
A Shared Decision-Making Approach to Telemedicine: Engaging Rural Patients in Glycemic Management

Abstract
:1. Introduction
2. Methods
2.1. Recruitment and Setting
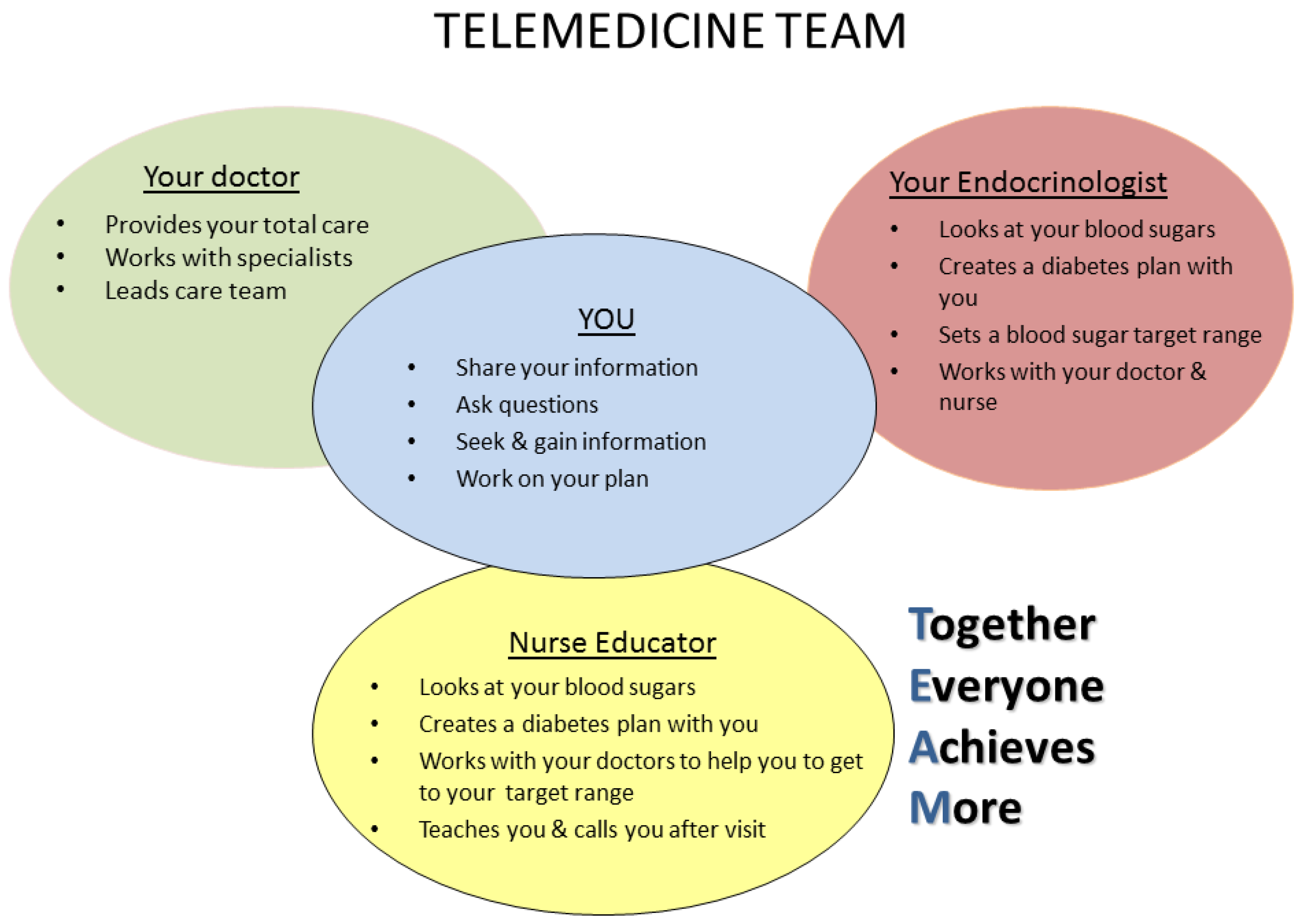
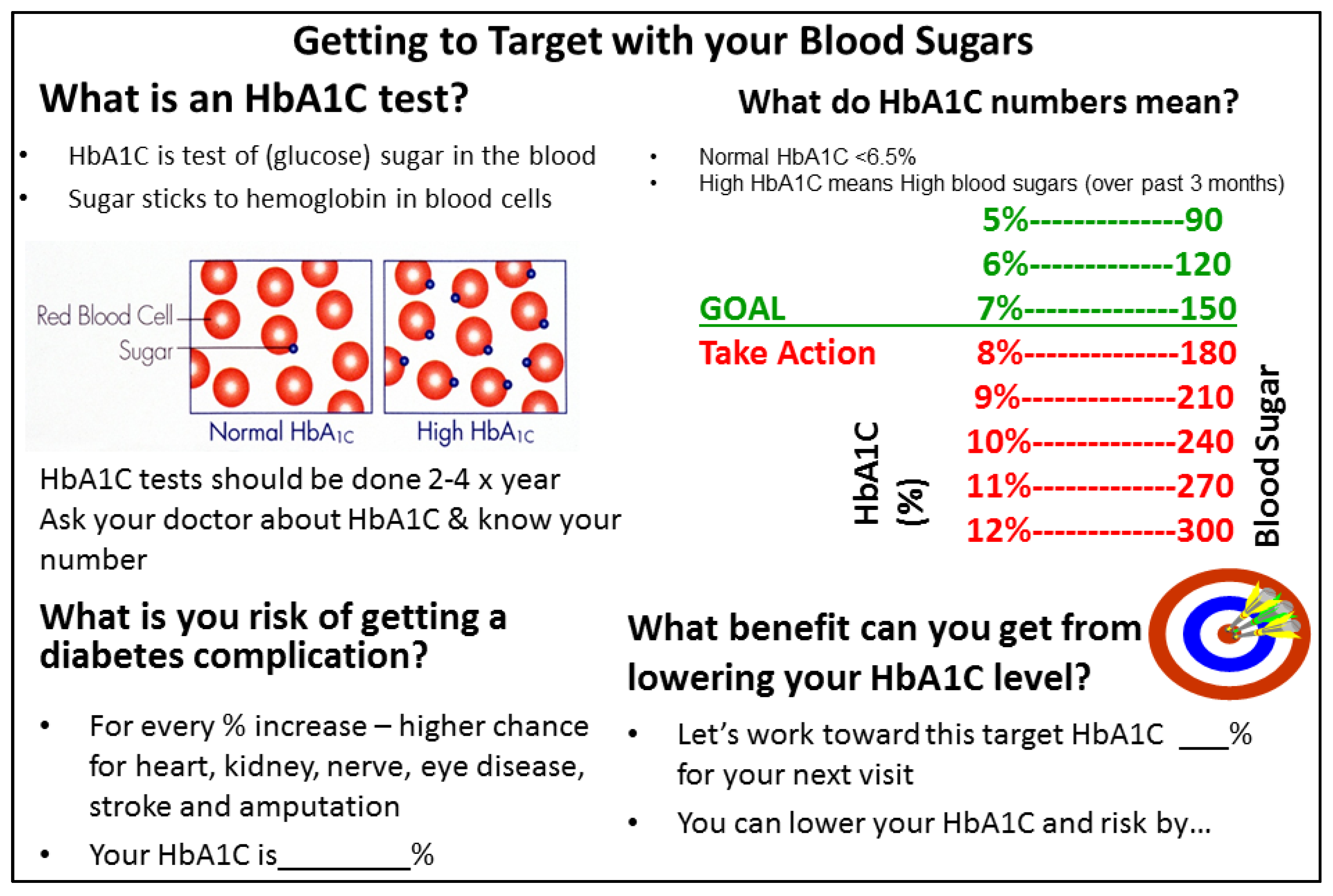
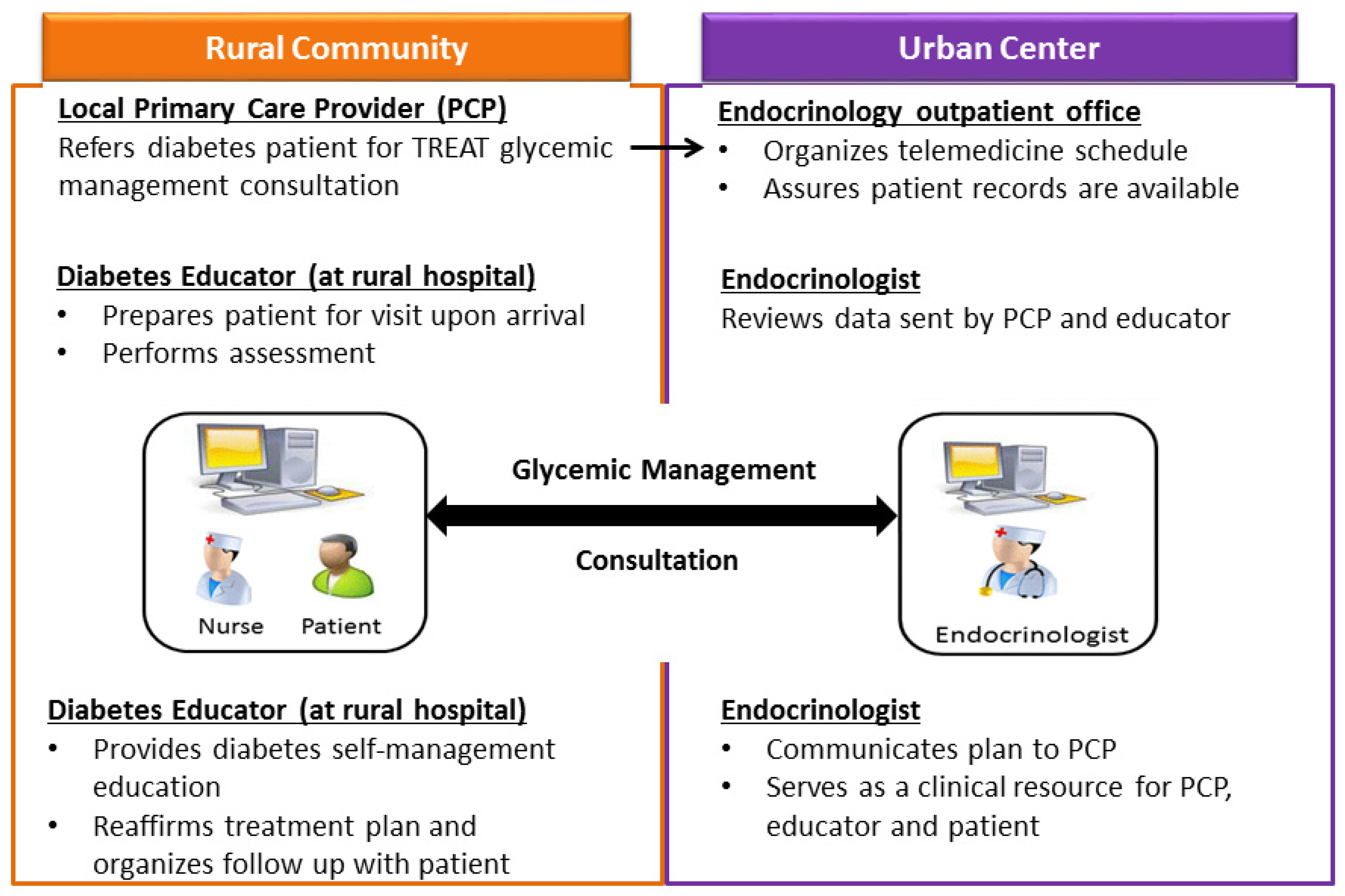
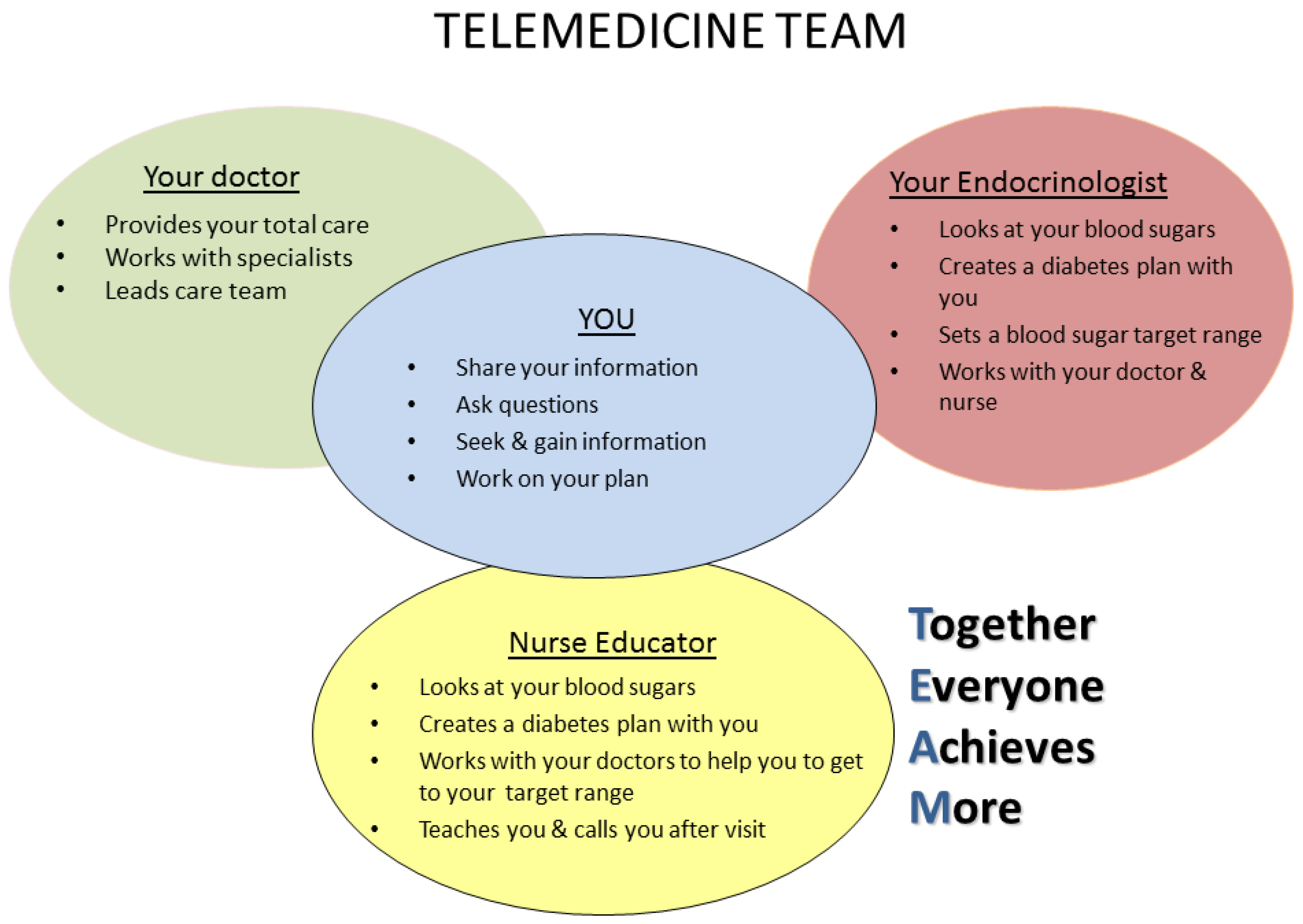
2.2. Intervention
2.3. Evaluation
2.4. Data Analysis
3. Results
3.1. Goal Setting
3.2. Diabetes Outcomes
3.3. Provider and Patient Feedback
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Lutfiyya, M.; Patel, Y.; Steele, J.; Tetteh, B.; Chang, L.; Aguero, C.; Lipsky, M.S. Are there disparities in diabetes care? A comparison of care received by US rural and non-rural adults with diabetes. Prim. Health Care Res. Dev. 2009, 10, 320–331. [Google Scholar] [CrossRef]
- Ciemens, E.; Coon, P.; Peck, R.; Holloway, B.; Min, S. Using telehealth to provide diabetes care to patients in rural Montana: Findings from the promoting realistic individual self-management program. Telemed. e-Health 2011, 17, 596–602. [Google Scholar] [CrossRef] [PubMed]
- Nyenwe, E.; Ashby, S.; Tidwell, J.; Nourer, S.; Kitachbi, A. Improving Diabetes Care via Telemedicine: Lessons From the Addressing Diabetes in Tennessee (ADT) Project. Diabetes Care 2011, 34, e34. [Google Scholar] [CrossRef] [PubMed]
