
Diagnosis of Atopic Dermatitis: Mimics, Overlaps, and Complications

Abstract
:1. AD Diagnosis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
 |
| Diagnosis | Relative Prevalence | |||
|---|---|---|---|---|
| Infants | Children | Adolescents/Adults | ||
| Inflammatory Skin Conditions (See Section 2) | seborrheic dermatitis | common | uncommon | common |
| psoriasis | less common | less common | common | |
| nummular dermatitis | less common | common | less common | |
| contact dermatitis a | common | common | common | |
| dermatographism a | less common | common | common | |
| pityriasis alba a | common | common | uncommon | |
| overlap (see Section 2.7) | common | common | common | |
| Infections (See Section 3) | impetigo a | common | common | less common |
| secondary syphilis | rare | rare | rare | |
| molluscum dermatitis a | common | common | less common | |
| eczema herpeticum a | uncommon | uncommon | rare | |
| eczema vaccinatum a | rare | rare | rare | |
| eczema coxsackium a | emerging | emerging | rare | |
| viral exanthem | common | common | less common | |
| tinea (as AD mimic) | uncommon | uncommon | uncommon | |
| candidiasis | common | less common | less common | |
| Infestations (See Section 4) | scabies (prevalence varies by region) | may be common | may be common | may be common |
| Genetic Disorders (See Section 6) | keratosis pilaris | less common | common | not common |
| ichthyosis vulgaris a | common | common | common | |
| Immunodeficiency Disorders (See Section 7) | HIV/AIDS-related skin changes (prevalence varies by region) | less common | less common | may be common |
| Other (See Section 9) | drug eruptions | less common | common | common |
| Infants | Children | Adolescents/Adults | |
|---|---|---|---|
| Malignancies (See Section 5) | ● Letterer-Siwe Disease | ● Letterer-Siwe Disease | ● Letterer-Siwe Disease |
| ● cutaneous T-cell lymphoma | ● cutaneous T-cell lymphoma | ● cutaneous T-cell lymphoma | |
| Genetic Disorders (See Section 6) | ● X-linked recessive ichthyosis (males only) | ● X-linked recessive ichthyosis (males only) | ● X-linked recessive ichthyosis (males only) |
| ● lamellar ichthyosis | ● lamellar ichthyosis | ||
| ● nonbullous ichthyosiform erythroderma | ● nonbullous ichthyosiform erythroderma | ● nonbullous ichthyosiform erythroderma | |
| Immunodeficiency Disorders (See Section 7) | ● Netherton syndrome | ● IgA deficiency ● IgM deficienc | ● IgA deficiency |
| ● STAT3 deficiency | |||
| ● DOCK8 deficiency | |||
| ● Wiskott-Aldrich syndrome (males only) | |||
| ● Leiner Phenotype | |||
| ○ severe combined immunodeficiency | |||
| ○ Omenn syndrome | ● IgM deficiency | ||
| ● hypohidrotic ectodermal dysplasia/NEMO | |||
| ● autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy (APECED) | |||
| Nutritional Disorders (See Section 8) | ● cystic fibrosis | ● | ● dermatitis herpetiformis |
| ● phenylketonuria | |||
| ● zinc deficiency | |||
| ● biotin deficiency | |||
| Other (See Section 9) | ● maternal-fetal graft-versus-host disease | ● graft-versus-host disease | ● graft-versus-host disease |
2. Inflammatory Skin Conditions
2.1. Seborrheic Dermatitis

2.2. Psoriasis

2.3. Nummular Dermatitis
2.4. Contact Dermatitis
2.5. Dermatographism


2.6. Pityriasis Alba

2.7. Overlap

3. Infections
3.1. Bacterial Infections
3.1.1. Impetigo

3.1.2. Secondary Syphilis


3.2. Viral Infections
3.2.1. Molluscum Dermatitis

3.2.2. Eczema Herpeticum

3.2.3. Eczema Vaccinatum
3.2.4. Eczema Coxsackium

3.2.5. Viral Exanthem

3.3. Fungal Infections
3.3.1. Tinea



3.3.2. Candidiasis

4. Infestations
4.1. Scabies


5. Malignancies
5.1. Letterer-Siwe Disease
5.2. Cutaneous T-Cell Lymphoma
6. Genetic Disorders
6.1. Keratosis Pilaris

6.2. Ichthyoses
6.2.1. Ichthyosis Vulgaris

6.2.2. Other Ichthyoses
7. Immunodeficiency Disorders
7.1. Netherton Syndrome
7.2. HIV/AIDS-Related Skin Changes
7.3. Other Immunodeficiency Disorders
8. Nutritional Disorders

