Accuracy of Commonly-Used Imaging Modalities in Assessing Left Atrial Appendage for Interventional Closure: Review Article

 ,
,
Abstract
1. Introduction
1.1. 3D TEE Modality Is Superior to 2D TEE
1.2. CT Is More Accurate Than TEE
1.3. The Use of 3D Printing Can Facilitate LAA Occlusion
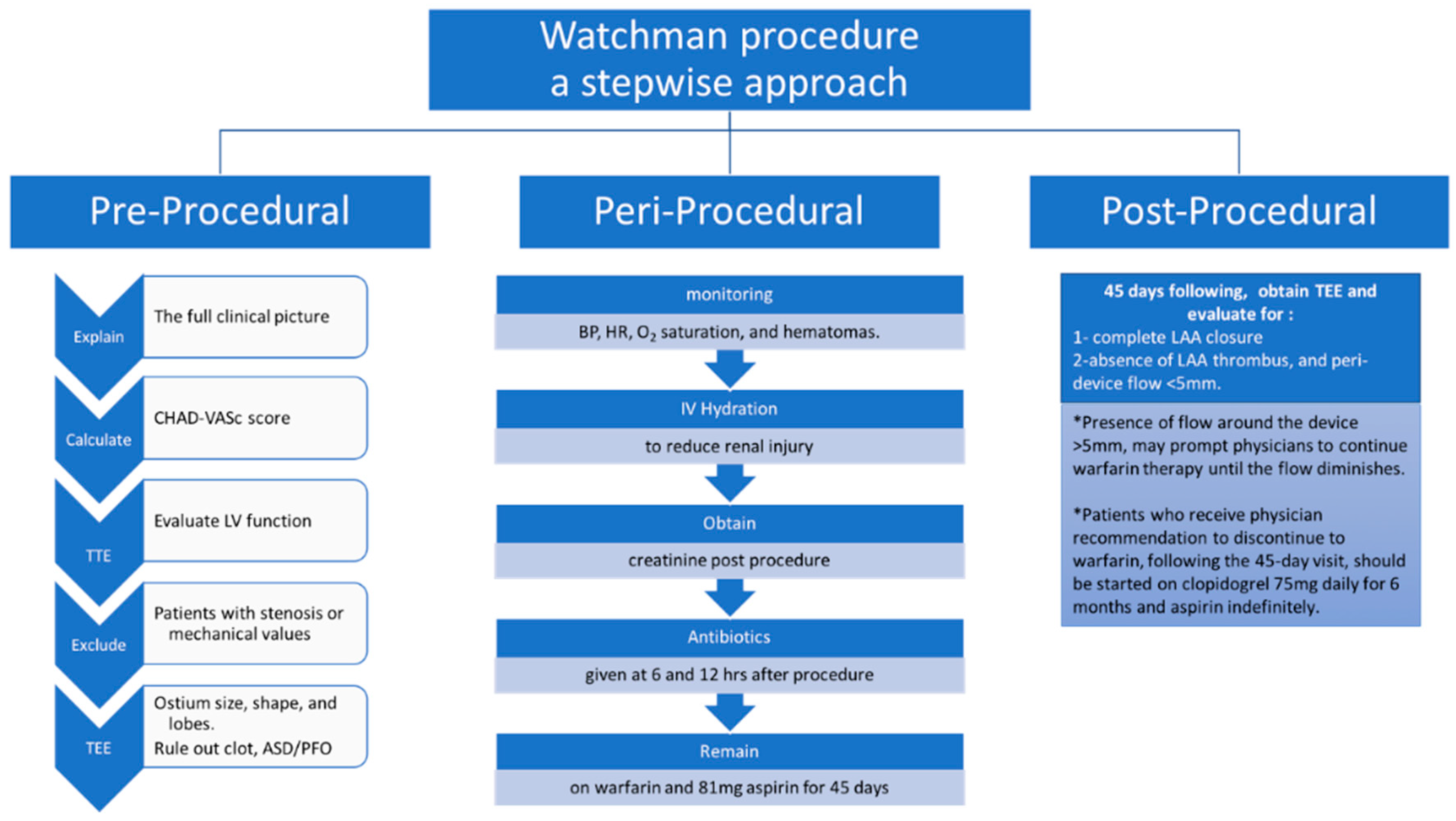
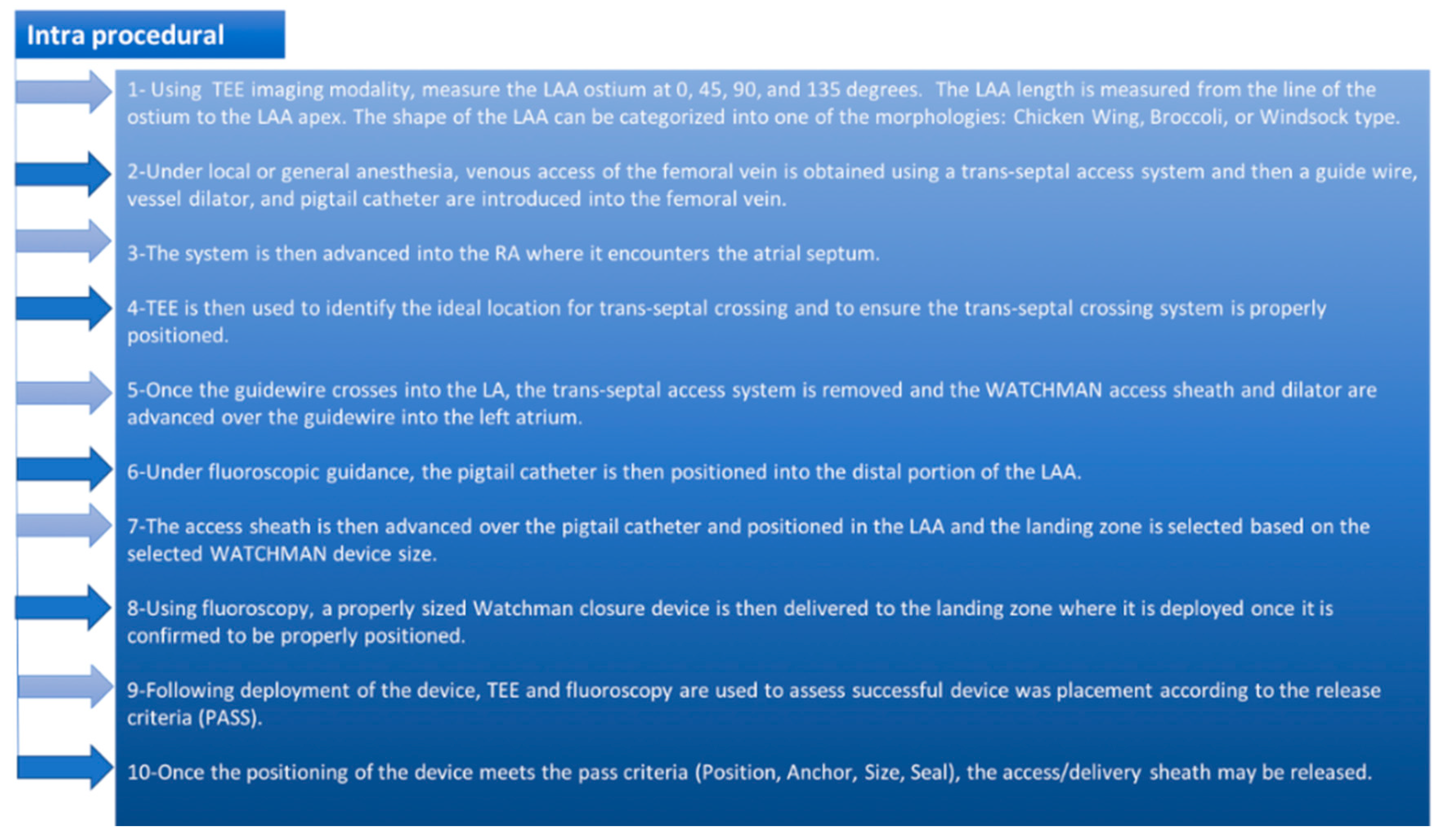
2. Algorithmic Approach for the WATCHMAN Procedural
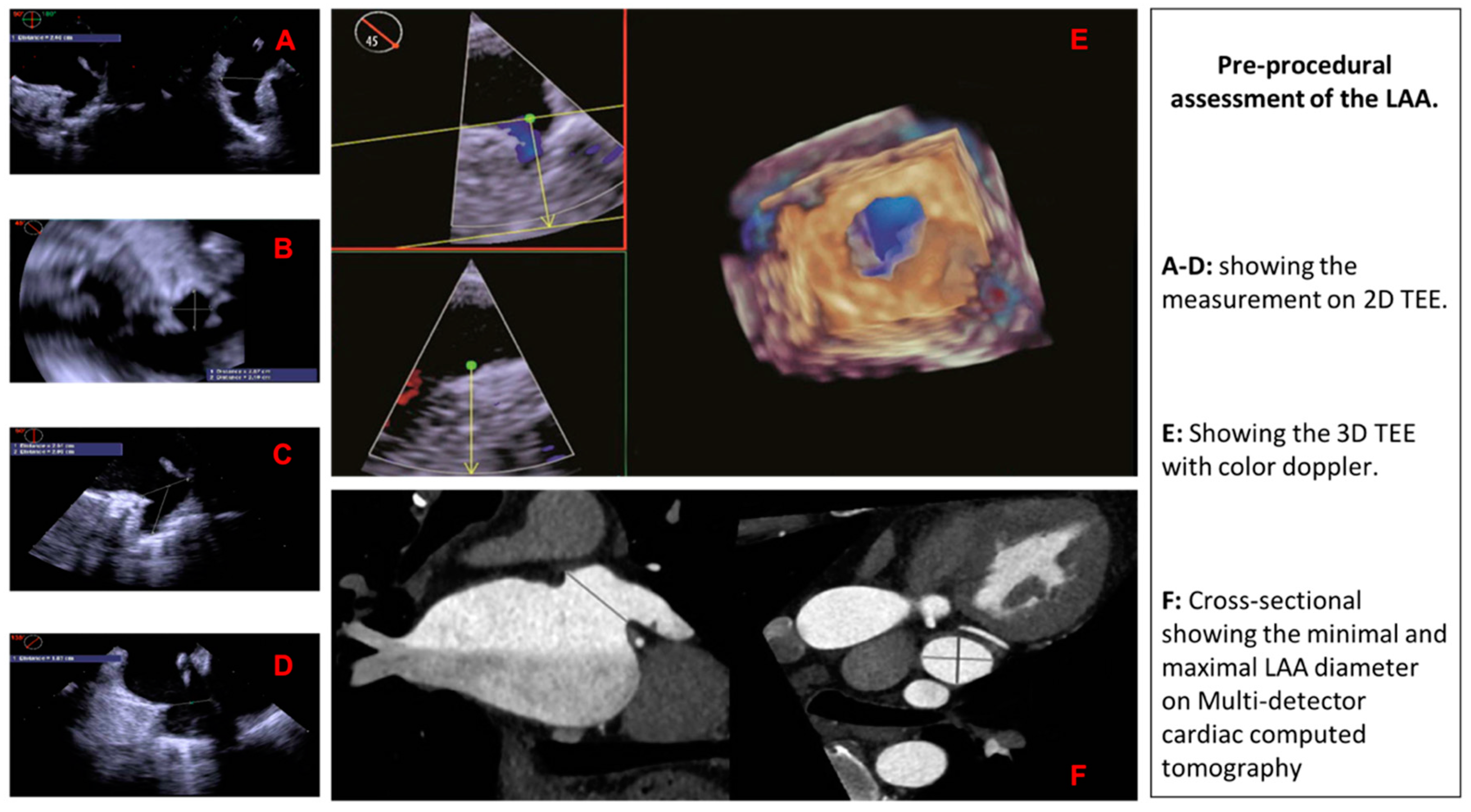
3. Pre-Procedural Assessment of the LAA
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Reiffel, J.A. Atrial fibrillation and stroke: Epidemiology. Am. J. Med. 2014, 127, e15–e16. [Google Scholar] [CrossRef] [PubMed]
- Sievert, H.; Lesh, M.D.; Trepels, T.; Omran, H.; Bartorelli, A.; Della Bella, P.; Nakai, T.; Reisman, M.; DiMario, C.; Block, P.; et al. Percutaneous left atrial appendage transcatheter occlusion to prevent stroke in high-risk patients with atrial fibrillation: Early clinical experience. Circulation 2002, 105, 1887–1889. [Google Scholar] [CrossRef] [PubMed]
- Go, A.S.; Hylek, E.M.; Borowsky, L.H.; Phillips, K.A.; Selby, J.V.; Singer, D.E. Warfarin use among ambulatory patients with nonvalvular atrial fibrillation: The anticoagulation and risk factors in atrial fibrillation (ATRIA) study. Ann. Intern. Med. 1999, 131, 927–934. [Google Scholar] [CrossRef] [PubMed]
- Wunderlich, N.C.; Beigel, R.; Swaans, M.J.; Ho, S.Y.; Siegel, R.J. Percutaneous interventions for left atrial appendage exclusion: Options, assessment, and imaging using 2D and 3D echocardiography. JACC Cardiovasc. Imaging 2015, 8, 472–488. [Google Scholar] [CrossRef] [PubMed]
- Holmes, D.R.; Reddy, V.Y.; Turi, Z.G.; Doshi, S.K.; Sievert, H.; Buchbinder, M.; Mulli, M.; Sick, P. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: A randomised non-inferiority trial. Lancet 2009, 374, 534–542. [Google Scholar] [CrossRef]
- Kamiński, R.; Kosiński, A.; Brala, M.; Piwko, G.; Lewicka, E.; Dąbrowska-Kugacka, A.; Raczak, G.; Kozłowski, D.; Grzybiak, M. Variability of the Left Atrial Appendage in Human Hearts. PLoS ONE 2015, 10, e0141901. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Q.; Song, H.; Zhang, L.; Deng, Q.; Chen, J.; Hu, B.; Wang, Y.; Guo, R. Roles of real-time three-dimensional transesophageal echocardiography in peri-operation of transcatheter left atrial appendage closure. Medicine 2017, 96, e5637. [Google Scholar] [CrossRef] [PubMed]
