Mortality Risks among Various Primary Renal Diseases in Children and Adolescents on Chronic Dialysis

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Experimental Section
2.1. Data Source
2.2. Study Population
2.3. Statistical Analysis
3. Results
3.1. Patients Characteristics
3.2. Overall Mortality in Patients on Dialysis
3.3. Mortality Risk in Patients on Dialysis
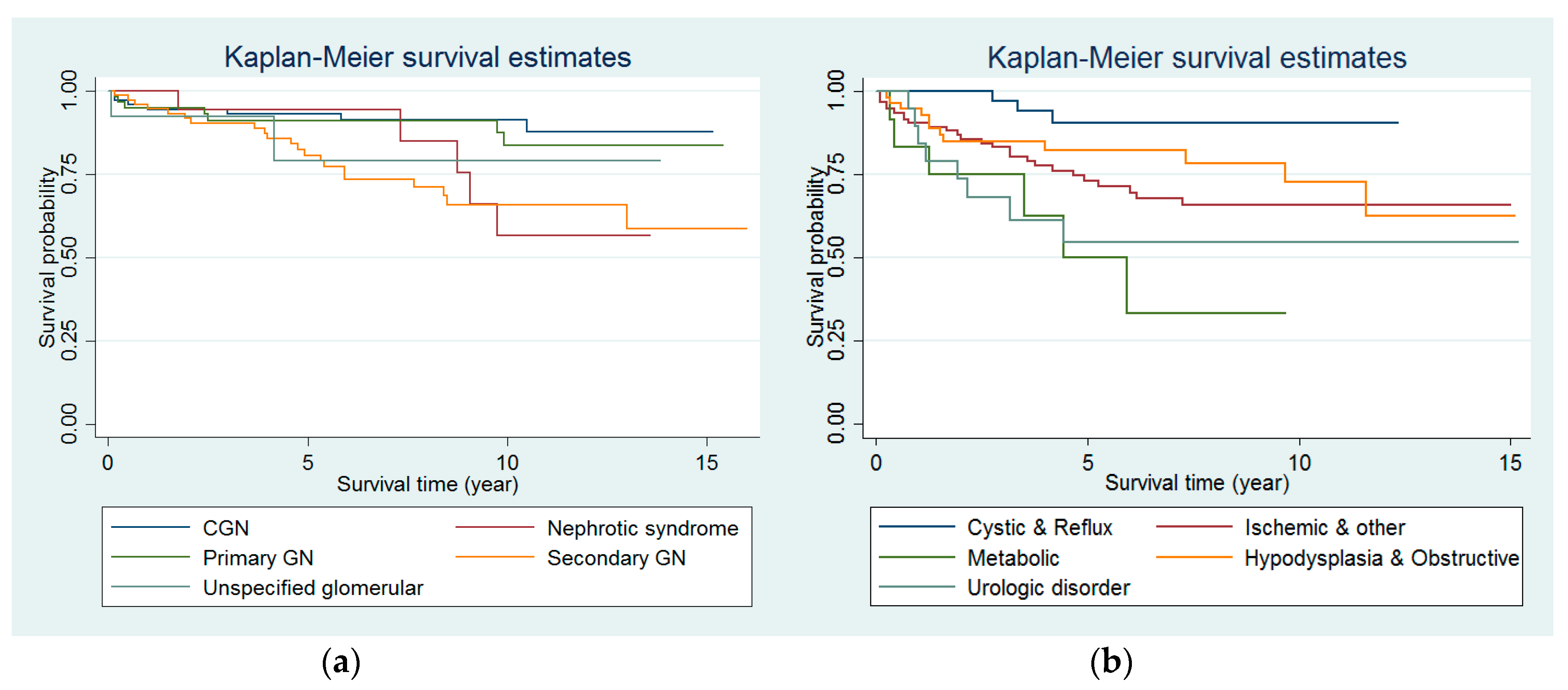
3.4. Mortality Rates and Differential Mortality Risks among Patients with Primary Renal Diseases
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Harambat, J.; van Stralen, K.J.; Kim, J.J.; Tizard, E.J. Epidemiology of chronic kidney disease in children. Pediatr. Nephrol. 2012, 27, 363–373. [Google Scholar] [CrossRef] [PubMed]
- Tjaden, L.A.; Vogelzang, J.; Jager, K.J.; van Stralen, K.J.; Maurice-Stam, H.; Grootenhuis, M.A.; Groothoff, J.W. Long-term quality of life and social outcome of childhood end-stage renal disease. J. Pediatr. 2014, 165, 336–342. [Google Scholar] [CrossRef] [PubMed]
- U.S. Renal Data System. USRDS 2006 Annual Data Report: Atlas of End Stage Renal Disease in the United States; Bethesda Softworks: Bethesda, MD, USA, 2006.