- Schreiner, A.; Simpson, K. Primary care and chronic disease: The intersection of comfort and specialty involvement—A cross-sectional study. J. Eval. Clin. Pract. 2016. [Google Scholar] [CrossRef] [PubMed]
- Janes, G.R. Ambulatory Medical Care for Diabetes: Diabetes in America; Publication No. 95-1468; National Institutes of Health, US Department of Health and Human Services: Bethesda, MD, USA, 1995.
- Saudek, C. The role of primary care professionals in managing diabetes. Clin. Diabetes 2002, 20, 65–66. [Google Scholar] [CrossRef]
- Anderson, R.M.; Fitzgerald, J.T.; Gorenflo, D.W.; Oh, M.S. A comparison of the diabetes-related attitudes of health care professionals and patients. Patient Educ. Couns. 1993, 21, 41–50. [Google Scholar] [CrossRef]
- Woodwell, D.A.; Cherry, D.K. National Ambulatory Medical Care Survey: 2002 Summary. Adv. Data 2004, 26, 1–44. [Google Scholar]
- Khunti, K.; Davies, M. Glycaemic goals in patients with type 2 diabetes: Current status, challenges and recent advances. Diabetes Obes. Metab. 2010, 12, 474–484. [Google Scholar] [CrossRef] [PubMed]
