
Integrated Treatment of PTSD and Substance Use Disorders: The Mediating Role of PTSD Improvement in the Reduction of Depression

Abstract
:1. Introduction
2. Method
2.1. Participants
2.2. Procedure
2.3. Treatments
2.4. Measures
2.5. Data Analytic Plan
3. Results
3.1. Baseline Demographics and Clinical Characteristics
3.2. Final Model Results
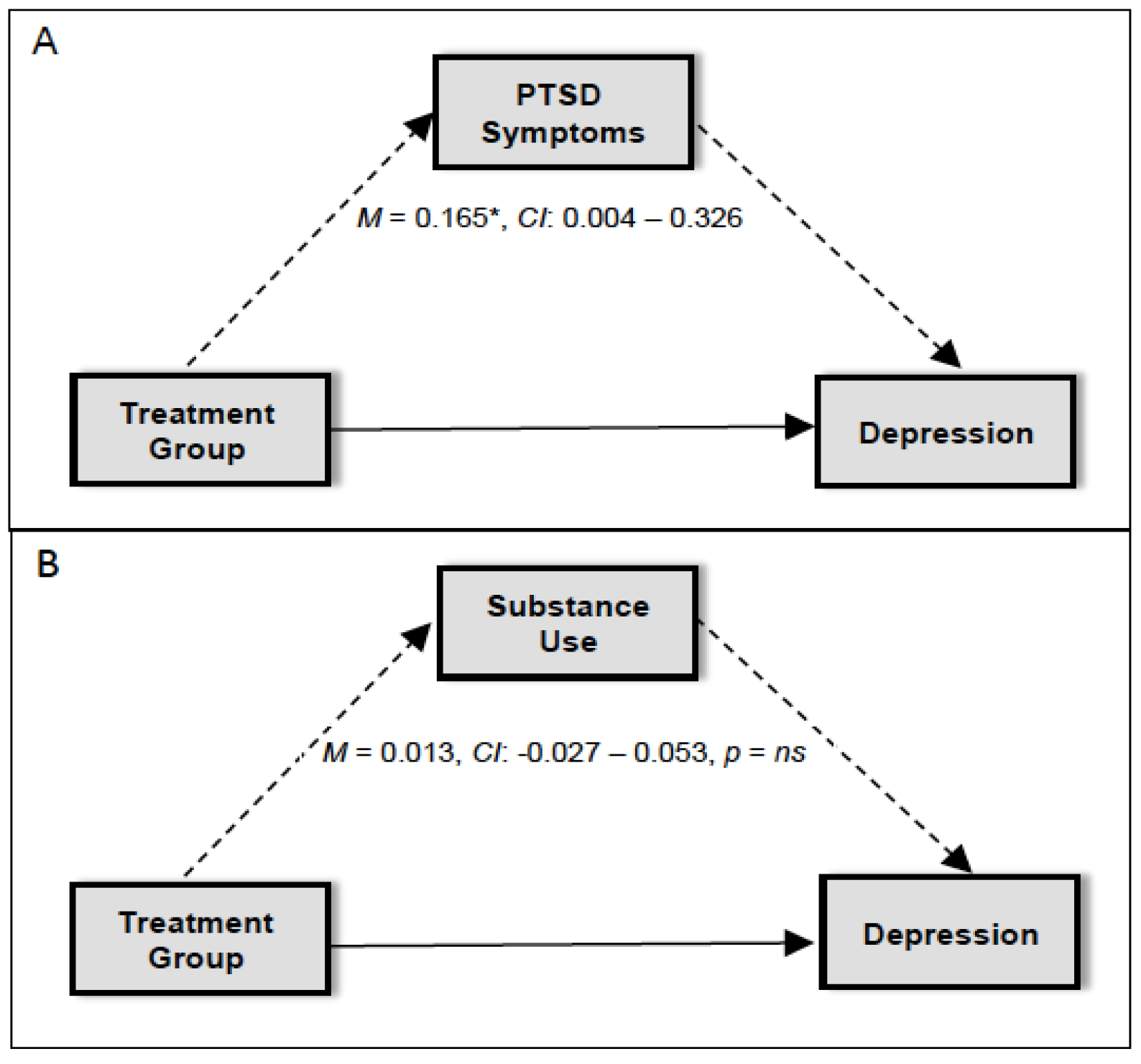
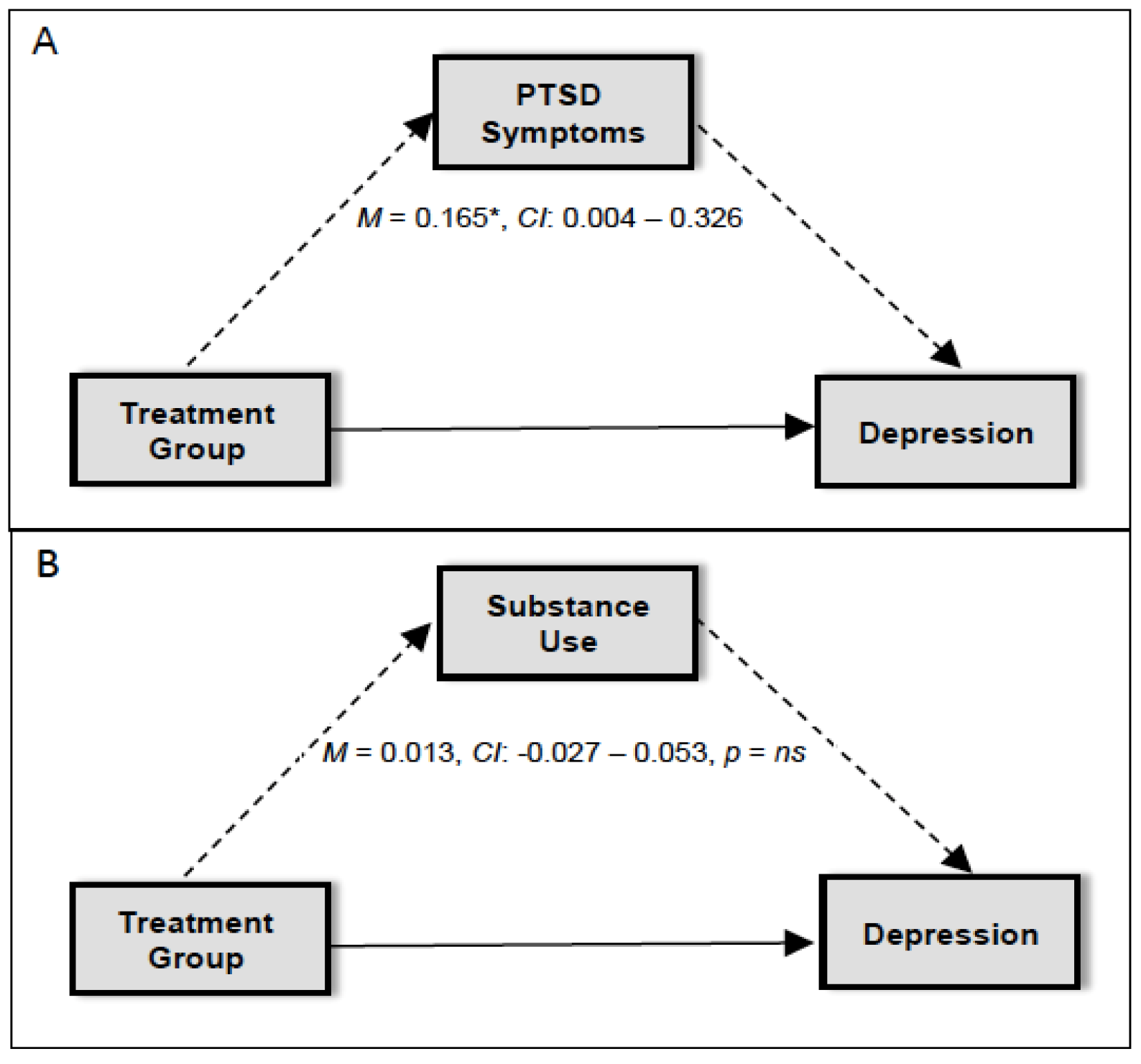
3.3. Mediators of Change in Depression
4. Discussion
4.1. Limitations
4.2. Future Directions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Kessler, R.C.; Chiu, W.T.; Demler, O.; Merikangas, K.R.; Walters, E.E. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 617–627. [Google Scholar] [CrossRef] [PubMed]
- Pietrzak, R.H.; Goldstein, R.B.; Southwick, S.M.; Grant, B.F. Prevalence and Axis I comorbidity of full and partial posttraumatic stress disorder in the United States: Results from Wave 2 of the National Epidemiologic Survey on Alcohol and Related Conditions. J. Anxiety Disord. 2011, 25, 456–465. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.K.; Natelson, B.H.; Mahan, C.M.; Lee, K.Y.; Murphy, F.M. Post-traumatic stress disorder and chronic fatigue syndrome-like illness among Gulf War veterans: A population-based survey of 30,000 veterans. Am. J. Epidemiol. 2003, 157, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Seal, K.H.; Bertenthal, D.; Miner, C.R.; Sen, S.; Marmar, C. Bringing the war back home: Mental health disorders among 103 788 US veterans returning from Iraq and Afghanistan seen at Department of Veterans Affairs Facilities. Arch. Intern. Med. 2007, 167, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Weiss, D.S.; Marmar, C.R.; Schlenger, W.E.; Fairbank, J.A.; Kathleen Jordan, B.; Hough, R.L.; Kulka, R.A. The prevalence of lifetime and partial post-traumatic stress disorder in Vietnam theater veterans. J. Trauma. Stress 1992, 5, 365–376. [Google Scholar] [CrossRef]
