
Implications of Hyponatremia in Liver Transplantation

{kind=link}
{kind=link}
Abstract
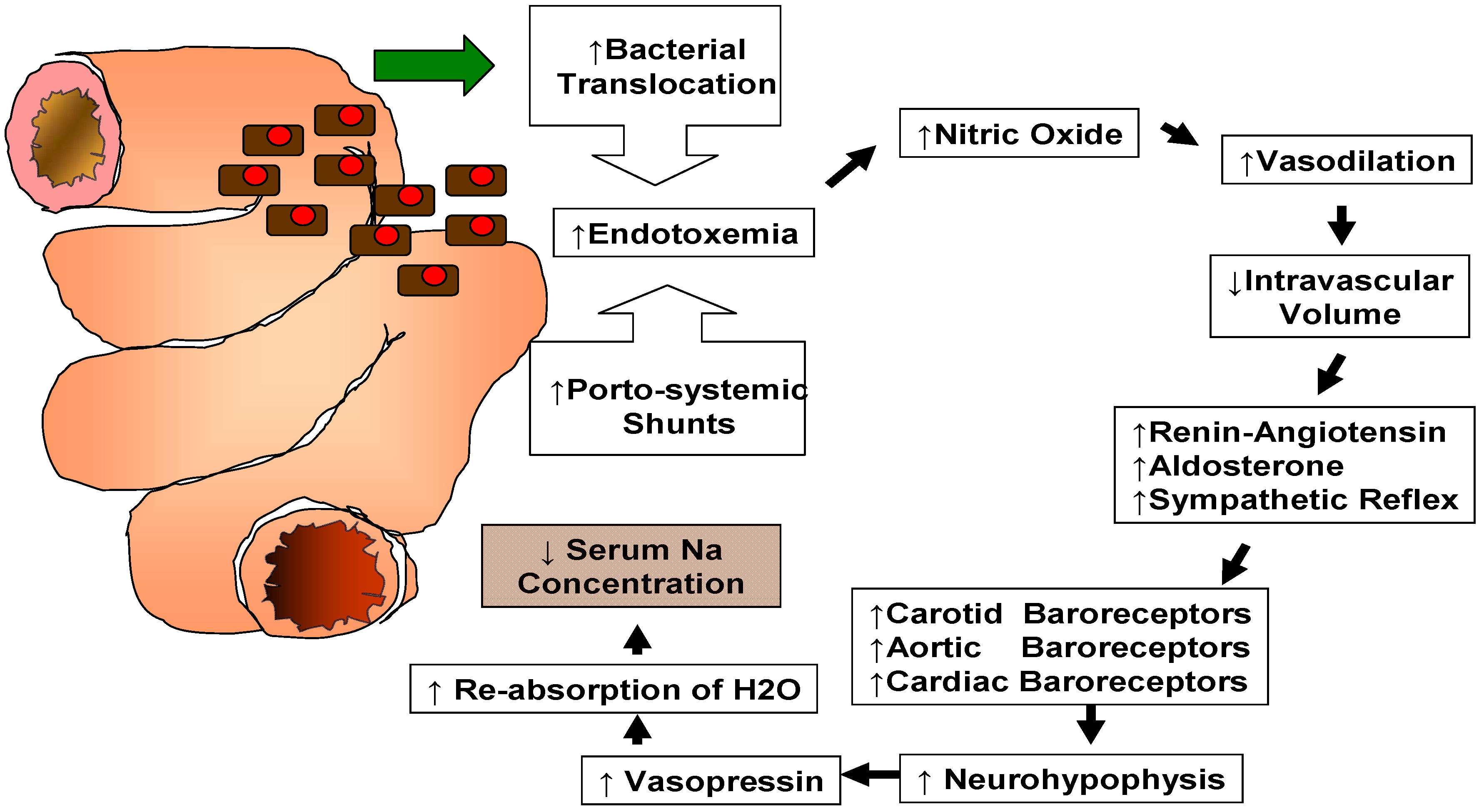
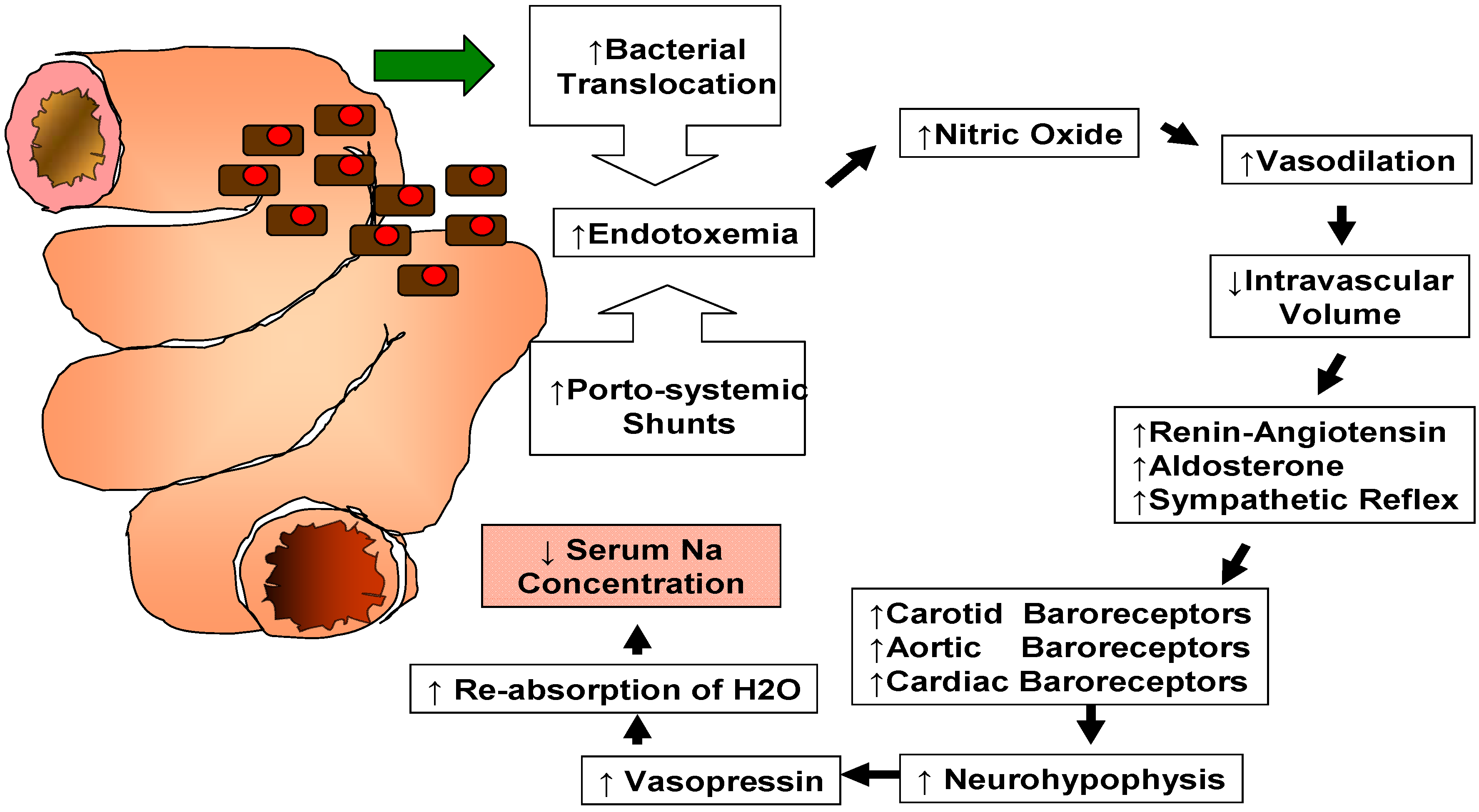
:1. Pathogenesis of Hyponatremia in Cirrhotic Patients
2. Clinical Implications
3. Predicting Mortality in Cirrhotic Patients Waiting for Liver Transplantation
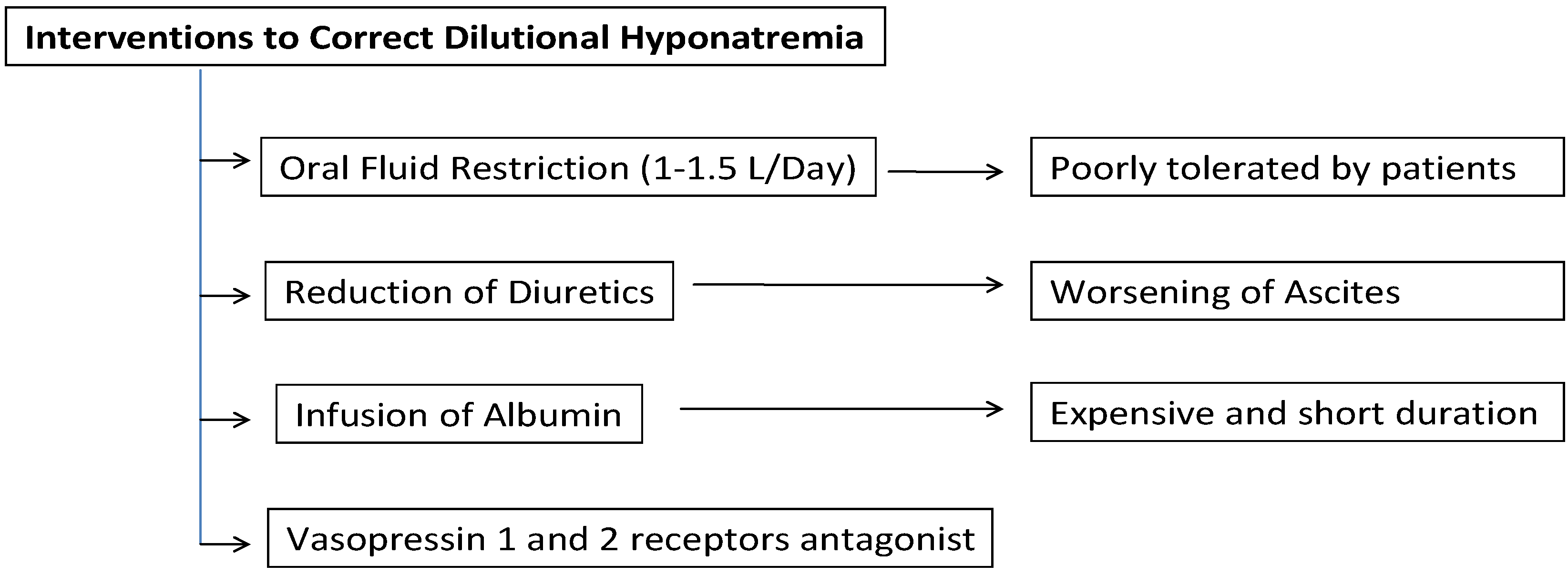
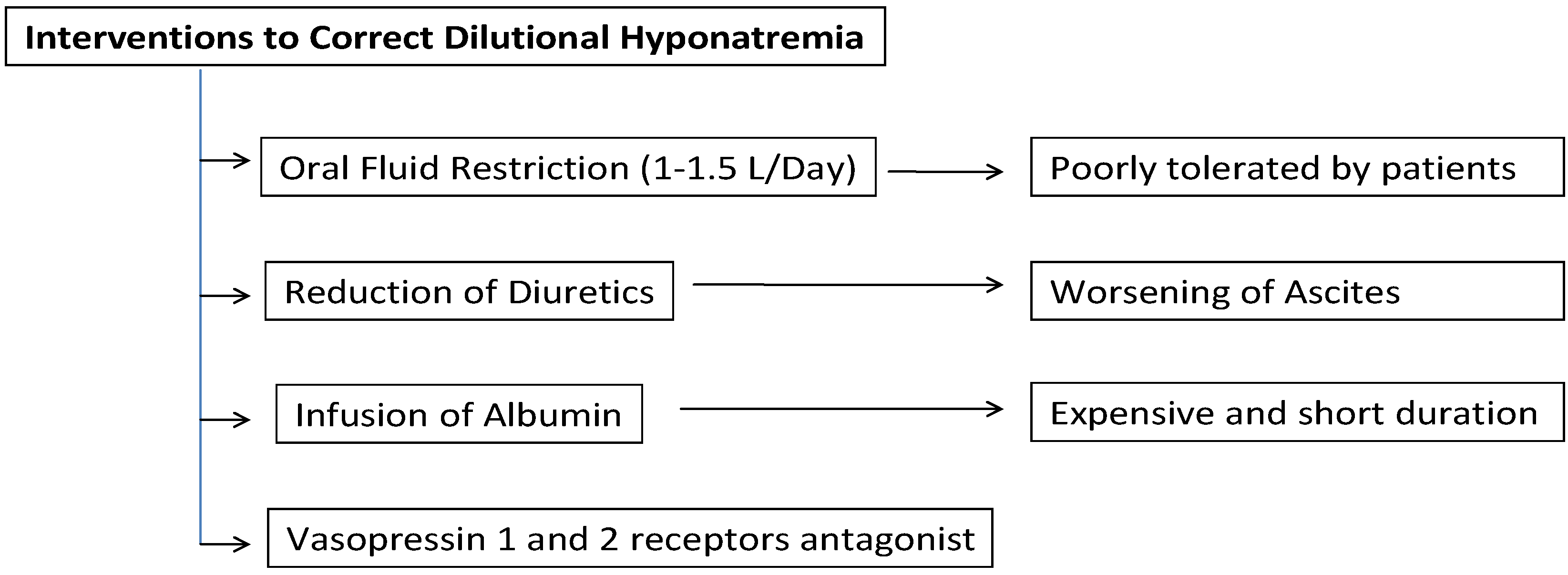
4. Pretransplant Management of Hyponatremia
5. Impact of Hyponatremia on Post-Transplant Outcomes
6. Pathophysiology of Adverse Events Associated with Hyponatremia
7. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Hackworth, W.A.; Heuman, D.M.; Sanyal, A.J.; Fisher, R.A.; Sterling, R.K.; Luketic, V.A.; Shiffman, M.L.; Maluf, D.G.; Cotterell, A.H.; Posner, M.P. Effect of hyponatraemia on outcomes following orthotopic liver transplantation. Liver Int. 2009, 29, 1071–1077. [Google Scholar] [CrossRef] [PubMed]
- Londono, M.C.; Guevara, M.; Rimola, A.; Navasa, M.; Taura, P.; Mas, A.; Garcia-Valdecasas, J.C.; Arroyo, V.; Gines, P. Hyponatremia impairs early posttransplantation outcome in patients with cirrhosis undergoing liver transplantation. Gastroenterology 2006, 130, 1135–1143. [Google Scholar] [CrossRef] [PubMed]
- Kuiper, J.J.; Boomsma, F.; van Buren, H.; de Man, R.; Danser, A.H.; van den Meiracker, A.H. Components of the renin-angiotensin-aldosterone system in plasma and ascites in hepatic cirrhosis. Eur. J. Clin. Investig. 2008, 38, 939–944. [Google Scholar] [CrossRef]
- Hecker, R.; Sherlock, S. Electrolyte and circulatory changes in terminal liver failure. Lancet 1956, 271, 1121–1125. [Google Scholar] [CrossRef] [PubMed]
- Angeli, P.; Wong, F.; Watson, H.; Gines, P. Hyponatremia in cirrhosis: Results of a patient population survey. Hepatology 2006, 44, 1535–1542. [Google Scholar] [CrossRef] [PubMed]
