A Lipidomics Study Reveals Lipid Signatures Associated with Early Allograft Dysfunction in Living Donor Liver Transplantation

 , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Blood Samples
2.3. NMR Analysis of The Plasma
2.4. Liquid Chromatography Coupled with Mass Spectrometry (LC-MS)-Based Lipidomic
2.5. Ultra-Performance Liquid Chromatography (UPLC)-Based Amino Acid Measurement
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Change in Circulatory Amino Acid Profiles in Recipients with EAD
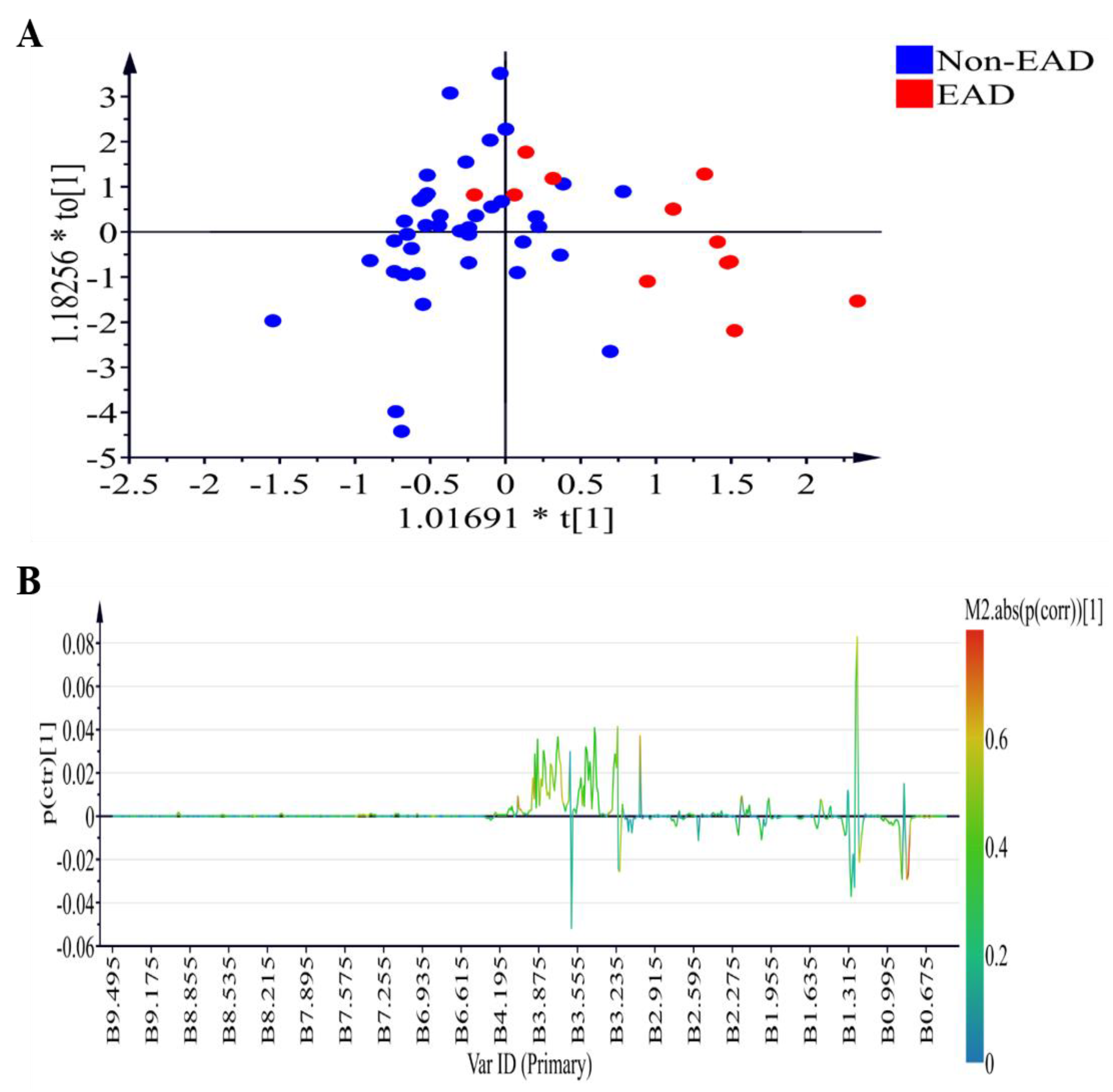
3.3. Changes in NMR Plasma Profiles in Recipients with EAD
3.4. Changes in Circulatory Lipid Profiles in Recipients with EAD
3.5. Discriminative Ability of Potential Biomarkers for EAD and In-Hospital Mortality
3.6. External Validation of Lipidomic Profiling as Prediction of EAD, Long Hospital Stay and In-Hospital Mortality
3.7. Schematic Illustration of Metabolite Alternation in EAD after LDLT
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rayar, M.; Levi Sandri, G.B.; Cusumano, C.; Lombard, N.; Lakehal, M.; Desfourneaux, V.; Meunier, B.; Sulpice, L.; Boudjema, K. A score model for the continuous grading of early allograft dysfunction severity. Liver Transplant. 2016, 22, 859–860. [Google Scholar] [CrossRef] [PubMed]
- Chok, K.S.; Fung, J.Y.; Chan, A.C.; Dai, W.C.; Sharr, W.W.; Cheung, T.T.; Chan, S.C.; Lo, C.M. Comparable short and long term outcomes in living donor and deceased donor liver transplantations for patients with model for end stage liver disease score >35 in hepatitis B endemic area. Ann. Surg. 2017, 265, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Fisher, R.A. Living donor liver transplantation: Eliminating the wait for death in end-stage liver disease? Nat. Rev. Gastroenterol. Hepatol. 2017, 14, 373–382. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.D.; Croome, K.P.; Shalev, J.A.; Musto, K.R.; Sharma, M.; Keaveny, A.P.; Taner, C.B. Early allograft dysfunction after liver transplantation: An intermediate outcome measure for targeted improvements. Ann. Hepatol. 2016, 15, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Hudcova, J.; Scopa, C.; Rashid, J.; Waqas, A.; Ruthazer, R.; Schumann, R. Effect of early allograft dysfunction on outcomes following liver transplantation. Clin. Transplant. 2017, 31, e12887. [Google Scholar] [CrossRef] [PubMed]
