Evaluation of Dose Dependent Maternal Exposure to Bisphenol A on Thyroid Functions in Newborns


Abstract
1. Introduction
2. Material Methods
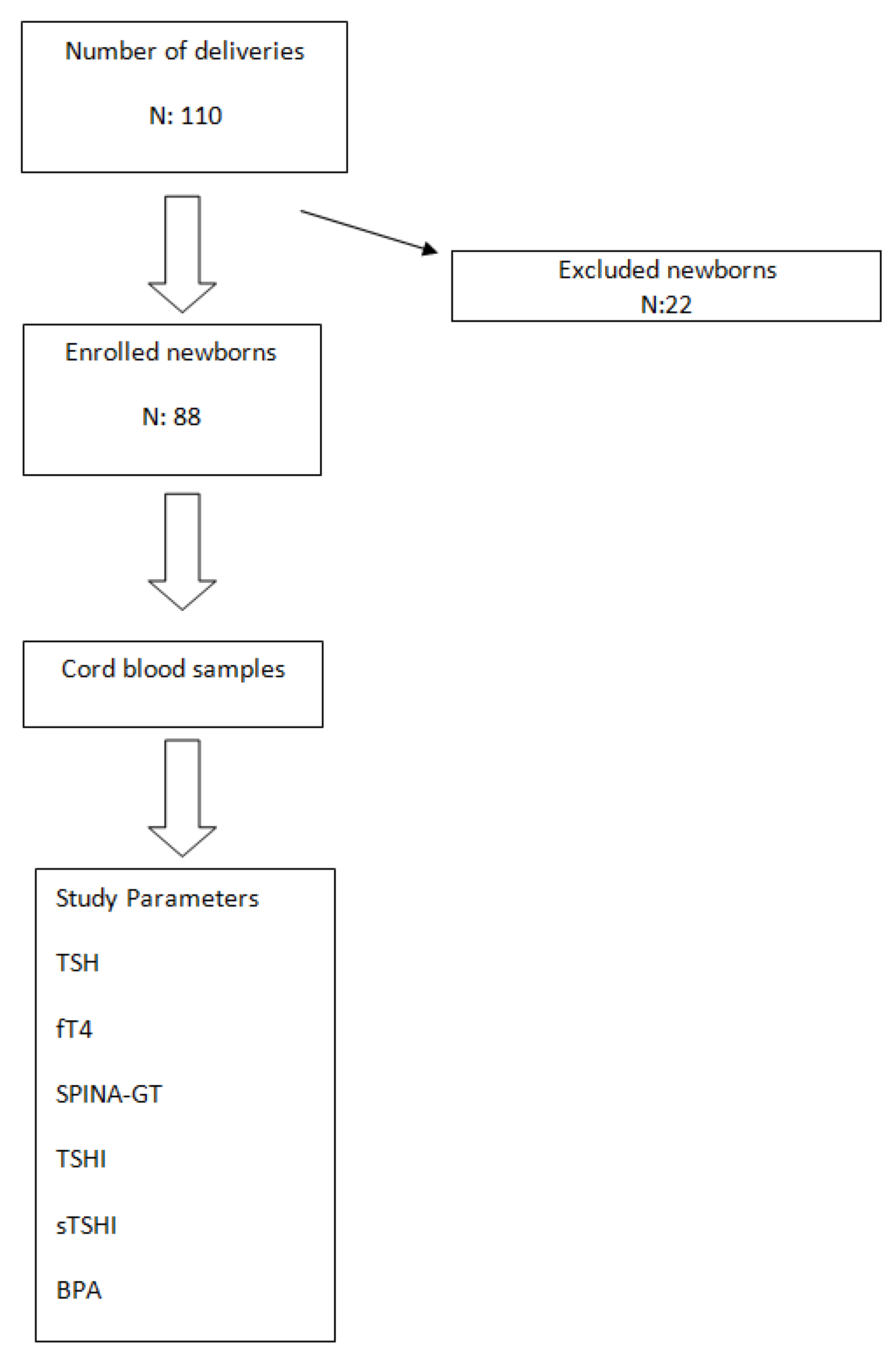
2.1. Study Setting
2.2. Blood Sampling and Measurements
2.3. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Lewis, J.B.; Rueggeberg, F.A.; Lapp, C.A.; Ergle, J.W.; Schuster, G.S. Identification and characterization of estrogen-like components in commercial resin-based dental restorative materials. Clin. Oral Investig. 1999, 3, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Gayathri, N.; Dhanya, C.; Indu, A.; Kurup, P. Changes in some hormones by low doses of di (2-ethyl hexyl) phthalate (DEHP), a commonly used plasticizer in PVC blood storage bags & medical tubing. Indian J. Med. Res. 2004, 119, 139–144. [Google Scholar] [PubMed]
- Guo, Y.; Zhang, Z.; Liu, L.; Li, Y.; Ren, N.; Kannan, K. Occurrence and profiles of phthalates in foodstuffs from China and their implications for human exposure. J. Agric. Food Chem. 2012, 60, 6913–6919. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.H.; Kondo, F. Determination of bisphenol A in milk and dairy products by high-performance liquid chromatography with fluorescence detection. J. Food Prot. 2003, 66, 1439–1443. [Google Scholar] [CrossRef] [PubMed]
- Thayer, K.A.; Doerge, D.R.; Hunt, D.; Schurman, S.H.; Twaddle, N.C.; Churchwell, M.I.; Garantziotis, S.; Kissling, G.E.; Easterling, M.R.; Bucher, J.R.; et al. Pharmacokinetics of bisphenol A in humans following a single oral administration. Environ. Int. 2015, 83, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Fromme, H.; Gruber, L.; Schlummer, M.; Wolz, G.; Böhmer, S.; Angerer, J.; Mayer, R.; Liebl, B.; Bolte, G. Intake of phthalates and di(2-ethylhexyl)adipate: Results of the Integrated Exposure Assessment Survey based on duplicate diet samples and biomonitoring data. Environ. Int. 2007, 33, 1012–1020. [Google Scholar] [CrossRef] [PubMed]
- Sathyanarayana, S.; Karr, C.J.; Lozano, P.; Brown, E.; Calafat, A.M.; Liu, F.; Swan, S.H. Baby care products: Possible sources of infant phthalate exposure. Pediatrics 2008, 121, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Rochester, J.R. Bisphenol A and human health: A review of the literature. Reprod. Toxicol. 2013, 42, 132–155. [Google Scholar] [CrossRef] [PubMed]
- Leung, A.M.; Korevaar, T.I.; Peeters, R.P.; Zoeller, R.T.; Köhrle, J.; Duntas, L.H.; Brent, G.A.; Demeneix, B.A. Exposure to thyroid-disrupting chemicals: A transatlantic call for action. Thyroid 2016, 26, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Muhamad, M.S.; Salim, M.R.; Lau, W.J.; Yusop, Z. A review on bisphenol A occurrences, health effects and treatment process via membrane technology for drinking water. Environ. Sci. Pollut. Res. Int. 2016, 23, 11549–11567. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Lin, Y.; Li, Y.; Ying, C.; Chen, J.; Song, L.; Zhou, Z.; Lv, Z.; Xia, W.; Chen, X.; et al. Perinatal exposure to bisphenol A at reference dose predisposes offspring to metabolic syndrome in adult rats on a high-fat diet. J. Endocrinol. 2011, 152, 3049–3061. [Google Scholar] [CrossRef] [PubMed]