- Asnaani, A.; Reddy, M.K.; Shea, M.T. The impact of PTSD symptoms on physical and mental health functioning in returning veterans. J. Anxiety Disord. 2014, 28, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Hoge, C.W.; Auchterlonie, J.L.; Milliken, C.S. Mental Health Problems, Use of Mental Health Services, and Attrition From Military Service After Returning From Deployment to Iraq or Afghanistan. JAMA 2015, 295, 1023–1032. [Google Scholar] [CrossRef] [PubMed]
- Read, J.P.; Brown, P.J.; Kahler, C.W. Substance use and posttraumatic stress disorders: Symptom interplay and effects on outcome. Addict. Behav. 2004, 29, 1665–1672. [Google Scholar] [CrossRef] [PubMed]
- Saladin, M.E.; Brady, K.T.; Dansky, B.S.; Kilpatrick, D.G. Understanding comorbidity between PTSD and substance use disorders: Two preliminary investigations. Addict. Behav. 1995, 20, 643–655. [Google Scholar] [CrossRef]
- Blanco, C.; Xu, Y.; Brady, K.T.; Pérez-Fuentes, G.; Okuda, M.; Wang, S. Comorbidity of posttraumatic stress disorder with alcohol dependence among US adults: Results from National Epidemiological Survey on Alcohol and Related Conditions. Drug Alcohol Depend. 2013, 132, 630–638. [Google Scholar] [CrossRef] [PubMed]
- Norman, S.B.; Tate, S.R.; Anderson, K.G.; Brown, S.A. Do trauma history and PTSD symptoms influence addiction relapse context? Drug Alcohol Depend. 2007, 90, 89–96. [Google Scholar] [CrossRef] [PubMed]
- Back, S.E.; Brady, K.T.; Sonne, S.C.; Verduin, M.L. Symptom improvement in co-occurring PTSD and alcohol dependence. J. Nerv. Ment. Dis. 2006, 194, 690–696. [Google Scholar] [CrossRef] [PubMed]
- Ford, J.D.; Hawke, J.; Alessi, S.; Ledgerwood, D.; Petry, N. Psychological trauma and PTSD symptoms as predictors of substance dependence treatment outcomes. Behav. Res. Ther. 2007, 45, 2417–2431. [Google Scholar] [CrossRef] [PubMed]
- Ouimette, P.C.; Ahrens, C.; Moos, R.H.; Finney, J.W. During treatment changes in substance abuse patients with posttraumatic stress disorder. The influence of specific interventions and program environments. J. Subst. Abus. Treat. 1998, 15, 555–564. [Google Scholar] [CrossRef]
