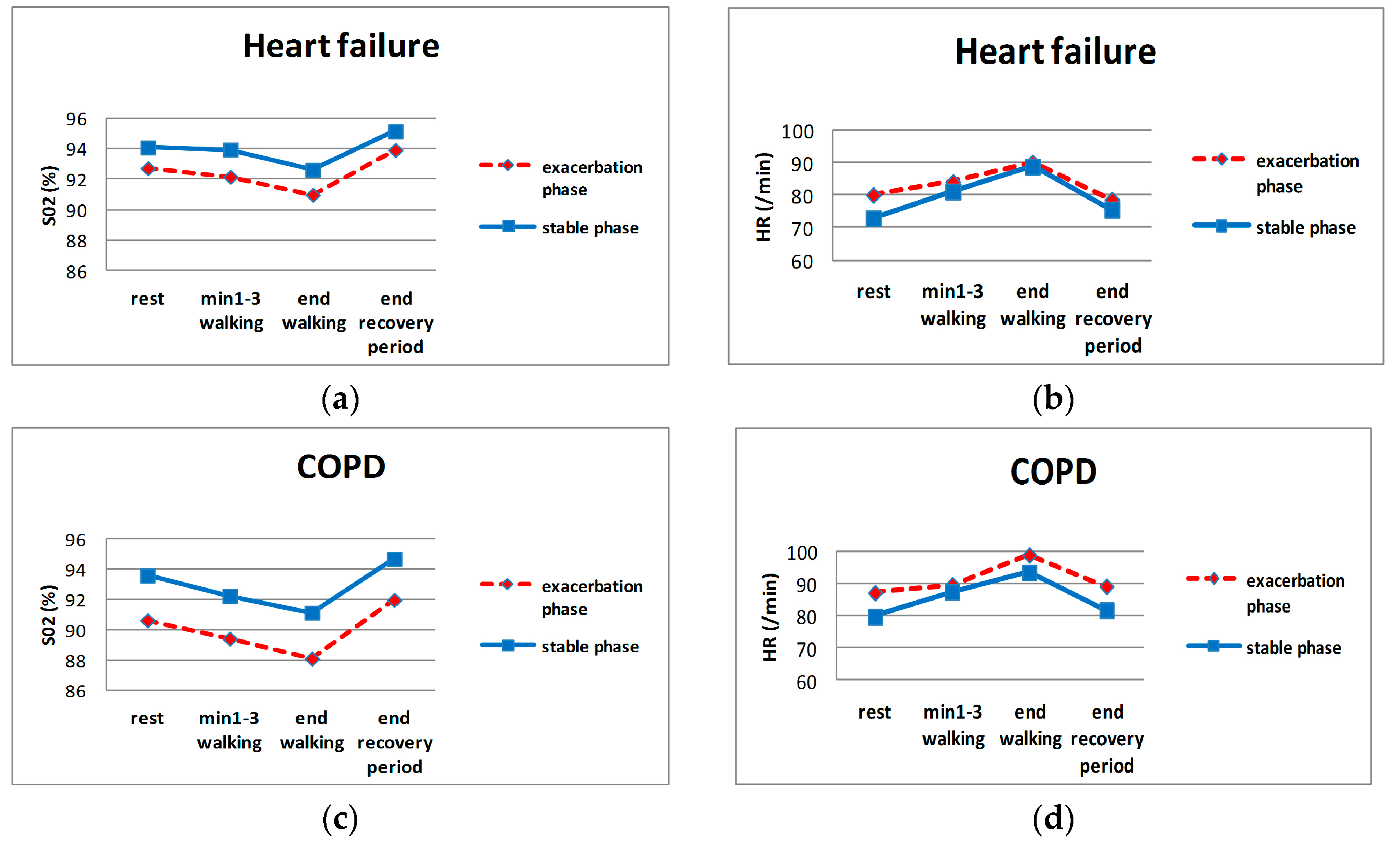
3.2. Mean and Diagnostic Performance of Individual Parameters
3.3. Diagnostic Performance of the Developed Algorithms
4. Discussion
4.1. Main Results
4.2. Clinical Usefulness/Feasibility
4.3. Validity/Bias
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Boult, C.; Altmann, M.; Gilbertson, D.; Yu, C.; Kane, R.L. Decreasing disability in the 21st century: The future effects of controlling six fatal and nonfatal conditions. Am. J. Public Health 1996, 86, 1388–1393. [Google Scholar] [CrossRef] [PubMed]
- Mannino, D.M. COPD: Epidemiology, prevalence, morbidity and mortality, and disease heterogeneity. Chest 2002, 121 (Suppl. 5), 121S–126S. [Google Scholar] [CrossRef]
- MuñizGarcía, J.; Crespo Leiro, M.G.; Castro Beiras, A. Epidemiology of heart failure in Spain and the importance of adhering to clinical practice guidelines. Rev. Esp. Cardiol. 2006, 6 (Suppl. F), 2–8. [Google Scholar]
- Anzueto, A.; Sethi, S.; Martinez, F.J. Exacerbations of chronic obstructive pulmonary disease. Proc. Am. Thorac. Soc. 2007, 4, 554–564. [Google Scholar] [CrossRef] [PubMed]
- Giamouzis, G.; Kalogeropoulos, A.; Georgiopoulou, V.; Laskar, S.; Smith, A.L.; Dunbar, S.; Triposkiadis, F.; Butler, J. Hospitalization epidemic in patients with heart failure: Risk factors, risk prediction, knowledge gaps, and future directions. J. Card. Fail. 2011, 17, 54–75. [Google Scholar] [CrossRef] [PubMed]
- Liao, L.; Allen, L.A.; Whellan, D.J. Economic burden of heart failure in the elderly. Pharmacoeconomics 2008, 26, 447–462. [Google Scholar] [CrossRef] [PubMed]
- Adamson, P.B.; Smith, A.L.; Abraham, W.T.; Kleckner, K.J.; Stadler, R.W.; Shih, A.; Rhodes, M.M. Continuous autonomic assessment in patients with symptomatic heart failure: Prognostic value of heart rate variability measured by an implanted cardiac resynchronization device. Circulation 2004, 110, 2389–2394. [Google Scholar] [CrossRef] [PubMed]
- Javed, F.; Farrugia, S.; Colefax, M.; Schindhelm, K. Early Warning of Acute Decompensation in Heart Failure Patients Using a Noncontact Measure of Stability Index. IEEE Trans. Biomed. Eng. 2016, 63, 438–448. [Google Scholar] [CrossRef]
- Masip, J.; Gayà, M.; Páez, J.; Betbesé, A.; Vecilla, F.; Manresa, R.; Ruíz, P. Pulse oximetry in the diagnosis of acute heart failure. Rev. Esp. Cardiol. (Engl. Ed.) 2012, 65, 879–884. [Google Scholar] [CrossRef]