8.1. Cystic Fibrosis
8.2. Phenylketonuria
8.3. Zinc Deficiency and Biotin Deficiency
8.4. Food Allergy
Dermatitis Herpetiformis
9. Other Differential Diagnoses
9.1. Graft-versus-Host Disease
9.2. Drug Eruptions

10. Distinguishing Features
11. Conclusions
| History | Signs/Symptoms | Distribution | Other Distinguishing/Diagnostic Features | ||||
|---|---|---|---|---|---|---|---|
| Infantile Onset | Associated with AD | Pruritus/Excoriations | Xerosis | Well Circumscribed Lesions | |||
| Atopic Dermatitis | ✓++ | – | ✓++ | ✓++ | infants: face, trunk, extensor extremities | chronic with intermittent flares | |
| children: flexors | |||||||
| adults: hands | |||||||
| all ages: spares “diaper area”/groin, axilla | |||||||
| Seborrheic Dermatitis a | ✓++ | ✓ | scalp, face, skin folds | coarse, greasy, yellow scale | |||
| Psoriasis a | ✓ | ✓ | ✓++ | extensors, scalp, “diaper area”; “Köebnerizes” | thick, silvery-white scaling | ||
| Nummular Dermatitis a | ✓ | ✓ | ✓+ | ✓++ | extremities | very TCS-responsive | |
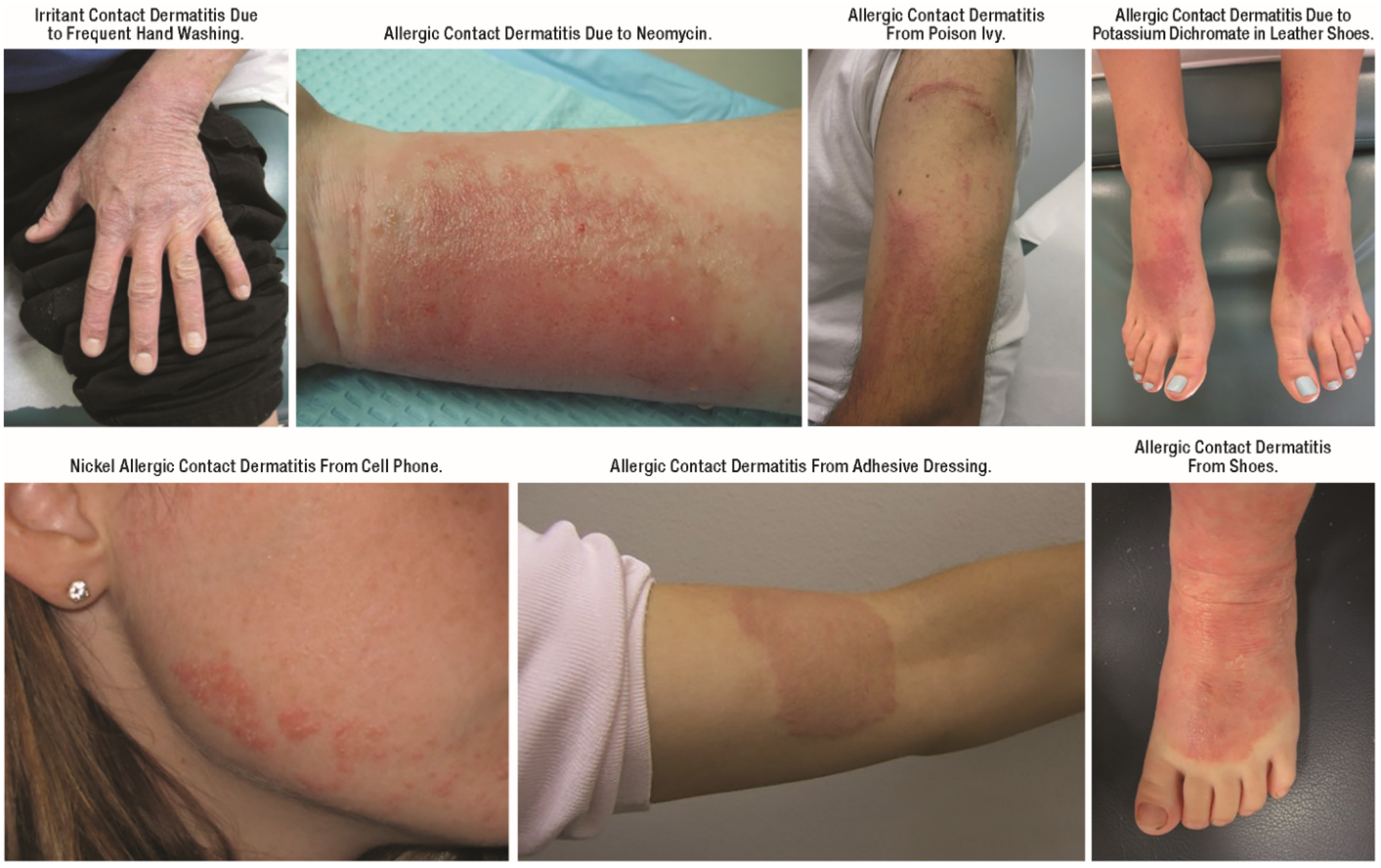
| Irritant Contact Dermatitis | ✓ | ✓+ | ✓+ | ✓+ | ✓+ | geographic, often asymmetric | history of irritant exposure |
| Allergic Contact Dermatitis a | ✓ | ✓++ | ✓ | ✓+ | often bilaterally symmetric | history of allergen exposure | |
| Dermatographism | ✓+ | ✓++ | ✓+ | “Köebnerizes” | clinical response to mechanical stimulation | ||
| Pityriasis Alba | ✓+ | ✓+ | ✓+ | face, trunk, extremities | poorly circumscribed, hypopigmented lesions; nonpruritic | ||
| Impetigo | ✓+ | ✓ | ✓+ | face, trunk, extremities | honey-colored crust, tenderness | ||
| Secondary Syphilis | ✓+ | ✓+ | trunk, extremities | mucous membrane and palmoplantar involvement | |||
| Molluscum Dermatitis | ✓+ | ✓+ | ✓+ | ✓+ | face, trunk, extremities | frequently localized; umbilicated papules (often subtle) | |
| Eczema Herpeticum/Vaccinatum | ✓+ | ✓+ | ✓+ | ✓+ | face, AD-affected areas | “punched out” lesions | |
| Eczema Coxsackium | ✓+ | ✓+ | ✓+ | ✓+ | AD-affected areas | acute onset, fever, subsequent onychomadesis | |
| Viral Exanthem | ✓++ | ✓ | ✓ | face, trunk extremities | acute onset, associated constitutional symptoms | ||
| Tinea | ✓ | ✓ | ✓++ | scalp, face, trunk, extremities | trailing edge scale, lymphadenopathy, hair loss | ||
| Candidiasis | ✓++ | ✓ | ✓ | ✓ | skin folds, genitalia | paronychia and/or thrush | |
| Scabies | ✓+ | ✓++ | ✓ | infants: palms, soles, face, scalp adults: finger webs, wrists, periareolar, genitals | visible burrows, palmoplantar pustules | ||
| Letterer-Siwe Disease | ✓++ | ✓ | skin fold and scalp accentuation | telangiectatic, hepatosplenomegaly | |||
| Early-Stage CTCL | ✓ | trunk, extremities | symptoms accompanied by weight loss or malaise | ||||
| Keratosis Pilaris | ✓ | ✓+ | ✓ | ✓+ | cheeks, extensor extremities | follicular keratotic papules, underlying macular erythema | |
| Ichthyosis Vulgaris | ✓+ | ✓+ | ✓ | ✓++ | spares popliteal and antecubital fossae | plate-like scale, palmoplantar hyperlinearity, non-responsive to CS | |
| XLRI (males only) | ✓++ | ✓ | ✓++ | extensor surfaces, neck, face, trunk, buttocks | grey adherent scale | ||
