Pediatric Bipolar Disorder: Subtype Trend and Impact of Behavioral Comorbidities

Abstract
:
1. Introduction
2. Methods
2.1. Data Source and Survey Design
2.2. Study Variables
2.2.1. Demographic, Visit and Prescribing Characteristics
2.2.2. Diagnosis
2.2.3. Psychotropic Medications
2.3. Analytical Plan
3. Results
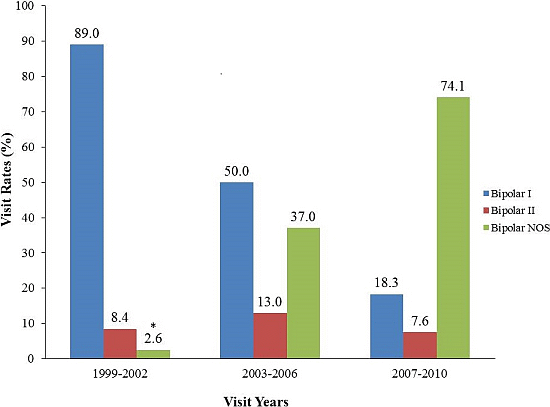
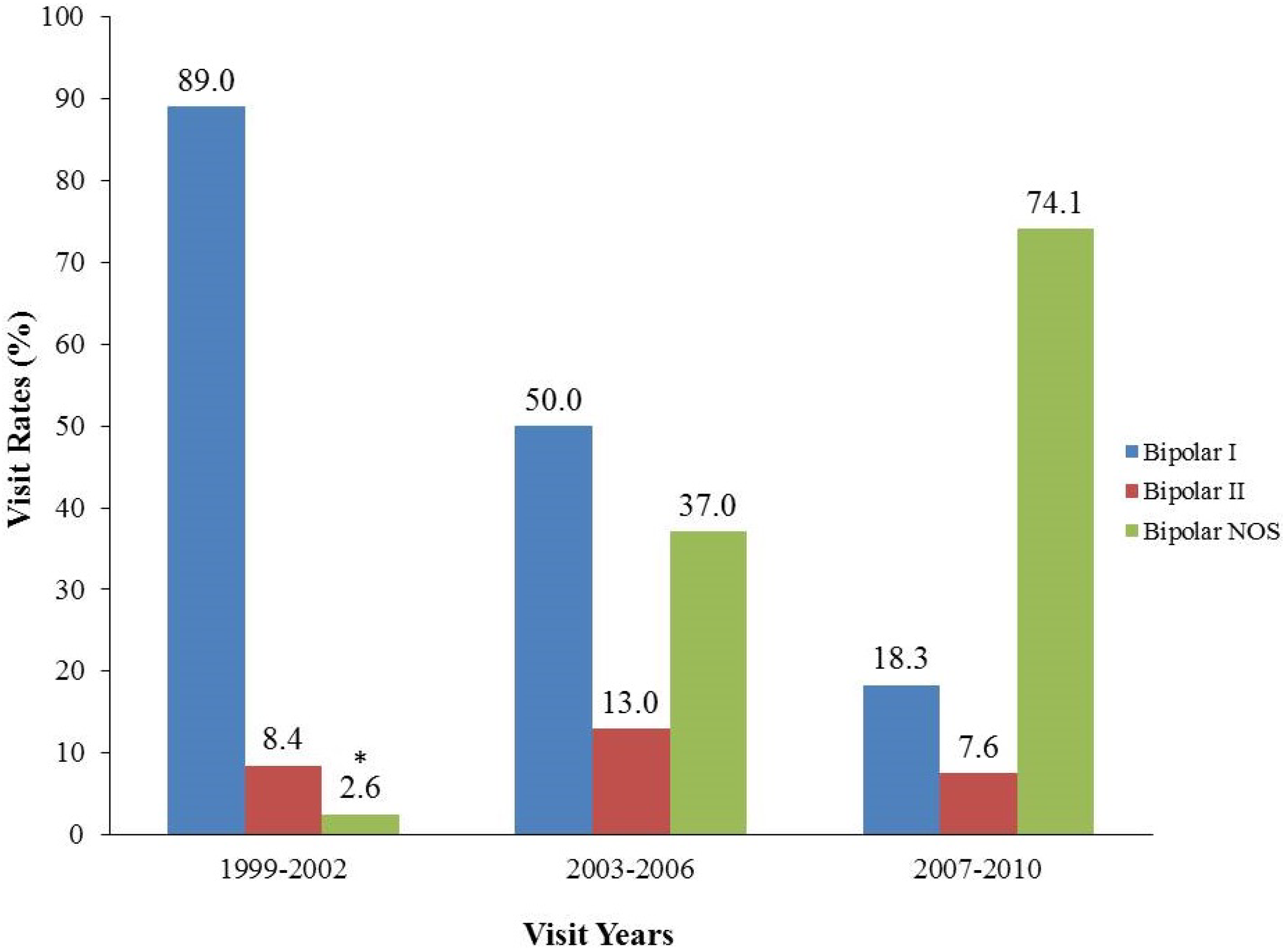
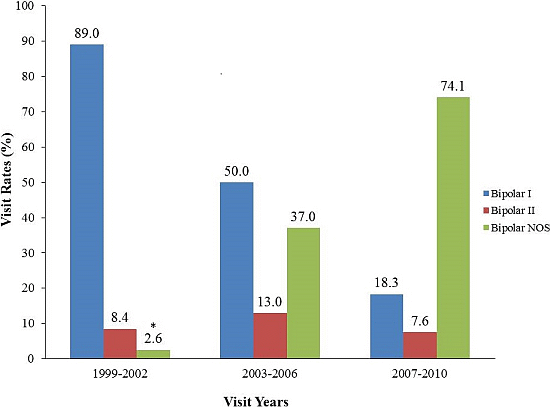
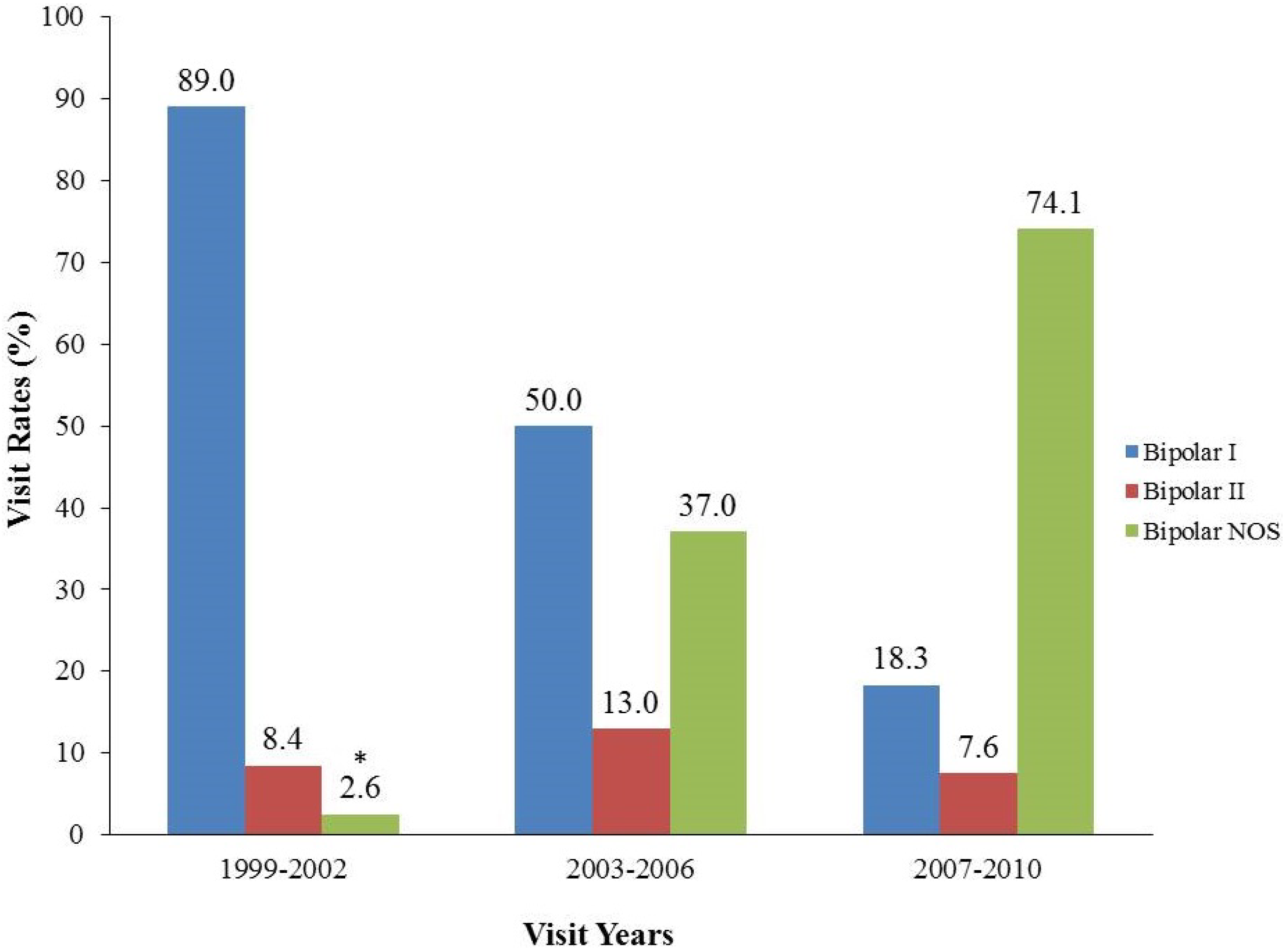
3.1. Recent Trends in PBD Office Visits, PBD Subtypes and Antipsychotic Medication Regimens

{kind=link}
{kind=link}
{kind=link}
| Characteristic | PBD with behavioral comorbidities | PBD without behavioral comorbidities | |||
|---|---|---|---|---|---|
| N | WC% | N | WC% | p Value | |
| Total | 162 | 156 | |||
| Bipolar NOS | 96 | 60.8 | 68 | 45.3 | 0.02 |
| Bipolar I & II | 66 | 39.2 | 88 | 54.7 | |
| Gender | |||||
| Male | 119 | 69.7 | 73 | 46.5 | <0.001 |
| Female | 43 | 30.3 | 83 | 53.5 | |
| Age group, years | |||||
| 2–9 | 36 | 19.1 | 13 | 7.5 | <0.0001 |
| 10–14 | 70 | 46.1 | 39 | 24.0 | |
| 15–19 | 56 | 34.8 | 104 | 68.5 | |
| Race/Ethnicity | |||||
