Epidemiology and Prognostic Importance of Atrial Fibrillation in Kidney Transplant Recipients: A Meta-Analysis

 , , ,
, , ,  ,
, 
Abstract
1. Introduction
2. Methods
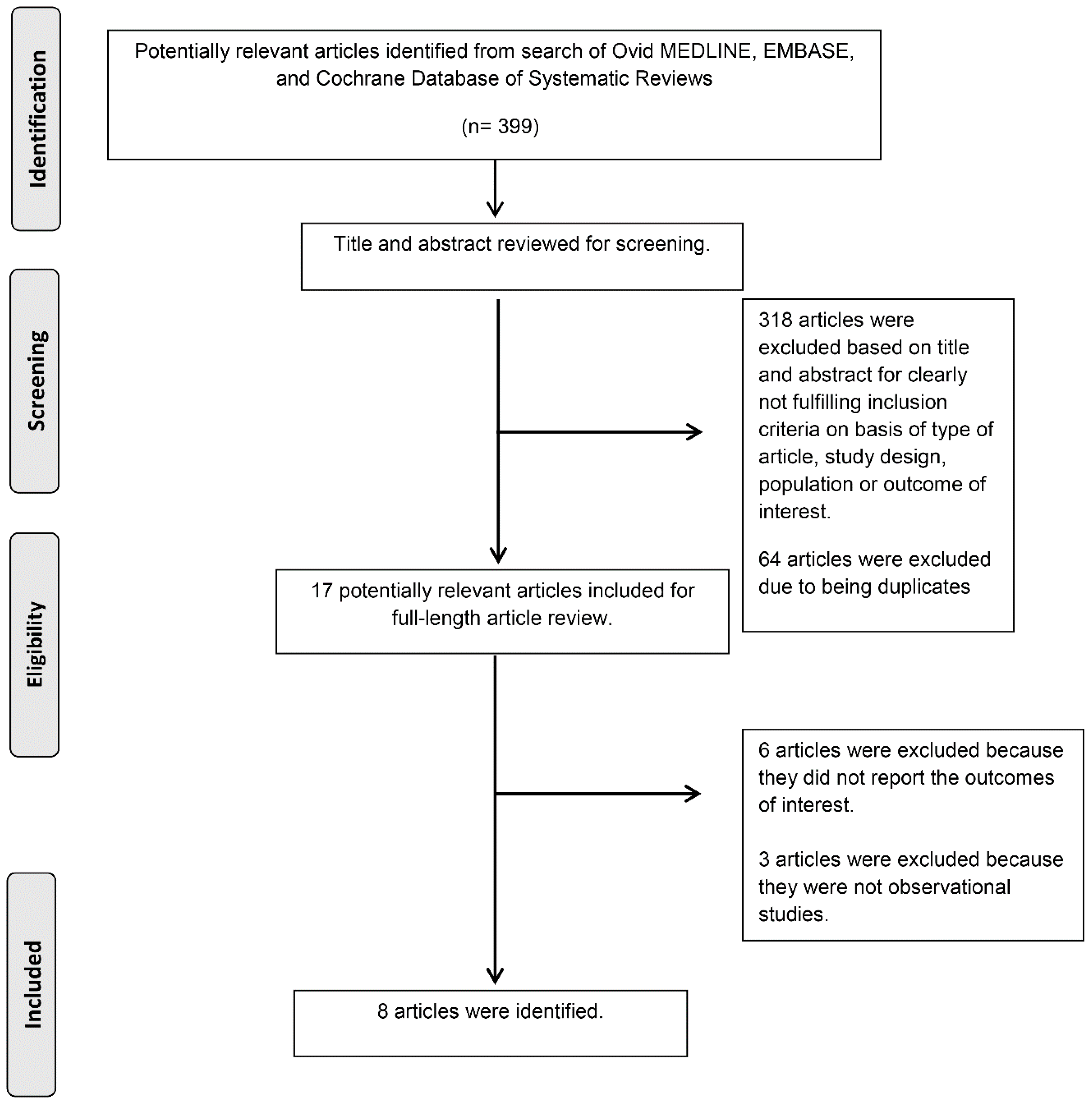
2.1. Search Strategy and Literature Review
2.2. Selection Criteria
2.3. Data Abstraction
2.4. Statistical Analysis
3. Results
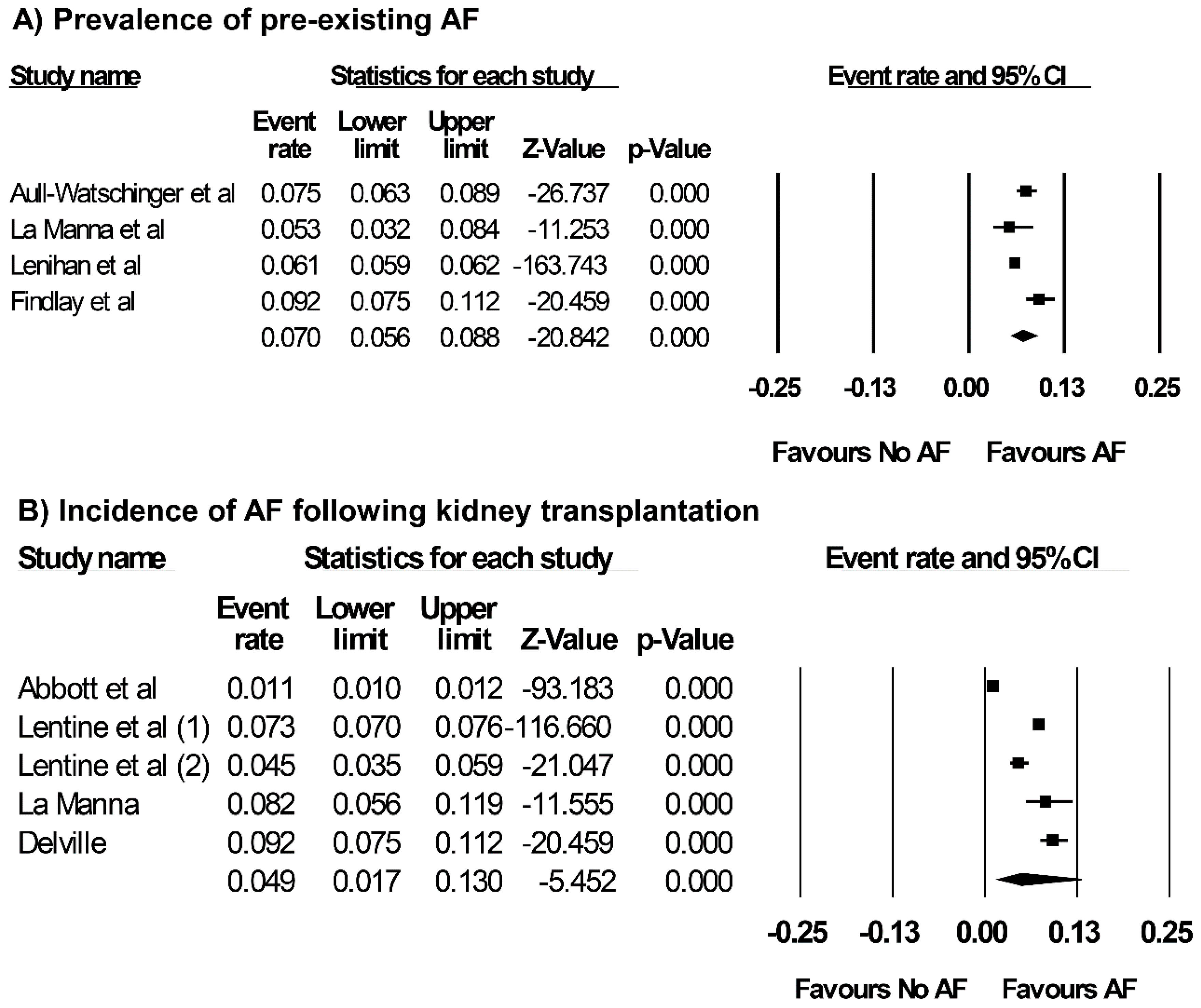
3.1. Prevalence of Pre-Existing AF and Incidence of AF after Kidney Transplantation
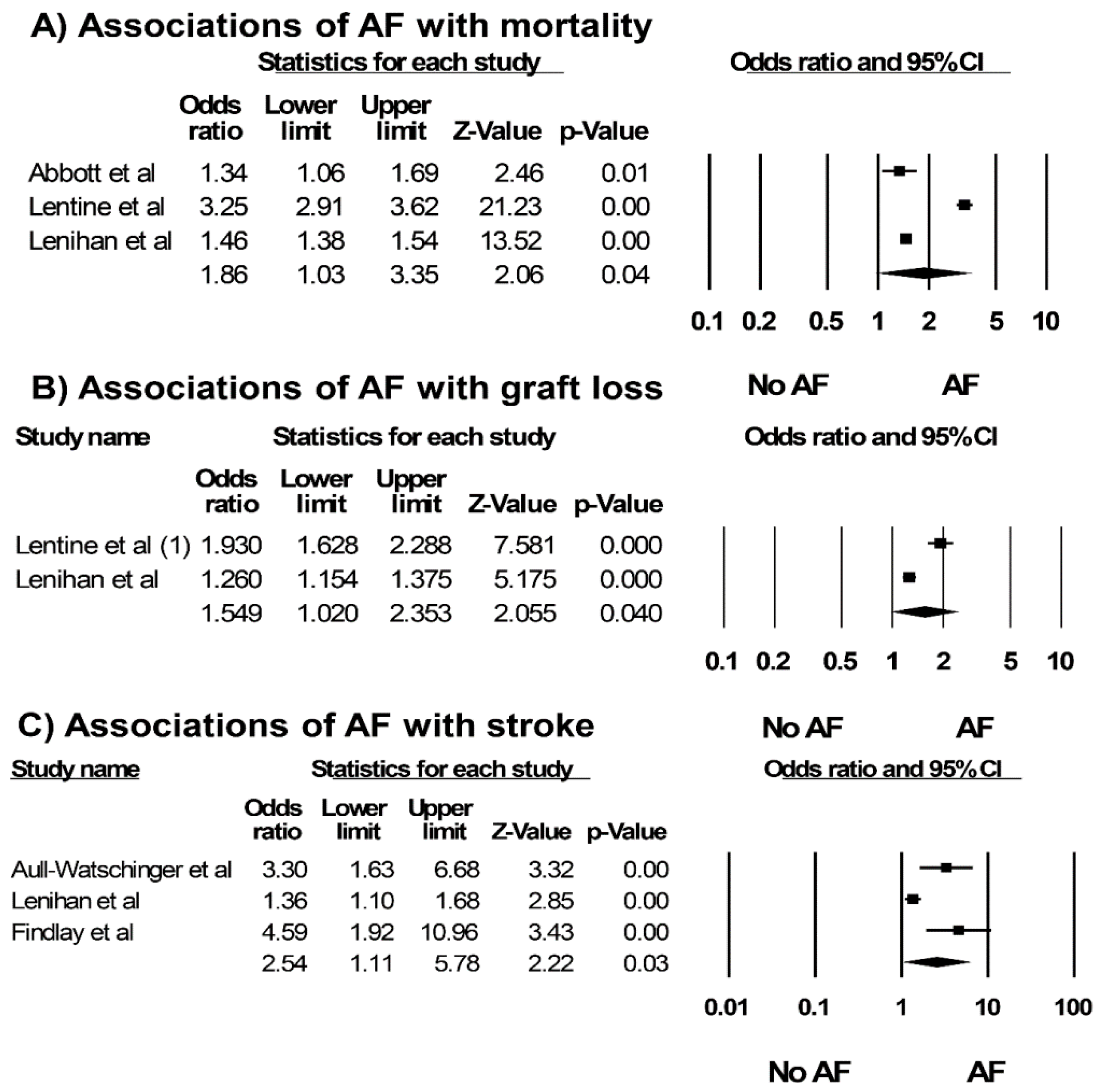
3.2. Risk Factors of AF and Outcomes of Kidney Transplant Recipients with AF
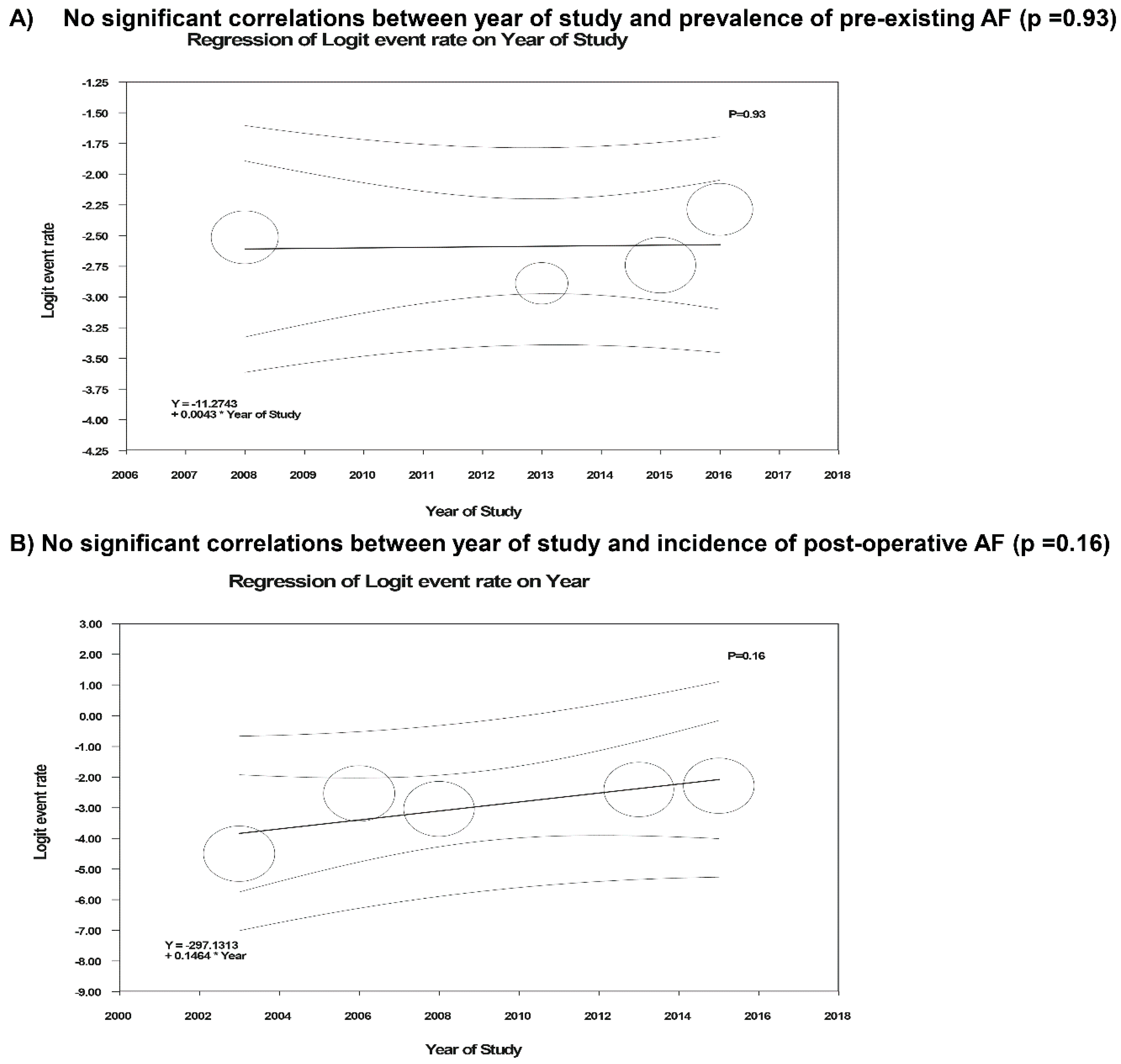
3.3. Evaluation for Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lip, G.Y.H.; Brechin, C.M.; Lane, D.A. The global burden of atrial fibrillation and stroke: A systematic review of the epidemiology of atrial fibrillation in regions outside North America and Europe. Chest 2012, 142, 1489–1498. [Google Scholar] [CrossRef] [PubMed]
- Schnabel, R.B.; Yin, X.; Gona, P.; Larson, M.G.; Beiser, A.S.; McManus, D.D.; Newton-Cheh, C.; Lubitz, S.A.; Magnani, J.W.; Ellinor, P.T.; et al. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: A cohort study. Lancet 2015, 386, 154–162. [Google Scholar] [CrossRef]
- Zoni-Berisso, M.; Lercari, F.; Carazza, T.; Domenicucci, S. Epidemiology of atrial fibrillation: European perspective. Clin. Epidemiol. 2014, 6, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Andrade, J.; Khairy, P.; Dobrev, D.; Nattel, S. The clinical profile and pathophysiology of atrial fibrillation: Relationships among clinical features, epidemiology, and mechanisms. Circ. Res. 2014, 114, 1453–1468. [Google Scholar] [CrossRef] [PubMed]
- Lenihan, C.R.; Montez-Rath, M.E.; Scandling, J.D.; Turakhia, M.P.; Winkelmayer, W.C. Outcomes after kidney transplantation of patients previously diagnosed with atrial fibrillation. Am. J. Transplant. 2013, 13, 1566–1575. [Google Scholar] [CrossRef] [PubMed]
- Miyasaka, Y.; Barnes, M.E.; Gersh, B.J.; Cha, S.S.; Bailey, K.R.; Abhayaratna, W.P.; Seward, J.B.; Tsang, T.S. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation 2006, 114, 119–125. [Google Scholar] [CrossRef] [PubMed]
- January, C.T.; Wann, L.S.; Alpert, J.S.; Calkins, H.; Cigarroa, J.E.; Cleveland, J.C., Jr.; Conti, J.B.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; et al. American College of Cardiology/American Heart Association Task Force on Practice G. 2014 AHA/ACC/HRS Guideline for the Management of Patients with Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. J. Am. Coll. Cardiol. 2014, 64, e1–e76. [Google Scholar] [CrossRef] [PubMed]
