Abstract
Congenital heart disease places a significant burden on the individual, family and community despite significant advances in our understanding of aetiology and treatment. Early research in ischaemic heart disease has paved the way for stem cell technology and bioengineering, which promises to improve both structural and functional aspects of disease. Stem cell therapy has demonstrated significant improvements in cardiac function in adults with ischaemic heart disease. This finding, together with promising case studies in the paediatric setting, demonstrates the potential for this treatment in congenital heart disease. Furthermore, induced pluripotent stems cell technology, provides a unique opportunity to address aetiological, as well as therapeutic, aspects of disease.
1. Clinical Consideration of Congenital Heart Disease
Treatment of congenital heart disease (CHD) occupies a unique place in the human history of cardiovascular medicine. This dates back to the pioneering development of early heart-lung machines in the early 1950s. Subsequent development of this technology allowed correction of simple heart defects in childhood that would have otherwise led to early death, with further evolution permitting routine adult cardiac surgery for ischaemic and valvular heart disease, now accepted as “everyday surgery”.
In modern CHD clinical research, both patients and practitioners look forward to similar paradigm shifts in treatments to address some of the inadequacies of current management that continue to impact individuals, families and workplaces. There are now more adults with congenital heart disease than children in advanced societies [1] and whilst many are effectively “cured” with childhood intervention (such as closure of infant ventricular septal defects) others have an ongoing need for close medical management including those with single ventricle physiology [2] or who require repeated surgeries, for example, those who will need replacement of right ventricle to pulmonary artery conduits.
The burden of disease is significant and has physical, psychological and economic impacts [3]. CHD occurs in ~7–8 in 1000 live births [4,5]. A subset of CHD is invariably lethal around birth unless treated, and these cases present significant challenges with respect to surgical reconstruction, critical care patient management, long term follow up and the ethics of focusing major health resources onto few individuals. CHD successfully treated in childhood carries a strong likelihood of complications in later life and a life-long emotional and financial burden for affected families [6]. The dramatic reduction in mortality after surgical correction of CHD in recent years has been accompanied by increasing recognition of poor neurological outcomes in survivors of CHD, which may involve genetic factors, abnormal brain perfusion and development in utero and/or susceptibilities to hypoxia resulting from CHD, or other environmental parameters such as anesthesia [7,8]. A key bottleneck in patient care is the transition from childhood to adulthood, where patients may be lost to follow up.
Childhood treatment is very costly and paediatric cardiac surgery is the most common reason for admission to paediatric intensive care. Over the last three decades, surgery has become more complex and is generally performed earlier—often during the neonatal period—to gain better functional outcomes in the long term. A diagnosis of CHD is associated with important psychosocial dysfunction with many parents reporting symptoms equivalent to post-traumatic stress disorders, high levels of parental depression and ongoing anxiety with similar problems observed in adolescent and adult survivors [9].
Addressing causation of CHD has been a high priority over the last decades, particularly for the minority of cases that show familial inheritance. Classical linkage analysis has been the mainstay methodology underpinning these studies. Studies on the interaction between genetic and environmental factors have revealed clinically important perturbations of the highly conserved and tightly regulated developmental cardiogenic processes but only in a smaller number of patients with single gene disorders and associated syndromes [10]. In the new era of genetic research, genome wide association studies have identified areas of common chromosomal variation associated with the most common but simple form of CHD, secundum ASD [11], but with relatively low odds ratios and limited clinical application. Massively parallel sequencing of the whole exome [12] and its more targeted approaches [13] have dramatically accelerated the disease gene discovery pipeline, yielding answers for additional families. Polygenic contribution, variable penetrance and variation in phenotype present ongoing challenges.
On the horizon is a new era of stem cell-based therapies and bioengineering, and it is hoped that these approaches can help reduce the burden of CHD. In broad terms, stem cell and bioengineering approaches may make contributions to: (i) improving structural solutions in repair of malformed hearts; (ii) improving the function of repaired hearts and their circulation; and (iii) facilitating modelling of CHD to advance our understanding of its molecular underpinnings. These will be discussed further below.
1.1. Structural Solutions
In paediatric heart surgery, there is a need to address the current demands of the circulation as well as future growth. Many forms of advanced neonatal surgery involve utilisation of the existing ventriculo-arterial connection as the systemic outflow (usually through a large ventricular septal defect) and creation of an extra-anatomic right ventricle to pulmonary artery conduit. Repairs of pulmonary atresia with VSD, and truncus arteriosus are examples that utilise this approach. Usually either a human cadaveric allograft (homograft) is used for this purpose, or a bovine jugular venous conduit, combining a “tube” with a valve. A larger group of patients, those with tetralogy of Fallot, may require pulmonary valve replacement, currently also utilising allograft or xenograft tissue valves.
Whilst effective in the short term, the long term functional outcomes of such approaches are poor, with all requiring replacement within 3 to 8 years depending on the size of the patient, patient growth, host response to the allograft or xenograft and other factors including the occasional development of endocarditis. Supplies of both types of conduit are limited and are associated with significant expense. Allosensitisation to donated human products can also be a problem if transplantation is later required. Percutaneous approaches are now available that are suitable for some patients, particularly in the adolescent group, but as xenoproducts they remain susceptible to immune mediated structural valve deterioration and infection.
Many biologic approaches have been attempted to improve longevity of the implanted valve, including decellularising and re-seeding allograft tissue with host endothelial cells [14]; however this approach has not yet been shown to produce meaningfully increased graft survival or somatic growth [15]. Generation of a vascularised matrix that can then be seeded and shaped [16] is emerging as an approach that avoids the need for allograft material but will require complex 3D construction to simulate tube and valve formation. Patients undergoing the Fontan operation as a final step in construction of a cavo-pulmonary connection have been managed with tissue engineered vascular grafts to convey the inferior vena caval blood to the pulmonary arteries [17]. This is valuable proof of principle work yielding understandings of optimal matrix construction, albeit that no significant growth is presently required of this connection using current surgical approaches [18]. Electrospinning and microfabrication techniques to engineer scaffolds that support the growth of valvular interstitial cells and mesenchymal stem cells [19] offer a way to customise the size and shape of the replacement tissue, perhaps guided by 3D imaging of the planned recipient. Repopulation with engineered patient-specific cells utilising adult stem cell or induced pluripotent stem cell technologies would seem logical for the future [20,21].