- Behnia, F.; Peltier, M.; Getahun, D.; Watson, C.; Saade, G.; Menon, R. High bisphenol A (BPA) concentration in the maternal, but not fetal, compartment increases the risk of spontaneous preterm delivery. J. Matern. Fetal Neonatal Med. 2016, 29, 3583–3589. [Google Scholar] [CrossRef] [PubMed]
- Poimenova, A.; Markaki, E.; Rahiotis, C.; Kitraki, E. Corticosterone-regulated actions in the rat brain are affected by perinatal exposure to low dose of bisphenol A. J. Neurosci. 2010, 167, 741–749. [Google Scholar] [CrossRef] [PubMed]
- Chevrier, J.; Gunier, R.B.; Bradman, A.; Holland, N.T.; Calafat, A.M.; Eskenazi, B.; Harley, K.G. Maternal urinary bisphenol a during pregnancy and maternal and neonatal thyroid function in the CHAMACOS study. Environ. Health Perspect. 2013, 121, 138–144. [Google Scholar] [PubMed]
- Giesbrecht, G.F.; Ejaredar, M.; Liu, J.; Thomas, J.; Letourneau, N.; Campbell, T.; Martin, J.W.; Dewey, D. Prenatal bisphenol a exposure and dysregulation of infant hypothalamic-pituitary-adrenal axis function: Findings from the APrON cohort study. Environ. Health 2017, 16, 47. [Google Scholar] [CrossRef] [PubMed]
- Franssen, D.; Gérard, A.; Hennuy, B.; Donneau, A.F.; Bourguignon, J.P.; Parent, A.S. Delayed neuroendocrine sexual maturation in female rats after a very low dose of Bisphenol A through altered GABAergic neurotransmission and opposing effects of a high dose. J. Endocrinol. 2016, 157, 1740–1750. [Google Scholar] [CrossRef] [PubMed]
- Soriano, S.; Ripoll, C.; Alonso-Magdalena, P.; Fuentes, E.; Quesada, I.; Nadal, A.; Martinez-Pinna, J. Effects of bisphenol A on ion channels: Experimental evidence and molecular mechanisms. Steroids 2016, 111, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Boas, M.; Feldt-Rasmussen, U.; Main, K.M. Thyroid effects of endocrine disrupting chemicals. Mol. Cell. Endocrinol. 2012, 355, 240–248. [Google Scholar] [CrossRef] [PubMed]
- Henrichs, J.; Ghassabian, A.; Peeters, R.P.; Tiemeier, H. Maternal hypothyroxinemia and effects on cognitive functioning in childhood: How and why? Clin. Endocrinol. 2013, 79, 152–162. [Google Scholar] [CrossRef] [PubMed]
- Romano, M.E.; Webster, G.M.; Vuong, A.M.; Zoeller, R.T.; Chen, A.; Hoofnagle, A.N.; Calafat, A.M.; Karagas, M.R.; Yolton, K.; Lanphear, B.P.; et al. Gestational urinary bisphenol A and maternal and newborn thyroid hormone concentrations: The HOME Study. Environ. Res. 2015, 138, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, R.G. Maternal bisphenol A alters fetal endocrine system: Thyroid adipokine dysfunction. Food Chem. Toxicol. 2016, 95, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, J.W.; Landgrafe-Mende, G.; Wiora, E.; Chatzitomaris, A.; Klein, H.H.; Midgley, J.E.; Hoermann, R. Calculated parameters of Thyroid Homeostasis: Emerging Tools for Differential Diagnosis and Clinical Research. Front. Endocrinol. 2016, 7, 57. [Google Scholar] [CrossRef] [PubMed]