- Zhang, J.; Goode, K.M.; Cuddihy, P.E.; Cleland, J.G.F. Predicting hospitalization due to worsening heart failure using daily weight measurement: Analysis of the Trans-European Network-Home-Care Management System (TEN-HMS) study. Eur. J. Heart Fail 2009, 11, 420–427. [Google Scholar] [CrossRef]
- Anand, I.S.; Tang, W.H.W.; Greenberg, B.H.; Chakravarthy, N.; Libbus, I.; Katra, R.P.; Music Investigators. Design and performance of a multisensor heart failure monitoring algorithm: Results from the multisensor monitoring in congestive heart failure (MUSIC) study. J. Card. Fail. 2012, 18, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Al Rajeh, A.M.; Hurst, J.R. Monitoring of Physiological Parameters to Predict Exacerbations of Chronic Obstructive Pulmonary Disease (COPD): A Systematic Review. J. Clin. Med. 2016, 5, 108. [Google Scholar] [CrossRef] [PubMed]
- Hurst, J.R.; Donaldson, G.C.; Quint, J.K.; Goldring, J.J.P.; Patel, A.R.C.; Wedzicha, J.A. Domiciliary pulse-oximetry at exacerbation of chronic obstructive pulmonary disease: Prospective pilot study. BMC Pulm. Med. 2010, 10, 52. [Google Scholar] [CrossRef] [PubMed]
- Van den Berge, M.; Hop, W.C.; van der Molen, T.; van Noord, J.A.; Creemers, J.P.; Schreurs, A.J.; Wouters, E.F.; Postma, D.S. Prediction and course of symptoms and lung function around an exacerbation in Chronic Obstructive Pulmonary Disease. Respir. Res. 2012, 13, 44. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.H.; Cichosz, S.L.; Dinesen, B.; Hejlesen, O.K. Moving prediction of exacerbation in chronic obstructive pulmonary disease for patients in telecare. J. Telemed. Telecare 2012, 18, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Yañez, A.M.; Guerrero, D.; Pérez de Alejo, R.; Garcia-Rio, F.; Alvarez-Sala, J.L.; Calle-Rubio, M.; de Molina, R.M.; Falcones, M.V.; Ussetti, P.; Sauleda, J.; et al. Monitoring breathing rate at home allows early identification of COPD exacerbations. Chest 2012, 142, 1524–1529. [Google Scholar] [CrossRef]
- Martín-Lesende, I.; Orruño, E.; Bilbao, A.; Vergara, I.; Cairo, M.C.; Bayón, J.C.; Reviriego, E.; Romo, M.I.; Larrañaga, J.; Asua, J.; et al. Impact of telemonitoring home care patients with heart failure or chronic lung disease from primary care on healthcare resource use (the TELBIL study randomised controlled trial). BMC Health Serv. Res. 2013, 13, 118. [Google Scholar] [CrossRef]
- Sund, Z.M.; Powell, T.; Greenwood, R.; Jarad, N.A. Remote daily real-time monitoring in patients with COPD—A feasibility study using a novel device. Respir. Med. 2009, 103, 1320–1328. [Google Scholar] [CrossRef]