- Schmidt-Salzmann, M.; Meincke, F.; Kreidel, F.; Spangenberg, T.; Ghanem, A.; Kuck, K.H.; Bergmann, M.W. Improved Algorithm for Ostium Size Assessment in Watchman Left Atrial Appendage Occlusion Using Three-Dimensional Echocardiography. J. Invasive Cardiol. 2017, 29, 232–238. [Google Scholar] [PubMed]
- Wang, D.D.; Eng, M.; Kupsky, D.; Myers, E.; Forbes, M.; Rahman, M.; Zaidan, M.; Parikh, S.; Wyman, J.; Pantelic, M.; et al. Application of 3-Dimensional Computed Tomographic Image Guidance to WATCHMAN Implantation and Impact on Early Operator Learning Curve: Single-Center Experience. JACC Cardiovasc. Interv. 2016, 9, 2329–2340. [Google Scholar] [CrossRef] [PubMed]
- Yosefy, C.; Laish-Farkash, A.; Azhibekov, Y.; Khalameizer, V.; Brodkin, B.; Katz, A. A New Method for Direct Three-Dimensional Measurement of Left Atrial Appendage Dimensions during Transesophageal Echocardiography. Echocardiography 2016, 33, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Nucifora, G.; Faletra, F.F.; Regoli, F.; Pasotti, E.; Pedrazzini, G.; Moccetti, T.; Auricchio, A. Evaluation of the left atrial appendage with real-time 3-dimensional transesophageal echocardiography: Implications for catheter-based left atrial appendage closure. Circ. Cardiovasc. Imaging 2011, 4, 514–523. [Google Scholar] [CrossRef] [PubMed]
- Yosefy, C.; Azhibekov, Y.; Brodkin, B.; Khalameizer, V.; Katz, A.; Laish-Farkash, A. Rotational method simplifies 3-dimensional measurement of left atrial appendage dimensions during transesophageal echocardiography. Cardiovasc. Ultrasound 2016, 14, 36. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, H.; Seo, Y.; Ishizu, T.; Yamamoto, M.; Machino, T.; Harimura, Y.; RyoKawamura, R.; Sekiguchi, Y.; Tada, H.; Aonuma, K. Analysis of the left atrial appendage by three-dimensional transesophageal echocardiography. Am. J. Cardiol. 2010, 106, 885–892. [Google Scholar] [CrossRef] [PubMed]
- Chow, D.H.; Bieliauskas, G.; Sawaya, F.J.; Millan-Iturbe, O.; Kofoed, K.F.; Søndergaard, L.; De Backer, O. A comparative study of different imaging modalities for successful percutaneous left atrial appendage closure. Open Heart 2017, 4, e000627. [Google Scholar] [CrossRef] [PubMed]
- Rajwani, A.; Nelson, A.J.; Shirazi, M.G.; Disney, P.J.; Teo, K.S.; Wong, D.T.; Young, G.D.; Worthley, S.G. CT sizing for left atrial appendage closure is associated with favourable outcomes for procedural safety. Eur. Heart J. Cardiovasc. Imaging 2017, 18, 1361–1368. [Google Scholar] [CrossRef] [PubMed]