- Chesnaye, N.; Bonthuis, M.; Schaefer, F.; Groothoff, J.W.; Verrina, E.; Heaf, J.G.; Jankauskiene, A.; Lukosiene, V.; Molchanova, E.A.; Mota, C.; et al. Demographics of paediatric renal replacement therapy in Europe: A report of the ESPN/ERA-EDTA registry. Pediatr. Nephrol. 2014, 29, 2403–2410. [Google Scholar] [CrossRef] [PubMed]
- Chesnaye, N.C.; Schaefer, F.; Groothoff, J.W.; Bonthuis, M.; Reusz, G.; Heaf, J.G.; Lewis, M.; Maurer, E.; Paripovic, D.; Zagozdzon, I.; et al. Mortality risk in European children with end-stage renal disease on dialysis. Kidney Int. 2016, 89, 1355–1362. [Google Scholar] [CrossRef] [PubMed]
- Mitsnefes, M.M.; Laskin, B.L.; Dahhou, M.; Zhang, X.; Foster, B.J. Mortality risk among children initially treated with dialysis for end-stage kidney disease, 1990–2010. JAMA 2013, 309, 1921–1929. [Google Scholar] [CrossRef] [PubMed]
- McDonald, S.P.; Craig, J.C. Long-term survival of children with end-stage renal disease. N. Engl. J. Med. 2004, 350, 2654–2662. [Google Scholar] [CrossRef] [PubMed]
- Shroff, R.; Ledermann, S. Long-term outcome of chronic dialysis in children. Pediatr. Nephrol. 2009, 24, 463–474. [Google Scholar] [CrossRef] [PubMed]
- National Health Insurance Administration. The National Health Insurance Statistics. 2014. Available online: https://www.nhi.gov.tw/english/Content_List.aspx?n=8162ED7256773F45&topn=616B97F8DF2C3614 (accessed on 4 November 2018).
- Cheng, C.L.; Chien, H.C.; Lee, C.H.; Lin, S.J.; Yang, Y.H. Validity of in-hospital mortality data among patients with acute myocardial infarction or stroke in National Health Insurance Research Database in Taiwan. Int. J. Cardiol. 2015, 201, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.P.; Liang, F.W.; Huang, Y.L.; Chen, L.H.; Lu, T.H. Maternal mortality in Taiwan: A nationwide data linkage study. PLoS ONE 2015, 10. [Google Scholar] [CrossRef] [PubMed]
- Flynn, J.T.; Mitsnefes, M.; Pierce, C.; Cole, S.R.; Parekh, R.S.; Furth, S.L.; Warady, B.A. Blood pressure in children with chronic kidney disease: A report from the Chronic Kidney Disease in Children study. Hypertension 2008, 52, 631–637. [Google Scholar] [CrossRef] [PubMed]
- European Renal Association-European Dialysis and Transplant Association. Registry: ERA-EDTA Registry Annual Report 2011; Academic Medical Center, Department of Medical Informatic: Amsterdam, The Netherlands, 2011. [Google Scholar]
- Hattori, M.; Sako, M.; Kaneko, T.; Ashida, A.; Matsunaga, A.; Igarashi, T.; Itami, N.; Ohta, T.; Gotoh, Y.; Satomura, K.; et al. End-stage renal disease in Japanese children: A nationwide survey during 2006–2011. Clin. Exp. Nephrol. 2015, 19, 933–938. [Google Scholar] [CrossRef] [PubMed]
- Chesnaye, N.C.; Schaefer, F.; Bonthuis, M.; Holman, R.; Baiko, S.; Baskın, E.; Bjerre, A.; Cloarec, S.; Cornelissen, E.A.M.; Espinosa, L.; et al. Mortality risk disparities in children receiving chronic renal replacement therapy for the treatment of end-stage renal disease across Europe: An ESPN-ERA/EDTA registry analysis. Lancet 2017, 389, 2128–2137. [Google Scholar] [CrossRef]