- Pomposelli, J.J.; Goodrich, N.P.; Emond, J.C.; Humar, A.; Baker, T.B.; Grant, D.R.; Fisher, R.A.; Roberts, J.P.; Olthoff, K.M.; Gillespie, B.W.; et al. Patterns of early allograft dysfunction in adult live donor liver transplantation: The A2ALL experience. Transplantation 2016, 100, 1490–1499. [Google Scholar] [CrossRef] [PubMed]
- Croome, K.P.; Wall, W.; Quan, D.; Vangala, S.; McAlister, V.; Marotta, P.; Hernandez-Alejandro, R. Evaluation of the updated definition of early allograft dysfunction in donation after brain death and donation after cardiac death liver allografts. Hepatobiliary Pancreat. Dis. Int. 2012, 11, 372–376. [Google Scholar] [CrossRef]
- Olthoff, K.M.; Kulik, L.; Samstein, B.; Kaminski, M.; Abecassis, M.; Emond, J.; Shaked, A.; Christie, J.D. Validation of a current definition of early allograft dysfunction in liver transplant recipients and analysis of risk factors. Liver Transplant. 2010, 16, 943–949. [Google Scholar] [CrossRef]
- Serkova, N.J.; Zhang, Y.; Coatney, J.L.; Hunter, L.; Wachs, M.E.; Niemann, C.U.; Mandell, M.S. Early detection of graft failure using the blood metabolic profile of a liver recipient. Transplantation 2007, 83, 517–521. [Google Scholar] [CrossRef]
- Tripathi, P.; Bala, L.; Saxena, R.; Yachha, S.K.; Roy, R.; Khetrapal, C.L. 1H NMR spectroscopic study of blood serum for the assessment of liver function in liver transplant patients. J. Gastrointestin. Liver Dis. 2009, 18, 329–336. [Google Scholar]
- Cortes, M.; Pareja, E.; Garcia-Canaveras, J.C.; Donato, M.T.; Montero, S.; Mir, J.; Castell, J.V.; Lahoz, A. Metabolomics discloses donor liver biomarkers associated with early allograft dysfunction. J. Hepatol. 2014, 61, 564–574. [Google Scholar] [CrossRef] [PubMed]
- McPhail, M.J.W.; Shawcross, D.L.; Lewis, M.R.; Coltart, I.; Want, E.J.; Antoniades, C.G.; Veselkov, K.; Triantafylou, E.; Patel, V.; Pop, O.; et al. Multivariate metabotyping of plasma predicts survival in patients with decompensated cirrhosis. J. Hepatol. 2016, 64, 1058–1067. [Google Scholar] [CrossRef] [PubMed]