1.2. Stem Cells to Improve Cardiac Function
There is extensive and ongoing work to support the use of stem cells in recovery from myocardial infarction in adult populations, particularly using bone marrow derived cells, albeit that the rationale for such studies is under intense scrutiny [22]. Regeneration of scar tissue into functional myocardium and improved ventricular performance are the aims of such interventions with recent promise [23,24,25]. In paediatric cardiology the aim would be the optimisation of ventricular performance for children subjected to volume or pressure loads, usually after correction of the structural abnormalities that promote ventricular dysfunction. There is particular interest in the subpopulation of patients with a functional single ventricle, especially those who have undergone complex single ventricle surgery such as the Norwood operation for hypoplastic left heart (HLH) [26].
Typically HLH patients would be infants after the first two stages of surgery involving long periods of cardiopulmonary bypass and shorter periods of planned and “protected” myocardial ischaemia. An increased volume load related to the shunt providing pulmonary blood flow after the initial operation adds to the work that the single right ventricle must perform, which is already at an anatomic disadvantage being a morphologic right ventricle working against systemic vascular resistance. It is not uncommon for the function of such ventricles to deteriorate, particularly after second stage surgery, promoting atrioventricular valve regurgitation which positively reinforces the ventricular dysfunction. Relative coronary insufficiency [27] or a primary myocardial process may contribute. Structural abnormalities have been identified in single right ventricular tissue [28]. Ventricular performance is a major determinant of suitability for the last stage of the single ventricle pathway, Fontan completion (total cavo-pulmonary connection) as well as performance and survival with the Fontan circulation.
In parallel with studies in animal models [29,30], various approaches to ventricular support using stem cell technology are being trialled in CHD patients with differing donor cell origins and modes of administration, as outlined by Tarui et al. [31]. A number of stem cell populations have been described in the mammalian heart using cell surface markers and various functional assays including colony formation, and growth and differentiation potential in vitro and in vivo [22] Cardiosphere-derived cells are among the first populations to be trialled in humans for ischaemic heart disease in adults [32,33]. They are heterogeneous cell preparations derived from the 3D cellular clusters (cardiospheres) that can be readily established from heart biopsies, and which are thought to provide a harbour (niche) for cells with stem or progenitor cell properties during in vitro culture. Cells derived from atrial tissue and administered via the intracoronary route at cardiac catheterisation, have been trialled in patients with HLH in Phase I and Phase II clinical trials, with other groups utilising umbilical cord [34] and bone marrow derived cell fractions [31]. Phase 1 trials have indicated the safety of this approach with some improvement in right ventricular systolic function evident, and Phase 2 studies are underway. In the recently reported Phase 1 study of autologous cardiosphere-derived cells delivered via the intracoronary route [35], no safety concerns were raised and an improvement in right ventricular function was observed at 18 months compared to controls. The effect size is encouraging and clinically relevant (a 10% increase in right ventricular ejection fraction). The use of autologous cells represents a clear advantage in this environment. Similar approaches may be of benefit in paediatric heart failure presenting as dilated cardiomyopathy.
Uncertainty persists about the mechanism by which the stem cells might induce functional improvement. In ischaemic disease and cardiomyopathy, paracrine activation of local regenerative pathways may significantly contribute to the improvements in performance, while tissue replacement due to stem cell deployment does not seem to be a dominant feature in animal studies [36].
Cord blood stem cells have been shown to engraft and augment right ventricular function in an ovine model in the presence of increased workload [30]. A similar model of right ventricular overloading in rats demonstrated improved diastolic dysfunction and suppression of ventricular fibrosis following skeletal myoblast transplantation (Hoashi et al. 2009). Case reports demonstrate improvement in ventricular function following intracoronary delivery of bone marrow derived cells in children with terminal cardiomyopathy [37,38] as well as ventricular failure following surgery for HLH [39]. In HLH, adaptation of the right ventricle to increased work load may require cellular proliferation beyond the capability of the intrinisic regenerative systems. The capacity for autologous modified cells in CHD to influence cardiac performance or myocyte proliferation may be diminished by the persistence of genetic characteristics that caused or contributed to abnormal development during primary cardiogenesis. However, the development of refined cell therapy approaches may support the growth and development required.
2. Induced Pluripotent Stem Cells to Study Causation in Congenital Heart Disease
Induced pluripotent stem cells (iPSC) can be created from virtually any somatic cell, most commonly from dermal fibroblasts [40]. These pluripotent cell types are created by the reprogramming of adult cells to a pluripotent state, giving them the ability to differentiate into all cell types of the human body, including cardiomyocytes (see Figure 1) as well as smooth muscle, endothelial and epicardial cells, the highly specialised cell types of the heart. This makes iPSC an invaluable resource for the study of CHD. The technology offers the unique opportunity to create human models of disease and development in a patient-specific context that incorporates the individual clinical features of the disease. Additionally, iPSC provide material to study the earliest time points in development, previously difficult due to restrictions on the availability of primary human tissue for study.
iPSC are playing an increasing role in personalised medicine, specifically in disease profiling of both rare and common diseases, and in the design of personalised therapies. Due to the recent success of directed differentiation protocols [41,42,43], iPSC allow the provision of lineage-specific stem and progenitor cells, as well as differentiated specialised cell types, for disease research, cellular therapies and tissue engineering. However, before iPSC are used as a source of biologic material for clinical application, concerns regarding the oncogenic effect of retained transgenes [44] and trans-differentiation need to be addressed [45]. Until then, iPSC are being increasingly used as a test bed to study development and disease mechanism. In the cardiac area, iPSC approaches have been successful in assessing the functional disorder associated with LEOPARD Syndrome [46,47] and various arrhythmias and cardiomyopathies [48,49].
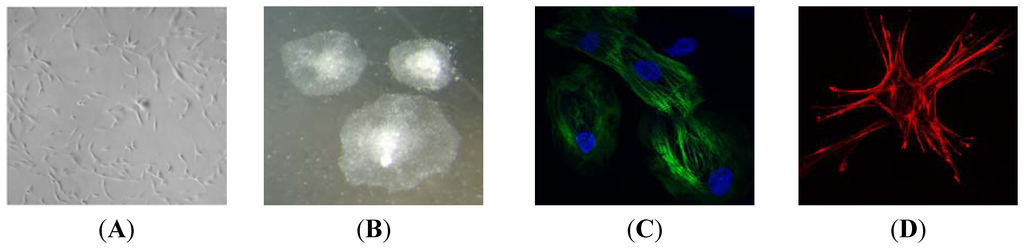
Figure 1.
