Is It Possible to Maintain High Compliance with the Enhanced Recovery after Surgery (ERAS) Protocol?—A Cohort Study of 400 Consecutive Colorectal Cancer Patients

 and
and
Abstract
1. Introduction
2. Materials and Methods
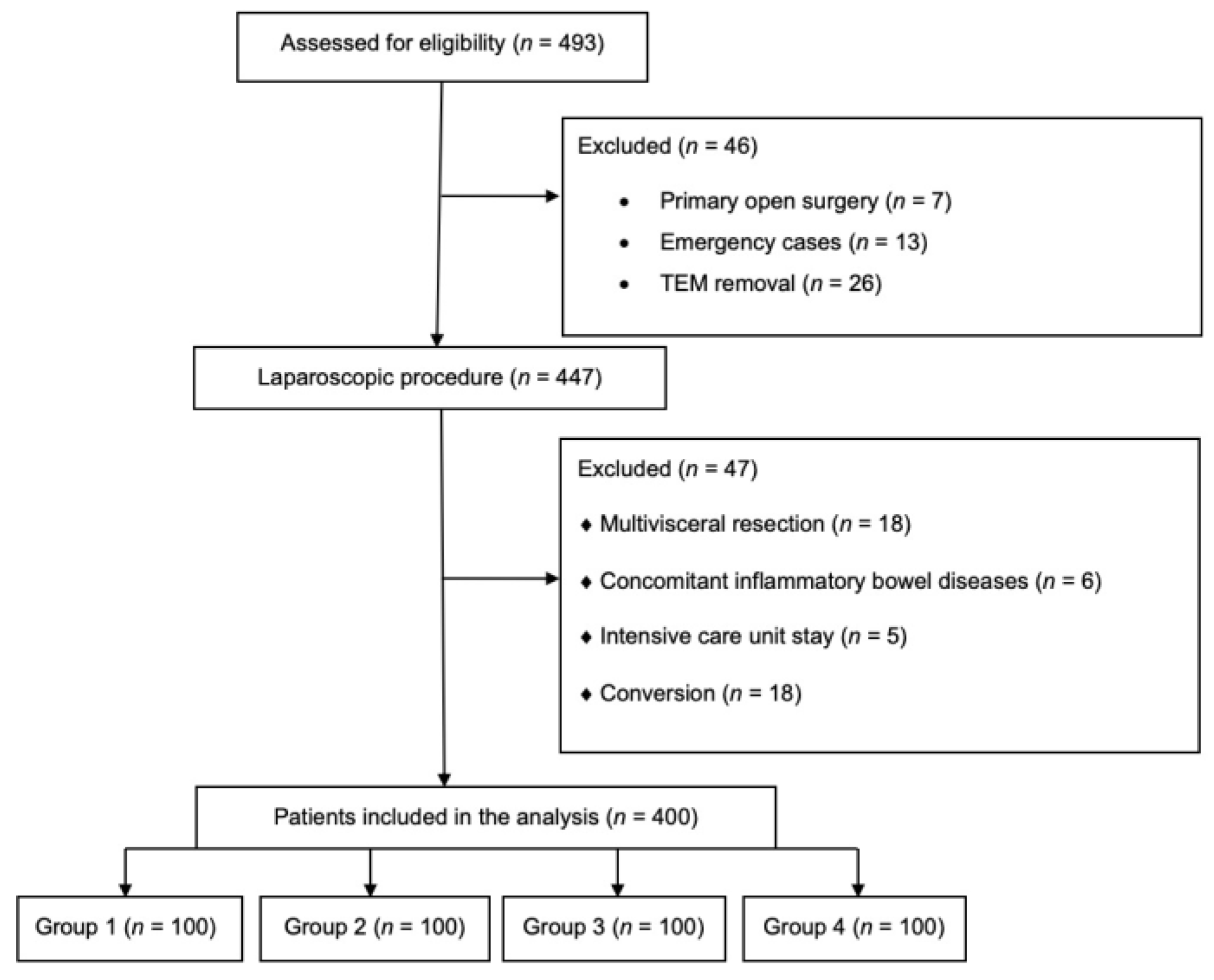
2.1. Inclusion and Exclusion Criteria
2.2. Statistical Analysis
2.3. Ethical Approval
3. Results
3.1. Demographic Parameters
3.2. Operative Parameters
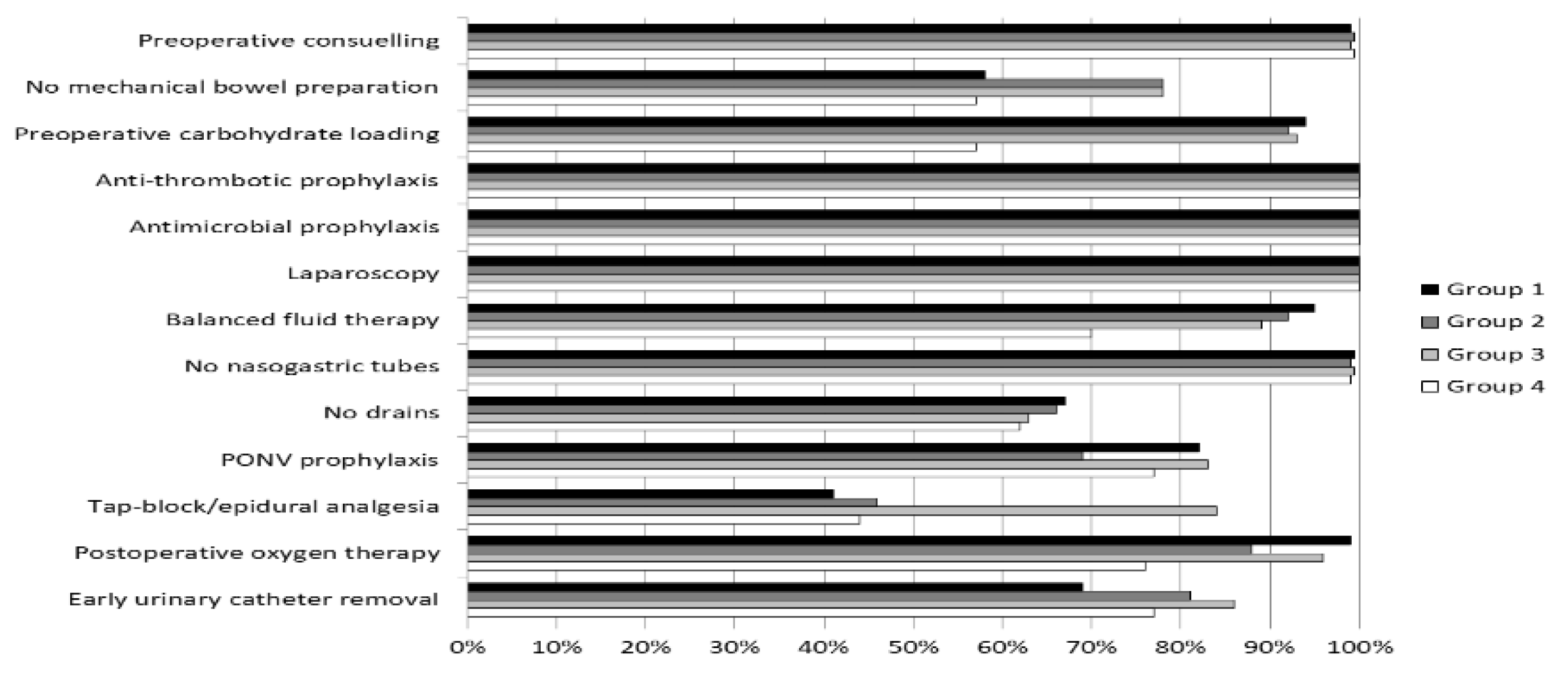
3.3. Compliance with ERAS Protocol
3.4. Short-Term Outcomes
3.5. Multivariate Analysis of Factors for Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Spanjersberg, W.R.; Van Sambeeck, J.D.; Bremers, A.; Rosman, C.; Van Laarhoven, C.J. Systematic review and meta-analysis for laparoscopic versus open colon surgery with or without an ERAS programme. Surg. Endosc. 2015, 29, 3443–3453. [Google Scholar] [CrossRef] [PubMed]
- Vlug, M.S.; Wind, J.; Hollmann, M.W.; Ubbink, D.T.; Cense, H.A.; Engel, A.F.; Gerhards, M.F.; Van Wagensveld, B.A.; Van der Zaag, E.S.; Van Geloven, A.A.; et al. Laparoscopy in combination with fast track multimodal management is the best perioperative strategy in patients undergoing colonic surgery: A randomized clinical trial (LAFA-study). Ann. Surg. 2011, 254, 868–875. [Google Scholar] [CrossRef] [PubMed]
- Greco, M.; Capretti, G.; Beretta, L.; Gemma, M.; Pecorelli, N.; Braga, M. Enhanced recovery program in colorectal surgery: A meta-analysis of randomized controlled trials. World J. Surg. 2014, 38, 1531–1541. [Google Scholar] [CrossRef] [PubMed]
- Tejedor, P.; Pastor, C.; Gonzalez-Ayora, S.; Ortega-Lopez, M.; Guadalajara, H.; Garcia-Olmo, D. Short-term outcomes and benefits of ERAS program in elderly patients undergoing colorectal surgery: A case-matched study compared to conventional care. Int. J. Colorectal Dis. 2018, 33, 1251–1258. [Google Scholar] [CrossRef] [PubMed]
- Marcotte, J.H.; Patel, K.; Desai, R.; Gaughan, J.P.; Rattigan, D.; Cahill, K.W.; Irons, R.F.; Dy, J.; Dobrowolski, M.; McElhenney, H.; et al. Acute kidney injury following implementation of an enhanced recovery after surgery (ERAS) protocol in colorectal surgery. Int. J. Colorectal Dis. 2018, 33, 1259–1267. [Google Scholar] [CrossRef] [PubMed]