- Back, S.E.; Killeen, T.K.; Teer, A.P.; Hartwell, E.E.; Federline, A.; Beylotte, F.; Cox, E. Substance use disorders and PTSD: An exploratory study of treatment preferences among military veterans. Addict. Behav. 2014, 39, 369–373. [Google Scholar] [CrossRef] [PubMed]
- Killeen, T.K.; Back, S.E.; Brady, K.T. The use of exposure-based treatment among individuals with PTSD and co-occurring substance use disorders: Clinical considerations. J. Dual Diagn. 2011, 7, 194–206. [Google Scholar] [CrossRef] [PubMed]
- Brady, K.T.; Dansky, B.S.; Back, S.E.; Foa, E.B.; Carroll, K.M. Exposure therapy in the treatment of PTSD among cocaine-dependent individuals: Preliminary findings. J. Subst. Abus. Treat. 2001, 21, 47–54. [Google Scholar] [CrossRef]
- Hien, D.A.; Jiang, H.; Campbell, A.N.; Hu, M.C.; Miele, G.M.; Cohen, L.R.; Nunes, E.V. Do treatment improvements in PTSD severity affect substance use outcomes? A secondary analysis from a randomized clinical trial in NIDA’s Clinical Trials Network. Am. J. Psychiatry 2010, 167, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Kaczkurkin, A.N.; Asnaani, A.; Alpert, E.; Foa, E.B. The impact of treatment condition and the lagged effects of PTSD symptom severity and alcohol use on changes in alcohol craving. Behav. Res. Ther. 2016, 79, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Mills, K.L.; Teesson, M.; Back, S.E.; Brady, K.T.; Baker, A.L.; Hopwood, S.; Ewer, P.L. Integrated exposure-based therapy for co-occurring posttraumatic stress disorder and substance dependence: A randomized controlled trial. JAMA 2012, 308, 690–699. [Google Scholar] [CrossRef] [PubMed]
- Back, S.E.; Brady, K.T.; Jaanimägi, U.; Jackson, J. Cocaine dependence and PTSD: Symptom interplay and treatment preferences. Addict. Behav. 2006, 31, 351–354. [Google Scholar] [CrossRef] [PubMed]