- Odutayo, A.; Wong, C.X.; Hsiao, A.J.; Hopewell, S.; Altman, D.G.; Emdin, C.A. Atrial fibrillation and risks of cardiovascular disease, renal disease, and death: Systematic review and meta-analysis. BMJ 2016, 354. [Google Scholar] [CrossRef] [PubMed]
- Abbott, K.C.; Trespalacios, F.C.; Taylor, A.J.; Agodoa, L.Y. Atrial fibrillation in chronic dialysis patients in the United States: Risk factors for hospitalization and mortality. BMC Nephrol. 2003, 4. [Google Scholar] [CrossRef]
- Bauer, A.; Limperger, V.; Nowak-Gottl, U. End-stage renal disease and thrombophilia. Hamostaseologie 2016, 36, 103–107. [Google Scholar] [CrossRef] [PubMed]
- Mavrakanas, T.A.; Charytan, D.M. Cardiovascular complications in chronic dialysis patients. Curr. Opin. Nephrol. Hypertens. 2016, 25, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, D.; Sood, M.M.; Rigatto, C.; Holden, R.M.; Hiremath, S.; Clase, C.M. Systematic review and meta-analysis of incidence, prevalence and outcomes of atrial fibrillation in patients on dialysis. Nephrol. Dial. Transplant. 2012, 27, 3816–3822. [Google Scholar] [CrossRef] [PubMed]
- Bansal, N.; Hsu, C.Y.; Go, A.S. Intersection of cardiovascular disease and kidney disease: Atrial fibrillation. Curr. Opin. Nephrol. Hypertens. 2014, 23, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Chugh, S.S.; Havmoeller, R.; Narayanan, K.; Singh, D.; Rienstra, M.; Benjamin, E.J.; Gillum, R.F.; Kim, Y.H.; McAnulty, J.H., Jr.; Zheng, Z.J.; et al. Worldwide epidemiology of atrial fibrillation: A Global Burden of Disease 2010 Study. Circulation 2014, 129, 837–847. [Google Scholar] [CrossRef] [PubMed]
- Winkelmayer, W.C.; Patrick, A.R.; Liu, J.; Brookhart, M.A.; Setoguchi, S. The increasing prevalence of atrial fibrillation among hemodialysis patients. J. Am. Soc. Nephrol. 2011, 22, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Schold, J.D.; Buccini, L.D.; Goldfarb, D.A.; Flechner, S.M.; Poggio, E.D.; Sehgal, A.R. Association between kidney transplant center performance and the survival benefit of transplantation versus dialysis. Clin. J. Am. Soc. Nephrol. 2014, 9, 1773–1780. [Google Scholar] [CrossRef] [PubMed]
- Kaballo, M.A.; Canney, M.; O’Kelly, P.; Williams, Y.; O’Seaghdha, C.M.; Conlon, P.J. A comparative analysis of survival of patients on dialysis and after kidney transplantation. Clin. Kidney J. 2018, 11, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, R.A.; Ashby, V.B.; Milford, E.L.; Ojo, A.O.; Ettenger, R.E.; Agodoa, L.Y.; Held, P.J.; Port, F.K. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N. Engl. J. Med. 1999, 341, 1725–1730. [Google Scholar] [CrossRef] [PubMed]