- Fisher, L.; Mullan, J.T.; Arean, P.; Glasgow, R.E.; Hessler, D.; Masharani, U. Diabetes distress but not clinical depression or depressive symptoms is associated with glycemic control in both cross-sectional and longitudinal analyses. Diabetes Care 2010, 33, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Fisher, L.; Mullan, J.T.; Skaff, M.M.; Glasgow, R.E.; Arean, P.; Hessler, D. Predicting diabetes distress in patients with Type 2 diabetes: A longitudinal study. Diabetes Med. 2009, 26, 622–627. [Google Scholar] [CrossRef] [PubMed]
- Fisher, L.; Skaff, M.M.; Mullan, J.T.; Arean, P.; Glasgow, R.; Masharani, U. A longitudinal study of affective and anxiety disorders, depressive affect and diabetes distress in adults with Type 2 diabetes. Diabetes Med. 2008, 25, 1096–101. [Google Scholar] [CrossRef] [PubMed]
- Charles, C.; Gafni, A.; Whelan, T. Decision-making in the physician-patient encounter: Revisiting the shared treatment decision-making model. Soc. Sci. Med. 1999, 49, 651–661. [Google Scholar] [CrossRef]
- Montori, V.; Gafni, A.; Charles, C. A shared treatment decision-making approach between patients with chronic conditions and their clinicians: The case of diabetes. Health Expect. 2006, 9, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.; Emanuel, E. Shared decision making to improve care and reduce costs. N. Engl. J. Med. 2013, 368, 6–8. [Google Scholar]