- Hardinge, M.; Rutter, H.; Velardo, C.; Shah, S.A.; Williams, V.; Tarassenko, L.; Farmer, A. Using a mobile health application to support self-management in chronic obstructive pulmonary disease: A six-month cohort study. BMC Med. Inform. Decis. Mak. 2015, 15, 46. [Google Scholar] [CrossRef]
- Riis, H.C.; Jensen, M.H.; Cichosz, S.L.; Hejlesen, O.K. Prediction of exacerbation onset in chronic obstructive pulmonary disease patients. J. Med. Eng. Technol. 2016, 40, 1–7. [Google Scholar] [CrossRef]
- Mohktar, M.S.; Redmond, S.J.; Antoniades, N.C.; Rochford, P.D.; Pretto, J.J.; Basilakis, J.; Lovell, N.H.; McDonald, C.F. Predicting the risk of exacerbation in patients with chronic obstructive pulmonary disease using home telehealth measurement data. Artif. Intell. Med. 2015, 63, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Ledwidge, M.T.; O’Hanlon, R.; Lalor, L.; Travers, B.; Edwards, N.; Kelly, D.; Voon, V.; McDonald, K.M. Can individualized weight monitoring using the HeartPhone algorithm improve sensitivity for clinical deterioration of heart failure? Eur. J. Heart Fail. 2013, 15, 447–455. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.A.; Velardo, C.; Farmer, A.; Tarassenko, L. Exacerbations in Chronic Obstructive Pulmonary Disease: Identification and Prediction Using a Digital Health System. J. Med. Internet Res. 2017, 19, e69. [Google Scholar] [CrossRef] [PubMed]
- Gilliam, F.R., III; Ewald, G.A.; Sweeney, R.J. Feasibility of Automated Heart Failure Decompensation Detection Using Remote Patient Monitoring: Results from the Decompensation Detection Study. J. Innov. Cardiac. Rhythm. Manag. 2012, 3, 735–745. [Google Scholar]
- Cohen-Solal, A.; Logeart, D.; Guiti, C.; Dahan, M.; Gourgon, R. Cardiac and peripheral responses to exercise in patients with chronic heart failure. Eur. Heart J. 1999, 20, 931–945. [Google Scholar] [CrossRef] [PubMed]
- Bartels, M.N.; Jelic, S.; Ngai, P.; Basner, R.C.; DeMeersman, R.E. High-frequency modulation of heart rate variability during exercise in patients with COPD. Chest 2003, 124, 863–869. [Google Scholar] [CrossRef] [PubMed]
- Van Gestel, A.J.R.; Kohler, M.; Steier, J.; Sommerwerck, U.; Teschler, S.; Russi, E.W.; Teschler, H. Cardiac autonomic function and cardiovascular response to exercise in patients with chronic obstructive pulmonary disease. COPD J. Chronic Obstr. Pulm. Dis. 2012, 9, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Dolgin, M.; New York Heart Association. Nomenclature and Criteria for Diagnosis of Diseases of the Heart and Great Vessels/The Criteria Committee of the New York Heart Association, 9th ed.; Little, Brown: Boston, MA, USA, 1994; ISBN 0316605387. [Google Scholar]