- Hrydziuszko, O.; Perera, M.T.; Laing, R.; Kirwan, J.; Silva, M.A.; Richards, D.A.; Murphy, N.; Mirza, D.F.; Viant, M.R. Mass spectrometry based metabolomics comparison of liver grafts from donors after cicurlatory death (DCD) and donors after brain death (DBD) used in human orthotopic liver transplantation. PLoS ONE 2016, 11, e0165884. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Casas-Ferreira, A.M.; Ma, Y.; Sen, A.; Kim, M.; Proitsi, P.; Shkodra, M.; Tena, M.; Srinivasan, P.; Heaton, N.; et al. Lipidomics comparing DCD and DBD liver allografts uncovers lysophospholipids elevated in recipients undergoing early allograft dysfunction. Sci. Rep. 2015, 5, 17737. [Google Scholar] [CrossRef] [PubMed]
- Ceglarek, U.; Kresse, K.; Becker, S.; Fiedler, G.M.; Thiery, J.; Quante, M.; Wieland, R.; Bartels, M.; Aust, G. Circulating sterols as predictors of early allograft dysfunction and clinical outcome in patients undergoing liver transplantation. Metabolomics 2016, 12, 182. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.M.; Eldeen, F.Z.; Lee, C.F.; Wu, T.J.; Chou, H.S.; Wu, T.H.; Soong, R.S.; Lee, W.C. “Left at right” adult liver transplantation: The feasibility of heterotopic implantation of left liver graft. Am. J. Transplant. 2012, 12, 1511–1518. [Google Scholar] [CrossRef] [PubMed]
- Dona, A.C.; Jimenez, B.; Schafer, H.; Humpfer, E.; Spraul, M.; Lewis, M.R.; Pearce, J.T.; Holmes, E.; Lindon, J.C.; Nicholson, J.K. Precision high-throughput proton NMR spectroscopy of human urine, serum, and plasma for large-scale metabolic phenotyping. Anal. Chem. 2014, 86, 9887–9894. [Google Scholar] [CrossRef]
- Sarafian, M.H.; Gaudin, M.; Lewis, M.R.; Martin, F.P.; Holmes, E.; Nicholson, J.K.; Dumas, M.E. Objectiveset of criteria for optimization of sample preparation procedures for ultra-high throughput untargeted blood plasma lipid profiling by ultra performance liquid chromatography-mass spectrometry. Anal. Chem. 2014, 86, 5766–5774. [Google Scholar] [CrossRef]
- Frank, M.P.; Powers, R.W. Simple and rapid quantitative high-performance liquid chromatographic analysis of plasma amino acids. J. Chromatogr. B 2007, 852, 646–649. [Google Scholar] [CrossRef]