- Gustafsson, U.O.; Oppelstrup, H.; Thorell, A.; Nygren, J.; Ljungqvist, O. Adherence to the ERAS protocol is associated with 5-year survival after colorectal cancer surgery: A retrospective cohort study. World J. Surg. 2016, 40, 1741–1747. [Google Scholar] [CrossRef] [PubMed]
- Asklid, D.; Segelman, J.; Gedda, C.; Hjern, F.; Pekkari, K.; Gustafsson, U.O. The impact of perioperative fluid therapy on short-term outcomes and 5-year survival among patients undergoing colorectal cancer surgery—A prospective cohort study within an ERAS protocol. Eur. J. Surg. Oncol. 2017, 43, 1433–1439. [Google Scholar] [CrossRef] [PubMed]
- Pędziwiatr, M.; Małczak, P.; Mizera, M.; Witowski, J.; Torbicz, G.; Major, P.; Pisarska, M.; Wysocki, M.; Budzyński, A. There is no difference in outcome between laparoscopic and open surgery for rectal cancer: A systematic review and meta-analysis on short- and long-term oncologic outcomes. Tech. Coloproctol. 2017, 21, 595–604. [Google Scholar] [CrossRef] [PubMed]
- Pisarska, M.; Pędziwiatr, M.; Małczak, P.; Major, P.; Ochenduszko, S.; Zub-Pokrowiecka, A.; Kulawik, J.; Budzyński, A. Do we really need the full compliance with ERAS protocol in laparoscopic colorectal surgery? A prospective cohort study. Int. J. Surg. 2016, 36, 377–382. [Google Scholar] [CrossRef] [PubMed]
- ERAS Compliance Group. The impact of enhanced recovery protocol compliance on elective colorectal cancer resection: Results from an international registry. Ann. Surg. 2015, 261, 1153–1159. [Google Scholar] [CrossRef] [PubMed]
- Ljungqvist, O.; Scott, M.; Fearon, K.C. Enhanced recovery after surgery: A review. JAMA Surg. 2017, 152, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Pędziwiatr, M.; Pisarska, M.; Kisielewski, M.; Major, P.; Mydlowska, A.; Rubinkiewicz, M.; Winiarski, M.; Budzyński, A. ERAS protocol in laparoscopic surgery for colonic versus rectal carcinoma: Are there differences in short-term outcomes? Med. Oncol. 2016, 33, 56. [Google Scholar] [CrossRef] [PubMed]