- Budge, L.P.; Shaffer, K.M.; Moorman, J.R.; Lake, D.E.; Ferguson, J.D.; Mangrum, J.M. Analysis of in vivo left atrial appendage morphology in patients with atrial fibrillation: A direct comparison of transesophageal echocardiography, planar cardiac CT, and segmented three-dimensional cardiac CT. J. Interv. Card. Electrophysiol. 2008, 23, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.A.N.; Di Biase, L.; Horton, R.P.; Nguyen, T.; Morhanty, P.; Natale, A. Left atrial appendage studied by computed tomography to help planning for appendage closure device placement. J. Cardiovasc. Electrophysiol. 2010, 21, 973–982. [Google Scholar] [CrossRef] [PubMed]
- Hell, M.M.; Achenbach, S.; Yoo, I.S.; Franke, J.; Blachutzik, F.; Roether, J.; Graf, V.; Raaz-Schrauder, D.; Marwan, D.; Schlundt, C. 3D printing for sizing left atrial appendage closure device: Head-to-head comparison with computed tomography and transoesophageal echocardiography. EuroIntervention 2017, 13, 1234–1241. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Shu, M.; Wang, X.; Song, Z. Application of 3D printing technology to left atrial appendage occlusion. Int. J. Cardiol. 2017, 231, 258–263. [Google Scholar] [CrossRef] [PubMed]
- Goitein, O.; Fink, N.; Guetta, V.; Beinart, R.; Brodov, Y.; Konen, E.; Goitein, D.; Di Segni, E.; Grupper, A.; Glikson, M. Printed MDCT 3D models for prediction of left atrial appendage (LAA) occluder device size: A feasibility study. EuroIntervention 2017, 13, e1076–e1079. [Google Scholar] [CrossRef] [PubMed]
- Möbius-Winkler, S.; Sandri, M.; Mangner, N.; Lurz, P.; Dähnert, I.; Schuler, G. The WATCHMAN left atrial appendage closure device for atrial fibrillation. J. Vis. Exp. 2012. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Author | Advantages of 3D TEE vs. 2D TEE | Study |
|---|---|---|
| Zhou et al. | -More accurate measuring of Landing zone and depth -More significant association between the closure device -Displaying cross-sectional images from any angle using Flexi Slice mode -Useful in displaying the LAA morphology after the occlusion device deployed -Visualizing any residual shunts around the entire device in one more view | [7] |
| Salzman et al. | -Producing (ADD) and (PDD) measurements of the LAA ostium -3D landing zone measurements demonstrated a higher reproducibility | [8] |