- Siminerio, L.M.; Piatt, G.; Zgibor, J.C. Implementing the chronic care model for improvements in diabetes care and education in a rural primary care practice. Diabetes Educ. 2005, 31, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Toledo, F.; Triola, A.; Ruppert, K.; Siminerio, L. Telemedicine consultations: An alternative model to increase access to diabetes specialist care in underserved rural communities. JMIR Res. Protoc. 2012, 1, e14. [Google Scholar] [CrossRef] [PubMed]
- Toledo, F.; Ruppert, K.; Huber, K.A.; Siminerio, L. Efficacy of the Telemedicine for Reach, Treatment, and Access Model (TREAT) Model for Diabetes Care. Diabetes Care 2014, 37, e179–e180. [Google Scholar] [CrossRef] [PubMed]
- Siminerio, L.; Ruppert, K.; Hubert, K.; Toledo, F.G.S. Telemedicine for Reach, Treatment, and Access Model (TREAT): Linking Telemedicine with Diabetes Self-management Education to Improve Care in Rural Communities. Diabetes Educ. 2014, 40, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Toobert, D.; Hampson, S.; Glasgow, R. The summary of diabetes self-care activities measure: Results from 7 studies and a revised scale. Diabetes Care 2000, 23, 943–950. [Google Scholar] [CrossRef] [PubMed]