- Fletcher, C. Standardised questionnaire on respiratory symptoms: A statement prepared and approved by the MRC Committee on the Aetiology of Chronic Bronchitis (MRC breathlessness score). BMJ 1960, 2, 1665. [Google Scholar]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Gordis, L. Epidemiology, 5th ed.; Elsevier Saunders: Philadelphia, PA, USA, 2014; pp. 88–115. [Google Scholar]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Bieri, D.; Reeve, R.A.; Champion, G.D.; Addicoat, L.; Ziegler, J.B. The Faces Pain Scale for the self-assessment of the severity of pain experienced by children: Development, initial validation, and preliminary investigation for ratio scale properties. Pain 1990, 41, 139–150. [Google Scholar] [CrossRef]
- Herr, K.A.; Mobily, P.R.; Kohout, F.J.; Wagenaar, D. Evaluation of the Faces Pain Scale for use with the elderly. Clin. J. Pain 1998, 14, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Burton, C.; Pinnock, H.; McKinstry, B. Changes in telemonitored physiological variables and symptoms prior to exacerbations of chronic obstructive pulmonary disease. J. Telemed. Telecare 2015, 21, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Alahmari, A.D.; Patel, A.R.C.; Kowlessar, B.S.; Mackay, A.J.; Singh, R.; Wedzicha, J.A.; Donaldson, G.C. Daily activity during stability and exacerbation of chronic obstructive pulmonary disease. BMC Pulm. Med. 2014, 14, 98. [Google Scholar] [CrossRef] [PubMed]
- Collins, S.P.; Thorn, M.; Nowak, R.M.; Levy, P.D.; Fermann, G.J.; Hiestand, B.C.; Cowart, T.D.; Venuti, R.P.; Hiatt, W.R.; Foo, S.; et al. Feasibility of Serial 6-min Walk Tests in Patients with Acute Heart Failure. J. Clin. Med. 2017, 6, 84. [Google Scholar] [CrossRef] [PubMed]
- McCabe, N.; Butler, J.; Dunbar, S.B.; Higgins, M.; Reilly, C. Six-minute walk distance predicts 30-day readmission after acute heart failure hospitalization. Heart Lung 2017, 46, 287–292. [Google Scholar] [CrossRef] [PubMed]
- Tabata, M.; Shimizu, R.; Kamekawa, D.; Kato, M.; Kamiya, K.; Akiyama, A.; Kamada, Y.; Tanaka, S.; Noda, C.; Masuda, T. Six-minute walk distance is an independent predictor of hospital readmission in patients with chronic heart failure. Int. Heart J. 2014, 55, 331–336. [Google Scholar] [CrossRef]