| Yosefi et al. | -3DTEE is a feasible, fast way to assess LAA morphology with similar accuracy to RT3DTEE and CT | [10] |
| Nucifora et al. | -RT3DTEE more significant agreement with the dimensions obtained from CT -RT3DTEE Provide accurate measurements without radiation exposure or contrast | [11] |
| Yosefi et al. | -RT3DTEE provides more accurate measurements of the maximal LAA orifice | [12] |
| Nakajima et al. | -Accurately visualize LAA morphological variations -Excellent correlation was found between full volume mode and zoom mode | [13] |
| Ref | Author | Country | Date (mm/dd) | Objective | Study | Result/Outcome | Conclusion |
|---|---|---|---|---|---|---|---|
| [7] | Zhou et al. | China | 01/17 | To determine the clinical values of RT-3D TEE in the peri-procedure of LAA closure. | Observational study, of 38 patients conducted real-time 3D TEE (3D TEE) of the LAA for all subjects | -The landing zone dimension of LAA revealed by 2D TEE, showed statistical difference compared with the dimensions obtained from the 3D TEE -No statistical difference was noticed in the landing zone values of 3D TEE compared with that of X-ray -No statistical difference was noticed in the landing zone values of 3D TEE compared with that of X-ray | RT-3D TEE has better visualization of the LAA compared with 2D TEE. |
| [8] | Salzman et al. | Germany | 07/17 | To establish measurements based on 3D TEE imaging that would be most helpful in achieving successful cardiovascular intervention | Retrospective study analyzed 55 patient who underwent LAA occlusion using Watchman | ADD) and perimeter-derived diameter (PDD) from 3D TEE can reduce intra-procedural recapture maneuvers, peridevice leakage, and device size changes compared with two-dimensional (2D) measurements. | 3D ADD and PDD may help with reducing intraprocedural recapture maneuvers, device size changes, and peridevice leakage. |
| [10] | Yosefi et al. | Israel | 01/16 | Compared RT3DTEE and 2DTEE versus CT when measuring LAA dimensions | Prospective study of 30 patients compared RT 3D TEE and 2D TEE versus 64 slice CT for measuring LAA dimensions | No difference was found between LAA depth using RT 3D TEE (19.5 ± 2.3 mm) vs. CT (19.6 ± 2.3, P = NS) and 2D TEE (19.4 ± 2.2 mm) vs. CT (P = NS). However, RT 3D TEE (24.5 ± 4.7 mm) vs. CT (24.6 ± 5, P = NS) was more accurate in measuring maximal LAA diameter compared to 2D TEE (23.5 ± 3.9 mm) vs. CT (P < 0.01). | RT3DTEE provides more accurate measurements of the maximal LAA orifice than 2D TEE. |
