An Inverse Relationship between Hyperuricemia and Mortality in Patients Undergoing Continuous Ambulatory Peritoneal Dialysis

Abstract
1. Introduction
2. Patients and Methods
3. Statistical Analysis
4. Results
4.1. Patient Characteristics
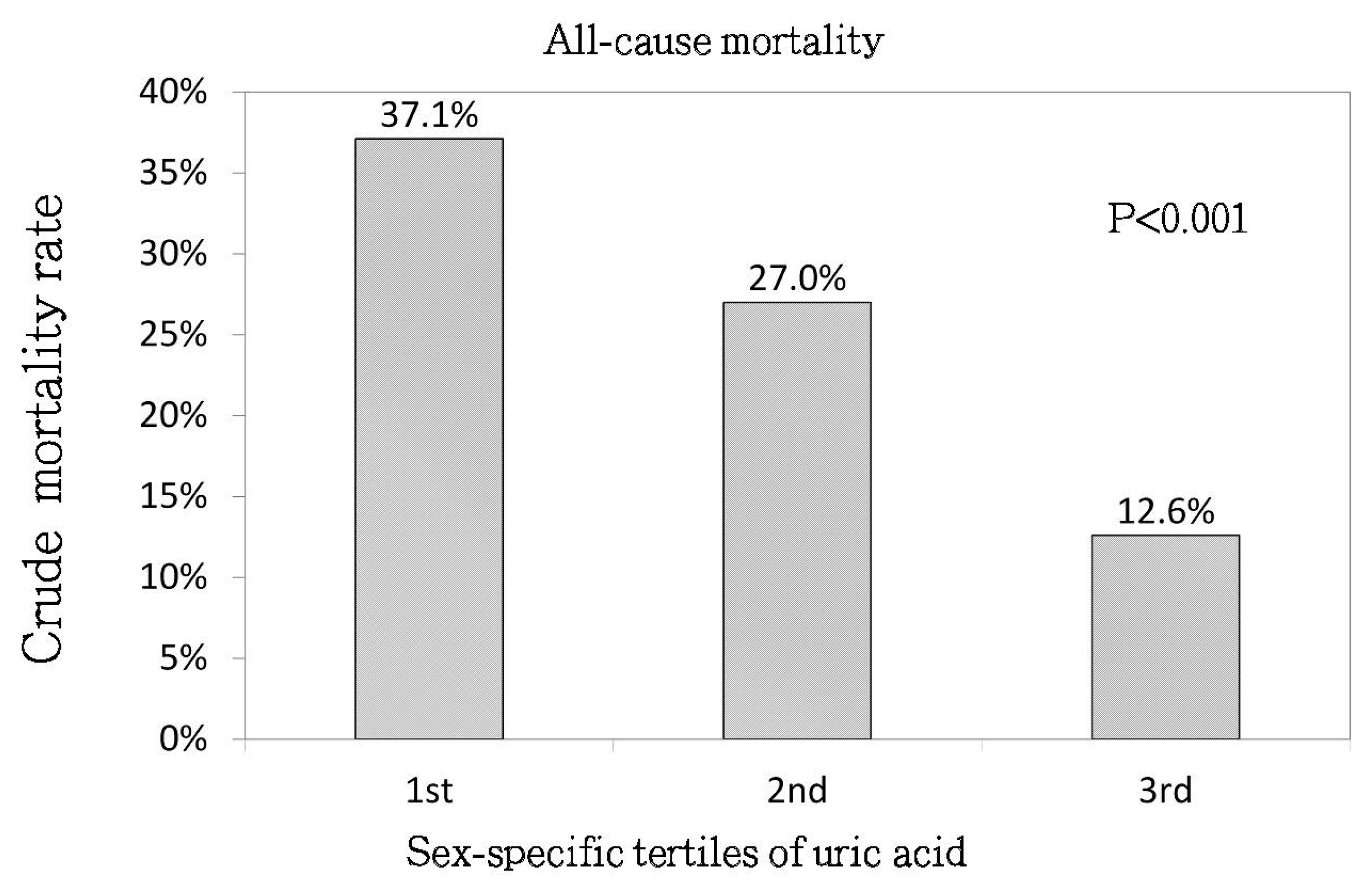
4.2. Uric Acid (Sex-Specific Tertiles) and All-Cause Mortality
4.3. Uric Acid (Sex-Specific Tertiles) and CV Mortality
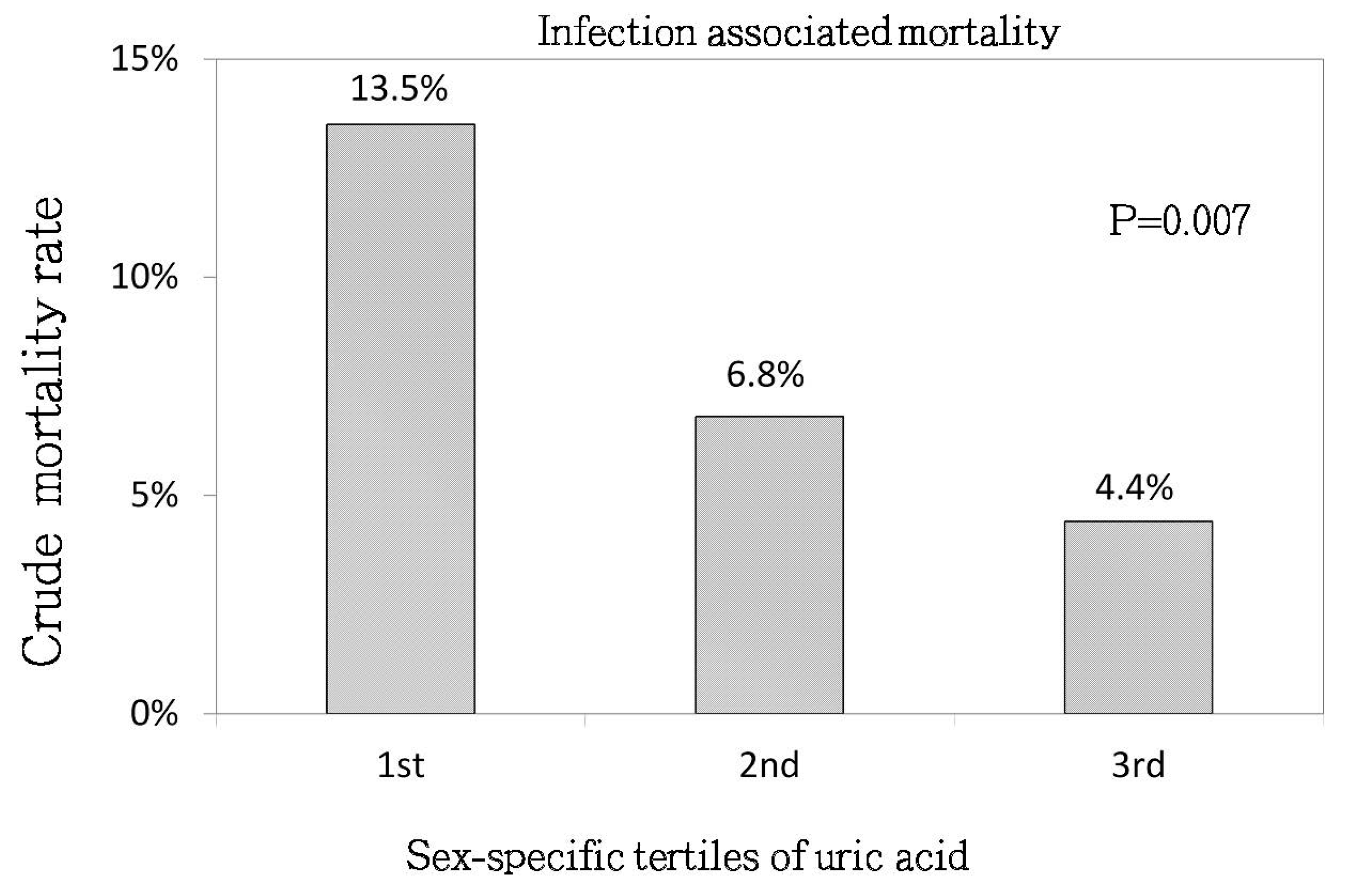
4.4. Uric Acid (Sex-Specific Tertiles) and Infection-Associated Mortality
4.5. The Association between Mortality and Non-Sex-Specific Uric Acid Tertiles
4.6. Sensitivity Analysis
4.7. The Correlation of UA with Other Parameters
4.8. Stratified Analyses
5. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Harrison, R. Structure and function of xanthine oxidoreductase: Where are we now? Free Radic. Biol. Med. 2002, 33, 774–797. [Google Scholar] [CrossRef]
- Mwasongwe, S.E.; Fülöp, T.; Katz, R.; Musani, S.K.; Sims, M.; Correa, A.; Flessner, M.G.; Young, B.A. Relation of uric acid level to rapid kidney function decline and development of kidney disease: The Jackson Heart Study. J. Clin. Hypertens. 2018, 20, 775–783. [Google Scholar] [CrossRef] [PubMed]
- Elsayed, E.F.; Tighiouart, H.; Griffith, J.; Kurth, T.; Levey, A.S.; Salem, D.; Sarnak, M.J.; Weiner, D.E. Cardiovascular disease and subsequent kidney disease. Arch. Intern. Med. 2007, 167, 1130–1136. [Google Scholar] [CrossRef] [PubMed]
- Collins, A.J.; Foley, R.N.; Chavers, B.; Gilbertson, D.; Herzog, C.; Johansen, K.; Kasiske, B.; Kutner, N.; Liu, J.; St Peter, W.; et al. United States Renal Data System 2011 annual data report: Atlas of chronic kidney disease and end-stage renal disease in the United States. Am. J. Kidney Dis. 2012, 59, e1–e420. [Google Scholar]
- Niskanen, L.K.; Laaksonen, D.E.; Nyyssonen, K.; Alfthan, G.; Lakka, H.M.; Lakka, T.A.; Salonen, J.T. Uric acid level as a risk factor for cardiovascular and all-cause mortality in middle-aged men: A prospective cohort study. Arch. Intern. Med. 2004, 164, 1546–1551. [Google Scholar] [CrossRef] [PubMed]
- Iwashima, Y.; Horio, T.; Kamide, K.; Rakugi, H.; Ogihara, T.; Kawano, Y. Uric acid, left ventricular mass index, and risk of cardiovascular disease in essential hypertension. Hypertension 2006, 47, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Madero, M.; Sarnak, M.J.; Wang, X.; Greene, T.; Beck, G.J.; Kusek, J.W.; Collins, A.J.; Levey, A.S.; Menon, V. Uric acid and long-term outcomes in CKD. Am. J. Kidney Dis. 2009, 53, 796–803. [Google Scholar] [CrossRef] [PubMed]
- Kanbay, M.; Yilmaz, M.I.; Sonmez, A.; Solak, Y.; Saglam, M.; Cakir, E.; Unal, H.U.; Arslan, E.; Verim, S.; Madero, M.; et al. Serum uric acid independently predicts cardiovascular events in advanced nephropathy. Am. J. Nephrol. 2002, 36, 324–331. [Google Scholar] [CrossRef] [PubMed]