- Gines, A.; Escorsell, A.; Gines, P.; Salo, J.; Jimenez, W.; Inglada, L.; Navasa, M.; Claria, J.; Rimola, A.; Arroyo, V. Incidence, predictive factors, and prognosis of the hepatorenal syndrome in cirrhosis with ascites. Gastroenterology 1993, 105, 229–236. [Google Scholar] [PubMed]
- Guevara, M.; Baccaro, M.E.; Torre, A.; Gomez-Anson, B.; Rios, J.; Torres, F.; Rami, L.; Monte-Rubio, G.C.; Martin-Llahi, M.; Arroyo, V. Hyponatremia Is a Risk Factor of Hepatic Encephalopathy in Patients With Cirrhosis: A Prospective Study With Time-Dependent Analysis. Am. J. Gastroenterol. 2009, 104, 1382–1389. [Google Scholar] [CrossRef] [PubMed]
- Borroni, G.; Maggi, A.; Sangiovanni, A.; Cazzaniga, M.; Salerno, F. Clinical relevance of hyponatraemia for the hospital outcome of cirrhotic patients. Dig. Liver Dis. 2000, 32, 605–610. [Google Scholar] [CrossRef] [PubMed]
- Malinchoc, M.; Kamath, P.S.; Gordon, F.D.; Peine, C.J.; Rank, J.; ter Borg, P.C. A model to predict poor survival in patients undergoing transjugular intrahepatic portosystemic shunts. Hepatology 2000, 31, 864–871. [Google Scholar] [CrossRef] [PubMed]
- Kamath, P.S.; Kim, W.R. The model for end-stage liver disease (MELD). Hepatology 2007, 45, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Kamath, P.S.; Wiesner, R.H.; Malinchoc, M.; Kremers, W.; Therneau, T.M.; Kosberg, C.L.; D’Amico, G.; Dickson, E.R.; Kim, W.R. A model to predict survival in patients with end-stage liver disease. Hepatology 2001, 33, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Jung, G.E.; Encke, J.; Schmidt, J.; Rahmel, A. Model for end-stage liver disease. New basis of allocation for liver transplantations. Chirurg 2008, 79, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Kim, W.R.; Biggins, S.W.; Kremers, W.K.; Wiesner, R.H.; Kamath, P.S.; Benson, J.T.; Edwards, E.; Therneau, T.M. Hyponatremia and mortality among patients on the liver-transplant waiting list. N. Engl. J. Med. 2008, 359, 1018–1026. [Google Scholar] [CrossRef] [PubMed]