- Pędziwiatr, M.; Pisarska, M.; Kisielewski, M.; Matłok, M.; Major, P.; Wierdak, M.; Budzyński, A.; Ljungqvist, O. Is ERAS in laparoscopic surgery for colorectal cancer changing risk factors for delayed recovery? Med. Oncol. 2016, 33, 25. [Google Scholar] [CrossRef] [PubMed]
- Pisarska, M.; Małczak, P.; Major, P.; Wysocki, M.; Budzyński, A.; Pędziwiatr, M. Enhanced recovery after surgery protocol in oesophageal cancer surgery: Systematic review and meta-analysis. PLoS ONE 2017, 12, e0174382. [Google Scholar] [CrossRef] [PubMed]
- Pędziwiatr, M.; Pisarska, M.; Major, P.; Grochowska, A.; Matłok, M.; Przęczek, K.; Stefura, T.; Budzyński, A.; Kłęk, S. Laparoscopic colorectal cancer surgery combined with enhanced recovery after surgery protocol (ERAS) reduces the negative impact of sarcopenia on short-term outcomes. Eur. J. Surg. Oncol. 2016, 42, 779–787. [Google Scholar] [CrossRef] [PubMed]
- Pędziwiatr, M.; Wierdak, M.; Nowakowski, M.; Pisarska, M.; Stanek, M.; Kisielewski, M.; Matłok, M.; Major, P.; Kłęk, S.; Budzyński, A. Cost minimization analysis of laparoscopic surgery for colorectal cancer within the enhanced recovery after surgery (ERAS) protocol: A single-centre, case-matched study. Wideochir. Inne Tech. Maloinwazyjne 2016, 11, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Agha, R.A.; Borrelli, M.R.; Vella-Baldacchino, M.; Thavayogan, R.; Orgill, D.P.; STROCSS Group. The STROCSS statement: Strengthening the reporting of cohort studies in surgery. Int. J. Surg. 2017, 46, 198–202. [Google Scholar] [CrossRef] [PubMed]
- Kisialeuski, M.; Pędziwiatr, M.; Matłok, M.; Major, P.; Migaczewski, M.; Kołodziej, D.; Zub-Pokrowiecka, A.; Pisarska, M.; Budzyński, P.; Budzyński, A. Enhanced recovery after colorectal surgery in elderly patients. Wideochir. Inne Tech. Maloinwazyjne 2015, 10, 30–36. [Google Scholar]
- Pędziwiatr, M.; Kisialeuski, M.; Wierdak, M.; Stanek, M.; Natkaniec, M.; Matłok, M.; Major, P.; Małczak, P.; Budzyński, A. Early implementation of enhanced recovery after surgery (ERAS®) protocol—Compliance improves outcomes: A prospective cohort study. Int. J. Surg. 2015, 21, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Jin, J.; Min, S.; Liu, D.; Liu, L. Compliance with the enhanced recovery after surgery protocol and prognosis after colorectal cancer surgery: A prospective cohort study. Oncotarget 2017, 8, 53531–53541. [Google Scholar] [PubMed]