- Ben-Dov, I.Z.; Kark, J.D. Serum uric acid is a GFR-independent long-term predictor of acute and chronic renal insufficiency: The Jerusalem Lipid Research Clinic cohort study. Nephrol. Dial. Transplant. 2011, 26, 2558–2566. [Google Scholar] [CrossRef] [PubMed]
- Alderman, M. Uric acid in hypertension and cardiovascular disease. Can. J. Cardiol. 1999, 15, S20F–S22F. [Google Scholar]
- Culleton, B.F.; Larson, M.G.; Kannel, W.B.; Levy, D. Serum uric acid and risk for cardiovascular disease and death: The Framingham Heart Study. Ann. Intern. Med. 1999, 131, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Suliman, M.E.; Johnson, R.J.; García-López, E.; Qureshi, A.R.; Molinaei, H.; Carrero, J.J.; Heimbürger, O.; Bárány, P.; Axelsson, J.; Lindholm, B.; et al. J-shaped mortality relationship for uric acid in CKD. Am. J. Kidney Dis. 2006, 48, 761–771. [Google Scholar] [CrossRef] [PubMed]
- Feng, S.; Jiang, L.; Shi, Y.; Shen, H.; Shi, X.; Jin, D.; Zeng, Y.; Wang, Z. Uric acid levels and all-cause mortality in peritoneal dialysis patients. Kidney Blood Press. Res. 2013, 37, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Xia, X.; He, F.; Wu, X.; Peng, F.; Huang, F.; Yu, X. Relationship between serum uric acid and all-cause and cardiovascular mortality in patients treated with peritoneal dialysis. Am. J. Kidney Dis. 2014, 64, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Dong, J.; Han, Q.F.; Zhu, T.Y.; Ren, Y.P.; Chen, J.H.; Zhao, H.P.; Chen, M.H.; Xu, R.; Wang, Y.; Hao, C.M.; et al. The associations of uric acid, cardiovascular and all-cause mortality in peritoneal dialysis patients. PLoS ONE 2014, 9, e82342. [Google Scholar] [CrossRef] [PubMed]
- Xia, X.; Zhao, C.; Peng, F.F.; Luo, Q.M.; Zhou, Q.; Lin, Z.C.; Yu, X.Q.; Huang, F.X. Serum uric acid predicts cardiovascular mortality in male peritoneal dialysis patients with diabetes. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Fang, J.; Alderman, M.H. Serum uric acid and cardiovascular mortality: The NHANES I epidemiologic follow-up study, 1971–1992. National Health and Nutrition Examination Survey. JAMA 2000, 283, 2404–2410. [Google Scholar] [CrossRef] [PubMed]
- Takiue, Y.; Hosoyamada, M.; Kimura, M.; Saito, H. The effect of female hormones upon urate transport systems in the mouse kidney. Nucleosides Nucleotides Nucleic Acids 2011, 30, 113–119. [Google Scholar] [CrossRef] [PubMed]
- Hosoyamada, M.; Takiue, Y.; Shibasaki, T.; Saito, H. The effect of testosterone upon the urate reabsorptive transport system in mouse kidney. Nucleosides Nucleotides Nucleic Acids 2010, 29, 574–579. [Google Scholar] [CrossRef] [PubMed]