- Biggins, S.W.; Kim, W.R.; Terrault, N.A.; Saab, S.; Balan, V.; Schiano, T.; Benson, J.; Therneau, T.; Kremers, W.; Wiesner, R. Evidence-based incorporation of serum sodium concentration into MELD. Gastroenterology 2006, 130, 1652–1660. [Google Scholar] [CrossRef] [PubMed]
- Heuman, D.M.; Abou-Assi, S.G.; Habib, A.; Williams, L.M.; Stravitz, R.T.; Sanyal, A.J.; Fisher, R.A.; Mihas, A.A. Persistent ascites and low serum sodium identify patients with cirrhosis and low MELD scores who are at high risk for early death. Hepatology 2004, 40, 802–810. [Google Scholar] [CrossRef] [PubMed]
- Ruf, A.E.; Kremers, W.K.; Chavez, L.L.; Descalzi, V.I.; Podesta, L.G.; Villamil, F.G. Addition of serum sodium into the MELD score predicts waiting list mortality better than MELD alone. Liver Transplant. 2005, 11, 336–343. [Google Scholar] [CrossRef]
- Yamashiki, N.; Sugawara, Y.; Tamura, S.; Kaneko, J.; Nojiri, K.; Aoki, T.; Sakamoto, Y.; Hasegawa, K.; Koike, K.; Kokudo, N. Model for end-stage liver disease and model for end-stage liver disease-Na scores predict both before-listing and wait-list mortality. Transplant. Proc. 2012, 44, 389–392. [Google Scholar] [CrossRef] [PubMed]
- Moini, M.; Hoseini-Asl, M.K.; Taghavi, S.A.; Sagheb, M.M.; Nikeghbalian, S.; Salahi, H.; Bahador, A.; Motazedian, M.; Jafari, P.; Malek-Hosseini, S.A. Hyponatremia a valuable predictor of early mortality in patients with cirrhosis listed for liver transplantation. Clin. Transplant. 2011, 25, 638–645. [Google Scholar] [CrossRef] [PubMed]