| [11] | Nucifora et al. | Switzerland | 09/11 | The accuracy of the measurements obtained via 2DTEE and RT3DTEE were subsequently compared against measurements obtained via CT. | Prospective study of 137 patients who underwent 2DTEE, RT3DTEE, and CT to measure the dimensions of the LAA orifice | -Compared to CT, both 2DTEE and RT3DTEE underestimated LAA dimensions. -RT3DTEE was found to be in greater agreement with the dimensions obtained from CT as demonstrated by smaller bias and narrower limits of agreement with CT | RT3DTEE may be the preferable imaging modality to assess LAA dimensions. |
| [12] | Yosefi et al. | Israel | 09/16 | To validate the accuracy of Rotational 3DTEE versus RT3DTEE when assessing LAA | Prospective study of 41 patients who underwent a rotational 3D TEE | Rotational 3D TEE measurements of LAA were not statistically different from RT3DTEE and from 64-slice CT regarding Rotational 3D TEE is achieved by rotating the sagittal plane (in the green box, x-plane) 360° and allows for a faster method of achieving necessary LAA measurements. | Choosing the appropriate device size for LAA closure can be achieved by Rotational 3DTEE (“Yosefy rotation”). |
| [13] | Nakajima et al. | Japan | 09/10 | To determined if 3D TEE could accurately visualize LAA morphological variations | Prospective od 107 patients, 55 were in SR in whom 3DTEE images were obtained from full-volume mode imaging, and 52 were in Afib, zoom-mode imaging was used. | 3D TEE proviced adequate 3D full volume images of all patients in NSR, whereas adequate images were obtained in 94.6% of patients with AF using zoom mode. Excellent correlation was found between full volume mode and zoom mode. | 3D TEE is a reliable modality when evaluating LAA geometry and LAA characteristics. |
| Author | Advantages of CT | Study |
|---|---|---|
| Chow et al. | -Allows more accurate assessment of the LAA ostium and landing zone. -Allows higher appreciation for the morphology of the LAA and surrounding structures | [14] |
| Rawjani et al. | -device sizing by CT-derived mean diameter was in most agreement with the actual device implanted -Better in detection and avoidance of sizing error by 2D TOE | [15] |
