Assessment of the Pro12Ala Polymorphism in the PPAR-γ2 Gene among Type 2 Diabetes Patients in a Nigerian Population

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population and Design
2.2. Data Collection and Laboratory Analysis
2.3. Genotyping of PPARγ2 Pro12Ala Variant
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristic of Participants
3.2. Obesity and Lipid Profile Indices of Patients
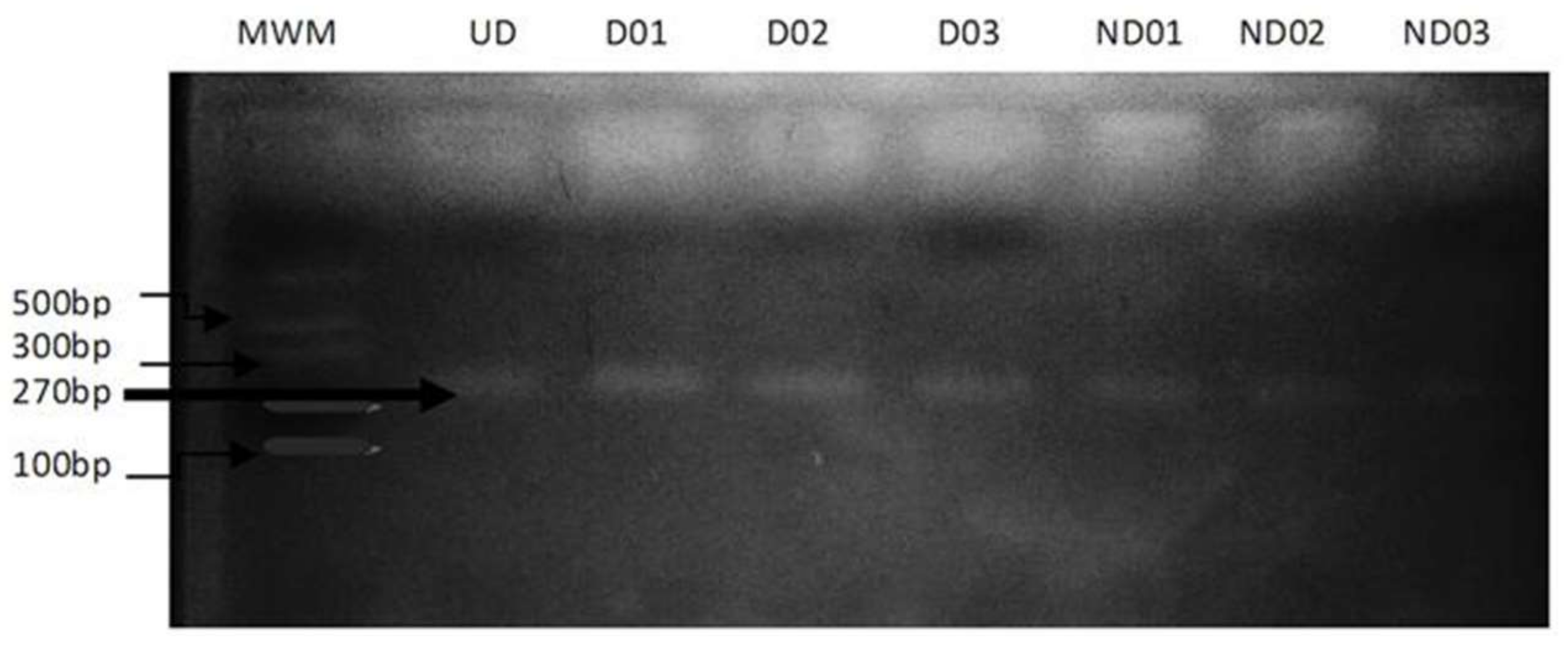
3.3. Genotyping for PPARγ2 Pro12Ala Polymorphism
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. Global Report on Diabetes; WHO Press: Geneva, Switzerland, 2016. [Google Scholar]
- Mokdad, A.H.; Bowman, B.A.; Ford, E.S.; Vinicor, F.; Marks, J.S.; Koplan, J.P. The continuing epidemics of obesity and diabetes in the United States. J. Am. Med. Assoc. 2001, 286, 1195–1200. [Google Scholar] [CrossRef]
- World Health Organization. Obesity and Overweight. WHO Fact Sheet. 2018. Available online: http://www.who.int/mediacentre/factsheets/fs311/en/ (accessed on 21 March 2018).