| ARCI | ✓++ | ✓ | ✓++ | face, trunk, extremities | “collodion baby” | ||
| Immunodeficiency Disorders | ✓++ | ✓ | Δ | Δ | variable | laboratory confirmation | |
| Nutritional Disorders | ✓ | ✓ | Δ | ✓ | variable | laboratory confirmation | |
| Acute Graft-versus-Host Disease | ✓ | ✓++ | face, trunk, extremities | oral mucous membrane/palmar involvement | |||
| Drug Eruptions | ✓ | ✓ | ✓ | face, trunk, extremities | clinico-pathological correlations | ||
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Shaw, T.E.; Currie, G.P.; Koudelka, C.W.; Simpson, E.L. Eczema prevalence in the United States: Data from the 2003 National Survey of Children’s Health. J. Investig. Dermatol. 2011, 131, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Mempel, M.; Schober, W.; Behrendt, H.; Ring, J. Gender difference, sex hormones, and immediate type hypersensitivity reactions. Allergy 2008, 63, 1418–1427. [Google Scholar] [CrossRef] [PubMed]
- Eichenfield, L.F.; Hanifin, J.M.; Luger, T.A.; Stevens, S.R.; Pride, H.B. Consensus conference on pediatric atopic dermatitis. J. Am. Acad. Dermatol. 2003, 49, 1088–1095. [Google Scholar] [CrossRef] [PubMed]
- Eichenfield, L.F.; Tom, W.L.; Berger, T.G.; Krol, A.; Paller, A.S.; Schwarzenberger, K.; Bergman, J.N.; Chamlin, S.L.; Cohen, D.E.; Cooper, K.D.; et al. Guidelines of care for the management of atopic dermatitis: Section 2. Management and treatment of atopic dermatitis with topical therapies. J. Am. Acad. Dermatol. 2014, 71, 116–132. [Google Scholar] [CrossRef]
- Sidbury, R.; Tom, W.L.; Bergman, J.N.; Cooper, K.D.; Silverman, R.A.; Berger, T.G.; Chamlin, S.L.; Cohen, D.E.; Cordoro, K.M.; Davis, D.M.; et al. Guidelines of care for the management of atopic dermatitis: Section 4. Prevention of disease flares and use of adjunctive therapies and approaches. J. Am. Acad. Dermatol. 2014, 71, 1218–1233. [Google Scholar] [CrossRef]
- Alexopoulos, A.; Kakourou, T.; Orfanou, I.; Xaidara, A.; Chrousos, G. Retrospective analysis of the relationship between infantile seborrheic dermatitis and atopic dermatitis. Pediatr. Dermatol. 2014, 31, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Sampaio, A.L.; Mameri, A.C.; Vargas, T.J.; Ramos-e-Silva, M.; Nunes, A.P.; Carneiro, S.C. Seborrheic dermatitis. An. Bras. Dermatol. 2011, 86, 1061–1071. [Google Scholar] [CrossRef] [PubMed]
- Apasrawirote, W.; Udompataikul, M.; Rattanamongkolgul, S. Topical antifungal agents for seborrheic dermatitis: Systematic review and meta-analysis. J. Med. Assoc. Thail. 2011, 94, 756–760. [Google Scholar]
- Kastarinen, H.; Oksanen, T.; Okokon, E.O.; Kiviniemi, V.V.; Airola, K.; Jyrkka, J.; Oravilahti, T.; Rannanheimo, P.K.; Verbeek, J.H. Topical anti-inflammatory agents for seborrhoeic dermatitis of the face or scalp. Cochrane Database Syst. Rev. 2014, 5. [Google Scholar] [CrossRef] [PubMed]
- Augustin, M.; Reich, K.; Glaeske, G.; Schaefer, I.; Radtke, M. Co-morbidity and age-related prevalence of psoriasis: Analysis of health insurance data in Germany. Acta Derm. Venereol. 2010, 90, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Guttman-Yassky, E.; Nograles, K.E.; Krueger, J.G. Contrasting pathogenesis of atopic dermatitis and psoriasis—Part I: Clinical and pathologic concepts. J. Allergy Clin. Immunol. 2011, 127, 1110–1118. [Google Scholar] [CrossRef] [PubMed]