| White | 131 | 82.9 | 126 | 81.6 | NS |
| Non-White | 31 | 17.2 | 30 | 18.4 | |
| Payment type | |||||
| Private | 71 | 45.0 | 91 | 60.5 | 0.03 |
| Public | 91 | 55.0 | 65 | 39.6 | |
| Type of Practice | |||||
| Psychiatry | 148 | 85.1 | 132 | 75.3 | NS |
| Non-Psychiatry | 14 † | 14.9 | 24 † | 24.7 | |
| Region | |||||
| North-East | 23 † | 13.6 | 37 | 12.2 | NS |
| Mid-West | 54 | 27.9 | 35 | 13.1 | |
| South | 38 | 30.9 | 36 | 13.8 | |
| West | 47 | 27.6 | 48 | 14.8 | |
| Prescribed psychotropic medications | |||||
| Any psychotropic visit | 151 | 94.6 | 147 | 92.8 | NS |
| Antipsychotics | 105 | 59.6 | 97 | 61.3 | NS |
| Antidepressants | 39 | 21.0 | 65 | 41.6 | 0.001 |
| Anxiolytics & Hypnotics | 6 † | 3.4 | 15 † | 11.5 | 0.01 |
| Lithium | 17 † | 9.7 | 17 † | 9.7 | NS |
| Alpha-agonist | 16 † | 8.3 | 5 † | 3.6 | NS |
| Anticonvulsant | 68 | 44.7 | 66 | 40.2 | NS |
| Stimulants | 104 | 67.8 | 14 † | 9.4 | <0.0001 |
| PBD with behavioral comorbidities | PBD without behavioral comorbidities | ||||
|---|---|---|---|---|---|
| ATP regimens | N | WC% | N | WC% | p Value |
| ATP monotherapy | 10 † | 4.2 | 29 † | 19.7 | <0.001 |