- Pappa-Louisi, A.; Nikitas, P.; Agrafiotou, P.; Papageorgiou, A. Optimization of separation and detection of 6-aminoquinolyl derivatives of amino acids by using reversed-phase liquid chromatography with on line UV, fluorescence and electrochemical detection. Anal. Chim. Acta 2007, 593, 92–97. [Google Scholar] [CrossRef]
- Team RDC. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2008. [Google Scholar]
- Ikegami, T.; Shimada, M.; Imura, S.; Arakawa, Y.; Nii, A.; Morine, Y.; Kanemura, H. Current concept of small-for-size grafts in living donor liver transplantation. Surg. Today 2008, 38, 971–982. [Google Scholar] [CrossRef] [PubMed]
- Shoreem, H.; Gad, E.H.; Soliman, H.; Hegazy, O.; Saleh, S.; Zakaria, H.; Ayoub, E.; Kamel, Y.; Abouelella, K.; Ibrahim, T.; et al. Small for size syndrome difficult dilemma: Lessons from 10 years single centre experience in living donor liver transplantation. World J. Hepatol. 2017, 9, 930–944. [Google Scholar] [CrossRef] [PubMed]
- Chen, E.; Lu, J.; Chen, D.; Zhu, D.; Wang, Y.; Zhang, Y.; Zhou, N.; Wang, J.; Li, J.; Li, L. Dynamic changes of plasma metabolites in pigs with GalN-induced acute liver failure using GC-MS and UPLC-MS. Biomed. Pharmacother. 2017, 93, 480–489. [Google Scholar] [CrossRef] [PubMed]
- Tessari, P.; Vettore, M.; Millioni, R.; Puricelli, L.; Orlando, R. Effect of liver cirrhosis on phenylalanine and tyrosine metabolism. Curr. Opin. Clin. Nutr. Metab. Care 2010, 13, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Tietge, U.J.; Bahr, M.J.; Manns, M.P.; Böker, K.H. Plasma amino acids in cirrhosis and after liver transplantation: Influence of liver function, hepatic hemodynamics and circulating hormones. Clin. Transplant. 2002, 16, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Cano, A.; Mariño, Z.; Millet, O.; Martínez-Arranz, I.; Navasa, M.; Falcón-Pérez, J.M.; Pérez-Cormenzana, M.; Caballería, J.; Embade, N.; Forns, X.; et al. A metabolomics signature linked to liver fibrosis in the serum of transplanted hepatitis C patients. Sci. Rep. 2017, 7, 10497. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| EAD 11 (n = 12) | Non-EAD 11 (n = 39) | p-Value | |
|---|---|---|---|
| Height (m) | 1.63 ± 0.09 | 1.63 ± 0.08 | 0.99 |
| Weight (kg) | 66.43 ± 13.47 | 67.63 ± 11.66 | 0.78 |
| BMI 1 | 24.92 ± 13.47 | 25.31 ± 3.44 | 0.74 |
| Age (years) | 56.42 ± 10.82 | 56.00 ± 7.30 | 0.88 |