- Ingle, L.; Cleland, J.G.; Clark, A.L. The long-term prognostic significance of 6-minute walk test distance in patients with chronic heart failure. BioMed Res. Int. 2014, 2014, 505969. [Google Scholar] [CrossRef]
- Dajczman, E.; Wardini, R.; Kasymjanova, G.; Préfontaine, D.; Baltzan, M.A.; Wolkove, N. Six minute walk distance is a predictor of survival in patients with chronic obstructive pulmonary disease undergoing pulmonary rehabilitation. Can. Respir. J. 2015, 22, 225–229. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Crouch, R. Minimal clinically important difference for change in 6-minute walk test distance of adults with pathology: A systematic review. J. Eval. Clin. Pract. 2017, 23, 377–381. [Google Scholar] [CrossRef]
- Holland, A.E.; Spruit, M.A.; Troosters, T.; Puhan, M.A.; Pepin, V.; Saey, D.; McCormack, M.C.; Carlin, B.W.; Sciurba, F.C.; Pitta, F.; et al. An official European Respiratory Society/American Thoracic Society technical standard: Field walking tests in chronic respiratory disease. Eur. Respir. J. 2014, 44, 1428–1446. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| HF (n = 54) | COPD (n = 56) | Both (n = 17) | p | |
|---|---|---|---|---|
| Age (SD) | 78.4 (8.3) | 73.4(8.4) | 75.8(9.6) | 0.010 |
| Male (%) | 24 (44.4) | 43 (76.8) | 16 (94.1) | <0.01 |
| Diabetes mellitus 2 (%) | 27 (50.0) | 11 (19.6) | 6 (35.3) | 0.002 |
| Dyslipidemia (%) | 16 (29.6) | 21 (37.5) | 5 (29.4) | 0.707 |
| Active smoking (%) | 2 (3.7) | 13 (23.2) | 1 (5.9) | 0.008 |
| Treatment with bradycardia-inducing drug (previous to current exacerbation) (%) | 37 (68.5) | 7 (12.5) | 12 (70.6) | <0.01 |
| Previous hospitalization due to cardiac/respiratory disease (SD) | 0.9 (1.2) | 1.9 (1.9) | 1.7 (1.4) | 0.007 |
| Length of stay in days (SD) | 9 (8.1) | 11.3 (11.4) | 7.9 (7.0) | 0.445 |
| Baseline evaluation time (days previous to discharge) (SD) | 2.3 (3.8) | 3.8 (4.4) | 2.9 (2.7) | 0.299 |
| Dyspnea (NYHA) (%) | ||||
| I | 16 (29.6) | 16 (28.6) | 5 (29.4) | 0.924 |
| II | 22 (40.7) | 20 (35.7) | 8 (47.1) | |
| III | 16 (29.6) | 20 (35.7) | 4 (23.5) | |
| Dyspnea (mMRC) (%) | ||||
| 0 | 12 (22.2) | 14 (25) | 4 (23.5) | 0.391 |
| 1 | 6 (11.1) | 9 (16.1) | 2 (11.8) | |
| 2 | 13 (24.1) | 16 (28.6) | 4 (23.5) | |
| 3 | 23 (42.6) | 17 (30.4) | 7 (41.2) | |
| Body mass index (SD) | 26.7 (4.6) | 25.2 (4.4) | 26.8 (8.2) | 0.235 |
| Osteoarthritis (%) | 35 (64.8) | 25 (44.6) | 7 (41.2) | 0.055 |
| Clinical Parameter | HF | COPD | ||||||