| Wang et al. | -WATCHMAN device selection was 100% accurate when selected by CT imaging -Provides a comprehensive assessment for LAA which is accurate | [9] |
| Budge et al. | -Provides accurate sizing of LAA occlusion devices | [16] |
| Ref | Author | Country | Date (mm/dd) | Objective | Study | Result/Outcome | Conclusion |
|---|---|---|---|---|---|---|---|
| [14] | Chow et al. | Denmark | 06/17 | To compare available LAA imaging and sizing modalities which lead to successful LAA closure | Retrospective, 67 patients who underwent preprocedural MSCT and 2D TEE for LAA closure device sizing from 2014 to 2016 | MSCT resulted in correct LAA sizing in 83% of patients, whereas 2D TEE would have produced in only 57% proper sizing | CT derived PD mean diameter may be the optimal measurement for sizing ‘closed-ended’ devices (Amulet and WATCHMANFLX) whereas CT derived maximal diameter is more accurate for sizing ‘open-ended’ devices (WATCHMAN) |
| [15] | Rawjani et al. | Australia | 12/17 | To evaluate the use of CT, procedural safety, and outcomes for percutaneous LAA closure | A registry between July 2010 and December 2015 was prospectively established for individuals undergoing LAA closure | 2D TEE sizing resulted in gross sizing errors in 3.4% of cases. 2D-TEE measurements resulted in device selection that was 3mm smaller than those from CT measurements | CT has excellent outcomes for procedural safety with absence of major residual leak |
| [9] | Wang et al. | USA | 11/16 | To determine the role of 3DCT guided planning for LAA occlusion on the early operator WATCHMAN learning curve | Prospective study studied 53 patients who underwent 2D TEE, 3D TEE, and 3D CT for Watchman device qualification and sizing | 53 patients underwent successful device implantation. Compared with 2D and 3D TEE sizing, 3D CT maximal width of the LAA landing zone was larger (p ≤ 0.0001). Pearson correlation coefficient showed a significant difference when sizing by CT against TEE (r < 0.001) | 3D CT is an excellent tool in advanced case planning for precise WATCHMAN device size selection in LAA closure procedures compared to standard 2D TEE |