- Heo, S.H.; Lee, S.H. High levels of serum uric acid are associated with silent brain infarction. J. Neurol. Sci. 2010, 297, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Cipolli, J.A.; Ferreira-Sae, M.C.; Martins, R.P.; Pio-Magalhães, J.A.; Bellinazzi, V.R.; Matos-Souza, J.R.; Junior, W.N. Relationship between serum uric acid and internal carotid resistive index in hypertensive women: A cross-sectional study. BMC Cardiovasc. Disord. 2012, 12, 52. [Google Scholar] [CrossRef] [PubMed]
- Fang, J.I.; Wu, J.S.; Yang, Y.C.; Wang, R.H.; Lu, F.H.; Chang, C.J. High uric acid level associated with increased arterial stiffness in apparently healthy women. Atherosclerosis 2014, 236, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.J.; Feig, D.I.; Herrera-Acosta, J.; Kang, D.H. Resurrection of uric acid as a causal risk factor in essential hypertension. Hypertension 2005, 45, 18–20. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, T.; Hu, H.; Zharikov, S.; Tuttle, K.R.; Short, R.A.; Glushakova, O.; Ouyang, X.; Feig, D.I.; Block, E.R.; Herrera-Acosta, J.; et al. A causal role for uric acid in fructose-induced metabolic syndrome. Am. J. Physiol. Ren. Physiol. 2006, 290, F625–F631. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.J.; Kang, D.H.; Feig, D.; Kivlighn, S.; Kanellis, J.; Watanabe, S.; Tuttle, K.R.; Rodriguez-Iturbe, B.; Herrera-Acosta, J.; Mazzali, M. Is there a pathogenetic role for uric acid in hypertension and cardiovascular and renal disease? Hypertension 2003, 41, 1183–1190. [Google Scholar] [CrossRef] [PubMed]
- Milionis, H.J.; Kalantzi, K.J.; Goudevenos, J.A.; Seferiadis, K.; Mikhailidis, D.P.; Elisaf, M.S. Serum uric acid levels and risk for acute ischaemic non-embolic stroke in elderly subjects. J. Intern. Med. 2005, 258, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Mazzali, M.; Hughes, J.; Kim, Y.G.; Jefferson, J.A.; Kang, D.H.; Gordon, K.L.; Lan, H.Y.; Kivlighn, S.; Johnson, R.J. Elevated uric acid increases blood pressure in the rat by a novel crystal-independent mechanism. Hypertension 2001, 38, 1101–1106. [Google Scholar] [CrossRef] [PubMed]
- Ginsberg, M.H.; Kozin, F.; O’Malley, M.; McCarty, D.J. Release of platelet constituents by monosodium urate crystals. J. Clin. Investig. 1997, 60, 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Park, J.T.; Kim, D.K.; Chang, T.I.; Kim, H.W.; Chang, J.H.; Park, S.Y.; Kim, E.; Kang, S.W.; Han, D.S.; Yoo, T.H. Uric acid is associated with the rate of residual renal function decline in peritoneal dialysis patients. Nephrol. Dial. Transplant. 2009, 24, 3520–3525. [Google Scholar] [CrossRef] [PubMed]