- Laupacis, A.; Keown, P.; Pus, N.; Krueger, H.; Ferguson, B.; Wong, C.; Muirhead, N. A study of the quality of life and cost-utility of renal transplantation. Kidney Int. 1996, 50, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Gill, J.S.; Tonelli, M.; Johnson, N.; Kiberd, B.; Landsberg, D.; Pereira, B.J. The impact of waiting time and comorbid conditions on the survival benefit of kidney transplantation. Kidney Int. 2005, 68, 2345–2351. [Google Scholar] [CrossRef] [PubMed]
- Hariharan, S.; Johnson, C.P.; Bresnahan, B.A.; Taranto, S.E.; McIntosh, M.J.; Stablein, D. Improved graft survival after renal transplantation in the United States, 1988 to 1996. N. Engl. J. Med. 2000, 342, 605–612. [Google Scholar] [CrossRef] [PubMed]
- Meier-Kriesche, H.U.; Schold, J.D.; Kaplan, B. Long-term renal allograft survival: Have we made significant progress or is it time to rethink our analytic and therapeutic strategies? Am. J. Transplant. 2004, 4, 1289–1295. [Google Scholar] [CrossRef] [PubMed]
- Wazna, E.; Pazik, J.; Perkowska-Ptasinska, A.; Durlik, M. Does histopathology of implanted kidney according to Banff 07 help predict long-term transplantation outcome? Transplant. Proc. 2018, 50, 1765–1768. [Google Scholar] [CrossRef] [PubMed]
- Bansal, N.; Zelnick, L.R.; Alonso, A.; Benjamin, E.J.; de Boer, I.H.; Deo, R.; Katz, R.; Kestenbaum, B.; Mathew, J.; Robinson-Cohen, C.; et al. eGFR and Albuminuria in Relation to Risk of Incident Atrial Fibrillation: A Meta-Analysis of the Jackson Heart Study, the Multi-Ethnic Study of Atherosclerosis, and the Cardiovascular Health Study. Clin. J. Am. Soc. Nephrol. 2017, 12, 1386–1398. [Google Scholar] [CrossRef] [PubMed]
- La Manna, G.; Boriani, G.; Capelli, I.; Marchetti, A.; Grandinetti, V.; Spazzoli, A.; Dalmastri, V.; Todeschini, P.; Rucci, P.; Stefoni, S. Incidence and predictors of postoperative atrial fibrillation in kidney transplant recipients. Transplantation 2013, 96, 981–986. [Google Scholar] [CrossRef] [PubMed]
- Aull-Watschinger, S.; Konstantin, H.; Demetriou, D.; Schillinger, M.; Habicht, A.; Horl, W.H.; Watschinger, B. Pre-transplant predictors of cerebrovascular events after kidney transplantation. Nephrol. Dial. Transplant. 2008, 23, 1429–1435. [Google Scholar] [CrossRef] [PubMed]
- Lenihan, C.R.; Montez-Rath, M.E.; Shen, J.I.; Scandling, J.D.; Turakhia, M.P.; Chang, T.I.; Winkelmayer, W.C. Correlates and outcomes of warfarin initiation in kidney transplant recipients newly diagnosed with atrial fibrillation. Nephrol. Dial. Transplant. 2015, 30, 321–329. [Google Scholar] [CrossRef] [PubMed]
- Findlay, M.D.; Thomson, P.C.; MacIsaac, R.; Jardine, A.G.; Patel, R.K.; Stevens, K.K.; Rutherford, E.; Clancy, M.; Geddes, C.C.; Dawson, J.; et al. Risk factors and outcome of stroke in renal transplant recipients. Clin. Transplant. 2016, 30, 918–924. [Google Scholar] [CrossRef] [PubMed]