- Peek, M.; Harmon, S.; Scott, S.; Eder, M.; Roberson, T.; Tang, H.; Chin, M. Culturally tailoring patient education and communication skills training to empower African-Americans with diabetes. Transl. Behav. Med. 2012, 2, 296–308. [Google Scholar] [CrossRef] [PubMed]
- Shay, L.A.; Lafata, J.E. Where is the evidence? A systematic review of shared decision making and patient outcomes. Med. Decis. Mak. 2015, 35, 114–131. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Initial HbA1c Goal | Detailed Behavioral Goal |
|---|---|
| HbA1c < 7% by making healthy food choices | Increase healthy food choices and limit carbohydrates with meals; limit sweets to once a week. |
| Lower HbA1c to 7.5% | Cut down on snacks at bedtime. |
| Lower HbA1c by 1 point to 7.5% by eating healthy and monitoring blood sugar | Follow Weight Watchers; check blood sugar more routinely. |
| Before Initial Telemedicine Visit | ~6 Months Post Visit | p-Value | |
|---|---|---|---|
| HbA1c (% ± standard deviation) | 10.1 ± 1.4 | 8.6 ± 1.2 | <0.05 |
| Diabetes Self-Care Measures (days/week) a | |||
| Adhere to general diet | 4.6 ± 1.9 | 4.4 ± 1.2 | ns |