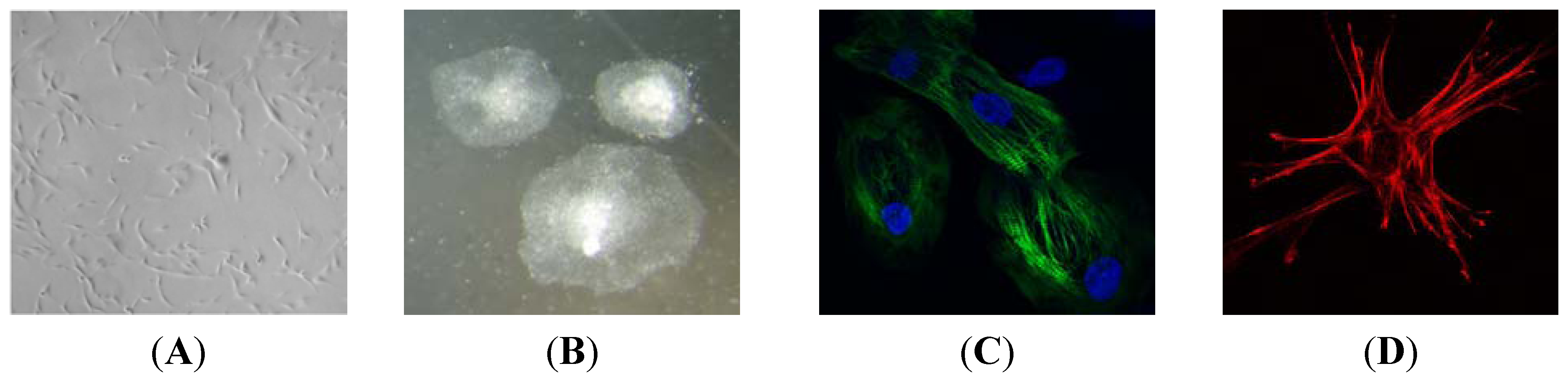
(A) Patient-derived fibroblasts generated from a skin biopsy; (B) Undifferentiated iPSC colonies derived from patient-derived fibroblasts; (C) Cardiomyocytes derived from iPSC stained for the sarcomeric protein, cardiac troponin T; (D) Smooth muscle cells derived from iPSC stained for the cell scaffolding protein, alpha smooth muscle actin.
Figure 1.
(A) Patient-derived fibroblasts generated from a skin biopsy; (B) Undifferentiated iPSC colonies derived from patient-derived fibroblasts; (C) Cardiomyocytes derived from iPSC stained for the sarcomeric protein, cardiac troponin T; (D) Smooth muscle cells derived from iPSC stained for the cell scaffolding protein, alpha smooth muscle actin.
iPSC are playing an increasing role in personalised medicine, specifically in disease profiling of both rare and common diseases, and in the design of personalised therapies. Due to the recent success of directed differentiation protocols [41,42,43], iPSC allow the provision of lineage-specific stem and progenitor cells, as well as differentiated specialised cell types, for disease research, cellular therapies and tissue engineering. However, before iPSC are used as a source of biologic material for clinical application, concerns regarding the oncogenic effect of retained transgenes [44] and trans-differentiation need to be addressed [45]. Until then, iPSC are being increasingly used as a test bed to study development and disease mechanism. In the cardiac area, iPSC approaches have been successful in assessing the functional disorder associated with LEOPARD Syndrome [46,47] and various arrhythmias and cardiomyopathies [48,49].
The approach is applicable to CHD particularly for cell-autonomous genetic disorders affecting, for example, the development or function of cardiomyocytes that can be modelled in 2D cell cultures or 3D tissue constructs [50,51]. The approach has its obvious limitations with respect to modelling the complex tissue interactions necessary for organ structure, and the non-cell autonomous environmental or epigenetic influences on disease. However, rapid progress is being made on directed differentiation of highly complex organoids and tissue layers from pluripotent stem cells [52,53], opening up vast new potential for therapies and modelling disease in this system.
Using a patient-specific in vitro model of HLH is of particular interest to clinicians and scientists in the field attempting to reconcile the most common theory about the genesis of HLH—reduced transventricular flow and altered loading during development—with the heterogeneity in morphology as well as performance and decline observed in clinical cases [54,55]. An iPSC approach will complement the forward genetic approach being taken in mice [56]. While it has been suggested that HLH is essentially a severe form of valve malformation [56,57], some cases of HLH have a bulky LV and small but formed mitral and aortic valves, whilst others have barely a recognisable LV cavity. In combination these studies lead to speculation that a primary myocardial disorder is present in HLH, which likely predetermines the size and function of the ventricle and perhaps contributes to difficulties in later childhood in some with this condition. HLH is thought to have a high genetic component with complex inheritance, and is often associated with chromosomal abnormalities [58], which could impact on either valvular structures or ventricular cardiomyocyte growth and function, or both. Of the limited number of gene pathways implicated in HLH [58], the transcription factors NKX2-5 and NOTCH1 are known to be involved in both valvular and chamber development [59,60]. Both genes are also involved in aortic coarctation and bicuspid aortic valve, which exist within the spectrum of left-sided abnormalities that includes HLH at its most severe end [61,62,63].
Jiang and colleagues made iPSC from a single HLH patient and used them to derive cardiomyocytes by directed differentiation. They found a number of important primary cardiac defects including altered expression of key cardiac transcription factors, fewer beating clusters and reduced myofibrillar organisation, persistence of a fetal gene expression pattern as well as altered calcium transients and calcium handling [54]. Kobayashi et al. analysed single clones from three HLH patients, using a clone from a patient with bicuspid aortic valve and total anomalous pulmonary venous connection as a control [55]. They showed reduced expression of a number of cardiac transcription factors at late time points after induced cardiomyocyte differentiation, and associated changes in total chromatin marks—di-methylation on histone H3 lysine 4, tri-methylation on histone H3 lysine 27, and acetylation of histone H3. Whether the reported changes are common to all cases of HLH remains to be seen. Such molecular phenotypes in patient specific iPSC-derived cardiomyocytes raises the possibility that disease modelling using the iPSC platform can provide both molecular diagnosis, as has been utilised in other cardiovascular diseases [64] and cell therapy into the future.