- Abbott, K.C.; Reynolds, J.C.; Taylor, A.J.; Agodoa, L.Y. Hospitalized atrial fibrillation after renal transplantation in the United States. Am. J. Transplant. 2003, 3, 471–476. [Google Scholar] [CrossRef] [PubMed]
- Lentine, K.L.; Schnitzler, M.A.; Abbott, K.C.; Li, L.; Xiao, H.; Burroughs, T.E.; Takemoto, S.K.; Willoughby, L.M.; Gavard, J.A.; Brennan, D.C. Incidence, predictors, and associated outcomes of atrial fibrillation after kidney transplantation. Clin. J. Am. Soc. Nephrol. 2006, 1, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Lentine, K.L.; Rocca-Rey, L.A.; Bacchi, G.; Wasi, N.; Schmitz, L.; Salvalaggio, P.R.; Abbott, K.C.; Schnitzler, M.A.; Neri, L.; Brennan, D.C. Obesity and cardiac risk after kidney transplantation: Experience at one center and comprehensive literature review. Transplantation 2008, 86, 303–312. [Google Scholar] [CrossRef]
- Delville, M.; Sabbah, L.; Girard, D.; Elie, C.; Manceau, S.; Piketty, M.; Martinez, F.; Mejean, A.; Legendre, C.; Sberro-Soussan, R. Prevalence and predictors of early cardiovascular events after kidney transplantation: Evaluation of pre-transplant cardiovascular work-up. PLoS ONE 2015, 10. [Google Scholar] [CrossRef]
- Rodriguez-Rodriguez, A.E.; Trinanes, J.; Porrini, E.; Velazquez-Garcia, S.; Fumero, C.; Vega-Prieto, M.J.; Diez-Fuentes, M.L.; Luis Lima, S.; Salido, E.; Torres, A. Glucose homeostasis changes and pancreatic beta-cell proliferation after switching to cyclosporin in tacrolimus-induced diabetes mellitus. Nefrologia 2015, 35, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Holdaas, H.; Potena, L.; Saliba, F. mTOR inhibitors and dyslipidemia in transplant recipients: a cause for concern? Transplant. Rev. (Orlando) 2015, 29, 93–102. [Google Scholar] [CrossRef] [PubMed]
- Pisano, G.; Fracanzani, A.L.; Caccamo, L.; Donato, M.F.; Fargion, S. Cardiovascular risk after orthotopic liver transplantation, a review of the literature and preliminary results of a prospective study. World J. Gastroenterol. 2016, 22, 8869–8882. [Google Scholar] [CrossRef] [PubMed]
- Muller-Deile, J.; Schwarz, A.; Menne, J. Thromboembolism in renal transplant artery due to atrial fibrillation. Clin. Nephrol. Case Stud. 2013, 1, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Hristova, M.; van Beek, C.; Schurgers, L.J.; Lanske, B.; Danziger, J. Rapidly progressive severe vascular calcification sparing the kidney allograft following warfarin initiation. Am. J. Kidney Dis. 2010, 56, 1158–1162. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. PLoS Med. 2007, 4. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6. [Google Scholar] [CrossRef] [PubMed]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Easterbrook, P.J.; Berlin, J.A.; Gopalan, R.; Matthews, D.R. Publication bias in clinical research. Lancet 1991, 337, 867–872. [Google Scholar] [CrossRef]