- Chou, H.H.; Lin, C.Y.; Chiou, Y.H.; Tain, Y.L.; Wang, Y.F.; Wang, H.H.; Chiou, Y.Y. Clinical characteristics and prevalence of complications of chronic kidney disease in children: The Taiwan Pediatric Renal Collaborative study. Pediatr. Nephrol. 2016, 31, 1113–1120. [Google Scholar] [CrossRef] [PubMed]
- Sule, S.; Fivush, B.; Neu, A.; Furth, S. Increased risk of death in pediatric and adult patients with ESRD secondary to lupus. Pediatr. Nephrol. 2011, 26, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Roman, M.J.; Shanker, B.A.; Davis, A.; Lockshin, M.D.; Sammaritano, L.; Simantov, R.; Crow, M.K.; Schwartz, J.E.; Paget, S.A.; Devereux, R.B.; et al. Prevalence and correlates of accelerated atherosclerosis in systemic lupus erythematosus. N. Engl. J. Med. 2003, 349, 2399–2406. [Google Scholar] [CrossRef] [PubMed]
- Petri, M.; Perez-Gutthann, S.; Spence, D.; Hochberg, M.C. Risk factors for coronary artery disease in patients with systemic lupus erythematosus. Am. J. Med. 1992, 93, 513–519. [Google Scholar] [CrossRef]
- Ilowite, N.T.; Samuel, P.; Ginzler, E.; Jacobson, M.S. Dyslipoproteinemia in pediatric systemic lupus erythematosus. Arthritis Rheum. 1998, 31, 859–863. [Google Scholar] [CrossRef]
- McKibben, M.J.; Seed, P.; Ross, S.S.; Borawski, K.M. Urinary tract infection and neurogenic bladder. Urol. Clin. N. Am. 2015, 42, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, L.; Bolen, J.; Valdez, R.; Joseph, D.; Baum, M.A.; Thibadeau, J. Characteristics and survival of patients with end stage renal disease and spina bifida in the United States renal data system. J. Urol. 2015, 193, 558–564. [Google Scholar] [CrossRef] [PubMed]
- Terryn, W.; Cochat, P.; Froissart, R.; Ortiz, A.; Pirson, Y.; Poppe, B.; Serra, A.; Van Biesen, W.; Vanholder, R.; Wanner, C. Fabry nephropathy: Indications for screening and guidance for diagnosis and treatment by the European Renal Best Practice. Nephrol. Dial. Transplant. 2013, 28, 505–517. [Google Scholar] [CrossRef] [PubMed]
- Harambat, J.; van Stralen, K.J.; Espinosa, L.; Groothoff, J.W.; Hulton, S.A.; Cerkauskiene, R.; Schaefer, F.; Verrina, E.; Jager, K.J.; Cochat, P. Characteristics and outcomes of children with primary oxalosis requiring renal replacement therapy. Clin. J. Am. Soc. Nephrol. 2012, 7, 458–465. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.C.; Chien, C.W.; Ho, J.D. Herpes zoster ophthalmicus and the risk of stroke: A population-based follow-up study. Neurology 2010, 74, 792–797. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Overall (n = 530) | Glomerular (n = 250) | Nonglomerular (n = 230) | Unknown (n = 50) | p-Value | |
|---|---|---|---|---|---|
| Age at dialysis initiation, median (IQR), years | 15.6 (12.2, 17.2) | 16.5 (13.0, 17.0) | 14.5 (9.1, 14.9) | 15.8 (13.6, 17.0) | <0.001 ** |
| Male sex, No. (%) | 305 (57.6%) | 136 (54.4%) | 144 (62.6%) | 25 (50.0%) | 0.101 |
| Initial dialysis modality, No. (%) | 0.378 | ||||
| Hemodialysis | 206 (38.9%) | 102 (40.8%) | 82 (35.7%) | 22 (44.0%) | |
| Peritoneal dialysis | 324 (61.1%) | 148 (59.2%) | 148 (64.4%) | 28 (56.0%) | |
| Survival status, Yes, No. (%) | 423 (79.8%) | 208 (83.2%) | 175 (76.1) | 40 (80.0%) | 0.152 |