Bioengineering Heart Muscle Using iPS Cells
Investigations into the creation of functional heart tissue in vitro by tissue engineering techniques using donor cardiomyocytes is still in its very early stages [65,66,67,68]. While there are no clinical applications of the method to date, cardiac tissue engineering has seen progress over the last twenty years in all four of the elements central to this method: generation of donor cardiomyocytes, development of scaffold materials and control of cell survival, engraftment and growth with bioactive molecules (see recent reviews [51,69,70]). The latest developments include ex vivo and in vivo approaches that promote the growth of vascular and structural elements of cardiac tissue [71,72]. Growing cells as sheets has made possible the insertion of iPSC-derived cardiomyocytes into the porcine heart for short term benefits [73]. Human embryonic stem cell-derived cardiomyocytes have been successfully engrafted in a non-human primate model of myocardial infarction [74]. This approach included development and application of mass culture techniques able to support production and delivery of a billion cells, selection of delivery techniques to optimise survival, such as a supportive hydrogel scaffold and application of a cocktail of preconditioning regimes. While this demonstrates potential for successful remuscularization of the human heart, issues with the incomplete maturation of cardiomyocytes, as well as arrhythmogenesis, need to be addressed. Contractile and vascularised human cardiac tissues have also been created from iPS cells [75,76] to provide long term survival and contractility, and 3D microtissues derived from iPSC also show promise for transplantation [77].
The ability to make whole functional hearts or bioengineered patches and conduits is challenging and has not been achieved for clinical use thus far. A form of bioengineered hearts have been configured using human iPSC-derived multipotential cardiovascular progenitors (MCP), which are likely similar to the earliest cardiac progenitors in heart development, by implanting them into a decellularized donor mouse heart [78]. The decellularized heart provides an excellent 3D structure for bioengineering whole organs or surgical implants as it utilises the natural extracellular matrix to promote cardiomyocyte proliferation, differentiation and function. The use of such native cardiac scaffold provides appropriate cues for engraftment, promotes rapid vascularisation and also avoids the biocompatibility problems of some artificial scaffold materials. MCP may offer an advantageous cell type for cardiac tissue bioengineering applications as they can potentially self-organise into structures containing cardiomyocytes, smooth muscle cells and endothelial cells, guided by extracellular matrix cues. However, before a whole heart can be bioengineered, a number of challenges remain, including safeguards surrounding the use of iPSC as discussed, as well as modulation of the immune response and, in CHD applications, finding ways that allow growth of the graft along with the patient’s heart.
3. Conclusions
Emerging technology in stem cells and bio-engineering may address major issues in congenital heart disease that limit lifespan and reduce quality of life for a significant number of children and adults. iPSC technology offers an opportunity to provide both molecular diagnosis and, in the future, tissue based therapy for some of the more complex reconstructive tasks in congenital heart disease.
Author Contributions
Alexis Bosman wrote sections of manuscript and provided figures and experimental data; Michael J. Edel, Gillian Blue, Rodney J. Dilley and Richard P. Harvey wrote sections of manuscript and provided critical review; David S. Winlaw drafted the initial manuscript, coordinated co-author’s efforts, and provided critical revision of manuscript and response to reviewers.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Blaha, M.J.; Dai, S.; Ford, E.S.; Fox, C.S.; Franco, S.; et al. Heart disease and stroke statistics—2014 update: A report from the American Heart Association. Circulation 2014, 129, e28–e292. [Google Scholar] [CrossRef] [PubMed]
- D’Udekem, Y.; Iyengar, A.J.; Galati, J.C.; Forsdick, V.; Weintraub, R.G.; Wheaton, G.R.; Bullock, A.; Justo, R.N.; Grigg, L.E.; Sholler, G.F.; et al. Redefining expectations of long-term survival after the Fontan procedure: Twenty-five years of follow-up from the entire population of Australia and New Zealand. Circulation 2014, 130, S32–S38. [Google Scholar] [CrossRef]
- Leggat, S. Childhood Heart Disease in Australia: Current Practices and Future Needs; HeartKids Australia: Pennant Hills, NSW, Australia, 2011; pp. 1–52. [Google Scholar]
- Hoffman, J.I.E.; Kaplan, S. The incidence of congenital heart disease. JAC 2002, 39, 1890–1900. [Google Scholar]
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. Heart disease and stroke statistics—2013 update: A report from the American Heart Association. Circulation 2013, 127, e6–e245. [Google Scholar] [CrossRef] [PubMed]
- Tutarel, O. Acquired heart conditions in adults with congenital heart disease: A growing problem. Heart 2014, 100, 1317–1321. [Google Scholar] [CrossRef] [PubMed]