- VanWagner, L.B.; Serper, M.; Kang, R.; Levitsky, J.; Hohmann, S.; Abecassis, M.; Skaro, A.; Lloyd-Jones, D.M. Factors associated with major adverse cardiovascular events after liver transplantation among a national sample. Am. J. Transplant. 2016, 16, 2684–2694. [Google Scholar] [CrossRef] [PubMed]
- Bezinover, D.; McQuillan, P.; Rossignol, J.; Uemura, T.; Kadry, Z.; Janicki, P. Vasoplegic shock during liver transplantation: Is the preoperative cGMP plasma level a potential predictor of hemodynamic instability? Med. Sci. Monit. 2010, 16, CS114–CS117. [Google Scholar] [PubMed]
- Rudnick, M.R.; Marchi, L.D.; Plotkin, J.S. Hemodynamic monitoring during liver transplantation: A state of the art review. World J. Hepatol. 2015, 7, 1302–1311. [Google Scholar] [CrossRef] [PubMed]
- Gallegos-Orozco, J.F.; Charlton, M.R. Predictors of cardiovascular events after liver transplantation. Clin. Liver Dis. 2017, 21, 367–379. [Google Scholar] [CrossRef] [PubMed]
- Bruhl, S.R.; Vetteth, S.; Rees, M.; Grubb, B.P.; Khouri, S.J. Post-reperfusion syndrome during renal transplantation: A retrospective study. Int. J. Med. Sci. 2012, 9, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.Z.; Huang, F.Y.; Fan, S.Z.; Chen, T.L.; Lee, B.H.; Lee, T.S.; Chen, K.M. Evaluation of systemic hemodynamic effects on post-transplant perfusion to renal allograft. Ma Zui Xue Za Zhi 1990, 28, 35–42. [Google Scholar] [PubMed]
- Schwenger, V.; Zeier, M.; Ritz, E. Hypertension after renal transplantation. Ann. Transplant. 2001, 6, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Lentine, K.L.; Costa, S.P.; Weir, M.R.; Robb, J.F.; Fleisher, L.A.; Kasiske, B.L.; Carithers, R.L.; Ragosta, M.; Bolton, K.; Auerbach, A.D.; et al. Cardiac disease evaluation and management among kidney and liver transplantation candidates: A scientific statement from the American Heart Association and the American College of Cardiology Foundation. J. Am. Coll. Cardiol. 2012, 60, 434–480. [Google Scholar] [CrossRef] [PubMed]
- Lentine, K.L.; Rocca Rey, L.A.; Kolli, S.; Bacchi, G.; Schnitzler, M.A.; Abbott, K.C.; Xiao, H.; Brennan, D.C. Variations in the risk for cerebrovascular events after kidney transplant compared with experience on the waiting list and after graft failure. Clin. J. Am. Soc. Nephrol. 2008, 3, 1090–1101. [Google Scholar] [CrossRef] [PubMed]
