Influence of Traditional Cardiovascular Risk Factors on Carotid and Femoral Atherosclerotic Plaque Volume as Measured by Three-Dimensional Ultrasound

Abstract
:1. Introduction
2. Methods
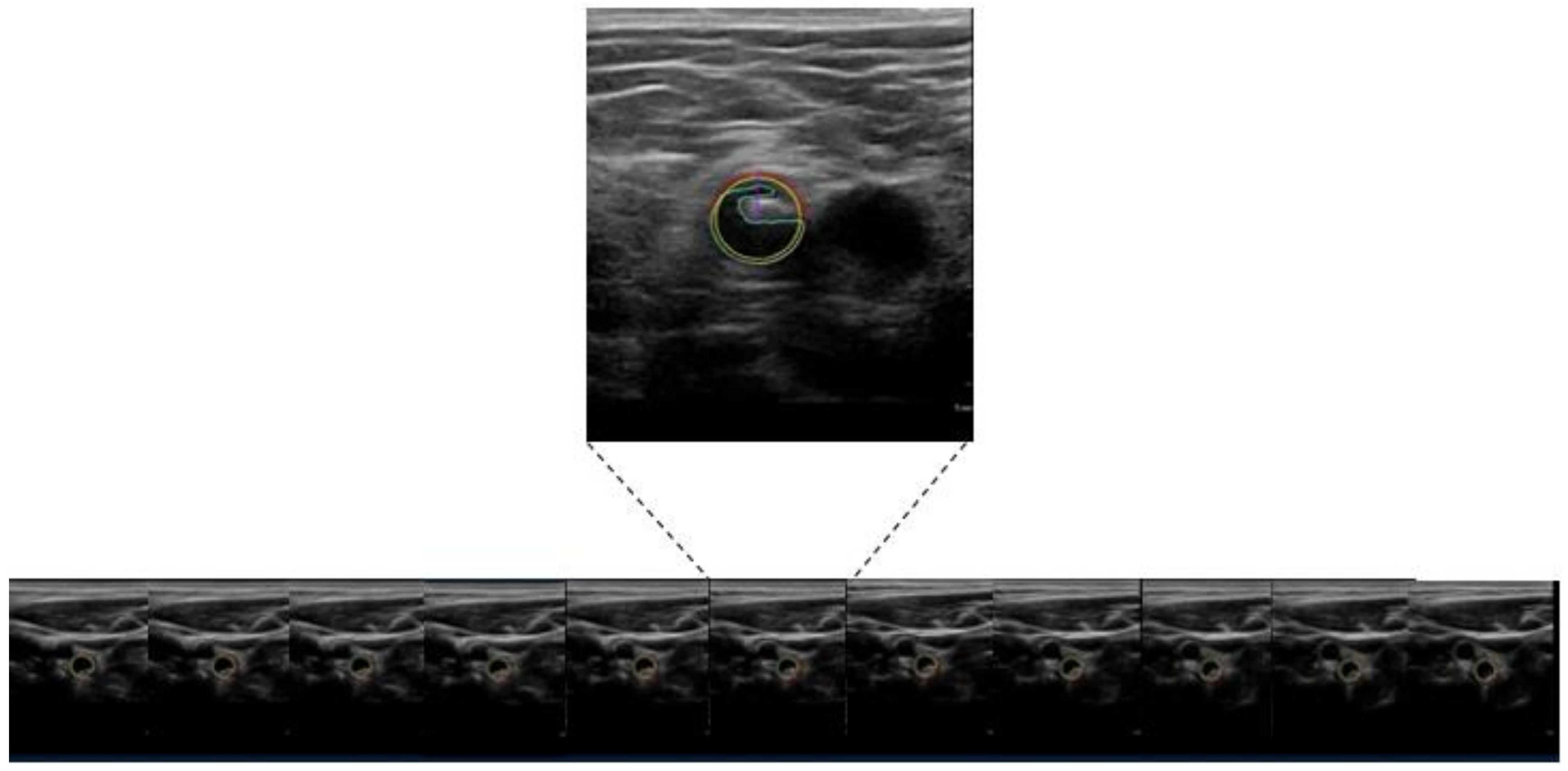
2.1. Ultrasound Imaging
2.2. Statistical Analysis
3. Results
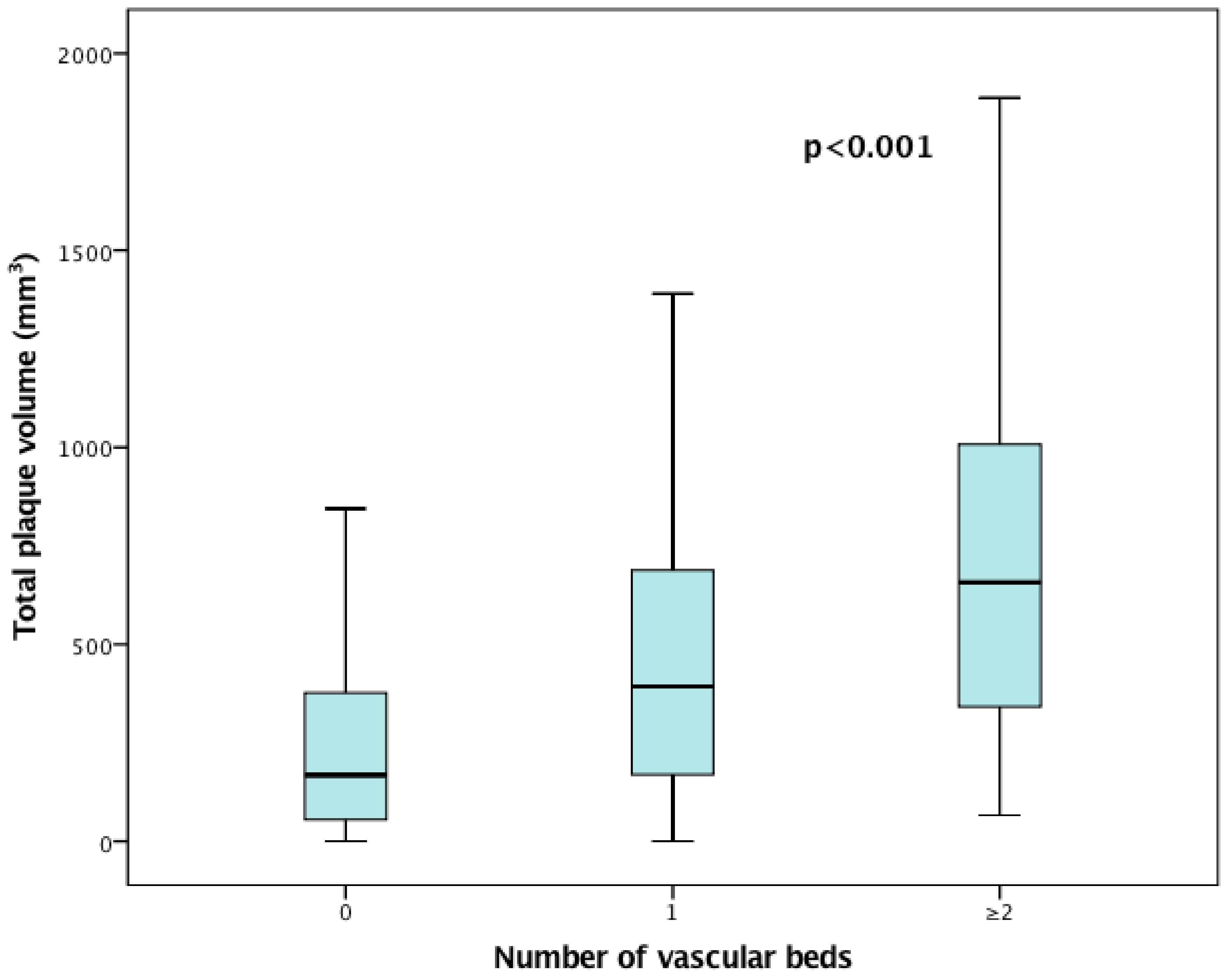
3.1. Influence of the Number of Risk Factors on the Extent of Plaque Volume
3.2. Distribution of Atherosclerotic Plaque Volume According to Cardiovascular Disease
3.3. Relationship of Smoking Expressed in Pack-Years and Atherosclerotic Plaque Volume
3.4. Association of CVRF, Cardiovascular Diseases and Plaque Volume
4. Discussion
4.1. Strengths
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Gallino, A.; Stuber, M.; Crea, F.; Falk, E.; Corti, R.; Lekakis, J.; Schwitter, J.; Camici, P.; Gaemperli, O.; Di Valentino, M.; et al. “In vivo” imaging of atherosclerosis. Atherosclerosis 2012, 224, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Polak, J.F.; Pencina, M.J.; Pencina, K.M.; O’Donnell, C.J.; Wolf, P.A.; D’Agostino, R.B., Sr. Carotid-wall intima-media thickness and cardiovascular events. N. Engl. J. Med. 2011, 365, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, M.W.; Markus, H.S.; Bots, M.L.; Rosvall, M.; Sitzer, M. Prediction of clinical cardiovascular events with carotid intima-media thickness: a systematic review and meta-analysis. Circulation 2007, 115, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Lorenz, M.W.; Schaefer, C.; Steinmetz, H.; Sitzer, M. Is carotid intima media thickness useful for individual prediction of cardiovascular risk? Ten-year results from the Carotid Atherosclerosis Progression Study (CAPS). Eur. Heart J. 2010, 31, 2041–2048. [Google Scholar] [CrossRef] [PubMed]
- Goff, D.C., Jr.; Lloyd-Jones, D.M.; Bennett, G.; Coady, S.; D’Agostino, R.B.; Gibbons, R.; Greenland, P.; Lackland, D.T.; Levy, D.; O’Donnell, C.J.; et al. 2013 ACC/AHA guideline on the assessment of cardiovascular risk: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines. Circulation 2014, 129, S49–S73. [Google Scholar] [CrossRef]