- Gaynor, J.W. The encephalopathy of congenital heart disease. J. Thorac. Cardiovasc. Surg. 2014, 148, 1790–1791. [Google Scholar] [CrossRef] [PubMed]
- Masoller, N.; Martínez, J.M.; Gómez, O.; Bennasar, M.; Crispi, F.; Sanz-Cortés, M.; Egaña-Ugrinovic, G.; Bartrons, J.; Puerto, B.; Gratacós, E. Evidence of second-trimester changes in head biometry and brain perfusion in fetuses with congenital heart disease. Ultrasound Obstet. Gynecol. 2014, 44, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Kasparian, N.A.; Fidock, B.; Sholler, G.F.; Camphausen, C.; Murphy, D.N.; Cooper, S.G.; Kaul, R.; Jones, O.; Winlaw, D.S.; Kirk, E.P.E. Parents’ perceptions of genetics services for congenital heart disease: The role of demographic, clinical, and psychological factors in determining service attendance. Genet. Med. 2014, 16, 460–468. [Google Scholar] [CrossRef] [PubMed]
- Blue, G.M.; Kirk, E.P.; Sholler, G.F.; Harvey, R.P.; Winlaw, D.S. Congenital heart disease: Current knowledge about causes and inheritance. Med. J. Aust. 2012, 197, 155–159. [Google Scholar] [CrossRef] [PubMed]
- Cordell, H.J.; Bentham, J.; Topf, A.; Zelenika, D.; Heath, S.; Mamasoula, C.; Cosgrove, C.; Blue, G.; Granados-Riveron, J.; Setchfield, K.; et al. Genome-wide association study of multiple congenital heart disease phenotypes identifies a susceptibility locus for atrial septal defect at chromosome 4p16. Nat. Genet. 2013, 45, 822–824. [Google Scholar] [CrossRef]
- Zaidi, S.; Choi, M.; Wakimoto, H.; Ma, L.; Jiang, J.; Overton, J.D.; Romano-Adesman, A.; Bjornson, R.D.; Breitbart, R.E.; Brown, K.K.; et al. De novo mutations in histone-modifying genes in congenital heart disease. Nature 2013, 498, 220–223. [Google Scholar] [CrossRef]
- Blue, G.M.; Kirk, E.P.; Giannoulatou, E.; Dunwoodie, S.L.; Ho, J.W.K.; Hilton, D.C.K.; White, S.M.; Sholler, G.F.; Harvey, R.P.; Winlaw, D.S. Targeted next-generation sequencing identifies pathogenic variants in familial congenital heart disease. J. Am. Coll. Cardiol. 2014, 64, 2498–2506. [Google Scholar] [CrossRef] [PubMed]
- Cebotari, S.; Lichtenberg, A.; Tudorache, I.; Hilfiker, A.; Mertsching, H.; Leyh, R.; Breymann, T.; Kallenbach, K.; Maniuc, L.; Batrinac, A.; et al. Clinical application of tissue engineered human heart valves using autologous progenitor cells. Circulation 2006, 114, I132–I137. [Google Scholar] [CrossRef] [PubMed]
- Dijkman, P.E.; Driessen-Mol, A.; Frese, L.; Hoerstrup, S.P.; Baaijens, F.P.T. Decellularized homologous tissue-engineered heart valves as off-the-shelf alternatives to xeno- and homografts. Biomaterials 2012, 33, 4545–4554. [Google Scholar] [CrossRef] [PubMed]
- Andrée, B.; Bela, K.; Horvath, T.; Lux, M.; Ramm, R.; Venturini, L.; Ciubotaru, A.; Zweigerdt, R.; Haverich, A.; Hilfiker, A. Successful re-endothelialization of a perfusable biological vascularized matrix (BioVaM) for the generation of 3D artificial cardiac tissue. Basic Res. Cardiol. 2014, 109. [Google Scholar] [CrossRef]
- Udelsman, B.V.; Maxfield, M.W.; Breuer, C.K. Tissue engineering of blood vessels in cardiovascular disease: Moving towards clinical translation. Heart 2013, 99, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Kurobe, H.; Maxfield, M.W.; Breuer, C.K.; Shinoka, T. Concise review: Tissue-engineered vascular grafts for cardiac surgery: Past, present, and future. Stem Cells Transl. Med. 2012, 1, 566–571. [Google Scholar] [CrossRef] [PubMed]
- Masoumi, N.; Annabi, N.; Assmann, A.; Larson, B.L.; Hjortnaes, J.; Alemdar, N.; Kharaziha, M.; Manning, K.B.; Mayer, J.E.; Khademhosseini, A. Tri-layered elastomeric scaffolds for engineering heart valve leaflets. Biomaterials 2014, 35, 7774–7785. [Google Scholar] [CrossRef] [PubMed]
- Weber, B.; Emmert, M.; Hoerstrup, S. Stem cells for heart valve regeneration. Swiss Med. Wkly. 2012, 142. [Google Scholar] [CrossRef]
- Simpson, D.L.; Wehman, B.; Galat, Y.; Sharma, S.; Mishra, R.; Galat, V.; Kaushal, S. Engineering patient-specific valves using stem cells generated from skin biopsy specimens. Ann. Thorac. Surg. 2014, 98, 947–954. [Google Scholar] [CrossRef] [PubMed]
- Chong, J.J.H.; Forte, E.; Harvey, R.P. Developmental origins and lineage descendants of endogenous adult cardiac progenitor cells. Stem Cell Res. 2014, 13, 592–614. [Google Scholar] [CrossRef] [PubMed]
- Malliaras, K.; Makkar, R.R.; Smith, R.R.; Cheng, K.; Wu, E.; Bonow, R.O.; Marbán, L.; Mendizabal, A.; Cingolani, E.; Johnston, P.V.; et al. Intracoronary cardiosphere-derived cells after myocardial infarction: Evidence of therapeutic regeneration in the final 1-year results of the CADUCEUS trial (CArdiosphere-Derived aUtologous stem CElls to reverse ventricUlar dySfunction). JAC 2014, 63, 110–122. [Google Scholar]
- Piepoli, M.F.; Vallisa, D.; Arbasi, C.; Cavanna, L.; Cerri, L.; Mori, M.; Passerini, F.; Tommasi, L.; Rossi, A.; Capucci, A. Two year follow-up results of the CARDIAC (CARDIomyoplasty by Autologous intraCoronary bone marrow in acute myocardial infarction) randomised controlled trial. Int. J. Cardiol. 2013, 168, e132. [Google Scholar] [CrossRef] [PubMed]