| Gender (M/F) | 0.74 | ||
| M | 8 | 22 | |
| F | 4 | 17 | |
| Blood type | |||
| A | 5 | 15 | 1.00 |
| B | 2 | 7 | |
| O | 5 | 15 | |
| AB | 0 | 2 | |
| MELD 2 | 19.92 ± 11.89 | 16.69 ± 0.09 | 0.29 |
| HBV 3 (Yes/No) | 6/6 | 18/21 | 0.82 |
| HCV 4 (Yes/No) | 3/9 | 12/27 | 1.00 |
| Alcoholism (Yes/No) | 4/8 | 12/2 | 1.00 |
| ABO incompatibility (Yes/No) | 2/10 | 6/33 | 1.00 |
| CKD 5 (Yes/No) | 5/7 | 5/34 | 0.04 |
| Graft (g) | 615.00 ± 122.21 | 644.36 ± 146.22 | 0.53 |
| GRWR 6 (%) | 0.96 ± 0.13 | 0.98 ± 0.30 | 0.82 |
| Blood loss (mL) PRBC 7 (U) FFP 8 (U) Platelet (U) | 2962.50 ± 2111.13 | 1705.64 ± 166348 | 0.04 |
| 13.42 ± 8.97 | 7.90 ± 7.52 | 0.04 | |
| 13.83 ± 11.07 | 11.69 ± 11.05 | 0.56 | |
| 12.00 ± 8.86 | 8.62 ± 9.52 | 0.28 | |
| CIT 9 (minutes) | 41.50 ± 37.48 | 52.97 ± 34.94 | 0.33 |
| WIT 10 (minutes) | 37.08 ± 7.83 | 42.31 ± 10.94 | |
| In hospital mortality (Yes/No) | 4/8 | 2/37 | 0.13 |
| Hospital stay ≥45 days (Yes/No) | 9/3 | 12/27 | |
| T1 EAD 10 (n = 12) | T1 Non-EAD 10 (n = 39) | T6 EAD 10 (n = 12) | T6 Non-EAD 10 (n = 39) | p-Value | p-Value | p-Value | p-Value | |
|---|---|---|---|---|---|---|---|---|
| (EAD 10) | (Non-EAD 10) | (T1) | (T6) | |||||
| Hemoglobin (g/dL) | 9.30 ± 2.05 | 10.76 ± 2.47 | 11.20 ± 2.77 | 10.28 ± 1.39 | <0.01 | 0.29 | 0.07 | 0.13 |
| Hematocrit (%) | 27.88 ± 6.15 | 50.38 ± 117.49 | 31.78 ± 6.97 | 30.08 ± 4.03 | 0.02 | 0.29 | 0.51 | 0.29 |
| Platelet (1000/dL) | 62.42 ± 42.55 | 87.94 ± 45.37 | 40.58 ± 16.43 | 71.41 ± 37.86 | 0.08 | <0.01 | 0.09 | <0.01 |
| PT 1 (sec) | 18.59 ± 6.48 | 19.11 ± 8.52 | 18.52 ± 4.89 | 14.05 ± 1.64 | 0.98 | <0.01 | 0.85 | <0.01 |
| INR 2 | 1.60 ± 0.61 | 1.67 ± 0.74 | 1.62 ± 0.43 | 1.23 ± 0.14 | 0.94 | <0.01 | 0.78 | <0.01 |
| APTT 3 (sec) | 40.92 ± 19.55 | 36.43 ± 12.16 | 45.77 ± 19.94 | 31.50 ± 7.80 | 0.43 | 0.03 | 0.34 | <0.01 |
| Total protein (g/dL) | 6.18 ± 1.42 | 6.66 ± 0.90 | 4.13 ± 0.43 | 4.33 ± 0.43 | <0.01 | <0.01 | 0.17 | <0.01 |
| Albumin (g/dL) | 3.02 ± 0.73 | 3.05 ± 0.72 | 2.53 ± 0.29 | 2.63 ± 0.31 | 0.05 | <0.01 | 0.90 | 0.17 |
| BUN 4 (mg/dL) | 39.17 ± 40.10 | 17.27 ± 17.59 | 53.78 ± 41.17 | 23.22 ± 12.13 | 0.07 | <0.01 | <0.01 | 0.37 |
| Creatinine (mg/dL) | 1.91 ± 2.20 | 1.08 ± 1.49 | 1.99 ± 1.32 | 0.78 ± 0.50 | 0.87 | 0.18 | 0.14 | <0.01 |