- Leise, M.D.; Kim, W.R.; Kremers, W.K.; Larson, J.J.; Benson, J.T.; Therneau, T.M. A revised model for end-stage liver disease optimizes prediction of mortality among patients awaiting liver transplantation. Gastroenterology 2011, 140, 1952–1960. [Google Scholar] [CrossRef] [PubMed]
- Gines, P.; Guevara, M. Hyponatremia in cirrhosis: Pathogenesis, clinical significance, and management. Hepatology 2008, 48, 1002–1010. [Google Scholar] [CrossRef] [PubMed]
- Gines, P.; Cardenas, A. The management of ascites and hyponatremia in cirrhosis. Semin. Liver Dis. 2008, 28, 43–58. [Google Scholar] [CrossRef] [PubMed]
- Keegan, M.T.; Wright, D.R. Sodium, potassium and glucose management in organ transplantation. Curr. Opin. Organ Transplant. 2010, 15, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Shangraw, R.E. Metabolic issues in liver transplantation. Int. Anesthesiol. Clin. 2006, 44, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Wright, D.R.; Desai, D.M.; Smith, A.; Wahl, K. Severe (Uncorrected) Hyponatremia and Liver Transplantation. Liver Transplant. 2008, 14, 75–76. [Google Scholar]
- Schrier, R.W.; Gross, P.; Gheorghiade, M.; Berl, T.; Verbalis, J.G.; Czerwiec, F.S.; Orlandi, C.; SALT investigators. Tolvaptan, a selective oral vasopressin V2-receptor antagonist, for hyponatremia. N. Engl. J. Med. 2006, 355, 2099–2112. [Google Scholar]
- O’Leary, J.G.; Davis, G.L. Conivaptan increases serum sodium in hyponatremic patients with end-stage liver disease. Liver Transplant. 2009, 15, 1325–1329. [Google Scholar] [CrossRef]
- Habib, S.; Boyer, T.D. Vasopressin V2-receptor antagonists in patients with cirrhosis, ascites and hyponatremia. Therap. Adv. Gastroenterol. 2012, 5, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Neuberger, J.; Altman, D.G.; Polson, R.; Buckels, J.; Rolles, K.; Elias, E.; Calne, R.; McMaster, P.; Williams, R. Prognosis after liver transplantation for primary biliary cirrhosis. Transplantation 1989, 48, 444–447. [Google Scholar] [CrossRef] [PubMed]