- Vrtovec, B.; Poglajen, G.; Lezaic, L.; Sever, M.; Domanovic, D.; Cernelc, P.; Socan, A.; Schrepfer, S.; Torre-Amione, G.; Haddad, F.; et al. Effects of intracoronary CD34+ stem cell transplantation in nonischemic dilated cardiomyopathy patients: 5-year follow-up. Circ. Res. 2013, 112, 165–173. [Google Scholar] [CrossRef] [PubMed]
- Tchervenkov, C.I.; Jacobs, J.P.; Weinberg, P.M.; Aiello, V.D.; Béland, M.J.; Colan, S.D.; Elliott, M.J.; Franklin, R.C.G.; Gaynor, J.W.; Krogmann, O.N.; et al. The nomenclature, definition and classification of hypoplastic left heart syndrome. CTY 2006, 16, 339–368. [Google Scholar] [CrossRef]
- Donnelly, J.P.; Raffel, D.M.; Shulkin, B.L.; Corbett, J.R.; Bove, E.L.; Mosca, R.S.; Kulik, T.J. Resting coronary flow and coronary flow reserve in human infants after repair or palliation of congenital heart defects as measured by positron emission tomography. J. Thorac. Cardiovasc. Surg. 1998, 115, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Salih, C.; McCarthy, K.P.; Ho, S.Y. The fibrous matrix of ventricular myocardium in hypoplastic left heart syndrome: A quantitative and qualitative analysis. Ann. Thorac. Surg. 2004, 77, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Yerebakan, C.; Sandica, E.; Prietz, S.; Klopsch, C.; Ugurlucan, M.; Kaminski, A.; Abdija, S.; Lorenzen, B.; Boltze, J.; Nitzsche, B.; et al. Autologous umbilical cord blood mononuclear cell transplantation preserves right ventricular function in a novel model of chronic right ventricular volume overload. Cell Transpl. 2009, 18, 855–868. [Google Scholar] [CrossRef]
- Davies, B.; Elwood, N.J.; Li, S.; Cullinane, F.; Edwards, G.A.; Newgreen, D.F.; Brizard, C.P. Human cord blood stem cells enhance neonatal right ventricular function in an ovine model of right ventricular training. Ann. Thorac. Surg. 2010, 89, 585–593. [Google Scholar] [CrossRef] [PubMed]
- Tarui, S.; Sano, S.; Oh, H. Stem cell therapies in patients with single ventricle physiology. Methodist Debakey Cardiovasc. J. 2014, 10, 77–81. [Google Scholar] [CrossRef] [PubMed]
- Bolli, R.; Chugh, A.R.; D’Amario, D.; Loughran, J.H.; Stoddard, M.F.; Ikram, S.; Beache, G.M.; Wagner, S.G.; Leri, A.; Hosoda, T.; et al. Cardiac stem cells in patients with ischaemic cardiomyopathy (SCIPIO): Initial results of a randomised phase 1 trial. Lancet 2011, 378, 1847–1857. [Google Scholar] [CrossRef] [PubMed]
- Makkar, R.R.; Smith, R.R.; Cheng, K.; Malliaras, K.; Thomson, L.E.J.; Berman, D.; Czer, L.S.C.; Marbán, L.; Mendizabal, A.; Johnston, P.V.; et al. Intracoronary cardiosphere-derived cells for heart regeneration after myocardial infarction (CADUCEUS): A prospective, randomised phase 1 trial. Lancet 2012, 379, 895–904. [Google Scholar] [CrossRef] [PubMed]
- Burkhart, H.M.; Qureshi, M.Y.; Peral, S.C.; O’Leary, P.W.; Olson, T.M.; Cetta, F.; Nelson, T.J.; The Wanek Program Clinical Pipeline Group. Regenerative therapy for hypoplastic left heart syndrome: First report of intraoperative intramyocardial injection of autologous umbilical-cord blood-derived cells. J. Thorac. Cardiovasc. Surg. 2014, 149, e35–e37. [Google Scholar] [CrossRef] [PubMed]
- Ishigami, S.; Ohtsuki, S.; Tarui, S.; Ousaka, D.; Eitoku, T.; Kondo, M.; Okuyama, M.; Kobayashi, J.; Baba, K.; Arai, S.; et al. Intracoronary autologous cardiac progenitor cell transfer in patients with hypoplastic left heart syndrome: The TICAP prospective phase 1 controlled trial. Circ. Res. 2015, 116, 653–664. [Google Scholar] [CrossRef] [PubMed]
- Li, T.-S.; Cheng, K.; Malliaras, K.; Smith, R.R.; Zhang, Y.; Sun, B.; Matsushita, N.; Blusztajn, A.; Terrovitis, J.; Kusuoka, H.; et al. Direct comparison of different stem cell types and subpopulations reveals superior paracrine potency and myocardial repair efficacy with cardiosphere-derived cells. J. Am. Coll. Cardiol. 2012, 59, 942–953. [Google Scholar] [CrossRef] [PubMed]
- Rupp, S.; Jux, C.; Bönig, H.; Bauer, J.; Tonn, T.; Seifried, E.; Dimmeler, S.; Zeiher, A.M.; Schranz, D. Intracoronary bone marrow cell application for terminal heart failure in children. CTY 2012, 22, 558–563. [Google Scholar] [CrossRef]
- Rupp, S.; Bauer, J.; Tonn, T.; Schächinger, V.; Dimmeler, S.; Zeiher, A.M.; Schranz, D. Intracoronary administration of autologous bone marrow-derived progenitor cells in a critically ill two-yr-old child with dilated cardiomyopathy. Pediatr. Transpl. 2009, 13, 620–623. [Google Scholar] [CrossRef]
- Rupp, S.; Zeiher, A.M.; Dimmeler, S.; Tonn, T.; Bauer, J.; Jux, C.; Akintuerk, H.; Schranz, D. A regenerative strategy for heart failure in hypoplastic left heart syndrome: Intracoronary administration of autologous bone marrow-derived progenitor cells. J. Heart Lung Transplant. 2010, 29, 574–577. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Tanabe, K.; Ohnuki, M.; Narita, M.; Ichisaka, T. Induction of pluripotent stem cells from adult human fibroblasts by defined factors. Cell 2007, 131, 861–872. [Google Scholar] [CrossRef] [PubMed]
- Lian, X.; Zhang, J.; Azarin, S.M.; Zhu, K.; Hazeltine, L.B.; Bao, X.; Hsiao, C.; Kamp, T.J.; Palecek, S.P. Directed cardiomyocyte differentiation from human pluripotent stem cells by modulating Wnt/β-catenin signaling under fully defined conditions. Nat. Protoc. 2013, 8, 162–175. [Google Scholar] [CrossRef] [PubMed]