- Back, S.E.; Killeen, T.; Badour, C.; Flanagan, J.; Korte, K.; Brady, K.T. Integrated Treatment of PTSD and Addiction in Veterans Using Prolonged Exposure. In Presented at the Annual Convention of the International Society for Traumatic Stress Studies, Dallas, TX, USA, 10–12 November 2016.
- Baker, T.B.; Piper, M.E.; McCarthy, D.E.; Majeskie, M.R.; Fiore, M.C. Addiction motivation reformulated: An affective processing model of negative reinforcement. Psychol. Rev. 2004, 111, 33–51. [Google Scholar] [CrossRef] [PubMed]
- Conger, J.J. Reinforcement theory and the dynamics of alcoholism. Q. J. Stud. Alcohol 1956, 17, 296–305. [Google Scholar] [PubMed]
- Koob, G.F.; Le Moal, M. Drug addiction, dysregulation of reward, and allostasis. Neuropsychopharmacology 2001, 24, 97–129. [Google Scholar] [CrossRef]
- Bonn-Miller, M.O.; Vujanovic, A.A.; Feldner, M.T.; Bernstein, A.; Zvolensky, M.J. Posttraumatic stress symptom severity predicts marijuana use coping motives among traumatic event-exposed marijuana users. J. Trauma. Stress 2007, 20, 577–586. [Google Scholar] [CrossRef] [PubMed]
- Lehavot, K.; Stappenbeck, C.A.; Luterek, J.A.; Kaysen, D.; Simpson, T.L. Gender differences in relationships among PTSD severity, drinking motives, and alcohol use in a comorbid alcohol dependence and PTSD sample. Psychol. Addict. Behav. 2014, 28, 42–52. [Google Scholar] [CrossRef] [PubMed]
- Van Minnen, A.; Zoellner, L.A.; Harned, M.S.; Mills, K. Changes in comorbid conditions after prolonged exposure for PTSD: A literature review. Curr. Psychiatry Rep. 2015, 17, 549. [Google Scholar] [CrossRef] [PubMed]
- Back, S.E.; Foa, E.B.; Killeen, T.K.; Teesson, M.; Mills, K.L.; Cotton, B.D.; Brady, K.T. Concurrent Treatment of PTSD and Substance Use Disorders Using Prolonged Exposure (COPE): Therapist Guide; Oxford University Press: New York, NY, USA, 2014. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 2002. [Google Scholar]
- Carroll, K.M. A Cognitive-Behavioral Approach: Treating Cociane Addiction; National Institute on Drug Abuse: Rockville, MD, USA, 1998.