| [16] | Budge et al. | USA | 11/08 | To compare multiple different imaging modalities to assess the morphology of the LAA in AF patients | Prospective study of 66 patients where measurement relationships of TEE to planar CT (CTp), CTp to 3D cardiac segmented CT (CTsg), and CTsg to TEE were compared | Similar to CTp, CTsg orifice values were usually slightly smaller than TEE for large orifices, and larger than TEE for smaller orifices. LAA orifice measurements among CTsg, CTp, and TEE are not interchangeable which is clinically significant because of the need of accurate sizing of LAA occlusion devices | CTsg, either alone or in conjunction with TEE measurements, could allow for more accurate initial device sizing |
| Ref | Author | Country | Date (mm/dd) | Objective | Study | Result/Outcome | Conclusion |
|---|---|---|---|---|---|---|---|
| [17] | Hell et al. | Europe | 11/17 | To determine If using 3D-printed LAA models based on CT will permit accurate device sizing | Prospective study of 22 patients who underwent pre-procedure TEE and CT examinations in which a 3D printed model was created based on the CT images and CT measurements recorded. | -Implantation was successful in all patients -In 95% of the patients (21/22), predicted device size based on simulated implantation in the 3D model was equal to the device ultimately implanted. TEE would have undersized the device in 45% of the patients (10/22) and device compression determined in the 3D-CT model corresponded closely with compression upon implantation of Watchman device (r = 0.622, p = 0.003). | CT 3D-printing models may assist with device selection and the prediction of device compression. |
| [18] | Li et al. | China | 03/17 | To assess 3DP feasibility using CT for LAA closure | Prospective study for 42 patients were randomly split into 2 groups, one that had 3D LAA model printing and a control group. For the control group, device size was was based on TEE, cardiac CT angiogram, and intraoperative LAA angiography only | The diameter of the occlusion devices used in the 3DP group and control group were 27.6 ± 2.4 mm (21–33 mm) and 26.3 ± 3.4 mm (21–33 mm), respectively. TOE showed that the compression ratios of the occlusion devices were 19.7% ± 0.8% and 19.3 ± 1.0% (p = 0.05), respectively. | 3DP enhance the work efficiency for LAA closure which is valuable for clinical application. |