- Hsu, S.P.; Pai, M.E.; Peng, Y.S.; Chiang, C.K.; Ho, T.I.; Hung, K.Y. Serum uric acid levels show a ‘J-shaped’ association with all-cause mortality in haemodialysis patients. Nephrol. Dial. Transplant. 2004, 19, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Carrero, J.J.; Qureshi, A.R.; Axelsson, J.; Avesani, C.M.; Suliman, M.E.; Kato, S.; Bárány, P.; Snaedal-Jonsdottir, S.; Alvestrand, A.; Heimbürger, O.; et al. Comparison of nutritional and inflammatory markers in dialysis patients with reduced appetite. Am. J. Clin. Nutr. 2007, 8, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Stenvinkel, P. Inflammation in end-stage renal disease: The hidden enemy. Nephrology (Carlton) 2006, 11, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Nieto, F.J.; Iribarren, C.; Gross, M.D.; Comstock, G.W.; Cutler, R.G. Uric acid and serum antioxidant capacity: A reaction to atherosclerosis? Atherosclerosis 2000, 148, 131–139. [Google Scholar] [CrossRef]
- Suzuki, T. Nitrosation of uric acid induced by nitric oxide under aerobic conditions. Nitric Oxide 2007, 16, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Urano, W.; Yamanaka, H.; Tsutani, H.; Nakajima, H.; Matsuda, Y.; Taniguchi, A.; Hara, M.; Kamatani, N. The inflammatory process in the mechanism of decreased serum uric acid concentrations during acute gouty arthritis. J. Rheumatol. 2002, 29, 1950–1953. [Google Scholar] [PubMed]
- Wu, V.C.; Huang, J.W.; Hsueh, P.R.; Yang, Y.F.; Tsai, H.B.; Kan, W.C.; Chang, H.W.; Wu, K.D. SARS Research Group of National Taiwan University College of Medicine, National Taiwan University Hospital. Renal hypouricemia is an ominous sign in patients with severe acute respiratory syndrome. Am. J. Kidney Dis. 2005, 45, 88–95. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Tertile 1 (n = 170) | Tertile 2 (n = 163) | Tertile 3 (n = 159) | p-Value | |
|---|---|---|---|---|
| Sex, men | 80 (47.1%) | 82 (50.3%) | 74 (46.5%) | 0.76 |
| Age (years) | 58 ± 14.8 | 52.9 ± 14 | 49.4 ± 15.8 | <0.001 |
| Body mass index (kg/m2) | 22.7 (20.6–25.2) | 23.8 (21.1–26.7) | 23.2 (20.7–26.6) | 0.09 |
| Smoker | 0.45 | |||
| never | 134 (78.8%) | 137 (84.1%) | 131 (82.4%) | |
| current | 5 (2.9%) | 5 (3.1%) | 2 (1.3%) | |
| ever | 31 (18.2%) | 21 (12.9%) | 26 (16.4%) | |
| Status before PD | 0.17 | |||
| pre-dialysis | 132 (77.7%) | 142 (87.1%) | 129 (81.1%) | |
| hemodialysis | 38 (22.4%) | 19 (11.7%) | 30 (18.9%) | |
| Failed transplant | 0 (0%) | 2 (1.2%) | 0 (0%) | |
| Medications use | ||||
| ACE inhibitor/ARB | 106 (62.4%) | 110 (67.5%) | 97 (61%) | 0.44 |
| Allopurinol | 42 (24.7%) | 46 (28.2%) | 38 (23.9%) | 0.64 |
| Furosemide | 78 (45.9%) | 75 (46%) | 78 (49.1%) | 0.81 |
| statin | 34 (20%) | 34 (20.9%) | 35 (22%) | 0.91 |
| Erythropoiesis stimulating agents | 155 (91.2%) | 157 (96.3%) | 153 (96.2%) | 0.06 |
| vitamin D | 159 (93.5%) | 153 (93.9%) | 148 (93.1%) | 0.96 |
| Calcium channel blocker | 117 (68.8%) | 116 (71.2%) | 113 (71.1%) | 0.87 |