- Christensen, E.; Gunson, B.; Neuberger, J. Optimal timing of liver transplantation for patients with primary biliary cirrhosis: Use of prognostic modelling. J. Hepatol. 1999, 30, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Bilbao, I.; Armadans, L.; Lazaro, J.L.; Hidalgo, E.; Castells, L.; Margarit, C. Predictive factors for early mortality following liver transplantation. Clin. Transplant. 2003, 17, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Yun, B.C.; Kim, W.R.; Benson, J.T.; Biggins, S.W.; Therneau, T.M.; Kremers, W.K.; Rosen, C.B.; Klintmalm, G.B. Impact of pretransplant hyponatremia on outcome following liver transplantation. Hepatology 2009, 49, 1610–1615. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.J.; Lee, S.K.; Jo, J.W.; Kim, S.J.; Kwon, C.H.; Park, J.W.; Han, Y.S.; Park, J.B. Prognosis after liver transplantation predicted by preoperative MELD score. Transplant. Proc. 2006, 38, 2095–2096. [Google Scholar] [CrossRef] [PubMed]
- Cywinski, J.B.; Mascha, E.; Miller, C.; Eghtesad, B.; Nakagawa, S.; Vincent, J.P.; Pesa, N.; Na, J.; Fung, J.J.; Parker, M.M. Association between donor-recipient serum sodium differences and orthotopic liver transplant graft function. Liver Transplant. 2008, 14, 59–65. [Google Scholar] [CrossRef]
- Karapanagiotou, A.; Kydona, C.; Papadopoulos, S.; Dimitriadis, C.; Giasnetsova, T.; Rempelakos, G.; Passakiotou, M.; Fouzas, I.; Papanikolaou, V.; Gritsi-Gerogianni, N. The effect of hyponatremia on the outcome of patients after orthotopic liver transplantation. Transplant. Proc. 2012, 44, 2724–2726. [Google Scholar] [CrossRef] [PubMed]