- Glicklich, D.; Vohra, P. Cardiovascular risk assessment before and after kidney transplantation. Cardiol. Rev. 2014, 22, 153–162. [Google Scholar] [CrossRef] [PubMed]
- January, C.T.; Wann, L.S.; Alpert, J.S.; Calkins, H.; Cigarroa, J.E.; Cleveland, J.C., Jr.; Conti, J.B.; Ellinor, P.T.; Ezekowitz, M.D.; Field, M.E.; et al. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society. Circulation 2014, 130, 2071–2104. [Google Scholar] [CrossRef] [PubMed]
- Kisters, K.; Cziborra, M.; Funke, C.; Brylak, S.; Hausberg, M. Amiodarone-tacrolimus interaction in kidney transplantation. Clin. Nephrol. 2008, 70, 563. [Google Scholar] [CrossRef] [PubMed]
- Burger, C.I.; Clase, C.M.; Gangji, A.S. Case report: Drug interaction between tacrolimus and amiodarone with QT prolongation. Transplantation 2010, 89, 1166–1167. [Google Scholar] [CrossRef] [PubMed]
- Malyszko, J.; Lopatowska, P.; Mlodawska, E.; Musialowska, D.; Malyszko, J.S.; Tomaszuk-Kazberuk, A. Atrial fibrillation in kidney transplant recipients: Is there a place for the novel drugs? Nephrol. Dial. Transplant. 2017, 33, 1304–1309. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Aull-Watschinger et al. [26] | La Manna et al. [25] | Lenihan et al. [5] | Findlay et al. [28] |
|---|---|---|---|---|
| Country | Austria | Italy | USA | UK |
| Study design | Cohort | Cohort | Cohort | Cohort |
| Study year | 2008 | 2013 | 2015 | 2016 |
| Total number | 1633 | 304 | 62706 | 956 |
| Patients | Kidney or kidney-pancreas transplant patients in a single center | Kidney or kidney/liver transplant patients in a single center | Kidney transplant patients in the US renal Data System | Functioning kidney transplant patients in a single hospital |
| Living donor | 174/1633 (11%) | N/A | 10409/62706 (17%) | N/A |
| Anticoagulation | Antiplatelet or anticoagulation 454/1633 (28%) | N/A | N/A | Warfarin 137/956 (14%) |
| AF ascertainment | History of AF before kidney transplant; identified by medical record review | Postoperative AF until hospital discharge; identified by medical record review | History of AF before kidney transplant; identified by identified by ICD-9 code 427.3x in Medicare claims | History of AF before kidney transplant; identified by medical record review |
| Pre-operative AF | 122/1633 (7.5%) | 16/304 (5.3%) | 3794/62706 (6.1%) | 88/956 (9.2%) |
| Estimated prevalence | ||||
| Post-operative AF | N/A | POAF 25/304 (8.2%) | N/A | N/A |
| Estimated prevalence | De novo POAF 21/304 (6.9%) | |||
| Follow-up | Median 4 (IQR 1.5–6.7) years | Until hospital discharge | Mean 4.9 years | Median 5.4 years |