|---|---|---|---|---|---|---|---|---|
| Exacerb. Phase (SD) | Stable Phase (SD) | Mean Difference (95% CI) | p | Exacerb. phase (SD) | Stable Phase (SD) | Mean Difference (95% CI) | p | |
| Oxygen saturation (%) | ||||||||
| Rest | 92.7 (3.4) | 94.1 (3.2) | −1.36 (−2.42; −0.3) | 0.01 | 90.6 (3.2) | 93.6 (2.6) | −2.96 (−3.77; −2.16) | <0.001 |
| Minute 1 to 3 of effort (mean) | 92.2 (3.6) | 94 (3.1) | −1.79 (−2.65; −0.93) | <0.001 | 89.4 (3.9) | 92.2 (3.2) | −2.84 (−3.91; −1.77) | <0.001 |
| End-of-effort | 91 (5.6) | 92.6 (4.1) | −1.64 (−2.82; −0.46) | 0.01 | 88.1 (5.1) | 91.1 (4.3) | −3.04 (−4.16; −1.91) | <0.001 |
| Mean-of-effort period | 91.2 (3.7) | 92.8 (3.4) | −1.63 (−2.45; −0.81) | <0.001 | 88.7 (3.7) | 91.3 (3.5) | −2.57 (−3.42; −1.72) | <0.001 |
| End-of-recovery | 93.9 (2.9) | 95.1 (2.5) | −1.23 (−1.96; −0.51) | <0.001 | 92 (3.1) | 94.7 (2.5) | −2.72 (−3.56; −1.87) | <0.001 |
| Mean of recovery period | 92.3 (3.4) | 93.7 (3.2) | −1.42 (−2.28; −0.57) | <0.001 | 90.5 (3.5) | 93 (3.1) | −2.48 (−3.39; −1.57) | <0.001 |
| Heart rate (beats/min) (1) | ||||||||
| Rest | 80.1 (12.2) | 72.9 (11.4) | 7.22 (2.11; 12.33) | 0.01 | 87.3 (15.4) | 79.9 (14.5) | 7.4 (3.05; 11.74) | <0.001 |
| Minute 1 to 3 of effort (mean) | 84.1 (9.9) | 81.2 (13.9) | 2.95 (−2.6; 8.49) | 0.29 | 89.8 (14.6) | 87.5 (16.8) | 2.21 (−3.45; 7.88) | 0.43 |
| End-of-effort | 90.2 (12.3) | 88.9 (16.1) | 1.28 (−4.91; 7.47) | 0.68 | 99 (16.2) | 93.6 (16.8) | 5.42 (0.84; 9.99) | 0.02 |
| Mean-of-effort period | 87.2 (9.5) | 83.2 (13.1) | 3.97 (−0.74; 8.68) | 0.1 | 93.3 (12.4) | 89.8 (14.7) | 3.47 (−1.18; 8.11) | 0.14 |
| End-of-recovery | 78.7 (14.6) | 75.6 (13.3) | 3.06 (−2.13; 8.24) | 0.24 | 89.3 (14.9) | 81.9 (13.2) | 7.4 (3.05; 11.76) | <0.001 |
| Mean of recovery period | 83.5 (11.6) | 80 (13.9) | 3.5 (−2.01; 9.01) | 0.21 | 89.4 (13.6) | 86.2 (14.4) | 3.19 (−1.42; 7.8) | 0.17 |
| Respiratory rate (breaths/min) | ||||||||
| Rest | 21.4 (5.1) | 20.8 (4.5) | 0.57 (−0.74; 1.88) | 0.38 | 21.2 (5.1) | 21.2 (4.6) | 0.02 (−0.92; 0.95) | 0.97 |
| End-of-effort | 24.5 (5.3) | 23.6 (5.3) | 0.85 (−0.43; 2.13) | 0.19 | 24.7 (5.6) | 23.9 (5) | 0.85 (−0.07; 1.77) | 0.07 |
| End-of-recovery | 22 (5.5) | 21.3 (4.7) | 0.65 (−0.78; 2.08) | 0.36 | 22.5 (4.6) | 21.3 (4.1) | 1.19 (0.21; 2.17) | 0.02 |
| Distance (m) | ||||||||
| Walking distance | 126.7 (89.8) | 133.1 (82.5) | −6.36 (−31.3; 18.57) | 0.61 | 134.1 (93.8) | 157.9 (100.2) | −23.78 (−49.99; 2.42) | 0.07 |