- Kattman, S.J.; Witty, A.D.; Gagliardi, M.; Dubois, N.C.; Niapour, M.; Hotta, A.; Ellis, J.; Keller, G. Stage-specific optimization of activin/nodal and BMP signaling promotes cardiac differentiation of mouse and human pluripotent stem cell lines. Cell Stem Cell 2011, 8, 228–240. [Google Scholar] [CrossRef] [PubMed]
- Witty, A.D.; Mihic, A.; Tam, R.Y.; Fisher, S.A.; Mikryukov, A.; Shoichet, M.S.; Li, R.-K.; Kattman, S.J.; Keller, G. Generation of the epicardial lineage from human pluripotent stem cells. Nat. Biotechnol. 2014, 32, 1026–1035. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Fernandez, A.; Nelson, T.J.; Reyes, S.; Alekseev, A.E.; Secreto, F.; Perez-Terzic, C.; Beraldi, R.; Sung, H.-K.; Nagy, A.; Terzic, A. iPS cell-derived cardiogenicity is hindered by sustained integration of reprogramming transgenes. Circ. Cardiovasc. Genet 2014, 7, 667–676. [Google Scholar] [CrossRef] [PubMed]
- Addis, R.C.; Epstein, J.A. Induced regeneration—the progress and promise of direct reprogramming for heart repair. Nat. Publ. Group 2013, 19, 829–836. [Google Scholar]
- Lin, B.; Kim, J.; Li, Y.; Pan, H.; Carvajal-Vergara, X.; Salama, G.; Cheng, T.; Li, Y.; Lo, C.W.; Yang, L. High-purity enrichment of functional cardiovascular cells from human iPS cells. Cardiovasc. Res. 2012, 95, 327–335. [Google Scholar] [CrossRef] [PubMed]
- Carvajal-Vergara, X.; Sevilla, A.; D’Souza, S.L.; Ang, Y.-S.; Schaniel, C.; Lee, D.-F.; Yang, L.; Kaplan, A.D.; Adler, E.D.; Rozov, R.; et al. Patient-specific induced pluripotent stem-cell-derived models of LEOPARD syndrome. Nature 2010, 465, 808–812. [Google Scholar] [CrossRef] [PubMed]
- Vitale, A.M.; Wolvetang, E.; Mackay-Sim, A. Induced pluripotent stem cells: A new technology to study human diseases. Int. J. Biochem. Cell Biol. 2011, 43, 843–846. [Google Scholar] [CrossRef] [PubMed]
- Sharma, A.; Marceau, C.; Hamaguchi, R.; Burridge, P.W.; Rajarajan, K.; Churko, J.M.; Wu, H.; Sallam, K.I.; Matsa, E.; Sturzu, A.C.; et al. Human induced pluripotent stem cell-derived cardiomyocytes as an in vitro model for coxsackievirus B3-induced myocarditis and antiviral drug screening platform. Circ. Res. 2014, 115, 556–566. [Google Scholar] [CrossRef] [PubMed]
- Hirt, M.N.; Boeddinghaus, J.; Mitchell, A.; Schaaf, S.; Börnchen, C.; Müller, C.; Schulz, H.; Hubner, N.; Stenzig, J.; Stoehr, A.; et al. Functional improvement and maturation of rat and human engineered heart tissue by chronic electrical stimulation. J. Mol. Cell. Cardiol. 2014, 74, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Hirt, M.N.; Hansen, A.; Eschenhagen, T. Cardiac tissue engineering: State of the art. Circ. Res. 2014, 114, 354–367. [Google Scholar] [CrossRef] [PubMed]
- Stern, J.; Temple, S. Stem cells for retinal repair. Dev. Ophthalmol. 2014, 53, 70–80. [Google Scholar] [PubMed]
- Takasato, M.; Maier, B.; Little, M.H. Recreating kidney progenitors from pluripotent cells. Pediatr. Nephrol. 2014, 29, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Habibollah, S.; Tilgner, K.; Collin, J.; Barta, T.; Al-Aama, J.Y.; Tesarov, L.; Hussain, R.; Trafford, A.W.; Kirkwood, G.; et al. An induced pluripotent stem cell model of hypoplastic left heart syndrome (HLHS) reveals multiple expression and functional differences in HLHS-derived cardiac myocytes. Stem Cells Transl. Med. 2014, 3, 416–423. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, J.; Yoshida, M.; Tarui, S.; Hirata, M.; Nagai, Y.; Kasahara, S.; Naruse, K.; Ito, H.; Sano, S.; Oh, H. Directed differentiation of patient-specific induced pluripotent stem cells identifies the transcriptional repression and epigenetic modification of NKX2-5, HAND1, and NOTCH1 in hypoplastic left heart syndrome. PLoS ONE 2014, 9, e102796. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Francis, R.; Kim, A.J.; Ramirez, R.; Chen, G.; Subramanian, R.; Anderton, S.; Kim, Y.; Wong, L.; Morgan, J.; et al. Interrogating congenital heart defects with noninvasive fetal echocardiography in a mouse forward genetic screen. Circ. Cardiovasc. Imaging 2014, 7, 31–42. [Google Scholar] [CrossRef] [PubMed]
- Feinstein, J.A.; Benson, D.W.; Dubin, A.M.; Cohen, M.S.; Maxey, D.M.; Mahle, W.T.; Pahl, E.; Villafañe, J.; Bhatt, A.B.; Peng, L.F.; et al. Hypoplastic left heart syndrome: Current considerations and expectations. J. Am. Coll. Cardiol. 2012, 59, S1–S42. [Google Scholar] [CrossRef] [PubMed]
- Hinton, R.B., Jr.; Martin, L.J.; Tabangin, M.E.; Mazwi, M.L.; Cripe, L.H.; Benson, D.W. Hypoplastic left heart syndrome is heritable. J. Am. Coll. Cardiol. 2007, 50, 1590–1595. [Google Scholar] [CrossRef] [PubMed]
- Elliott, D.A.; Kirk, E.P.; Yeoh, T.; Chandar, S.; McKenzie, F.; Taylor, P.; Grossfeld, P.; Fatkin, D.; Jones, O.; Hayes, P.; et al. Cardiac homeobox gene NKX2-5 mutations and congenital heart disease: Associations with atrial septal defect and hypoplastic left heart syndrome. JAC 2003, 41, 2072–2076. [Google Scholar]
- Iascone, M.; Ciccone, R.; Galletti, L.; Marchetti, D.; Seddio, F.; Lincesso, A.R.; Pezzoli, L.; Vetro, A.; Barachetti, D.; Boni, L.; et al. Identification of de novo mutations and rare variants in hypoplastic left heart syndrome. Clin. Genet. 2012, 81, 542–554. [Google Scholar] [CrossRef] [PubMed]