- Mathiesen, E.B.; Johnsen, S.H.; Wilsgaard, T.; Bonaa, K.H.; Lochen, M.L.; Njolstad, I. Carotid plaque area and intima-media thickness in prediction of first-ever ischemic stroke: A 10-year follow-up of 6584 men and women: The Tromso Study. Stroke 2011, 42, 972–978. [Google Scholar] [CrossRef]
- Inaba, Y.; Chen, J.A.; Bergmann, S.R. Carotid plaque, compared with carotid intima-media thickness, more accurately predicts coronary artery disease events: A meta-analysis. Atherosclerosis 2012, 220, 128–133. [Google Scholar] [CrossRef]
- Plichart, M.; Celermajer, D.S.; Zureik, M.; Helmer, C.; Jouven, X.; Ritchie, K.; Tzourio, C.; Ducimetiere, P.; Empana, J.P. Carotid intima-media thickness in plaque-free site, carotid plaques and coronary heart disease risk prediction in older adults. The three-city study. Atherosclerosis 2011, 219, 917–924. [Google Scholar] [CrossRef]
- Nambi, V.; Chambless, L.; Folsom, A.R.; He, M.; Hu, Y.; Mosley, T.; Volcik, K.; Boerwinkle, E.; Ballantyne, C.M. Carotid intima-media thickness and presence or absence of plaque improves prediction of coronary heart disease risk: the ARIC (Atherosclerosis Risk In Communities) study. J. Am. Coll. Cardiol. 2010, 55, 1600–1607. [Google Scholar] [CrossRef]
- Schwaiger, J.P.; Lamina, C.; Neyer, U.; Konig, P.; Kathrein, H.; Sturm, W.; Lhotta, K.; Grochenig, E.; Dieplinger, H.; Kronenberg, F. Carotid plaques and their predictive value for cardiovascular disease and all-cause mortality in hemodialysis patients considering renal transplantation: A decade follow-up. Am. J. Kidney Dis. 2006, 47, 888–897. [Google Scholar] [CrossRef] [PubMed]
- Arnold, J.A.; Modaresi, K.B.; Thomas, N.; Taylor, P.R.; Padayachee, T.S. Carotid plaque characterization by duplex scanning: Observer error may undermine current clinical trials. Stroke 1999, 30, 61–65. [Google Scholar] [CrossRef] [PubMed]
- Belcaro, G.; Nicolaides, A.N.; Ramaswami, G.; Cesarone, M.R.; De Sanctis, M.; Incandela, L.; Ferrari, P.; Geroulakos, G.; Barsotti, A.; Griffin, M.; et al. Carotid and femoral ultrasound morphology screening and cardiovascular events in low risk subjects: A 10-year follow-up study (the CAFES-CAVE study(1)). Atherosclerosis 2001, 156, 379–387. [Google Scholar] [CrossRef]