- Blake, D.D.; Weathers, F.W.; Nagy, L.M.; Kaloupek, D.G.; Gusman, F.D.; Charney, D.S.; Keane, T.M. The development of a clinician-administered PTSD scale. J. Trauma. Stress 1995, 8, 75–90. [Google Scholar] [CrossRef] [PubMed]
- Weathers, F.W.; Litz, B.T.; Herman, D.S.; Huska, J.A.; Keane, T.M. The PTSD checklist: Reliability, validity, & diagnostic utility. In Presented at the Annual Meeting of the International Society for Traumatic Stress Studies, San Antonio, TX, USA, 25 October 1993.
- Sheehan, D.V.; Lecrubier, Y.; Harnett-Sheehan, K.; Amorim, P.; Janavs, J.; Weiller, E.; Hergueta, T.; Baker, R.; Dunbar, G. The M.I.N.I. International Neuropsychiatric Interview (M.I.N.I.): The Development and Validation of a Structured Diagnostic Psychiatric Interview. J. Clin. Psychiatry 1998, 59, 22–33. [Google Scholar] [PubMed]
- Sobell, L.C.; Sobell, M.B. Timeline Follow-Back: A technique for assessing self-reported ethanol Consumption. In Measuring Alcohol Consumption: Psychosocial and Biological Methods; Allen, J., Litten, R.Z., Eds.; Human Press: Totowa, NJ, USA, 2002. [Google Scholar]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for Beck Depression Inventory, 2nd ed.; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Dozois, D.J.A.; Dobson, K.S.; Ahnberg, J.L. A psychometric evaluation of the Beck Depression Inventory-II. Psychol. Assess. 1998, 10, 83–89. [Google Scholar] [CrossRef]
- Steer, R.A.; Clark, D.A. Psychometric characteristics of the Beck Depression Inventory-II with college students. Measurement Eval. Couns. Dev. 1997, 30, 128–136. [Google Scholar]
- Muthen, L.K.; Muthen, B.O. Mplus (Version 7) (Computer Software), Muthen & Muthen: Los Angleas, CA, USA, 1998–2011.
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance strucutre analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Foa, E.B.; Hembree, E.A.; Rothbaum, B.O. Prolonged Exposure Therapy for PTSD: Emotional Processing of Traumatic Experiences: Therapist Guide; Oxford University Press: New York, NY, USA, 2007. [Google Scholar]
- Foa, E.B.; Hembree, E.A.; Cahill, S.P.; Rauch, S.A.M.; Riggs, D.S.; Feeny, N.C.; Yadin, E. Randomized trial of prolonged exposure for posttraumatic stress disorder with and without cognitive restructuring: Outcome at academic and community clinics. J. Consult. Clin. Psychol. 2005, 73, 953–964. [Google Scholar] [CrossRef] [PubMed]
- Nacasch, N.; Foa, E.B.; Huppert, J.D.; Tzur, D.; Fostick, L.; Dinstein, Y.; Polliack, M.; Zohar, J. Prolonged exposure therapy for combat- and terror-related posttraumatic stress disorder: A randomized control comparison with treatment as usual. J. Clin. Psychiatry 2011, 72, 1174–1180. [Google Scholar] [CrossRef] [PubMed]
- Kraemer, H.C.; Wilson, T.G.; Fairburn, C.G.; Agras, S.W. Mediators and Moderators of Treatment Effects in Randomized Clinical Trials. Arch. Gen. Psychiatry 2002, 59, 877–883. [Google Scholar] [CrossRef] [PubMed]
- Slade, T.; Watson, D. The structure of common DSM-IV and ICD-10 mental disorders in the Australian general population. Psychol. Med. 2006, 36, 1593–1600. [Google Scholar] [CrossRef] [PubMed]