| Consume 5+ servings fruit & vegetables | 4.3 ± 2.1 | 4.2 ± 1.9 | ns |
| Consume high fat foods | 4.4 ± 2.4 | 2.7 ± 1.7 | <0.05 |
| Monitor blood glucose | 5.3 ± 2.3 | 6 ± 1.4 | ns |
| Adhere to insulin or oral medications | 7 | 6.4 ± 2.1 | ns |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Griffith, M.L.; Siminerio, L.; Payne, T.; Krall, J. A Shared Decision-Making Approach to Telemedicine: Engaging Rural Patients in Glycemic Management. J. Clin. Med. 2016, 5, 103. https://doi.org/10.3390/jcm5110103
Griffith ML, Siminerio L, Payne T, Krall J. A Shared Decision-Making Approach to Telemedicine: Engaging Rural Patients in Glycemic Management. Journal of Clinical Medicine. 2016; 5(11):103. https://doi.org/10.3390/jcm5110103
Chicago/Turabian StyleGriffith, Michelle L., Linda Siminerio, Tammie Payne, and Jodi Krall. 2016. "A Shared Decision-Making Approach to Telemedicine: Engaging Rural Patients in Glycemic Management" Journal of Clinical Medicine 5, no. 11: 103. https://doi.org/10.3390/jcm5110103
APA StyleGriffith, M. L., Siminerio, L., Payne, T., & Krall, J. (2016). A Shared Decision-Making Approach to Telemedicine: Engaging Rural Patients in Glycemic Management. Journal of Clinical Medicine, 5(11), 103. https://doi.org/10.3390/jcm5110103