| Laboratory data | ||||
| Uric acid (mg/dL) | 6 (5.2–6.4) | 7.3 (6.9–7.5) | 8.7 (8.2–9.6) | <0.001 |
| Serum albumin (g/dL) | 3.3 (2.9–3.7) | 3.4 (3–3.9) | 3.4 (3.1–3.9) | 0.01 |
| Hemoglobin (g/dL) | 8.79 (8–9.5) | 8.7 (7.8–9.4) | 8.6 (7.4–9.4) | 0.09 |
| BUN (mg/dL) | 76.5 (64–90) | 82 (68–96) | 92 (76–109) | <0.001 |
| Creatinine (mg/dL) | 8.8 (7.6–11) | 9.7 (8.1–11.9) | 10 (8.5–12.8) | <0.001 |
| Alkaline phosphatase (U/L) | 101 (73–150) | 98 (68–159) | 97 (64–161) | 0.68 |
| Calcium (mg/dL) | 8.3 (7.9–8.9) | 8.4 (8–8.9) | 8.3 (7.8–8.6) | 0.18 |
| Phosphorus (mg/dL) | 5 (4.2–5.7) | 5.3 (4.6–6.1) | 5.9 (5.2–6.7) | <0.001 |
| Cholesterol (mg/dL) | 176 (152–209) | 185 (154–219) | 185 (151–217) | 0.41 |
| Triglyceride (mg/dL) | 110.5 (83–151) | 122 (96–173) | 127 (91–182) | 0.005 |
| WBC count (×103/μL) | 7.1 (5.7–8.5) | 7.2 (5.9–8.8) | 6.9 (5.6–8.9) | 0.75 |
| Ferritin (ng/mL) | 302.7 (158.5–550) | 260.2 (127.6–421.7) | 259 (136–550.6) | 0.18 |
| Transferrin saturation (%) | 26.5 (17.62–35.39) | 22.61 (16.72–31.31) | 24.24 (17.12–34.59) | 0.08 |
| GPT (U/L) | 16 (12–24) | 15 (12–22) | 16 (12–23) | 0.92 |
| Intact PTH (pg/mL) | 312.17 (184–445.5) | 350.8 (200.67–544) | 375.8 (196–641) | 0.06 |
| Comorbidities | ||||
| Hypertension | 146 (85.9%) | 139 (85.3%) | 134 (84.3%) | 0.92 |
| Diabetes mellitus | 66 (38.8%) | 64 (39.3%) | 49 (30.8%) | 0.21 |
| Cardiovascular disease | 69 (40.6%) | 64 (39.3%) | 53 (33.3%) | 0.36 |
| Charlson index | 3 (2–4) | 3 (2–4) | 2 (2–4) | 0.12 |
| Peritoneal dialysis-related data | ||||
| D/P Creatinine at 4 h | 0.7 (0.62–0.76) | 0.67 (0.6–0.77) | 0.65 (0.59–0.73) | 0.01 |
| Ultrafiltration (L/day) | 0.22 (−0.2–0.6) | 0.35 (−0.1–0.75) | 0.5 (0.1–0.98) | <0.001 |
| 24 h urine volume (L) | 0.93 (0.53–1.35) | 0.88 (0.5–1.3) | 0.85 (0.46–1.22) | 0.35 |
| Total Weekly Kt/V | 2.14 (1.79–2.37) | 2.03 (1.75–2.32) | 2.01 (1.77–2.27) | 0.31 |
| nPNA (g/kg/day) | 1.01 (0.82–1.2) | 1.02 (0.8–1.22) | 1.05 (0.89–1.26) | 0.13 |
| Residual renal function (mL/min/1.73 m2) | 2.96 (2.13–3.68) | 2.96 (2.13–3.82) | 2.94 (1.96–3.74) | 0.82 |
| Tertiles of Uric Acid | All-Cause Mortality | Cardiovascular Mortality | Infection-Related Mortality | ||||
|---|---|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | ||
| Unadjusted | Tertile 2 | 0.71 (0.48–1.04) | 0.08 | 0.74 (0.45–1.23) | 0.25 | 0.48 (0.23–0.98) | 0.04 |
| Tertile 3 | 0.32 (0.19–0.52) | <0.0001 | 0.33 (0.17–0.63) | 0.001 | 0.31 (0.13–0.72) | 0.007 | |
| Model 1 | Tertile 2 | 1.03 (0.69–1.54) | 0.87 | 0.99 (0.59–1.67) | 0.97 | 0.81 (0.37–1.66) | 0.58 |
| Tertile 3 | 0.49 (0.29–0.82) | 0.006 | 0.44 (0.23–0.86) | 0.02 | 0.52 (0.21–1.16) | 0.14 | |
| Model 2 | Tertile 2 | 1.02 (0.68–1.51) | 0.94 | 1.03 (0.61–1.72) | 0.92 | 0.83 (0.38–1.71) | 0.62 |