| GFR 5(mL/mL/m/1.73 min/1.73 m2) | 81.42 ± 60.10 | 114.00 ± 53.55 | 65.50 ± 79.17 | 116.36 ± 47.78 | 0.27 | 0.78 | 0.08 | <0.01 |
| Sodium (mEq/L) | 140.42 ± 7.17 | 138.43 ± 3.92 | 123.98 ± 35.50 | 136.92 ± 3.03 | 0.15 | 0.07 | 0.22 | <0.01 |
| Potassium (mEq/L) | 3.61 ± 0.55 | 4.63 ± 5.51 | 3.77 ± 0.67 | 3.71 ± 0.50 | 0.50 | 0.31 | 0.53 | 0.03 |
| Calcium (mg/dL) | 8.39 ± 0.40 | 8.26 ± 0.57 | 7.62 ± 0.75 | 7.43 ± 0.49 | 0.01 | <0.01 | 0.47 | 0.74 |
| Sugar (mg/dL) | 140.92 ± 45.05 | 132.08 ± 48.87 | 219.92 ± 78.30 | 179.74 ± 55.22 | <0.01 | <0.01 | 0.58 | 0.32 |
| LDH 6 (U/L) | 299.58 ± 203.00 | 245.10 ± 79.19 | 439.67 ± 236.66 | 328.15 ± 129.62 | 0.111 | <0.01 | 0.171 | 0.04 |
| Total bilirubin (mg/dL) | 10.44 ± 16.24 | 4.25 ± 5.85 | 13.99 ± 8.96 | 2.64 ± 2.24 | 0.360 | 0.071 | 0.048 | <0.01 |
| Direct bilirubin (mg/dL) | 6.02 ± 10.14 | 2.03 ± 2.98 | 8.14 ± 5.57 | 1.51 ± 1.43 | 0.363 | 0.241 | 0.032 | <0.01 |
| AST 7 (U/L) | 123.50 ± 189.12 | 68.90 ± 19.08 | 109.58 ± 79.96 | 119.90 ± 84.13 | 0.811 | <0.01 | 0.112 | 0.71 |
| ALT 8 (U/L) | 52.00 ± 37.67 | 34.87 ± 19.08 | 191.58 ± 134.26 | 214.56 ± 181.85 | <0.01 | <0.01 | 0.039 | 0.69 |
| ALP 9 (U/L) | 95.83 ± 44.70 | 108.64 ± 53.20 | 127.00 ± 65.96 | 88.31 ± 49.30 | 0.154 | 0.040 | 0.454 | 0.03 |
| T6 EAD 3 (n = 12) | T6 non-EAD 3 (n = 39) | p-Value | |
|---|---|---|---|
| Histidine (μM) | 110.6 ± 38.7 | 78.8 ± 15.4 | 0.0166 |
| Asparagine (μM) | 59.8 ± 17.2 | 65.3 ± 18.0 | 0.3511 |
| Taurine (μM) | 47.0 ± 28.5 | 39.7 ± 15.0 | 0.4101 |
| Serine (μM) | 111.0 ± 53.7 | 116.6 ± 29.7 | 0.7349 |
| Glutamine (μM) | 595.8 ± 250.5 | 557.4 ± 97.3 | 0.6135 |
| Arginine (μM) | 90.6 ± 48.9 | 90.7 ± 23.8 | 0.9935 |
| Glycine (μM) | 333.5 ± 157.9 | 275.9 ± 131.9 | 0.2129 |
| Citrulline (μM) | 41.4 ± 24.8 | 32.9 ± 8.9 | 0.2664 |
| Glutamate (μM) | 64.6 ± 34.6 | 71.9 ± 32.7 | 0.5043 |
| Threonine (μM) | 149.8 ± 69.7 | 172.7 ± 49.7 | 0.2114 |
| Alanine (μM) | 264.5 ± 159.7 | 246.3 ± 92.6 | 0.7131 |
| Proline (μM) | 237.2 ± 174.0 | 176.5 ± 61.8 | 0.2590 |
| Ornithine (μM) | 57.9 ± 33.5 | 58.3 ± 17.5 | 0.9735 |
| Cystine (μM) | 64.2 ± 35.4 | 51.5 ± 20.5 | 0.2594 |
| Lysine (μM) | 208.2 ± 72.6 | 246.6 ± 56.6 | 0.0607 |