- Bakker, N.; Cakir, H.; Doodeman, H.J.; Houdijk, A.P. Eight years of experience with enhanced recovery after surgery in patients with colon cancer: Impact of measures to improve adherence. Surgery 2015, 157, 1130–1136. [Google Scholar] [CrossRef] [PubMed]
- Martin, D.; Roulin, D.; Addor, V.; Blanc, C.; Demartines, N.; Hübner, M. Enhanced recovery implementation in colorectal surgery-temporary or persistent improvement? Langenbecks Arch. Surg. 2016, 401, 1163–1169. [Google Scholar] [CrossRef] [PubMed]
- Gillissen, F.; Hoff, C.; Maessen, J.M.; Winkens, B.; Teeuwen, J.H.; Von Meyenfeldt, M.F.; Dejong, C.H. Structured synchronous implementation of an enhanced recovery program in elective colonic surgery in 33 hospitals in The Netherlands. World J. Surg. 2013, 37, 1082–1093. [Google Scholar] [CrossRef] [PubMed]
- Hendry, P.O.; Hausel, J.; Nygren, J.; Lassen, K.; Dejong, C.H.; Ljungqvist, O.; Fearon, K.C.; Enhanced Recovery after Surgery Study Group. Determinants of outcome after colorectal resection within an enhanced recovery programme. Br. J. Surg. 2009, 96, 197–205. [Google Scholar] [CrossRef] [PubMed]
- Gillissen, F.; Ament, S.M.; Maessen, J.M.; Dejong, C.H.; Dirksen, C.D.; van der Weijden, T.; Von Meyenfeldt, M.F. Sustainability of an enhanced recovery after surgery program (ERAS) in colonic surgery. World J. Surg. 2015, 39, 526–533. [Google Scholar] [CrossRef] [PubMed]
- Garfinkle, R.; Abou-Khalil, J.; Morin, N.; Ghitulescu, G.; Vasilevsky, C.A.; Gordon, P.; Demian, M.; Boutros, M. Is there a role for oral antibiotic preparation alone before colorectal surgery? ACS-NSQIP analysis by coarsened exact matching. Dis. Colon Rectum 2017, 60, 729–737. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Parameter | Group 1 | Group 2 | Group 3 | Group 4 | p Value |
|---|---|---|---|---|---|
| Number of patients, n | 100 | 100 | 100 | 100 | - |
| Females, n (%) | 47 | 48 | 39 | 48 | 0.5095 |
| Males, n (%) | 53 | 52 | 61 | 52 | |