- Spence, J.D.; Eliasziw, M.; DiCicco, M.; Hackam, D.G.; Galil, R.; Lohmann, T. Carotid plaque area: A tool for targeting and evaluating vascular preventive therapy. Stroke 2002, 33, 2916–2922. [Google Scholar] [CrossRef] [PubMed]
- Ainsworth, C.D.; Blake, C.C.; Tamayo, A.; Beletsky, V.; Fenster, A.; Spence, J.D. 3D ultrasound measurement of change in carotid plaque volume: A tool for rapid evaluation of new therapies. Stroke 2005, 36, 1904–1909. [Google Scholar] [CrossRef] [PubMed]
- Johri, A.M.; Chitty, D.W.; Matangi, M.; Malik, P.; Mousavi, P.; Day, A.; Gravett, M.; Simpson, C. Can carotid bulb plaque assessment rule out significant coronary artery disease? A comparison of plaque quantification by two- and three-dimensional ultrasound. J. Am. Soc. Echocardiogr. 2013, 26, 86–95. [Google Scholar] [CrossRef] [PubMed]
- Sillesen, H.; Muntendam, P.; Adourian, A.; Entrekin, R.; Garcia, M.; Falk, E.; Fuster, V. Carotid plaque burden as a measure of subclinical atherosclerosis: comparison with other tests for subclinical arterial disease in the High Risk Plaque BioImage study. JACC Cardiovasc. Imaging 2012, 5, 681–689. [Google Scholar] [CrossRef]
- Gotto, A.M., Jr.; Moon, J.E. Management of cardiovascular risk: The importance of meeting lipid targets. Am. J. Cardiol. 2012, 110, 3–14. [Google Scholar] [CrossRef]
- Ferri, N.; Paoletti, R.; Corsini, A. Biomarkers for atherosclerosis: Pathophysiological role and pharmacological modulation. Curr. Opin. Lipidol. 2006, 17, 495–501. [Google Scholar] [CrossRef]
- Lopez-Melgar, B.; Fernandez-Friera, L.; Oliva, B.; Garcia-Ruiz, J.M.; Penalvo, J.L.; Gomez-Talavera, S.; Sánchez-González, J.; Mendiguren, J.M.; Ibáñez, B.; Fernández-Ortiz, A.; et al. Subclinical atherosclerosis burden by 3D ultrasound in mid-life: The PESA study. J. Am. Coll. Cardiol. 2017, 70, 301–313. [Google Scholar] [CrossRef]
- D’Agostino, R.B., Sr.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General cardiovascular risk profile for use in primary care: The Framingham Heart study. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef] [PubMed]