- Mooradian, A.D. Dyslipidemia in type 2 diabetes mellitus. Nat. Clin. Prac. Endocrinol. Met. 2009, 5, 150–159. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, I.J. Diabetic dyslipidemia: Causes and consequences. J. Clin. Endocrinol. Met. 2001, 8, 965–971. [Google Scholar] [CrossRef] [PubMed]
- Boden, G.; Shulman, G.I. Free fatty acids in obesity and type 2 diabetes: Defining their role in the development of insulin resistance and beta-cell dysfunction. Eur. J. Clin. Investig. 2002, 32, 14–23. [Google Scholar] [CrossRef]
- Blaschke, F.; Takata, Y.; Caglayan, E.; Law, R.E.; Hsueh, W.A. Obesity, peroxisome proliferator activated receptor, and atherosclerosis in type 2 diabetes. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 28–40. [Google Scholar] [CrossRef] [PubMed]
- Desvergne, B.; Wahli, W. Peroxisome proliferator-activated receptors: Nuclear control of metabolism. Endocr. Rev. 1999, 20, 649–688. [Google Scholar] [CrossRef] [PubMed]
- Chawla, A.; Schwarz, E.J.; Dimaculangan, D.D.; Lazar, M.A. Peroxisome proliferator-activated receptor (PPAR) gamma: Adipose-predominant expression and induction early in adipocyte differentiation. Endocrinology 1994, 135, 798–800. [Google Scholar] [CrossRef] [PubMed]
- Tavares, V.; Hirata, R.D.; Rodrigues, A.C.; Monte, O.; Salles, J.E.; Scalissi, N.; Speranza, R.C.; Hirata, M.H. Association between Pro12Ala polymorphism of the PPAR-G2 gene and insulin sensitivity in Brazilian patients with type-2 diabetes mellitus. Diabetes Obes. Metab. 2005, 7, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; St Peter, J.V.; Xue, J.L. A prospective, randomized comparison of the metabolic effects of pioglitazone or rosiglitazone in patients with type 2 diabetes who were previously treated with troglitazone. Diabetes Care 2002, 25, 708–711. [Google Scholar] [CrossRef] [PubMed]
- Stumvoll, M.; Haring, H. The peroxisome proliferator–activated receptor-γ2 Pro12Ala polymorphism. Diabetes 2002, 51, 2341–2347. [Google Scholar] [CrossRef] [PubMed]
- Yen, C.J.; Beamer, B.A.; Negri, C.; Silver, K.; Brown, K.A.; Yarnall, D.P.; Burns, D.K.; Roth, J.; Shuldiner, A.R. Molecular scanning of the human peroxisome proliferator activated receptor gamma (hPPAR gamma) gene in diabetic Caucasians: Identification of a Pro12Ala PPAR gamma 2 missense mutation. Biochem. Biophys. Res. Commun. 1997, 241, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Vigouroux, C.; Fajas, L.; Khallouf, E.; Meier, M.; Gyapay, G.; Lascols, O.; Auwerx, J.; Weissenbach, J.; Capeau, J.; Magre, J. Human peroxisome proliferator activated receptor-gamma2: Genetic mapping, identification of a variant in the coding sequence, and exclusion as the gene responsible for lipoatrophic diabetes. Diabetes 1998, 47, 490–492. [Google Scholar] [CrossRef] [PubMed]
- Deeb, S.S.; Fajas, L.; Nemoto, M.; Pihlajamaki, J.; Mykkanen, L.; Kuusisto, J.; Laakso, M.; Fujimoto, W.; Auwerx, J. A Pro12Ala substitution in PPARγ2 associated with decreased receptor activity, lower body mass index and improved insulin sensitivity. Nat. Genet. 1998, 20, 284–287. [Google Scholar] [CrossRef] [PubMed]