| Dyspnea | ||||||||
| NYHA scale | 2.1 (0.9) | 1.9 (0.7) | 0.17 (−0.05; 0.39) | 0.13 | 2.1 (0.9) | 1.8 (0.7) | 0.28 (0.01; 0.55) | 0.04 |
| mMRC scale | 2 (1.2) | 1.7 (1.1) | 0.28 (−0.02; 0.57) | 0.06 | 1.7 (1.4) | 1.5 (1.3) | 0.24 (−0.15; 0.63) | 0.22 |
| Borg scale (rest) | 1.7 (1.3) | 1.7 (1.5) | −0.09 (−0.61; 0.44) | 0.75 | 1.6 (1.3) | 1.6 (1.3) | 0.04 (−0.45; 0.52) | 0.88 |
| Borg scale (effort) | 2.7 (1.9) | 3.1 (2.4) | −0.43 (−1.2; 0.35) | 0.27 | 3.3 (2.5) | 2.9 (2.4) | 0.41 (−0.45; 1.27) | 0.35 |
| Blood pressure | ||||||||
| Systolic pressure | 120.1 (19.6) | 125.1 (23.6) | −5.04 (−10.75; 0.66) | 0.08 | 125.4 (18.3) | 126.7 (20.3) | −1.28 (−6.85; 4.29) | 0.65 |
| Diastolic pressure | 70.4 (13.3) | 70 (13.4) | 0.38 (−3.77; 4.53) | 0.85 | 73.8 (10.8) | 73.7 (12.1) | 0.07 (−3.33; 3.48) | 0.97 |
| Clinical Parameter | Cutpoint (2) | HF | COPD | ||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Sn (95% CI) | n | Sp (95% CI) | n | Sn (95% CI) | n | Sp (95% CI) | ||
| Oxygen saturation (%) | |||||||||
| Rest | ≥1 | 54 | 0.85 (0.73–0.92) | 46 | 0.72 (0.57–0.83) | ||||
| 2 | 47 | 0.53 (0.39–0.67) | 43 | 0.86 (0.73–0.93) | |||||
| 3 | 47 | 0.34 (0.22–0.48) | 43 | 0.95 (0.85–0.99) | |||||
| Minute 1 to 3 of effort (mean) | 2 | 35 | 0.4 (0.26–0.56) | 33 | 0.91 (0.76–0.97) | 35 | 0.57 (0.41–0.72) | 29 | 0.93 (0.78–0.98) |
| End-of-effort | 3 | 54 | 0.5 (0.37–0.63) | 46 | 0.87 (0.74–0.94) | ||||
| Mean-of-effort period | 2 | 46 | 0.46 (0.32–0.6) | 40 | 0.88 (0.74–0.95) | ||||
| End-of-recovery | 2 | 47 | 0.51 (0.37–0.65) | 43 | 0.88 (0.76–0.95) | ||||
| 3 | 47 | 0.28 (0.17–0.42) | 43 | 0.95 (0.85–0.99) | 53 | 0.53 (0.4–0.66) | 46 | 0.89 (0.77–0.95) | |
| Mean of recovery period | 2 | 45 | 0.47 (0.33–0.61) | 40 | 0.88 (0.74–0.95) | ||||
| 3 | 45 | 0.31 (0.2–0.46) | 40 | 0.93 (0.8–0.97) | 48 | 0.44 (0.31–0.58) | 38 | 0.89 (0.76–0.96) | |
| Heart rate (beats/min) | |||||||||
| Rest | ≥10 | 36 | 0.42 (0.27–0.58) | 32 | 0.84 (0.68–0.93) | ||||
| 15 | 36 | 0.36 (0.22–0.52) | 32 | 0.91 (0.76–0.97) | 48 | 0.31 (0.2–0.45) | 41 | 0.95 (0.84–0.99) | |
| Minute 1 to 3 of effort (mean) | 10 | 31 | 0.42 (0.26–0.59) | 26 | 0.92 (0.76–0.98) | 33 | 0.3 (0.17–0.47) | 27 | 0.93 (0.77–0.98) |
| End-of-effort | 10 | 48 | 0.4 (0.27–0.54) | 41 | 0.93 (0.81–0.97) | ||||
| Mean-of-effort period | 10 | 35 | 0.4 (0.26–0.56) | 29 | 0.97 (0.83–0.99) | ||||
| Mean of recovery period | 10 | 34 | 0.35 (0.21–0.52) | 29 | 0.93 (0.78–0.98) | ||||
| 15 | 34 | 0.26 (0.15–0.43) | 29 | 1 (0.88–1) | |||||