- Touboul, P.J.; Hennerici, M.G.; Meairs, S.; Adams, H.; Amarenco, P.; Bornstein, N.; Csiba, L.; Desvarieux, M.; Ebrahim, S.; Hernandez Hernandez, R.; et al. Mannheim carotid intima-media thickness and plaque consensus (2004-2006-2011). An update on behalf of the advisory board of the 3rd, 4th and 5th watching the risk symposia, at the 13th, 15th and 20th European Stroke Conferences, Mannheim, Germany, 2004, Brussels, Belgium, 2006, and Hamburg, Germany, 2011. Cerebrovasc. Dis. 2012, 34, 290–296. [Google Scholar] [PubMed]
- Massey, F.J. The Kolmogorov-Smirnov test for goodness of fit. J. Am. Stat. Assoc. 1951, 46, 68–78. [Google Scholar] [CrossRef]
- Yerly, P.; Rodondi, N.; Viswanathan, B.; Riesen, W.; Vogt, P.; Bovet, P. Association between conventional risk factors and different ultrasound-based markers of atherosclerosis at carotid and femoral levels in a middle-aged population. Int. J. Cardiovasc. Imaging 2013, 29, 589–599. [Google Scholar] [CrossRef] [PubMed]
- Laclaustra, M.; Casasnovas, J.A.; Fernandez-Ortiz, A.; Fuster, V.; Leon-Latre, M.; Jimenez-Borreguero, L.J.; Pocovi, M.; Hurtado-Roca, Y.; Ordovas, J.M.; Jarauta, E.; et al. Femoral and Carotid Subclinical Atherosclerosis Association With Risk Factors and Coronary Calcium: The AWHS Study. J. Am. Coll. Cardiol. 2016, 67, 1263–1274. [Google Scholar] [CrossRef] [PubMed]
- Kerenyi, L.; Mihalka, L.; Csiba, L.; Bacso, H.; Bereczki, D. Role of hyperlipidemia in atherosclerotic plaque formation in the internal carotid artery. J. Clin. Ultrasound 2006, 34, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Baber, U.; Mehran, R.; Sartori, S.; Schoos, M.M.; Sillesen, H.; Muntendam, P.; Garcia, M.J.; Gregson, J.; Pocock, S.; Falk, E.; et al. Prevalence, impact, and predictive value of detecting subclinical coronary and carotid atherosclerosis in asymptomatic adults: The BioImage study. J. Am. Coll. Cardiol. 2015, 65, 1065–1074. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Total Population (n = 404) | Low Total Plaque Volume (n = 202, 50%, 0–255 mm3) | High Total Plaque Volume (n = 202, 50%, 256–2048 mm3) | p Value | |