| Outcomes | TIA/stroke 3.30 (1.63–6.67) | POAF and myocardial ischemia 11.58 (0.70–191.06) | Death 1.46 (1.38–1.54) | Stroke 4.59 (1.92–10.94) |
| All-cause graft loss 1.41 (1.34–1.48) | Ischemic stroke in AF 1.72% at 1 year and 4.07% at 3 years | |||
| Death-censored graft loss 1.26 (1.15–1.37) | ||||
| Death-censored ischemic stroke 1.36 (1.10–1.68) | Ischemic stroke risk in non-AF 0.72% at 1 year and 2.07% at 3 years | |||
| Confounder adjustment | DM, ejection fraction, C-reactive protein, hyperlipidemia, polycystic kidney disease, duration of dialysis, sex, age, degree of carotid stenosis | None | Age, sex, race, BMI, cause of ESRD, dialysis vintage and modality, SNF utilization, number of hospital days and non-nephrology clinic visits, previous transplants, comorbidities, blood type, PRA, donor age and sex, transplant type, HLA mismatches, cold ischemia time | None |
| Newcastle-Ottawa Scale | S 3 | S 3 | S 4 | S 3 |
| C 2 | C 2 | C 2 | C 2 | |
| O 3 | O 3 | O 3 | O 3 |
| Study | Abbott et al. [29] | Lentine et al. [30] | Lentine et al. [31] | Delville et al. [32] |
|---|---|---|---|---|
| Country | USA | USA | USA | France |
| Study design | Cohort | Cohort | Cohort | Cohort |
| Study year | 2003 | 2006 | 2008 | 2015 |
| Total number | 39628 | 31136 | 1102 | 244 |
| Patients | Kidney transplant patients in the US Renal Data System | Kidney transplant patients in the US Renal Data System | Kidney transplant patients in a single center | Kidney transplant patients aged >50 years in a single center |
| Living donor | 12259/39628 (31%) | 6993/31136 (22%) | 344/1102 (31%) | N/A |
| Anticoagulation | N/A | N/A | N/A | N/A |
| AF ascertainment | Hospitalizations for a primary diagnosis of AF; identified by ICD-9 code 427.31 | AF after kidney transplant; identified by ICD-9 code 427.3x | New-onset atrial fibrillation after kidney transplant; identified by ECG | New-onset atrial fibrillation after kidney transplant; identified by medical record review and ECG |
| Pre-operative AF | N/A | N/A | N/A | N/A |
| Estimated prevalence | ||||
| Post-operative AF | 432/39628 (1.1%) | New-onset AF | 5-year 50/1102 (4.5%) | 13/244 (5.3%) |
| At 6 months 810/31136 (2.6%) | ||||
| At 12 months 1121/31136 (3.6%) | ||||
| Estimated prevalence | ||||
| At 36 months 2273/31136 (7.3%) | ||||
| Follow-up | Mean 1.89 ± 1.15 years | Up to 36 months | 5 year | 1 year |
| Outcomes | Mortality 1.34 (1.06–1.69) | Mortality 3.25 (2.92–3.63) | N/A | N/A |
| Death-censored graft loss 1.93 (1.63–2.29) | ||||
| All-cause graft loss 2.88 (2.60–3.12) | ||||