| Tyrosine (μM) | 82.6 ± 29.9 | 68.9 ± 24.4 | 0.1133 |
| Methionine (μM) | 41.3 ± 37.6 | 34.6 ± 16.2 | 0.5573 |
| Valine (μM) | 201.5 ± 52.7 | 229.2 ± 61.8 | 0.1670 |
| Isoleucine (μM) | 63.4 ± 18.8 | 72.6 ± 26.7 | 0.2728 |
| Leucine (μM) | 91.4 ± 24.4 | 110.8 ± 40.6 | 0.1239 |
| Phenylalanine (μM) | 97.2 ± 36.9 | 73.2 ± 18.5 | 0.0498 |
| Tryptophan (μM) | 51.0 ± 21.4 | 43.0 ± 13.1 | 0.2399 |
| Essential AA (μM) | 1046.0 ± 295.1 | 1087.4 ± 234.7 | 0.6174 |
| BCAA 1 (μM) | 356.3 ± 90.7 | 412.6 ± 126.2 | 0.1587 |
| AAA 2 (μM) | 230.8 ± 80.3 | 185.1 ± 47.1 | 0.0827 |
| Fischer’s ratio | 1.7 ± 0.5 | 2.3 ± 0.5 | 0.0010 |
| Metabolites | Adduct | EAD (n = 12) | Non-EAD (n = 39) | p-Value | VIP Value |
|---|---|---|---|---|---|
| PC 2 (16:0–18:1) | M + H | 293,234.70 ± 88,445.42 | 190,835.04 ± 64,727.83 | 8.80 × 10−8 | 14.87 |
| Cholesterol linoleate | 8247.39 ± 9123.72 | 23,705.64 ± 10,062.66 | 1.41 × 10−13 | 5.94 | |
| PC (18:1–18:1) | M + H | 109,562.18 ± 32,521.47 | 86,965.79 ± 23,297.41 | 0.0004 | 5.71 |
| PC (16:1–16:0) | M + H | 19,371.66 ± 14,900.85 | 7182.02 ± 5130.27 | 3.08 × 10−5 | 5.13 |
| PC (36:4) | M + H | 21,621.80 ± 8897.53 | 11,880.11 ± 5475.14 | 2.51 × 10−7 | 4.67 |
| PC (16:0–16:0) | M + H | 13,302.07 ± 5827.96 | 6006.07 ± 3085.78 | 1.33 × 10−8 | 4.33 |
| PC (16:0–18:2) | M + H | 42,095.65 ± 15,600.17 | 31,631.49 ± 11,841.82 | 0.0006 | 3.76 |
| Cholesterol linoleate | M + NH4 | 1768.35 ± 3256.70 | 7312.47 ± 3399.90 | 1.36 × 10−14 | 3.62 |
| LysoPC 3 (16:0) | M + H | 1245.59 ± 1282.79 | 4852.28 ± 2746.80 | 1.52 × 10−19 | 2.79 |
| PC (18:1–18:0) | M + H | 9301.80 ± 3127.75 | 5999.75 ± 2319.29 | 6.12 × 10−7 | 2.57 |
| Cholesterol oleate | 1655.40 ± 934.69 | 3933.22 ± 1373.84 | 2.79 × 10−18 | 2.38 | |
| TG 4 (52:3) | M + Na | 15,257.06 ± 3186.91 | 18,383.95 ± 3284.08 | 1.77 × 10−6 | 2.20 |
| Met0295 | 2752.32 ± 2798.94 | 774.76 ± 766.19 | 0.0002 | 2.00 | |
| Met0592 | 3071.09 ± 1361.53 | 1429.76 ± 1076.40 | 7.83 × 10−12 | 1.87 | |
| LysoPC (18:2) | M + H | 764.32 ± 840.10 | 2425.17 ± 1466.14 | 2.32 × 10−13 | 1.78 |
| L–Acetylcarnitine | M + H | 2265.22 ± 2044.40 | 849.66 ± 824.14 | 0.0003 | 1.61 |
| Cholesterol arachidonate | 227.70 ± 354.57 | 1312.62 ± 883.71 | 7.51 × 10−20 | 1.50 | |