- Dietrich, J.W.; Fischer, M.R.; Jauch, J.; Pantke, E.; Gärtner, R.; Pickardt, C.R. SPINA-THYR: A Novel Systems Theoretic Approach to Determine the Secretion Capacity of the Thyroid Gland. Eur. J. Intern. Med. 1999, 10, 34. [Google Scholar]
- Jostel, A.; Ryder, W.D.; Shalet, S.M. The use of thyroid function tests in the diagnosis of hypopituitarism: Definition and evaluation of the TSH Index. Clin. Endocrinol. 2009, 71, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Diamanti-Kandarakis, E.; Bourguignon, J.P.; Giudice, L.C.; Hauser, R.; Prins, G.S.; Soto, A.M.; Zoeller, R.T.; Gore, A.C. Endocrine-disrupting chemicals: An Endocrine Society scientific statement. Endocr. Rev. 2009, 30, 293–342. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.D.; Crofton, K.M.; Rice, D.C.; Zoeller, R.T. Thyroid-disrupting chemicals: Interpreting upstream biomarkers of adverse outcomes. Environ. Health Perspect. 2009, 117, 1033–1041. [Google Scholar] [CrossRef] [PubMed]
- Mori, C. Fetal exposure to endocrine disrupting chemicals (EDCs) and possible effects of EDCs on the male reproductive system in Japan. In Proceedings of the International Symposium on Environmental Endocrine Disrupters, Kyoto, Japan, 11–13 December 1998; p. 39. [Google Scholar]
- Sakurai, K.; Mori, C. Fetal exposure to endocrine disruptors. Nippon Rinsho 2000, 58, 2508–2513. [Google Scholar] [PubMed]
- Takeuchi, T.; Tsutsumi, O. Serum bisphenol concentrations showed gender differences, possibly linked to androgen levels. Biochem. Biophys. Res. Commun. 1991, 291, 76–78. [Google Scholar] [CrossRef] [PubMed]
- Moriyama, K.; Tagami, T.; Akamizu, T.; Usui, T.; Saijo, M.; Kanamoto, N.; Hataya, Y.; Shimatsu, A.; Kuzuya, H.; Nakao, K. Thyroid hormone action is disrupted by bisphenol A as an antagonist. J. Clin. Endocrinol. Metab. 2002, 87, 5185–5190. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, M.; Okada, R.; Yamamoto, K.; Nakamura, M.; Mosconi, G.; Polzonetti-Magni, A.M.; Kikuyama, S. Bisphenol A acts differently from and independently of thyroid hormone in suppressing thyrotropin release from the bullfrog pituitary. Gen. Comp. Endocrinol. 2008, 155, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Zoeller, R.T.; Bansal, R.; Parris, C. Bisphenol-A, an environmental contaminant that acts as a thyroid hormone receptor antagonist in vitro, increases serum thyroxine and alters RC3/neurogranin expression in the developing rat brain. Endocrinology 2005, 146, 607–612. [Google Scholar] [CrossRef] [PubMed]
- Minatoya, M.; Sasaki, S.; Araki, A.; Miyashita, C.; Itoh, S.; Yamamoto, J.; Matsumura, T.; Mitsui, T.; Moriya, K.; Cho, K.; et al. Cord Blood Bisphenol A Levels and Reproductive and Thyroid Hormone Levels of Neonates: The Hokkaido Study on Environment and Children’s Health. Epidemiology 2017, 28, S3–S9. [Google Scholar] [CrossRef] [PubMed]