| Walking distance (m) | |||||||||
| Walking distance difference | ≥35 | 44 | 0.34 (0.22–0.49) | 42 | 0.95 (0.84–0.99) | 51 | 0.43 (0.31–0.57) | 46 | 0.93 (0.82–0.98) |
| 40 | 44 | 0.34 (0.22–0.49) | 42 | 0.98 (0.88–1) | |||||
| Disease | Clinical Parameter | Cutpoint | n | Sn (95% CI) | n | Sp (95% CI) | ROC Area (95% CI) |
|---|---|---|---|---|---|---|---|
| HF | Oxygen saturation decrease (mean-of-effort period) of at least 2 points; | at least 1 condition | 33 | 0.85 (0.69–0.93) | 28 | 0.75 (0.57–0.87) | 0.841 (0.741–0.941) |
| heart rate increase (mean-of-effort period) of at least 10 beats/min; | |||||||
| Walking distance decrease of at least 40 m | |||||||
| COPD | oxygen saturation decrease (average of minute 1 to 3 of effort period) of at least 2 points | at least 1 condition | 31 | 0.9 (0.75–0.97) | 27 | 0.89 (0.72–0.96) | 0.921 (0.847–0.995) |
| heart rate increase (end-of-effort) of at least 10 beats/min | |||||||
| Walking distance decrease of at least 35 m |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gálvez-Barrón, C.; Villar-Álvarez, F.; Ribas, J.; Formiga, F.; Chivite, D.; Boixeda, R.; Iborra, C.; Rodríguez-Molinero, A. Effort Oxygen Saturation and Effort Heart Rate to Detect Exacerbations of Chronic Obstructive Pulmonary Disease or Congestive Heart Failure. J. Clin. Med. 2019, 8, 42. https://doi.org/10.3390/jcm8010042
Gálvez-Barrón C, Villar-Álvarez F, Ribas J, Formiga F, Chivite D, Boixeda R, Iborra C, Rodríguez-Molinero A. Effort Oxygen Saturation and Effort Heart Rate to Detect Exacerbations of Chronic Obstructive Pulmonary Disease or Congestive Heart Failure. Journal of Clinical Medicine. 2019; 8(1):42. https://doi.org/10.3390/jcm8010042
Chicago/Turabian StyleGálvez-Barrón, César, Felipe Villar-Álvarez, Jesús Ribas, Francesc Formiga, David Chivite, Ramón Boixeda, Cristian Iborra, and Alejandro Rodríguez-Molinero. 2019. "Effort Oxygen Saturation and Effort Heart Rate to Detect Exacerbations of Chronic Obstructive Pulmonary Disease or Congestive Heart Failure" Journal of Clinical Medicine 8, no. 1: 42. https://doi.org/10.3390/jcm8010042
APA StyleGálvez-Barrón, C., Villar-Álvarez, F., Ribas, J., Formiga, F., Chivite, D., Boixeda, R., Iborra, C., & Rodríguez-Molinero, A. (2019). Effort Oxygen Saturation and Effort Heart Rate to Detect Exacerbations of Chronic Obstructive Pulmonary Disease or Congestive Heart Failure. Journal of Clinical Medicine, 8(1), 42. https://doi.org/10.3390/jcm8010042