| Confounder adjustment | Adjusted but not specified | Age, sex, race, education, employment, BMI, causes of ESRD, dialysis duration, sensitization, comorbid conditions, smoking, alcohol abuse. donor age and source, donor CMV status, degree of HLA matching, induction and maintenance immunosuppression, DGF, post-transplantation complications | N/A | N/A |
| Newcastle-Ottawa Scale | S 4 | S 4 | S 3 | S 3 |
| C 1 | C 2 | C 2 | C 2 | |
| O 3 | O 3 | O 3 | O 3 |
| Studies | Follow-up Time | Risk Factor Associated with AF after Kidney Transplantation |
|---|---|---|
| Abbott et al. [29] | Mean 1.89 ± 1.15 years | Older recipient age, higher BMI, DGF, rejection, ESRD due to hypertension, cyclosporine use, Graft loss |
| Lentine et al. [30] | Up to 36 months | Older recipient age, male sex, Caucasian, non-Hispanic, ESRD due to hypertension, longer dialysis duration before transplant, CAD, DGF, older donor age, post-transplantation complications (hypertension, anemia, new-onset diabetes, MI, graft failure) |
| La Manna et al. [25] | Until hospital discharge | Older age, kidney/liver transplant, history of acute myocardial infarction |
| Lentine et al. [31] | 5 year | BMI |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thongprayoon, C.; Chokesuwattanaskul, R.; Bathini, T.; Khoury, N.J.; Sharma, K.; Ungprasert, P.; Prasitlumkum, N.; Aeddula, N.R.; Watthanasuntorn, K.; Salim, S.A.; et al. Epidemiology and Prognostic Importance of Atrial Fibrillation in Kidney Transplant Recipients: A Meta-Analysis. J. Clin. Med. 2018, 7, 370. https://doi.org/10.3390/jcm7100370
Thongprayoon C, Chokesuwattanaskul R, Bathini T, Khoury NJ, Sharma K, Ungprasert P, Prasitlumkum N, Aeddula NR, Watthanasuntorn K, Salim SA, et al. Epidemiology and Prognostic Importance of Atrial Fibrillation in Kidney Transplant Recipients: A Meta-Analysis. Journal of Clinical Medicine. 2018; 7(10):370. https://doi.org/10.3390/jcm7100370
Chicago/Turabian StyleThongprayoon, Charat, Ronpichai Chokesuwattanaskul, Tarun Bathini, Nadeen J. Khoury, Konika Sharma, Patompong Ungprasert, Narut Prasitlumkum, Narothama Reddy Aeddula, Kanramon Watthanasuntorn, Sohail Abdul Salim, and et al. 2018. "Epidemiology and Prognostic Importance of Atrial Fibrillation in Kidney Transplant Recipients: A Meta-Analysis" Journal of Clinical Medicine 7, no. 10: 370. https://doi.org/10.3390/jcm7100370
APA StyleThongprayoon, C., Chokesuwattanaskul, R., Bathini, T., Khoury, N. J., Sharma, K., Ungprasert, P., Prasitlumkum, N., Aeddula, N. R., Watthanasuntorn, K., Salim, S. A., Kaewput, W., Koller, F. L., & Cheungpasitporn, W. (2018). Epidemiology and Prognostic Importance of Atrial Fibrillation in Kidney Transplant Recipients: A Meta-Analysis. Journal of Clinical Medicine, 7(10), 370. https://doi.org/10.3390/jcm7100370