- Freylikhman, O.; Tatarinova, T.; Smolina, N.; Zhuk, S.; Klyushina, A.; Kiselev, A.; Moiseeva, O.; Sjoberg, G.; Malashicheva, A.; Kostareva, A. Variants in the NOTCH1 gene in patients with aortic coarctation. Congenit. Heart Dis. 2014, 9, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Garg, V.; Muth, A.N.; Ransom, J.F.; Schluterman, M.K.; Barnes, R.; King, I.N.; Grossfeld, P.D.; Srivastava, D. Mutations in NOTCH1 cause aortic valve disease. Nature 2005, 437, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Hinton, R.B.; Martin, L.J.; Rame-Gowda, S.; Tabangin, M.E.; Cripe, L.H.; Benson, D.W. Hypoplastic left heart syndrome links to chromosomes 10q and 6q and is genetically related to bicuspid aortic valve. J. Am. Coll. Cardiol. 2009, 53, 1065–1071. [Google Scholar] [CrossRef] [PubMed]
- Kinnear, C.; Chang, W.Y.; Khattak, S.; Hinek, A.; Thompson, T.; de Carvalho Rodrigues, D.; Kennedy, K.; Mahmut, N.; Pasceri, P.; Stanford, W.L.; et al. Modeling and rescue of the vascular phenotype of Williams-Beuren syndrome in patient induced pluripotent stem cells. Stem Cells Transl. Med. 2013, 2, 2–15. [Google Scholar] [CrossRef] [PubMed]
- Carrier, R.L.; Papadaki, M.; Rupnick, M.; Schoen, F.J.; Bursac, N.; Langer, R.; Freed, L.E.; Vunjak-Novakovic, G. Cardiac tissue engineering: Cell seeding, cultivation parameters, and tissue construct characterization. Biotechnol. Bioeng. 1999, 64, 580–589. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, T.; Yamato, M.; Akutsu, T.; Shibata, T.; Isoi, Y.; Kikuchi, A.; Umezu, M.; Okano, T. Electrically communicating three-dimensional cardiac tissue mimic fabricated by layered cultured cardiomyocyte sheets. J. Biomed. Mater. Res. 2002, 60, 110–117. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, W.-H.; Schneiderbanger, K.; Schubert, P.; Didié, M.; Münzel, F.; Heubach, J.F.; Kostin, S.; Neuhuber, W.L.; Eschenhagen, T. Tissue engineering of a differentiated cardiac muscle construct. Circ. Res. 2002, 90, 223–230. [Google Scholar] [CrossRef] [PubMed]
- Dar, A.; Shachar, M.; Leor, J.; Cohen, S. Optimization of cardiac cell seeding and distribution in 3D porous alginate scaffolds. Biotechnol. Bioeng. 2002, 80, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Coulombe, K.L.K.; Bajpai, V.K.; Andreadis, S.T.; Murry, C.E. Heart regeneration with engineered myocardial tissue. Annu. Rev. Biomed. Eng. 2014, 16, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Dilley, R.J.; Morrison, W.A. Vascularisation to improve translational potential of tissue engineering systems for cardiac repair. Int. J. Biochem. Cell Biol. 2014, 56, 38–46. [Google Scholar] [CrossRef] [PubMed]
- Ott, H.C.; Matthiesen, T.S.; Goh, S.K.; Black, L.D.; Kren, S.M.; Netoff, T.I.; Taylor, D.A. Perfusion-decellularized matrix: Using nature’s platform to engineer a bioartificial heart. Nat. Med. 2008, 14, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Morritt, A.N.; Bortolotto, S.K.; Dilley, R.J.; Han, X.; Kompa, A.R.; McCombe, D.; Wright, C.E.; Itescu, S.; Angus, J.A.; Morrison, W.A. Cardiac tissue engineering in an in vivo vascularized chamber. Circulation 2007, 115, 353–360. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, M.; Miyagawa, S.; Miki, K.; Saito, A.; Fukushima, S.; Higuchi, T.; Kawamura, T.; Kuratani, T.; Daimon, T.; Shimizu, T.; et al. Feasibility, safety, and therapeutic efficacy of human induced pluripotent stem cell-derived cardiomyocyte sheets in a porcine ischemic cardiomyopathy model. Circulation 2012, 126, S29–S37. [Google Scholar] [CrossRef] [PubMed]
- Chong, J.J.H.; Yang, X.; Don, C.W.; Minami, E.; Liu, Y.-W.; Weyers, J.J.; Mahoney, W.M.; van Biber, B.; Cook, S.M.; Palpant, N.J.; et al. Human embryonic-stem-cell-derived cardiomyocytes regenerate non-human primate hearts. Nature 2014, 510, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Lim, S.Y.; Sivakumaran, P.; Crombie, D.E.; Dusting, G.J.; Pébay, A.; Dilley, R.J. Trichostatin A enhances differentiation of human induced pluripotent stem cells to cardiogenic cells for cardiac tissue engineering. Stem Cells Transl. Med. 2013, 2, 715–725. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, M.; Miyagawa, S.; Fukushima, S.; Saito, A.; Miki, K.; Ito, E.; Sougawa, N.; Kawamura, T.; Daimon, T.; Shimizu, T.; et al. Enhanced survival of transplanted human induced pluripotent stem cell-derived cardiomyocytes by the combination of cell sheets with the pedicled omental flap technique in a porcine heart. Circulation 2013, 128, S87–S94. [Google Scholar] [CrossRef] [PubMed]
- Emmert, M.Y.; Wolint, P.; Wickboldt, N.; Gemayel, G.; Weber, B.; Brokopp, C.E.; Boni, A.; Falk, V.; Bosman, A.; Jaconi, M.E.; et al. Human stem cell-based three-dimensional microtissues for advanced cardiac cell therapies. Biomaterials 2013, 34, 6339–6354. [Google Scholar] [CrossRef] [PubMed]
- Lu, T.-Y.; Lin, B.; Kim, J.; Sullivan, M.; Tobita, K.; Salama, G.; Yang, L. Repopulation of decellularized mouse heart with human induced pluripotent stem cell-derived cardiovascular progenitor cells. Nat. Commun. 2013, 4, 2307. [Google Scholar] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).