- Wilsmann-Theis, D.; Hagemann, T.; Jordan, J.; Bieber, T.; Novak, N. Facing psoriasis and atopic dermatitis: Are there more similarities or more differences? Eur. J. Dermatol. 2008, 18, 172–180. [Google Scholar] [PubMed]
- Scott, L.J.; Dunn, C.J.; Goa, K.L. Calcipotriol ointment. A review of its use in the management of psoriasis. Am. J. Clin. Dermatol. 2001, 2, 95–120. [Google Scholar] [CrossRef] [PubMed]
- Hendriks, A.G.; Keijsers, R.R.; de Jong, E.M.; Seyger, M.M.; van de Kerkhof, P.C. Combinations of classical time-honoured topicals in plaque psoriasis: A systematic review. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 399–410. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Lin, A. Efficacy of topical calcineurin inhibitors in psoriasis. J. Cutan. Med. Surg. 2014, 18, 8–14. [Google Scholar] [PubMed]
- Krol, A.; Krafchik, B. The differential diagnosis of atopic dermatitis in childhood. Dermatol. Ther. 2006, 19, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Fonacier, L.S.; Aquino, M.R. The role of contact allergy in atopic dermatitis. Immunol. Allergy Clin. N. Am. 2010, 30, 337–350. [Google Scholar] [CrossRef]
- Spiewak, R. Contact dermatitis in atopic individuals. Curr. Opin. Allergy Clin. Immunol. 2012, 12, 491–497. [Google Scholar] [CrossRef] [PubMed]
- De Waard-van der Spek, F.B.; Andersen, K.E.; Darsow, U.; Mortz, C.G.; Orton, D.; Worm, M.; Muraro, A.; Schmid-Grendelmeier, P.; Grimalt, R.; Spiewak, R.; et al. Allergic contact dermatitis in children: Which factors are relevant? (review of the literature). Pediatr. Allergy Immunol. 2013, 24, 321–329. [Google Scholar] [CrossRef]
- Aquino, M.; Fonacier, L. The role of contact dermatitis in patients with atopic dermatitis. J. Allergy Clin. Immunol. Pract. 2014, 2, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Bruckner, A.L.; Weston, W.L. Allergic contact dermatitis in children: A practical approach to management. Skin Ther. Lett. 2002, 7, 3–5. [Google Scholar]
- Pigatto, P.; Martelli, A.; Marsili, C.; Fiocchi, A. Contact dermatitis in children. Ital. J. Pediatr. 2010, 36, 2. [Google Scholar] [CrossRef] [PubMed]
- Seyfarth, F.; Schliemann, S.; Antonov, D.; Elsner, P. Dry skin, barrier function, and irritant contact dermatitis in the elderly. Clin. Dermatol. 2011, 29, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Simonsen, A.B.; Deleuran, M.; Johansen, J.D.; Sommerlund, M. Contact allergy and allergic contact dermatitis in children—A review of current data. Contact Dermatitis 2011, 65, 254–265. [Google Scholar] [CrossRef] [PubMed]
- Ramsing, D.W.; Agner, T. Efficacy of topical corticosteroids on irritant skin reactions. Contact Dermatitis 1995, 32, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Levin, C.; Maibach, H.I. An overview of the efficacy of topical corticosteroids in experimental human nickel contact dermatitis. Contact Dermatitis 2000, 43, 317–321. [Google Scholar] [CrossRef] [PubMed]