- Boin, I.F.S.F.; Capel, C.; Ataide, E.C.; Cardoso, A.R.; Caruy, C.A.; Stucchi, R.S.B. Pretransplant Hyponatremia Could Be Associated With a Poor Prognosis After Liver Transplantation. Transplant. Proc. 2010, 42, 4119–4122. [Google Scholar] [CrossRef] [PubMed]
- Dawwas, M.F.; Lewsey, J.D.; Neuberger, J.M.; Gimson, A.E. The impact of serum sodium concentration on mortality after liver transplantation: A cohort multicenter study. Liver Transplant. 2007, 13, 1115–1124. [Google Scholar] [CrossRef]
- Fukuhara, T.; Ikegami, T.; Morita, K.; Umeda, K.; Ueda, S.; Nagata, S.; Sugimachi, K.; Gion, T.; Soejima, Y. Impact of preoperative serum sodium concentration in living donor liver transplantation. J. Gastroenterol. Hepatol. 2010, 25, 978–984. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.M.; Kang, J.K.; Yun, S.C.; Kim, K.H.; Kim, S.J.; Hwang, K.S.; Lee, S.G. Risk factors for central pontine and extrapontine myelinolysis following orthotopic liver transplantation. Eur. Neurol. 2009, 62, 362–368. [Google Scholar] [CrossRef] [PubMed]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cimen, S.; Guler, S.; Ayloo, S.; Molinari, M. Implications of Hyponatremia in Liver Transplantation. J. Clin. Med. 2015, 4, 66-74. https://doi.org/10.3390/jcm4010066
Cimen S, Guler S, Ayloo S, Molinari M. Implications of Hyponatremia in Liver Transplantation. Journal of Clinical Medicine. 2015; 4(1):66-74. https://doi.org/10.3390/jcm4010066
Chicago/Turabian StyleCimen, Sertac, Sanem Guler, Subhashini Ayloo, and Michele Molinari. 2015. "Implications of Hyponatremia in Liver Transplantation" Journal of Clinical Medicine 4, no. 1: 66-74. https://doi.org/10.3390/jcm4010066
APA StyleCimen, S., Guler, S., Ayloo, S., & Molinari, M. (2015). Implications of Hyponatremia in Liver Transplantation. Journal of Clinical Medicine, 4(1), 66-74. https://doi.org/10.3390/jcm4010066