| Survival time, median (IQR), years | 6.0 (3.6, 8.5) | 7.0 (4.8, 9.6) | 4.5 (2.3, 7.0) | 7.5 (5.0, 10.2) | <0.001 ** |
| Crude mortality rate at dialysis initiation, 2000–2014 | 31.5 per 1000 py | 23.4 per 1000 py | 43.7 per 1000 py | 28.9 per 1000 py | 0.024 ** |
| Dialysis modality at the end of observation | <0.001 ** | ||||
| Hemodialysis | 179 (33.8%) | 63 (25.2%) | 93 (40.4%) | 23 (46.0%) | |
| Peritoneal dialysis | 76 (14.3%) | 17 (6.8%) | 51 (22.2%) | 8 (16.0%) | |
| Kidney transplant | 275 (51.9%) | 170 (68.0%) | 86 (37.4%) | 19 (38.0%) | |
| Number of comorbidities, No. (%) | 0.050 | ||||
| None | 256 (48.3%) | 116 (46.4%) | 109 (47.4%) | 31 (62.0%) | |
| 1 | 229 (43.2%) | 119 (47.6%) | 95 (41.3%) | 15 (30.0%) | |
| ≥2 | 45 (8.5%) | 15 (6.0%) | 26 (11.3%) | 4 (8.0%) |
| No. of Patients | Patient-Years (py) | No. of Deaths | Deaths per 1000 py | Unadjusted HR (95% CI) | Adjusted HR * (95% CI) | |
|---|---|---|---|---|---|---|
| Age at dialysis initiation | ||||||
| 0–1 | 9 | 26.25 | 7 | 266.67 | 11.53 (5.16–25.76) | 11.45 (4.74–27.67) |
| 2–5 | 19 | 67.08 | 8 | 119.26 | 5.12 (2.40–10.93) | 5.43 (2.45–12.04) |
| 6–12 | 116 | 682.92 | 37 | 54.18 | 2.63 (1.70–4.07) | 2.57 (1.62–4.07) |
| 13–19 | 336 | 2283.58 | 45 | 19.71 | Reference | Reference |
| Sex | ||||||
| Male | 280 | 1808.67 | 52 | 28.75 | 0.81 (0.54–1.21) | 0.95 (0.62–1.44) |
| Female | 200 | 1251.17 | 45 | 35.97 | Reference | Reference |
| Primary cause of ESRD | ||||||
| Glomerular | 250 | 1701.92 | 42 | 24.68 | Reference | Reference |
| Nonglomerular | 230 | 1257.92 | 55 | 43.72 | 1.74 (1.17–2.61) | 1.26 (0.82–1.94) |
| Calendar year at dialysis initiation, per 1000 py | ||||||
| 2000–2004 | 177 | 1580.0 | 43 | 27.22 | Reference | Reference |
| 2005–2009 | 170 | 1021.67 | 36 | 35.24 | 1.12 (0.71–1.76) | 1.01 (0.63–1.60) |
| 2010–2014 | 133 | 458.17 | 18 | 39.29 | 1.08 (0.61–1.92) | 1.04 (0.58–1.86) |
| Initial dialysis modality, No. (%) | ||||||
| Hemodialysis | 184 | 1248.83 | 37 | 29.63 | 0.95 (0.63–1.43) | 1.38 (0.88–2.14) |
| Peritoneal dialysis | 296 | 1811.0 | 60 | 33.13 | Reference | Reference |
| No. of comorbidities | ||||||
| 0 | 225 | 1567.17 | 44 | 28.08 | Reference | Reference |
| 1 | 214 | 1280.08 | 41 | 32.03 | 1.09 (0.71–1.67) | 1.09 (0.70–1.67) |
| ≥2 | 41 | 212.58 | 12 | 56.45 | 1.88 (0.99–3.56) | 1.57 (0.81–3.03) |
| Primary Renal Disease | N (%) |
|---|---|
| Glomerular | 249 (47.0%) |
| Primary glomerulonephritis | 61 (11.5%) |
| Nephrotic syndrome | 24 (4.5%) |
| Chronic glomerulonephritis | 74 (14.0%) |
| Secondary glomerulonephritis | 72 (13.6%) |
| Lupus nephritis | 59 (11.1%) |
| HSP | 5 (0.9%) |
| HUS | 6 (1.1%) |
| Other secondary glomerulonephritis | 2 (0.4%) |
| Others | 18 (3.4%) |
| Nonglomerular | 230 (43.4%) |
| Renal hypodysplasia | 46 (8.7%) |
| Renal agenesis/dysplasia | 43 (8.1%) |
| Renal atrophy of unknown cause | 3 (0.6%) |
| Reflux nephropathy | 32 (6.0%) |
| Obstructive uropathy | 12 (2.3%) |
| Urologic disorder | 20 (3.8%) |
| Neurogenic bladder | 15 (2.8%) |
| Other urologic disorder | 5 (0.9%) |
| Cystic kidney disease | 13 (2.5%) |