- Anderson, B.E.; Marks, J.G., Jr.; Mauger, D.T. Efficacy of tacrolimus ointment in the prevention and treatment of contact dermatitis. Dermatitis 2004, 15, 158–159. [Google Scholar] [CrossRef] [PubMed]
- Day, I.; Lin, A.N. Use of pimecrolimus cream in disorders other than atopic dermatitis. J. Cutan. Med. Surg. 2008, 12, 17–26. [Google Scholar] [PubMed]
- Fonacier, L.S.; Aquino, M.R.; Mucci, T. Current strategies in treating severe contact dermatitis in pediatric patients. Curr. Allergy Asthma Rep. 2012, 12, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Mecoli, C.A.; Morgan, A.J.; Schwartz, R.A. Symptomatic dermatographism: Current concepts in clinical practice with an emphasis on the pediatric population. Cutis 2011, 87, 221–225. [Google Scholar] [PubMed]
- Lin, R.L.; Janniger, C.K. Pityriasis alba. Cutis 2005, 76, 21–24. [Google Scholar] [PubMed]
- Fujita, W.H.; McCormick, C.L.; Parneix-Spake, A. An exploratory study to evaluate the efficacy of pimecrolimus cream 1% for the treatment of pityriasis alba. Int. J. Dermatol. 2007, 46, 700–705. [Google Scholar] [CrossRef] [PubMed]
- Rigopoulos, D.; Gregoriou, S.; Charissi, C.; Kontochristopoulos, G.; Kalogeromitros, D.; Georgala, S. Tacrolimus ointment 0.1% in pityriasis alba: An open-label, randomized, placebo-controlled study. Br. J. Dermatol. 2006, 155, 152–155. [Google Scholar] [CrossRef] [PubMed]
- Kapila, S.; Hong, E.; Fischer, G. A comparative study of childhood psoriasis and atopic dermatitis and greater understanding of the overlapping condition, psoriasis-dermatitis. Australas. J. Dermatol. 2012, 53, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Abramovits, W.; Cockerell, C.; Stevenson, L.C.; Goldstein, A.M.; Ehrig, T.; Menter, A. PsEma—A hitherto unnamed dermatologic entity with clinical features of both psoriasis and eczema. Skinmed 2005, 4, 275–281. [Google Scholar] [CrossRef] [PubMed]
- Kiriakis, K.P.; Tadros, A.; Dimou, A.; Karamanou, M.; Banaka, F.; Alexoudi, I. Case detection rates of impetigo by gender and age. Infez. Med. 2012, 20, 105–107. [Google Scholar] [PubMed]
- Ortega-Loayza, A.G.; Diamantis, S.A.; Gilligan, P.; Morrell, D.S. Characterization of Staphylococcus aureus cutaneous infections in a pediatric dermatology tertiary health care outpatient facility. J. Am. Acad. Dermatol. 2010, 62, 804–811. [Google Scholar] [CrossRef] [PubMed]
- Matiz, C.; Tom, W.L.; Eichenfield, L.F.; Pong, A.; Friedlander, S.F. Children with atopic dermatitis appear less likely to be infected with community acquired methicillin-resistant Staphylococcus aureus: The San Diego experience. Pediatr. Dermatol. 2011, 28, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.C.; Stovall, S.H.; Scurlock, A.M.; Perry, T.T.; Jones, S.M.; Harik, N.S. Addressing antimicrobial resistance to treat children with atopic dermatitis in a tertiary pediatric allergy clinic. Clin. Pediatr. (Phila) 2012, 51, 1025–1029. [Google Scholar] [CrossRef]
- Hetem, D.J.; Bonten, M.J. Clinical relevance of mupirocin resistance in Staphylococcus aureus. J. Hosp. Infect. 2013, 85, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.L.; Frank, J.E. Diagnosis and management of syphilis. Am. Fam. Physician 2003, 68, 283–290. [Google Scholar] [PubMed]