| [19] | Goiten et al. | Israel | 10/17 | To determine the feasibility of MDCT when predicting the accurate size of device for LAA closure | Prospective study including 29 patients compared 3D LAA model printing for predicting occlusion device size based on pre-procedure CT scan Amplatzer Amulet (St. Jude Medical/Abbott) was deployed in 12 patients and the other 17 received the Watchman device | Two procedures were aborted due to mismatch between LAA and any Watchman device dimensions in which all three interventional cardiology physicians that were involved in the study predicted the failures using the printed 3D model According to Bland-Altman analysis, the average difference between the predicted Amulet size using the 3D LAA printed model and the inserted Amulet was 0.848 mm (95% limit of agreement (LOA): −4.215, 5.912). The average difference between the predicted Watchman size using the 3D print and the inserted Watchman was 0.956 mm (95% LOA: −6.534, 8.445) | LAA 3DP model is not accurate for prediction of LAA using WATCHMAN devi. |
| Imaging Modality | Impact on Implantation Success |
|---|---|
| 2D TEE | Less accurate |
| 3D TEE | Accurate without requiring radiation exposure or contrast administration |
| 3D CT | Exceptional accuracy when merged with three-dimensional printing technology |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morcos, R.; Al Taii, H.; Bansal, P.; Casale, J.; Manam, R.; Patel, V.; Cioci, A.; Kucharik, M.; Malhotra, A.; Maini, B. Accuracy of Commonly-Used Imaging Modalities in Assessing Left Atrial Appendage for Interventional Closure: Review Article. J. Clin. Med. 2018, 7, 441. https://doi.org/10.3390/jcm7110441
Morcos R, Al Taii H, Bansal P, Casale J, Manam R, Patel V, Cioci A, Kucharik M, Malhotra A, Maini B. Accuracy of Commonly-Used Imaging Modalities in Assessing Left Atrial Appendage for Interventional Closure: Review Article. Journal of Clinical Medicine. 2018; 7(11):441. https://doi.org/10.3390/jcm7110441
Chicago/Turabian StyleMorcos, Ramez, Haider Al Taii, Priya Bansal, Joel Casale, Rupesh Manam, Vikram Patel, Anthony Cioci, Michael Kucharik, Arjun Malhotra, and Brijeshwar Maini. 2018. "Accuracy of Commonly-Used Imaging Modalities in Assessing Left Atrial Appendage for Interventional Closure: Review Article" Journal of Clinical Medicine 7, no. 11: 441. https://doi.org/10.3390/jcm7110441
APA StyleMorcos, R., Al Taii, H., Bansal, P., Casale, J., Manam, R., Patel, V., Cioci, A., Kucharik, M., Malhotra, A., & Maini, B. (2018). Accuracy of Commonly-Used Imaging Modalities in Assessing Left Atrial Appendage for Interventional Closure: Review Article. Journal of Clinical Medicine, 7(11), 441. https://doi.org/10.3390/jcm7110441