| Cholesterol | 1745.76 ± 640.41 | 994.24 ± 411.78 | 5.96 × 10−8 | 1.32 | |
| LysoPC (18:1) | M + H | 392.86 ± 576.23 | 1254.31 ± 834.29 | 9.18 × 10−10 | 1.23 |
| LysoPC (18:0) | M + H | 139.32 ± 229.46 | 876.64 ± 626.57 | 1.03 × 10−19 | 1.22 |
| Cholesterol linoleate | M + Na | 267.63 ± 856.69 | 1036.13 ± 854.38 | 6.75 × 10−6 | 1.06 |
| PC (32:1) | M + Na | 559.23 ± 782.39 | 44.72 ± 119.20 | 0.0005 | 1.02 |
| Metabolites | Study Group | Validation Group | ||
|---|---|---|---|---|
| AUC 6 | Standard Error | AUC 6 | Standard Error | |
| Cholesterol oleate | 0.9338 | 0.0350 | 0.6389 | 0.1271 |
| LysoPC 1 (16:0) | 0.8921 | 0.0491 | 0.8241 | 0.0942 |
| PC 2 (16:0–16:0) | 0.8376 | 0.0767 | 0.9537 | 0.0428 |
| Total bilirubin | 0.9103 | 0.0530 | 0.5880 | 0.1365 |
| INR 3 | 0.8002 | 0.0823 | 0.6991 | 0.1149 |
| ALT 4 | 0.5053 | 0.1011 | 0.6852 | 0.1218 |
| AST 5 | 0.5449 | 0.0988 | 0.6699 | 0.1280 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsai, H.-I.; Lo, C.-J.; Zheng, C.-W.; Lee, C.-W.; Lee, W.-C.; Lin, J.-R.; Shiao, M.-S.; Cheng, M.-L.; Yu, H.-P. A Lipidomics Study Reveals Lipid Signatures Associated with Early Allograft Dysfunction in Living Donor Liver Transplantation. J. Clin. Med. 2019, 8, 30. https://doi.org/10.3390/jcm8010030
Tsai H-I, Lo C-J, Zheng C-W, Lee C-W, Lee W-C, Lin J-R, Shiao M-S, Cheng M-L, Yu H-P. A Lipidomics Study Reveals Lipid Signatures Associated with Early Allograft Dysfunction in Living Donor Liver Transplantation. Journal of Clinical Medicine. 2019; 8(1):30. https://doi.org/10.3390/jcm8010030
Chicago/Turabian StyleTsai, Hsin-I, Chi-Jen Lo, Chih-Wen Zheng, Chao-Wei Lee, Wei-Chen Lee, Jr-Rung Lin, Ming-Shi Shiao, Mei-Ling Cheng, and Huang-Ping Yu. 2019. "A Lipidomics Study Reveals Lipid Signatures Associated with Early Allograft Dysfunction in Living Donor Liver Transplantation" Journal of Clinical Medicine 8, no. 1: 30. https://doi.org/10.3390/jcm8010030
APA StyleTsai, H.-I., Lo, C.-J., Zheng, C.-W., Lee, C.-W., Lee, W.-C., Lin, J.-R., Shiao, M.-S., Cheng, M.-L., & Yu, H.-P. (2019). A Lipidomics Study Reveals Lipid Signatures Associated with Early Allograft Dysfunction in Living Donor Liver Transplantation. Journal of Clinical Medicine, 8(1), 30. https://doi.org/10.3390/jcm8010030