|---|---|---|---|---|
| Age, years | 64 (56–71) | 60 (54–67) | 67 (60–74) | <0.001 |
| Female, n (%) | 174 (43.1) | 104 (51.5) | 70 (34.7) | 0.001 |
| Body mass index, kg/m2 | 25.4 (23.5–28.2) | 25.3 (23.2–28.3) | 25.8 (23.9–28.2) | 0.483 |
| Hypertension, n (%) | 264 (65.3) | 107 (53) | 157 (77.7) | <0.001 |
| Family history for CV-disease, n (%) | 96 (23.8) | 58 (28.7) | 38 (18.8) | 0.020 |
| Smoking (pack years) | 12 (± 18.5) | 8.7 (± 14.9) | 15.3 (±21) | 0.010 |
| Hyperlipidaemia, n (%) | 354 (87.6) | 175 (86.6) | 179 (88.6) | 0.546 |
| Diabetes mellitus, n (%) | 51 (12.6) | 20 (9.9) | 31 (15.3) | 0.100 |
| Framingham risk score, (%) | 12.8 (7.5–21.6) | 9.4 (5.3–16) | 17.1 (9.8–26.3) | <0.001 |
| hs-CRP, mg/dL | 0.18 (0.09–0.37) | 0.16 (0.08–0.35) | 0.21 (0.09–0.42) | 0.031 |
| Total cholesterol, mg/dL | 193 (164.3–225) | 199 (173.3–232.5) | 183.5 (158.3–213) | 0.003 |
| LDL-cholesterol, mg/dL | 115 (91–146) | 120 (97.3–150) | 109 (86–138.8) | 0.009 |
| HDL-cholesterol, mg/dL | 58 (47–73) | 61 (48.3–76) | 56 (45–67.8) | 0.009 |
| Triglyceride, mg/dL | 129 (94–179.8) | 122 (83.3–171.5) | 135 (97.3–190.8) | 0.030 |
| Creatinine, mg/dL | 0.94 (0.83–1.08) | 0.91 (0.82-1.02) | 0.98 (0.83–1.12) | 0.003 |
| Lipid lowering therapy | 234 (58.1) | 103 (51) | 131 (64.9) | 0.005 |
| Antihypertensive therapy | 238 (59.1) | 100 (49.5) | 138 (68.3) | <0.001 |
| Antidiabetic therapy | 47 (11.7) | 18 (8.9) | 29 (14.4) | 0.088 |
| Total Population (n = 404) | Low Total Plaque Volume (n = 202, 50%) | High Total Plaque Volume (n = 202, 50%) | p Value | |
|---|---|---|---|---|
| CAD, n (%) | 122 (30.2) | 41 (20.3) | 81 (40.1) | <0.001 |
| CVD, n (%) | 39 (9.7) | 14 (6.9) | 25 (12.4) | 0.064 |
| PAD, n (%) | 32 (7.9) | 5 (2.5) | 27 (13.4) | <0.001 |
| Any vascular disease, n (%) | 155 (38.4) | 53 (26.2) | 102 (50.5) | <0.001 |
| No vascular disease, n (%) | 249 (61.6) | 149 (59.8) | 100 (40.2) | <0.001 |
| Total Population (n = 404) | Low Total Plaque Volume (n = 202, 50%) | High Total Plaque Volume (n = 202, 50%) | p Value | |