| Tertile 3 | 0.46 (0.27–0.76) | 0.003 | 0.48 (0.25–0.93) | 0.03 | 0.57 (0.23–1.29) | 0.21 | |
| Model 3 | Tertile 2 | 0.88 (0.59–1.32) | 0.53 | 0.91 (0.54–1.53) | 0.72 | 0.81 (0.37–1.69) | 0.59 |
| Tertile 3 | 0.4 (0.24–0.67) | 0.001 | 0.39 (0.2–0.77) | 0.006 | 0.53 (0.21–1.19) | 0.15 | |
| Model 4 | Tertile 2 | 0.83 (0.55–1.24) | 0.36 | 1.01 (0.6–1.69) | 0.97 | 0.83 (0.38–1.73) | 0.63 |
| Tertile 3 | 0.35 (0.21–0.59) | <0.0001 | 0.38 (0.19–0.74) | 0.005 | 0.43 (0.17–0.97) | 0.06 | |
| Model 5 | Tertile 2 | 1.06 (0.7–1.58) | 0.8 | 1.04 (0.62–1.77) | 0.87 | 0.9 (0.41–1.94) | 0.8 |
| Tertile 3 | 0.4 (0.24–0.68) | 0.001 | 0.4 (0.2–0.81) | 0.01 | 0.47 (0.19–1.09) | 0.1 | |
| Tertiles of Uric Acid | All-Cause Mortality | Cardiovascular Mortality | Infection-Related-Mortality | ||||
|---|---|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | HR (95% CI) | p-Value | ||
| Unadjusted | Tertile 2 | 0.74 (0.50–1.11) | 0.15 | 0.80 (0.47–1.35) | 0.41 | 0.53 (0.26–1.08) | 0.08 |
| Tertile 3 | 0.35 (0.21–0.56) | <0.001 | 0.39 (0.21–0.72) | 0.003 | 0.21 (0.08–0.55) | 0.002 | |
| Model 1 | Tertile 2 | 0.97 (0.64–1.45) | 0.87 | 0.99 (0.58–1.69) | 0.96 | 0.88 (0.42–1.83) | 0.73 |
| Tertile 3 | 0.52 (0.32–0.85) | 0.01 | 0.51 (0.27–0.97) | 0.04 | 0.40 (0.15–1.05) | 0.06 | |
| Model 2 | Tertile 2 | 0.95 (0.64–1.43) | 0.81 | 0.86 (0.49–1.50) | 0.60 | 0.90 (0.43–1.88) | 0.78 |
| Tertile 3 | 0.51 (0.31–0.84) | 0.007 | 0.46 (0.24–0.88) | 0.02 | 0.46 (0.17–1.24) | 0.12 | |
| Model 3 | Tertile 2 | 0.82 (0.54–1.24) | 0.34 | 0.89 (0.52–1.52) | 0.67 | 0.79 (0.37–1.65) | 0.53 |
| Tertile 3 | 0.43 (0.26–0.69) | 0.001 | 0.42 (0.22–0.78) | 0.007 | 0.39 (0.15–1.05) | 0.06 | |
| Model 4 | Tertile 2 | 0.86 (0.58–1.29) | 0.47 | 0.98 (0.58–1.68) | 0.96 | 0.59 (0.28–1.26) | 0.17 |
| Tertile 3 | 0.36 (0.22–0.60) | <0.001 | 0.396 (0.21–0.75) | 0.004 | 0.29 (0.11–0.78) | 0.01 | |
| Model 5 | Tertile 2 | 0.79 (0.52–1.21) | 0.28 | 0.98 (0.57–1.69) | 0.96 | 0.58 (0.27–1.23) | 0.15 |
| Tertile 3 | 0.43 (0.26–0.72) | 0.001 | 0.45 (0.24–0.86) | 0.01 | 0.24 (0.09–0.69) | 0.008 | |
| All-Cause Mortality | Cardiovascular Mortality | Infection-Associated Mortality | |||||||
|---|---|---|---|---|---|---|---|---|---|
| HR (95% CI) | p-Value | p for Interaction | HR (95% CI) | p-Value | p for Interaction | HR (95% CI) | p-Value | p for Interaction | |
| mortality risk for every 1-mg/dL increase in serum uric acid level | |||||||||
| Total cohort | |||||||||
| All patients (n = 492) | 0.79 (0.69–0.9) | 0.001 | 0.25 | 0.8 (0.68–0.96) | 0.01 | 0.44 | 0.67 (0.53–0.84) | 0.001 | 0.37 |
| Men | 0.84 (0.69–1.02) | 0.07 | 0.79 (0.61–1.01) | 0.06 | 0.79 (0.48–1.22) | 0.32 | |||
| Women | 0.57 (0.44–0.73) | <0.0001 | 0.6 (0.41–0.87) | 0.006 | 0.41 (0.26–0.59) | <0.0001 | |||