- Baughn, R.E.; Musher, D.M. Secondary syphilitic lesions. Clin. Microbiol. Rev. 2005, 18, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Dohil, M.A.; Lin, P.; Lee, J.; Lucky, A.W.; Paller, A.S.; Eichenfield, L.F. The epidemiology of molluscum contagiosum in children. J. Am. Acad. Dermatol. 2006, 54, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Berger, E.M.; Orlow, S.J.; Patel, R.R.; Schaffer, J.V. Experience with molluscum contagiosum and associated inflammatory reactions in a pediatric dermatology practice: The bump that rashes. Arch. Dermatol. 2012, 148, 1257–1264. [Google Scholar] [CrossRef]
- Netchiporouk, E.; Cohen, B.A. Recognizing and managing eczematous id reactions to molluscum contagiosum virus in children. Pediatrics 2012, 129, e1072–e1075. [Google Scholar] [CrossRef] [PubMed]
- Osio, A.; Deslandes, E.; Saada, V.; Morel, P.; Guibal, F. Clinical characteristics of molluscum contagiosum in children in a private dermatology practice in the greater Paris area, France: A prospective study in 661 patients. Dermatology 2011, 222, 314–320. [Google Scholar] [CrossRef] [PubMed]
- Hayashida, S.; Furusho, N.; Uchi, H.; Miyazaki, S.; Eiraku, K.; Gondo, C.; Tsuji, G.; Hachisuka, J.; Fukagawa, S.; Kido, M.; et al. Are lifetime prevalence of impetigo, molluscum and herpes infection really increased in children having atopic dermatitis? J. Dermatol. Sci. 2010, 60, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Olsen, J.R.; Gallacher, J.; Piguet, V.; Francis, N.A. Epidemiology of molluscum contagiosum in children: A systematic review. Fam. Pract. 2014, 31, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Frisch, S.; Siegfried, E.C. The clinical spectrum and therapeutic challenge of eczema herpeticum. Pediatr. Dermatol. 2011, 28, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Beck, L.A.; Boguniewicz, M.; Hata, T.; Schneider, L.C.; Hanifin, J.; Gallo, R.; Paller, A.S.; Lieff, S.; Reese, J.; Zaccaro, D.; et al. Phenotype of atopic dermatitis subjects with a history of eczema herpeticum. J. Allergy Clin. Immunol. 2009, 124, 260–269. [Google Scholar] [CrossRef] [PubMed]
- Peng, W.M.; Jenneck, C.; Bussmann, C.; Bogdanow, M.; Hart, J.; Leung, D.Y.; Bieber, T.; Eis-Hubinger, A.M.; Novak, N. Risk factors of atopic dermatitis patients for eczema herpeticum. J. Investig. Dermatol. 2007, 127, 1261–1263. [Google Scholar] [CrossRef] [PubMed]
- Aronson, P.L.; Shah, S.S.; Mohamad, Z.; Yan, A.C. Topical corticosteroids and hospital length of stay in children with eczema herpeticum. Pediatr. Dermatol. 2013, 30, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Lubbe, J.; Pournaras, C.C.; Saurat, J.H. Eczema herpeticum during treatment of atopic dermatitis with 0.1% tacrolimus ointment. Dermatology 2000, 201, 249–251. [Google Scholar] [CrossRef] [PubMed]
- Osawa, K.; Etoh, T.; Ariyoshi, N.; Ishii, I.; Ohtani, M.; Kariya, S.; Uchino, K.; Kitada, M. Relationship between Kaposi’s varicelliform eruption in Japanese patients with atopic dermatitis treated with tacrolimus ointment and genetic polymorphisms in the IL-18 gene promoter region. J. Dermatol. 2007, 34, 531–536. [Google Scholar] [CrossRef] [PubMed]