| Mean age, years ± SD | 65.2 ± 12.2 | 64.2 ± 13.4 | 65.2 ± 13.5 | 62.4 ± 13.9 | 0.0712 |
| BMI, kg/m2 ± SD | 25.7 ± 4.4 | 26.9 ± 5.8 | 26.2 ± 4.3 | 26.7 ± 4.4 | 0.1102 |
| ASA 1, n (%) | 3 | 3 | 1 | 4 | 0.6989 |
| ASA 2, n (%) | 58 | 57 | 65 | 60 | |
| ASA 3, n (%) | 33 | 39 | 30 | 31 | |
| ASA 4, n (%) | 3 | 1 | 4 | 2 | |
| Any comorbidity, n (%) | 74 | 75 | 68 | 61 | 0.1167 |
| Cardiovascular, n (%) | 40 | 30 | 37 | 35 | 0.5061 |
| Hypertension, n (%) | 49 | 56 | 52 | 48 | 0.6699 |
| Diabetes, n (%) | 20 | 17 | 15 | 19 | 0.7962 |
| Pulmonary disease, n (%) | 15 | 14 | 5 | 7 | |
| Renal disease, n (%) | 6 | 11 | 5 | 5 | 0.3085 |
| Liver disease, n (%) | 3 | 5 | 5 | 3 | 0.7886 |
| AJCC Stage 1, n (%) | 27 | 44 | 36 | 36 | 0.1108 |
| AJCC Stage 2, n (%) | 37 | 27 | 25 | 27 | |
| AJCC Stage 3, n (%) | 24 | 20 | 21 | 29 | |
| AJCC Stage 4, n (%) | 12 | 9 | 18 | 8 | |
| Colon, n (%) | 67 | 74 | 59 | 61 | 0.1101 |
| Rectum, n (%) | 33 | 26 | 41 | 39 | |
| Median operative time, min (IQR) | 175 (130–200) | 210 (180–240) | 180 (150–240) | 185 (150–220) | <0.0001 |
| Median intraoperative blood loss, mL (IQR) | 50 (30–100) | 50 (50–100) | 100 (50–200) | 100 (50–150) | 0.0002 |
| Parameter | Group 1 | Group 2 | Group 3 | Group 4 | p Value |
|---|---|---|---|---|---|
| Median compliance with ERAS protocol, % (IQR) | 76.9 (69.2–84.6) | 92.3 (84.6–100) | 84.6 (76.9–92.3) | 84.6 (76.9–92.3) | <0.0001 * |
| Preoperative compliance, % (IQR) | 80 (60–100) | 100 (90–100) | 100 (80–100) | 100 (80–100) | |
| Intraoperative compliance, % (IQR) | 80 (60–80) | 80 (80–100) | 80 (60-80) | 80 (60–80) | |
| Postoperative compliance, % (IQR) | 67 (50–83) | 83 (83.3–100) | 83 (83–100) | 83 (67–83) | |
| Introduction of full oral diet on the first postoperative day, n (%) | 54 | 83 | 83 | 64 | <0.0001 ** |
| Mobilisation on the first postoperative day, n (%) | 74 | 92 | 91 | 94 | <0.0001* |
| No postoperative use of opioids, n (%) | 58 | 67 | 58 | 44 | 0.0114 *** |
| Parameter | Group 1 | Group 2 | Group 3 | Group 4 | p Value |
|---|---|---|---|---|---|
| Time to first flatus, days ± SD | 2.5 ± 1.4 | 2.1 ± 2.6 | 2.0 ± 1.8 | 1.7 ± 1.4 | 0.0001 * |