|---|---|---|---|---|
| Total plaque volume, mm3 | 255.5 (83.1–514) | 83.3 (22–156.8) | 513 (371.5–772.8) | <0.001 |
| Femoral plaque volume, mm3 | 139.5 (28.3–284) | 39.5 (0–98.8) | 283 (188–481.8) | <0.001 |
| Carotid plaque volume, mm3 | 79.5 (12.3–240.3) | 19.5 (0–56.5) | 239.5 (109–403.5) | <0.001 |
| Femoral IMT, mm | 0.48 (0.44–0.53) | 0. 47 (0.42–0.52) | 0.50 (0.45–0.54) | <0.001 |
| Carotid IMT, mm | 0.72 (0.62–0.82) | 0.68 (0.60–0.78) | 0.75 (0.68–0.85) | <0.001 |
| Ankle-brachial index | 0.91 (±0.10) | 0.93 (±0.10) | 0.89 (±0.10) | 0.002 |
| Pulse wave velocity, m/s | 5.8 (4.8–7.1) | 5.5 (4.7–6.8) | 6.1 (4.8–7.4) | 0.012 |
| Total Plaque Volume | Femoral Paque Volume | Carotid Plaque Volume | ||
|---|---|---|---|---|
| n (%) | Median (IQR), mm3 | Median (IQR), mm3 | Median (IQR), mm3 | |
| 1 CVRF | n = 123,31 | 152 (58–360) | 79 (14–226) | 35 (5–160) |
| 2 CVRF | n = 187,47 | 257 (83–506) | 144 (29–290) | 87 (11–222) |
| ≥ 3 CVRF | n = 88,22 | 448 (167–701) | 215 (84–445) | 139 (52–351) |
| Total Plaque Volume | Femoral Plaque Volume | Carotid Plaque Burden | |
|---|---|---|---|
| Median (IQR), mm3 | Median (IQR), mm3 | Median (IQR), mm3 | |
| Smokers (n = 102) | 362 (91–666) | 196 (55–396) | 73 (12–283) |
| Non-smokers (n = 302) | 240 (72–496) | 124 (21–253) | 81 (13–223) |
| <30 pack-years (n = 119) | 226 (50–522) | 125 (15–298) | 63 (5–250) |
| 31–60 pack-years (n = 55) | 393 (145–672) | 234 (103–420) | 120 (27–275) |
| >60 pack-years (n = 6) | 706 (333–1079) | 443 (164–819) | 195 (110–402) |
| High Total Plaque Volume | High Femoral Plaque Volume | High Carotid Plaque Volume | ||||
|---|---|---|---|---|---|---|
| Multivariate proportional odds | OR (95CI) | p value | OR (95CI) | p value | OR (95CI) | p value |
| Smoking | 2.68 (1.52–4.71) | 0.001 | 2.69(1.57–4.62) | <0.001 | 1.50 (0.86–2.63) | 0.154 |
| Hypertension | 1.95 (1.17–3.25) | 0.010 | 1.91 (1.17–3.11) | 0.010 | 1.89 (1.12–3.19) | 0.016 |
| Hyperlipidaemia | 1.02 (0.52–2.01) | 0.945 | 0.95 (0.50–1.83) | 0.886 | 2.23 (1.09–4.55) | 0.028 |
| Diabetes | 1.21 (0.60–2.46) | 0.594 | 0.70 (0.36–1.38) | 0.306 | 1.34 (0.65–2.74) | 0.428 |