- Mathes, E.F.; Oza, V.; Frieden, I.J.; Cordoro, K.M.; Yagi, S.; Howard, R.; Kristal, L.; Ginocchio, C.C.; Schaffer, J.; Maguiness, S.; et al. “Eczema coxsackium” and unusual cutaneous findings in an enterovirus outbreak. Pediatrics 2013, 132, e149–e157. [Google Scholar] [CrossRef] [PubMed]
- Biesbroeck, L.; Sidbury, R. Viral exanthems: An update. Dermatol. Ther. 2013, 26, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Sanfilippo, A.M.; Barrio, V.; Kulp-Shorten, C.; Callen, J.P. Common pediatric and adolescent skin conditions. J. Pediatr. Adolesc. Gynecol. 2003, 16, 269–283. [Google Scholar] [CrossRef] [PubMed]
- Ely, J.W.; Rosenfeld, S.; Seabury Stone, M. Diagnosis and management of tinea infections. Am. Fam. Physician 2014, 90, 702–710. [Google Scholar] [PubMed]
- Orrico, J.A.; Krause-Parello, C.A. Facts, fiction, and figures of the Sarcoptes scabiei infection. J. Sch. Nurs. 2010, 26, 260–266. [Google Scholar] [CrossRef]
- Pope, E.; Weitzman, S.; Ngan, B.; Walsh, S.; Morel, K.; Williams, J.; Stein, S.; Garzon, M.; Knobler, E.; Lieber, C.; et al. Mycosis fungoides in the pediatric population: Report from an international Childhood Registry of Cutaneous Lymphoma. J. Cutan. Med. Surg. 2010, 14, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Carr, W.W. Topical calcineurin inhibitors for atopic dermatitis: Review and treatment recommendations. Paediatr. Drugs 2013, 15, 303–310. [Google Scholar] [CrossRef] [PubMed]
- Tennis, P.; Gelfand, J.M.; Rothman, K.J. Evaluation of cancer risk related to atopic dermatitis and use of topical calcineurin inhibitors. Br. J. Dermatol. 2011, 165, 465–473. [Google Scholar] [CrossRef] [PubMed]
- Breithaupt, A.D.; Alio, A.; Friedlander, S.F. A comparative trial comparing the efficacy of tacrolimus 0.1% ointment with Aquaphor ointment for the treatment of keratosis pilaris. Pediatr. Dermatol. 2011, 28, 459–460. [Google Scholar] [CrossRef] [PubMed]
- Traupe, H.; Fischer, J.; Oji, V. Nonsyndromic types of ichthyoses—An update. J. Dtsch. Dermatol. Ges. 2014, 12, 109–121. [Google Scholar] [PubMed]
- Bremmer, S.F.; Hanifin, J.M.; Simpson, E.L. Clinical detection of ichthyosis vulgaris in an atopic dermatitis clinic: Implications for allergic respiratory disease and prognosis. J. Am. Acad. Dermatol. 2008, 59, 72–78. [Google Scholar] [CrossRef] [PubMed]
- Allen, A.; Siegfried, E.; Silverman, R.; Williams, M.L.; Elias, P.M.; Szabo, S.K.; Korman, N.J. Significant absorption of topical tacrolimus in 3 patients with Netherton syndrome. Arch. Dermatol. 2001, 137, 747–750. [Google Scholar] [PubMed]
- Yan, A.C.; Honig, P.J.; Ming, M.E.; Weber, J.; Shah, K.N. The safety and efficacy of pimecrolimus, 1%, cream for the treatment of Netherton syndrome: Results from an exploratory study. Arch. Dermatol. 2010, 146, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Cedeno-Laurent, F.; Gomez-Flores, M.; Mendez, N.; Ancer-Rodriguez, J.; Bryant, J.L.; Gaspari, A.A.; Trujillo, J.R. New insights into HIV-1-primary skin disorders. J. Int. AIDS Soc. 2011, 14, 5. [Google Scholar] [CrossRef] [PubMed]