| Patients without complications, n (%) | 67 | 77 | 73 | 73 | 0.4649 |
| Patients with complications, n (%) | 33 | 23 | 27 | 27 | |
| Clavien-Dindo 1, n (%) | 20 | 10 | 7 | 12 | 0.4521 |
| Clavien-Dindo 2, n (%) | 4 | 4 | 7 | 6 | |
| Clavien-Dindo 3, n (%) | 7 | 7 | 10 | 5 | |
| Clavien-Dindo4, n (%) | 1 | 2 | 1 | 3 | |
| Clavien-Dindo 5, n (%) | 1 | 0 | 2 | 1 | |
| Mean length of hospital stay, days ± SD | 6.6 ± 5.6 | 5.9 ± 6.2 | 4.9 ± 3.1 | 5.2 ± 3.4 | 0.0025 * |
| Median length of hospital stay, days (IQR) | 5 (4–7) | 4 (2–6) | 4 (2–7) | 4 (3–6) | |
| Readmission, n (%) | 11 | 10 | 8 | 12 | 0.7397 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pisarska, M.; Gajewska, N.; Małczak, P.; Wysocki, M.; Major, P.; Milian-Ciesielska, K.; Budzyński, A.; Pędziwiatr, M. Is It Possible to Maintain High Compliance with the Enhanced Recovery after Surgery (ERAS) Protocol?—A Cohort Study of 400 Consecutive Colorectal Cancer Patients. J. Clin. Med. 2018, 7, 412. https://doi.org/10.3390/jcm7110412
Pisarska M, Gajewska N, Małczak P, Wysocki M, Major P, Milian-Ciesielska K, Budzyński A, Pędziwiatr M. Is It Possible to Maintain High Compliance with the Enhanced Recovery after Surgery (ERAS) Protocol?—A Cohort Study of 400 Consecutive Colorectal Cancer Patients. Journal of Clinical Medicine. 2018; 7(11):412. https://doi.org/10.3390/jcm7110412
Chicago/Turabian StylePisarska, Magdalena, Natalia Gajewska, Piotr Małczak, Michał Wysocki, Piotr Major, Katarzyna Milian-Ciesielska, Andrzej Budzyński, and Michał Pędziwiatr. 2018. "Is It Possible to Maintain High Compliance with the Enhanced Recovery after Surgery (ERAS) Protocol?—A Cohort Study of 400 Consecutive Colorectal Cancer Patients" Journal of Clinical Medicine 7, no. 11: 412. https://doi.org/10.3390/jcm7110412
APA StylePisarska, M., Gajewska, N., Małczak, P., Wysocki, M., Major, P., Milian-Ciesielska, K., Budzyński, A., & Pędziwiatr, M. (2018). Is It Possible to Maintain High Compliance with the Enhanced Recovery after Surgery (ERAS) Protocol?—A Cohort Study of 400 Consecutive Colorectal Cancer Patients. Journal of Clinical Medicine, 7(11), 412. https://doi.org/10.3390/jcm7110412