| Excluding those taking allopurinol | |||||||||
| All patients (n = 366) | 0.78 (0.65–0.94) | 0.009 | 0.79 | 0.7 (0.52–0.93) | 0.01 | 0.94 | 0.66 (0.5–0.85) | 0.002 | 0.49 |
| Men | 0.7 (0.44–1.1) | 0.12 | 0.63 (0.4–1.01) | 0.05 | 0.63 (0.38–1.04) | 0.07 | |||
| Women | 0.47 (0.31–0.7) | <0.0001 | 0.54 (0.34–0.79) | 0.004 | 0.41 (0.24–0.63) | <0.0001 | |||
| Hyperuricemia vs. non-hyperuricemia | |||||||||
| All patients | 0.55 (0.37–0.82) | 0.003 | 0.18 | 0.52 (0.31–0.87) | 0.01 | 0.52 | 0.46 (0.26–0.59) | 0.02 | 0.09 |
| Men (>7 mg/dL) | 0.63 (0.37–1.05) | 0.08 | 0.53 (0.26–1.08) | 0.08 | 0.64 (0.38–1.08) | 0.1 | |||
| Women (>6 mg/dL) | 0.29 (0.15–0.58) | 0.001 | 0.28 (0.11–0.7) | 0.007 | 0.48 (0.26–0.92) | 0.03 | |||
| Unstandardized Coefficients | Standardized Coefficients Beta | p-Value | ||
|---|---|---|---|---|
| B | Std. Error | |||
| Sex (male vs. female) | 0.280 | 0.137 | 0.088 | 0.04 |
| Age | −0.013 | 0.005 | −0.121 | 0.01 |
| Albumin | 0.463 | 0.132 | 0.159 | 0.001 |
| Alkaline phosphate | −0.002 | 0.001 | −0.084 | 0.05 |
| BUN | 0.008 | 0.003 | 0.119 | 0.02 |
| Intact PTH | 0.000 | 0.000 | 0.097 | 0.04 |
| Phosphorus | 0.225 | 0.066 | 0.186 | 0.001 |
| Triglyceride | 0.003 | 0.001 | 0.183 | <0.001 |
| WBC counts | 0.053 | 0.028 | 0.080 | 0.06 |
| Cardiovascular disease | 0.347 | 0.146 | 0.106 | 0.02 |
| Ultrafiltration | 0.155 | 0.090 | 0.073 | 0.09 |
| 24-h urine output | −0.575 | 0.166 | −0.216 | 0.001 |
| Residual renal function | 0.21 | 0.058 | 0.216 | <0.001 |
| UA Tertiles | All-Cause Mortality | Cardiovascular Mortality | Infection-Mortality | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| aHR (95% CI) | p-Value | Pinteraction | aHR (95% CI) | p-Value | Pinteraction | aHR (95% CI) | p-Value | Pinteraction | ||
| BMI ≥ 23.1 | Tertile 2 | 0.93 (0.52–1.68) | 0.82 | 0.39 | 0.94 (0.49–1.81) | 0.85 | 0.34 | 1.11 (0.16–7.9) | 0.91 | 0.43 |
| Tertile 3 | 0.38 (0.17–0.86) | 0.02 | 0.41 | 0.24 (0.09–0.66) | 0.006 | 0.22 | 0.51 (0.07–3.54) | 0.49 | 0.38 | |
| BMI < 23.1 | Tertile 2 | 1.16 (0.64–2.09) | 0.63 | 1.17 (0.48–2.85) | 0.72 | 1.12 (0.38–3.33) | 0.83 | |||
| Tertile 3 | 0.33 (0.15–0.71) | 0.005 | 0.39 (0.13–1.11) | 0.08 | 0.86 (0.23–3.21) | 0.83 | ||||
| Albumin ≥ 3.4 | Tertile 2 | 1.32 (0.65–2.69) | 0.44 | 0.81 | 1.08 (0.42–2.75) | 0.87 | 0.81 | 2.02 (0.46–8.78) | 0.34 | 0.10 |
| Tertile 3 | 0.38 (0.15–0.92) | 0.03 | 0.14 | 0.48 (0.16–1.43) | 0.18 | 0.64 | 0.81 (0.10–6.38) | 0.84 | 0.36 | |
| Albumin < 3.4 | Tertile 2 | 0.80 (0.49–1.33) | 0.39 | 0.94 (0.48–1.81) | 0.85 | 0.48 (0.17–1.37) | 0.17 | |||
| Tertile 3 | 0.47 (0.25–0.90) | 0.02 | 0.54 (0.23–1.27) | 0.15 | 0.39 (0.13–1.19) | 0.09 | ||||
| Cholesterol ≥ 181 | Tertile 2 | 1.17 (0.64–2.16) | 0.61 | 0.43 | 1.09 (0.52–2.32) | 0.81 | 0.48 | 1.05 (0.17–6.38) | 0.96 | 0.28 |