| Family history of CV disease | 0.63 (0.37–1.09) | 0.097 | 1.05 (0.63–1.75) | 0.865 | 0.45 (0.26–0.78) | 0.005 |
| Age | 1.09 (1.06–1.12) | <0.001 | 1.07 (1.04–1.10) | <0.001 | 1.10 (1.06–1.13) | <0.001 |
| PAD | 4.33 (1.46–12.86) | 0.008 | 5.06 (1.75–14.69) | 0.003 | 2.34 (0.88–6.21) | 0.089 |
| CAD | 1.87 (1.10–3.19) | 0.020 | 1.54 (0.93–2.55) | 0.091 | 2.19 (1.27–3.80) | 0.005 |
| CVD | 1.19 (0.53–2.70) | 0.673 | 0.67 (0.31–1.44) | 0.298 | 2.93 (1.19–7.26) | 0.020 |
| Chronic kidney disease | 1.80 (0.91–3.55) | 0.090 | 1.36 (0.71–2.57) | 0.353 | 1.45 (0.74–2.84) | 0.285 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noflatscher, M.; Schreinlechner, M.; Sommer, P.; Kerschbaum, J.; Berggren, K.; Theurl, M.; Kirchmair, R.; Marschang, P. Influence of Traditional Cardiovascular Risk Factors on Carotid and Femoral Atherosclerotic Plaque Volume as Measured by Three-Dimensional Ultrasound. J. Clin. Med. 2019, 8, 32. https://doi.org/10.3390/jcm8010032
Noflatscher M, Schreinlechner M, Sommer P, Kerschbaum J, Berggren K, Theurl M, Kirchmair R, Marschang P. Influence of Traditional Cardiovascular Risk Factors on Carotid and Femoral Atherosclerotic Plaque Volume as Measured by Three-Dimensional Ultrasound. Journal of Clinical Medicine. 2019; 8(1):32. https://doi.org/10.3390/jcm8010032
Chicago/Turabian StyleNoflatscher, Maria, Michael Schreinlechner, Philip Sommer, Julia Kerschbaum, Katharina Berggren, Markus Theurl, Rudolf Kirchmair, and Peter Marschang. 2019. "Influence of Traditional Cardiovascular Risk Factors on Carotid and Femoral Atherosclerotic Plaque Volume as Measured by Three-Dimensional Ultrasound" Journal of Clinical Medicine 8, no. 1: 32. https://doi.org/10.3390/jcm8010032
APA StyleNoflatscher, M., Schreinlechner, M., Sommer, P., Kerschbaum, J., Berggren, K., Theurl, M., Kirchmair, R., & Marschang, P. (2019). Influence of Traditional Cardiovascular Risk Factors on Carotid and Femoral Atherosclerotic Plaque Volume as Measured by Three-Dimensional Ultrasound. Journal of Clinical Medicine, 8(1), 32. https://doi.org/10.3390/jcm8010032