| ARPKD | 4 (0.8%) |
| ADPKD | 1 (0.2%) |
| Other cystic kidney disease | 8 (1.5%) |
| Ischemic | 30 (5.7%) |
| Asphyxia/hypoxia | 15 2.8%) |
| Shock or severe sepsis | 10 (1.9%) |
| Other ischemic disorder | 5 (0.9%) |
| Metabolic | 12 (2.3%) |
| Urolithiasis or nephrocalcinosis | 5 (0.9%) |
| Disorders of amino acid transport | 3 (0.6%) |
| Fabry disease | 2 (0.4%) |
| Other enzymopathy | 2 (0.4%) |
| Others | 65 (12.3%) |
| Multiple anomalies | 18 (3.4%) |
| Wilms’ tumor | 5 (0.9%) |
| Hypertensive chronic kidney disease | 19 (3.6%) |
| Other nonglomerular disorder | 23 (4.6%) |
| Unknown | 51 (9.6%) |
| No. of Deaths | Patient-Years (py) | Death Rate per 1000 py | Unadjusted HR (95% CI) | Adjusted HR * (95% CI) | |
|---|---|---|---|---|---|
| Glomerular disease | |||||
| Primary GN | 7 | 454.5 | 15.40 | Reference | Reference |
| Nephrotic syndrome | 5 | 147.33 | 33.94 | 2.10 (0.67–6.62) | 1.65 (0.51–5.34) |
| CGN | 7 | 589.92 | 11.87 | 0.78 (0.27–2.23) | 0.81 (0.28–2.32) |
| Secondary GN | 21 | 530.92 | 39.55 | 2.53 (1.03–5.95) | 2.50 (1.03–6.08) |
| Other glomerular disease | 2 | 79.25 | 25.24 | 1.58 (0.32–7.50) | 1.37 (0.28–6.68) |
| Nonglomerular disease | |||||
| Renal hypodysplasia | 10 | 266.17 | 37.57 | 2.93 (0.87–6.03) | 1.32 (0.49–3.54) |
| Cystic kidney disease | 1 | 56.75 | 17.62 | 0.98 (0.12–7.98) | 0.39 (0.05–3.30) |
| Reflux nephropathy | 2 | 182.0 | 10.99 | 0.65 (0.13–3.15) | 0.47 (0.10–2.32) |
| Urologic disorder | 8 | 106.25 | 75.29 | 4.58 (1.66–12.65) | 4.77 (1.69–13.46) |
| Ischemic | 8 | 192.5 | 41.56 | 2.56 (0.93–7.07) | 1.64 (0.58–4.46) |
| Metabolic | 6 | 46.92 | 127.89 | 6.85 (2.92–20.47) | 5.57 (1.84–16.85) |
| Obstructive uropathy | 2 | 68.33 | 29.27 | 1.77 (0.37–8.54) | 1.50 (0.31–7.30) |
| Other nonglomerular disease | 18 | 339.0 | 53.10 | 3.17 (1.32–7.59) | 2.13 (0.87–5.21) |
| Unknown | 10 | 338.08 | 29.58 | 1.89 (0.72–4.97) | 1.80 (0.67–4.84) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chou, H.-H.; Chiou, Y.-Y.; Chiou, Y.-H.; Tain, Y.-L.; Wang, H.-H.; Yu, M.-C.; Hsu, C.-C.; Lin, C.-Y. Mortality Risks among Various Primary Renal Diseases in Children and Adolescents on Chronic Dialysis. J. Clin. Med. 2018, 7, 414. https://doi.org/10.3390/jcm7110414
Chou H-H, Chiou Y-Y, Chiou Y-H, Tain Y-L, Wang H-H, Yu M-C, Hsu C-C, Lin C-Y. Mortality Risks among Various Primary Renal Diseases in Children and Adolescents on Chronic Dialysis. Journal of Clinical Medicine. 2018; 7(11):414. https://doi.org/10.3390/jcm7110414
Chicago/Turabian StyleChou, Hsin-Hsu, Yuan-Yow Chiou, Yee-Hsuan Chiou, You-Lin Tain, Hsin-Hui Wang, Mei-Ching Yu, Chih-Cheng Hsu, and Ching-Yuang Lin. 2018. "Mortality Risks among Various Primary Renal Diseases in Children and Adolescents on Chronic Dialysis" Journal of Clinical Medicine 7, no. 11: 414. https://doi.org/10.3390/jcm7110414
APA StyleChou, H.-H., Chiou, Y.-Y., Chiou, Y.-H., Tain, Y.-L., Wang, H.-H., Yu, M.-C., Hsu, C.-C., & Lin, C.-Y. (2018). Mortality Risks among Various Primary Renal Diseases in Children and Adolescents on Chronic Dialysis. Journal of Clinical Medicine, 7(11), 414. https://doi.org/10.3390/jcm7110414