- Mammadov, E.; Uncu, M.; Dalkan, C. High prenatal exposure to bisphenol A reduces anogenital distance in healthy male newborns. J. Clin. Res. Pediatr. Endocrinol. 2017. [CrossRef] [PubMed]
- Fenichel, P.; Dechaux, H.; Harthe, C.; Gal, J.; Ferrari, P.; Pacini, P.; Wagner-Mahler, K.; Pugeat, M.; Brucker-Davis, F. Unconjugated bisphenol A cord blood levels in boys with descended or undescended testes. Hum. Reprod. 2012, 27, 983–990. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Male (n: 55) Mean ± SD | Female (n: 33) Mean ± SD | p Value | |
|---|---|---|---|
| Gestational week | 38.07 ± 2.2 | 38.47 ± 0.83 | 0.135 |
| Birth weight (g) | 3283 ± 537 | 3105 ± 440 | 0.647 |
| Birth height (cm) | 48.51 ± 2.34 | 48.05 ± 1.88 | 0.558 |
| Head circumference (cm) | 34.39 ± 1.77 | 33.70 ± 1.59 | 0.06 |
| TSH (uIu/mL) | 4.87 ± 1.83 | 4.80 ± 1.35 | 0.05 |
| fT4 (ng/dL) | 0.92 ± 0.22 | 0.97 ± 1.92 | 0.89 |
| BPA level (ng/mL) | 4.51 ± 2.06 | 5.48 ± 2.56 | 0.22 |
| BPA Quantile | BPA Level (ng/mL) |
|---|---|
| <20% | 0–2.68 |
| 20–40% 25 | 2.64–3.81 |
| 40–60% 50 | 3.81–5.02 |
| 60–80% 75 | 5.02–7.00 |
| >80% 90 | >7.00 |
| BPA Quantiles | p Value | |||||
|---|---|---|---|---|---|---|
| <20% | 20–40% | 40–60% | 60–80% | >80% | ||
| fT4 (mr*) | 13.00 | 17.00 | 17.08 | 19.58 | 16.60 | 0.916 |
| TSH (mr*) | 20.83 | 15.25 | 23.33 | 14.92 | 14.70 | 0.386 |
| SPINA-GT (mr*) | 10.00 | 20.19 | 13.33 | 18.17 | 18.05 | 0.476 |
| TSHI (mr*) | 20.33 | 15.25 | 23.17 | 15.33 | 14.70 | 0.433 |
| sTSHI (mr*) | 20.33 | 15.25 | 23.17 | 15.33 | 14.70 | 0.433 |
| BPA Quantiles | p Value | |||||
|---|---|---|---|---|---|---|
| <20% | 20–40% | 40–60% | 60–80% | >80% | ||
| fT4 (mr*) | 21.88 | 23.78 | 31.50 | 29.59 | 23.79 | 0.476 |
| TSH (mr*) | 25.08 | 26.33 | 23.92 | 28.18 | 31.29 | 0.859 |
| SPINA-GT (mr*) | 24.71 | 26.11 | 32.00 | 26.68 | 19.57 | 0.50 |
| TSHI (mr*) | 23.92 | 26.22 | 24.62 | 28.73 | 31.29 | 0.829 |
| sTSHI (mr*) | 23.92 | 26.22 | 24.62 | 28.73 | 31.29 | 0.829 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sanlidag, B.; Dalkan, C.; Yetkin, O.; Bahçeciler, N.N. Evaluation of Dose Dependent Maternal Exposure to Bisphenol A on Thyroid Functions in Newborns. J. Clin. Med. 2018, 7, 119. https://doi.org/10.3390/jcm7060119
Sanlidag B, Dalkan C, Yetkin O, Bahçeciler NN. Evaluation of Dose Dependent Maternal Exposure to Bisphenol A on Thyroid Functions in Newborns. Journal of Clinical Medicine. 2018; 7(6):119. https://doi.org/10.3390/jcm7060119
Chicago/Turabian StyleSanlidag, Burcin, Ceyhun Dalkan, Osman Yetkin, and Nerin N. Bahçeciler. 2018. "Evaluation of Dose Dependent Maternal Exposure to Bisphenol A on Thyroid Functions in Newborns" Journal of Clinical Medicine 7, no. 6: 119. https://doi.org/10.3390/jcm7060119
APA StyleSanlidag, B., Dalkan, C., Yetkin, O., & Bahçeciler, N. N. (2018). Evaluation of Dose Dependent Maternal Exposure to Bisphenol A on Thyroid Functions in Newborns. Journal of Clinical Medicine, 7(6), 119. https://doi.org/10.3390/jcm7060119