- Paller, A.S. Genetic immunodeficiency disorders. Clin. Dermatol. 2005, 23, 68–77. [Google Scholar] [CrossRef] [PubMed]
- Freeman, A.F.; Holland, S.M. Clinical manifestations of hyper IgE syndromes. Dis. Markers 2010, 29, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Minegishi, Y.; Saito, M. Cutaneous manifestations of Hyper IgE syndrome. Allergol. Int. 2012, 61, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Sillevis Smitt, J.H.; Kuijpers, T.W. Cutaneous manifestations of primary immunodeficiency. Curr. Opin. Pediatr. 2013, 25, 492–497. [Google Scholar] [CrossRef] [PubMed]
- Fiorino, G.; Danese, S.; Pariente, B.; Allez, M. Paradoxical immune-mediated inflammation in inflammatory bowel disease patients receiving anti-TNF-alpha agents. Autoimmun. Rev. 2014, 13, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Hebert, A.A. Laboratory evaluation of the child with recalcitrant eczema. Dermatol. Clin. 1994, 12, 109–121. [Google Scholar] [PubMed]
- Bernstein, M.L.; McCusker, M.M.; Grant-Kels, J.M. Cutaneous manifestations of cystic fibrosis. Pediatr. Dermatol. 2008, 25, 150–157. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.J. Phenylalanine hydroxylase deficiency. In GeneReviews® [Internet]; Pagon, R.A., Adam, M.P., Ardinger, H.H., Bird, T.D., Dolan, C.R., Fong, C.T., Smith, R.J.H., Stephens, K., Eds.; University of Washington, Seattle: Seattle, WA, USA, 1993–2015. Available online: http://www.ncbi.nlm.nih.gov/books/NBK1504 (acccessed on 16 January 2015). [Google Scholar]
- Zone, J.J. Skin manifestations of celiac disease. Gastroenterology 2005, 128, S87–S91. [Google Scholar] [CrossRef] [PubMed]
- Caproni, M.; Antiga, E.; Melani, L.; Fabbri, P. Guidelines for the diagnosis and treatment of dermatitis herpetiformis. J. Eur. Acad. Dermatol. Venereol. 2009, 23, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Goker, H.; Haznedaroglu, I.C.; Chao, N.J. Acute graft-vs.-host disease: Pathobiology and management. Exp. Hematol. 2001, 29, 259–277. [Google Scholar] [CrossRef] [PubMed]
- Jacobsohn, D.A.; Vogelsang, G.B. Acute graft versus host disease. Orphanet J. Rare Dis. 2007, 2, 35. [Google Scholar] [CrossRef] [PubMed]
- Muller, S.M.; Ege, M.; Pottharst, A.; Schulz, A.S.; Schwarz, K.; Friedrich, W. Transplacentally acquired maternal T lymphocytes in severe combined immunodeficiency: A study of 121 patients. Blood 2001, 98, 1847–1851. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siegfried, E.C.; Hebert, A.A. Diagnosis of Atopic Dermatitis: Mimics, Overlaps, and Complications. J. Clin. Med. 2015, 4, 884-917. https://doi.org/10.3390/jcm4050884
Siegfried EC, Hebert AA. Diagnosis of Atopic Dermatitis: Mimics, Overlaps, and Complications. Journal of Clinical Medicine. 2015; 4(5):884-917. https://doi.org/10.3390/jcm4050884
Chicago/Turabian StyleSiegfried, Elaine C., and Adelaide A. Hebert. 2015. "Diagnosis of Atopic Dermatitis: Mimics, Overlaps, and Complications" Journal of Clinical Medicine 4, no. 5: 884-917. https://doi.org/10.3390/jcm4050884
APA StyleSiegfried, E. C., & Hebert, A. A. (2015). Diagnosis of Atopic Dermatitis: Mimics, Overlaps, and Complications. Journal of Clinical Medicine, 4(5), 884-917. https://doi.org/10.3390/jcm4050884