| Tertile 3 | 0.59 (0.26–1.34) | 0.21 | 0.85 | 0.47 (0.16–1.35) | 0.16 | 0.41 | 0.87 (0.16–4.76) | 0.87 | 0.75 | |
| Cholesterol < 181 | Tertile 2 | 0.68 (0.36–1.28) | 0.22 | 0.55 (0.22–1.37) | 0.20 | 0.88 (0.35–2.22) | 0.79 | |||
| Tertile 3 | 0.41 (0.20–0.84) | 0.01 | 0.54 (0.21–1.36) | 0.19 | 0.51 (0.16–1.56) | 0.24 | ||||
| nPNA ≥ 1.03 | Tertile 2 | 1.02 (0.47–2.24) | 0.95 | 0.09 | 0.42 (0.15–1.16) | 0.09 | 0.47 | 0.86 (0.16–4.64) | 0.86 | 0.28 |
| Tertile 3 | 0.39 (0.15–1.01) | 0.05 | 0.96 | 0.25 (0.07–0.88) | 0.03 | 0.95 | 0.93 (0.21–4.17) | 0.93 | 0.59 | |
| nPNA < 1.03 | Tertile 2 | 1.16 (0.71–1.92) | 0.55 | 0.87 (0.35–2.19) | 0.77 | 0.78 (0.3–2.03) | 0.61 | |||
| Tertile 3 | 0.56 (0.29–1.08) | 0.08 | 0.43 (0.13–1.44) | 0.17 | 0.43 (0.14–1.32) | 0.14 | ||||
| Phosphorus ≥ 5.4 | Tertile 2 | 0.96 (0.41–2.24) | 0.92 | 0.21 | 1.03 (0.28–3.78) | 0.96 | 0.99 | 1.05 (0.19–5.71) | 0.95 | 0.04 |
| Tertile 3 | 0.26 (0.09–0.69) | 0.007 | 0.23 | 0.50 (0.14–1.76) | 0.28 | 0.63 | 0.59 (0.08–4.32) | 0.60 | 0.51 | |
| Phosphorus < 5.4 | Tertile 2 | 0.84 (0.51–1.36) | 0.47 | 0.86 (0.44–1.67) | 0.65 | 0.45 (0.17–1.17) | 0.10 | |||
| Tertile 3 | 0.54 (0.28–1.01) | 0.05 | 0.36 (0.14–0.94) | 0.03 | 0.41 (0.14–1.15) | 0.09 | ||||
| Creatinine ≥ 9.6 | Tertile 2 | 0.89 (0.44–1.83) | 0.76 | 0.39 | 0.87 (0.28–2.77) | 0.82 | 0.97 | 0.51 (0.09–2.58) | 0.41 | 0.11 |
| Tertile 3 | 0.41 (0.15–1.09) | 0.07 | 0.99 | 0.21 (0.04–1.16) | 0.07 | 0.96 | 0.51 (0.08–3.18) | 0.47 | 0.56 | |
| Creatinine < 9.6 | Tertile 2 | 0.82 (0.49–1.36) | 0.45 | 0.96 (0.46–2.01) | 0.91 | 0.51 (0.21–1.28) | 0.15 | |||
| Tertile 3 | 0.39 (0.21–0.75) | 0.004 | 0.39 (0.15–1.04) | 0.06 | 0.56 (0.17–1.81) | 0.33 | ||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, K.-J.; Kor, C.-T.; Hsieh, Y.-P. An Inverse Relationship between Hyperuricemia and Mortality in Patients Undergoing Continuous Ambulatory Peritoneal Dialysis. J. Clin. Med. 2018, 7, 416. https://doi.org/10.3390/jcm7110416
Lai K-J, Kor C-T, Hsieh Y-P. An Inverse Relationship between Hyperuricemia and Mortality in Patients Undergoing Continuous Ambulatory Peritoneal Dialysis. Journal of Clinical Medicine. 2018; 7(11):416. https://doi.org/10.3390/jcm7110416
Chicago/Turabian StyleLai, Kuan-Ju, Chew-Teng Kor, and Yao-Peng Hsieh. 2018. "An Inverse Relationship between Hyperuricemia and Mortality in Patients Undergoing Continuous Ambulatory Peritoneal Dialysis" Journal of Clinical Medicine 7, no. 11: 416. https://doi.org/10.3390/jcm7110416
APA StyleLai, K.-J., Kor, C.-T., & Hsieh, Y.-P. (2018). An Inverse Relationship between Hyperuricemia and Mortality in Patients Undergoing Continuous Ambulatory Peritoneal Dialysis. Journal of Clinical Medicine, 7(11), 416. https://doi.org/10.3390/jcm7110416