- Mori, H.; Ikegami, H.; Kawaguchi, Y.; Seino, S.; Yokoi, N.; Takeda, J.; Inoue, I.; Seino, Y.; Yasuda, K.; Hanafusa, T.; et al. The Pro12 3Ala substitution in PPAR-γ is associated with resistance to development of diabetes in the general population: Possible involvement in impairment of insulin secretion in individuals with type 2 diabetes. Diabetes 2001, 50, 891–894. [Google Scholar] [CrossRef] [PubMed]
- Scacchi, R.; Pinto, A.; Rickards, O.; Pacella, A.; De Stefano, G.F.; Cannella, C.; Corbo, R.M. An analysis of peroxisome proliferatoractivated receptor gamma (PPAR-gamma2) Pro12Ala polymorphism distribution and prevalence of type 2 diabetes mellitus (T2DM) in world populations in relation to dietary habits. Nutr. Metab. Cardiovasc. Dis. 2007, 17, 632–641. [Google Scholar] [CrossRef] [PubMed]
- Ben Ali, S.; Ben Yahia, F.; Sediri, Y.; Kallel, A.; Ftouhi, B.; Feki, M.; Elasmi, M.; Haj-Taieb, S.; Souheil, O.; Sanhagi, H.; et al. Gender-specific effect of Pro12Ala polymorphism in peroxisome proliferator-activated receptor gamma-2 gene on obesity risk and leptin levels in a Tunisian population. Clin. Biochem. 2009, 42, 1642–1647. [Google Scholar] [CrossRef] [PubMed]
- Mato, E.; Pokam-Fosso, P.; Atogho-Tiedeu, B.; Noubiap, J.; Evehe, M.; Djokam-Dadjeu, R.; Donfack, O.; Ngwa, E.; Guewo-Fokeng, M.; Mbacham, W.; et al. The Pro12Ala polymorphism in the PPAR-γ2 gene is not associated to obesity and type 2 diabetes mellitus in a Cameroonian population. BMC Obes. 2016, 3, 26. [Google Scholar] [CrossRef] [PubMed]
- WHO-IDF. Definition and Diagnosis of Diabetes Mellitus and Intermediate Hyperglycemia: Report of a WHO/IDF Consultation. 2014. Available online: http://www.idf.org/webdata/docs/WHO_IDF_definition_diagnosis_of_diabetes.pdf (accessed on 1 October 2017).
- Trinder, P. Determination of blood glucose using 4-aminophenazone as oxygen acceptor. J. Clin. Pathol. 1969, 22, 1–6. [Google Scholar] [CrossRef]
- Allain, C.C.; Poon, L.S.; Chan, C.S.; Richmond, W. Total cholesterol assay. Clin. Chem. 1974, 20, 470–471. [Google Scholar] [PubMed]
- Esders, T.N.; Michira, C.A. Triglyceride estimation. J. Biol. Chem. 1997, 254, 2710–2712. [Google Scholar]
- Grove, T.H. Grove’s method of high density lipiptotein estimation. Clin. Chem. 1979, 25, 560–562. [Google Scholar] [PubMed]
- Friedwald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma without use of preparative ultracenrifugation. Clin. Chem. 1972, 18, 499–502. [Google Scholar]
- International Diabetes Federation (IDF). IDF Diabetes Atlas, 6th ed.; International Diabetes Federation: Brussels, Belgium, 2013. [Google Scholar]
- Arnaiz-Villena, A.; Fernandez-Honrado, M.; Areces, C.; Enriquez-de-Salamanca, M.; Abd-El-Fatah-Khalil, S.; Coca, C.; Arribas, I.; Algora, M.; Rey, D. Amerindians show no association of PPAR-γ2 gene Ala12 allele and obesity: An “unthrifty” variant population genetics. Mol. Biol. Rep. 2013, 40, 1767–1774. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Narvaez, E. Is the Ala12 variant of the PPARγ gene an “unthrifty allele”? J. Med. Genet. 2005, 42, 547–550. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Stumvoll, M.; Wahl, H.G.; Loblein, K.; Becker, R.; Machicao, F.; Jacob, S.; Haring, H. The Pro12Ala polymorphism in the peroxisome proliferator–activated receptor-2 gene (PPARγ2) is associated with increased antilipolytic insulin sensitivity. Diabetes 2001, 50, 876–881. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Stumvoll, M.; Haring, H. Reduced lipolysis as possible cause for greater weight gain in subjects with the Pro12Ala polymorphism in PPARγ2. Diabetologia 2001, 45, 152–153. [Google Scholar]
- Danquah, I.; Othmer, T.; Frank, K.L.; Bedu-Addo, G.; Schulze, M.B.; Mockenhaupt, F.P. The TCF7L2 rs7903146 (T) allele is associated with type 2 diabetes in urban Ghana: A hospital-based case–control study. BMC Med. Genet. 2013, 14, 96. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.S.; Li, J.; Jin, Y.L.; Chen, Y.; He, L.P. Association between PPARγ2 Pro12Ala polymorphism and obesity: A meta-analysis. Mol. Biol. Rep. 2014, 41, 8211–8217. [Google Scholar]


{kind=link}
| Characteristics | T2D Patients | ND Patients | p-Value |
|---|---|---|---|
| Age (years) | 56.83 ± 1.21 | 49.03 ± 1.89 | 0.001 |
| Height (m) | 1.58 ± 0.01 | 1.61 ± 0.01 | 0.179 |
| Weight (kg) | 78.85 ± 3.42 | 71.52 ± 1.95 | 0.043 |
| SBP (mmHg) | 132.69 ± 2.65 | 132.86 ± 3.23 | 0.967 |
| DSP (mmHg) | 78.80 ± 1.36 | 81.76 ± 2.24 | 0.240 |
| FBS (mg/dL) | 166.71 ± 11.39 | 65.75 ± 3.79 | 0.000 |
| Parameter | T2D Patients | n (%) | ND Patients | n (%) | p-Value |
|---|---|---|---|---|---|
| BMI (Kg/m2) | 31.38 ± 1.41 | 31 (21.1) | 27.81 ± 0.76 | 22 (15.0) | 0.026 |
| WC (cm) | 100.15 ± 1.70 | 53 (36.1) | 89.37 ± 2.25 | 32 (21.8) | <0.001 |
| TC (mg/dL) | 291.78 ± 28.90 | 58 (39.4) | 159.43 ± 7.77 | 11 (7.5) | <0.001 |
| TG (mg/dL) | 241.33 ± 15.443 | 60 (40.8) | 148.82 ± 7.59 | 31 (21.1) | <0.001 |
| LDL (mg/dL) | 212.40 ± 29.42 | 41 (27.8) | 78.96 ± 7.96 | 9 (6.2) | <0.001 |
| HDL (mg/dL) | 33.55 ± 2.14 | 45 (30.6%) | 62.74 ± 5.16 | 25 (17.0%) | <0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Engwa, G.A.; Nwalo, F.N.; Chiezey, V.O.; Unachukwu, M.N.; Ojo, O.O.; Ubi, B.E. Assessment of the Pro12Ala Polymorphism in the PPAR-γ2 Gene among Type 2 Diabetes Patients in a Nigerian Population. J. Clin. Med. 2018, 7, 69. https://doi.org/10.3390/jcm7040069
Engwa GA, Nwalo FN, Chiezey VO, Unachukwu MN, Ojo OO, Ubi BE. Assessment of the Pro12Ala Polymorphism in the PPAR-γ2 Gene among Type 2 Diabetes Patients in a Nigerian Population. Journal of Clinical Medicine. 2018; 7(4):69. https://doi.org/10.3390/jcm7040069
Chicago/Turabian StyleEngwa, Godwill Azeh, Friday Nweke Nwalo, Venatus Osita Chiezey, Marian N. Unachukwu, Opeolu Oyejide Ojo, and Benjamin Ewa Ubi. 2018. "Assessment of the Pro12Ala Polymorphism in the PPAR-γ2 Gene among Type 2 Diabetes Patients in a Nigerian Population" Journal of Clinical Medicine 7, no. 4: 69. https://doi.org/10.3390/jcm7040069
APA StyleEngwa, G. A., Nwalo, F. N., Chiezey, V. O., Unachukwu, M. N., Ojo, O. O., & Ubi, B. E. (2018). Assessment of the Pro12Ala Polymorphism in the PPAR-γ2 Gene among Type 2 Diabetes Patients in a Nigerian Population. Journal of Clinical Medicine, 7(4), 69. https://doi.org/10.3390/jcm7040069