- Brady, K.T.; Back, S.E.; Coffey, S. Substance Abuse and Posttraumatic Stress Disorder. Curr. Dir. Psychol. Sci. 2004, 13, 206–209. [Google Scholar] [CrossRef]

{kind=link}
| Variable | COPE | RP | Total |
|---|---|---|---|
| (n = 54) | (n = 27) | (n = 81) | |
| M (SD) or % | M (SD) or % | M (SD) or % | |
| Age (Years) | 39.7 (10.9) | 41.9 (10.3) | 40.4 (10.7) |
| Gender (Male) | 92.6% | 85.20% | 90.1% |
| Race (Caucasian) | 68.50% | 44.40% | 60.5% |
| Race (African American) | 29.60% | 51.90% | 37.0% |
| BDI | |||
| Baseline BDI | 29.2 (12.3) | 29.6 (9.7) | 29.3 (11.5) |
| Session 6 BDI | 19.5 (11.7) | 26.2 (13.7) | 21.3 (12.5) |
| Session 12 BDI | 13.0 (11.0) | 19.4 (12.3) | 15.02 (11.7) |
| PCL | |||
| Baseline PCL | 62.2 (11.1) | 64.3 (8.9) | 62.9 (10.4) |
| Session 6 PCL | 45.5 (15.6) | 58.0 (18.5) | 48.9 (17.2) |
| TLFB | |||
| Baseline TLFB | 0.47 (0.36) | 0.50 (0.34) | 0.48 (0.35) |
| Session 6 TLFB | 0.21 (0.26) | 0.29 (0.30) | 0.23 (0.27) |
| Predictor | Session 6 PTSD Symptoms | Session 6 Substance Use | Session 12 Depressive Symptoms | |||
|---|---|---|---|---|---|---|
| B | SE | B | SE | B | SE | |
| Age | 0.370 ** | 0.103 | −0.220 | 0.114 | ||
| Gender | −0.046 | 0.109 | 0.054 | 0.118 | ||
| Race | −0.208 * | 0.089 | −0.027 | 0.097 | ||
| Treatment Group | 0.236 * | 0.112 | 0.136 | 0.122 | −0.072 | 0.123 |
| Baseline PTSD Symptoms | 0.405 ** | 0.126 | -0.052 | 0.141 | ||
| Baseline Substance Use | −0.056 | 0.109 | 0.477 ** | 0.104 | ||
| Session 1 Depressive Symptoms | 0.118 | 0.120 | 0.019 | 0.131 | ||
| Session 6 PTSD Symptoms | -- | -- | -- | -- | 0.700 *** | 0.091 |
| Session 6 Substance Use | -- | -- | 0.096 | 0.122 | ||
© 2017 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korte, K.J.; Bountress, K.E.; Tomko, R.L.; Killeen, T.; Moran-Santa Maria, M.; Back, S.E. Integrated Treatment of PTSD and Substance Use Disorders: The Mediating Role of PTSD Improvement in the Reduction of Depression. J. Clin. Med. 2017, 6, 9. https://doi.org/10.3390/jcm6010009
Korte KJ, Bountress KE, Tomko RL, Killeen T, Moran-Santa Maria M, Back SE. Integrated Treatment of PTSD and Substance Use Disorders: The Mediating Role of PTSD Improvement in the Reduction of Depression. Journal of Clinical Medicine. 2017; 6(1):9. https://doi.org/10.3390/jcm6010009
Chicago/Turabian StyleKorte, Kristina J., Kaitlin E. Bountress, Rachel L. Tomko, Therese Killeen, Megan Moran-Santa Maria, and Sudie E. Back. 2017. "Integrated Treatment of PTSD and Substance Use Disorders: The Mediating Role of PTSD Improvement in the Reduction of Depression" Journal of Clinical Medicine 6, no. 1: 9. https://doi.org/10.3390/jcm6010009
APA StyleKorte, K. J., Bountress, K. E., Tomko, R. L., Killeen, T., Moran-Santa Maria, M., & Back, S. E. (2017). Integrated Treatment of PTSD and Substance Use Disorders: The Mediating Role of PTSD Improvement in the Reduction of Depression. Journal of Clinical Medicine, 6(1), 9. https://doi.org/10.3390/jcm6010009