| ATP + ≥1 concomitant psychotropic classes | 95 | 41.2 | 68 | 34.9 | |
| ATP + concomitant stimulant | 72 | 19.5 | 8 † | 2.7 | <0.0001 |
| ATP + concomitant ATC-MS | 38 | 10.4 | 38 | 12.2 | NS |
| ATP + concomitant ATD | 28 † | 7.2 | 36 | 12.2 | NS |
3.2. Multivariable Analyses
| Variable | AOR | 95% CI |
|---|---|---|
| Diagnosis (reference: Bipolar I & II) | ||
| Bipolar NOS | 2.3 | 1.3–4.1 |
| Gender (reference: female) | ||
| Male | 2.3 | 1.3–4.0 |
| Age group (reference: 15–19 years) | ||
| 2–9 years | 5.3 | 2.7–10.6 |
| 10–14 years | 3.7 | 1.8–7.4 |
| Race-ethnicity (reference: white) | ||
| Non white | 0.6 | 0.3–1.3 |
| Payment (reference: public) | ||
| Private | 0.6 | 0.3–1.0 |
4. Discussion
4.1. Limitations
4.2. Future Research and Practice Directions
5. Conclusions
Conflicts of Interest
References
- Birmaher, B.; Axelson, D.; Goldstein, B.; Strober, M.; Gill, M.K.; Hunt, J.; Houck, P.; Ha, W.; Iyengar, S.; Kim, E.; et al. Four-year longitudinal course of children and adolescents with bipolar spectrum disorders: The Course and Outcome of Bipolar Youth (COBY) study. Am. J. Psychiatry 2009, 166, 795–804. [Google Scholar] [CrossRef]
- Blader, J.C.; Carlson, G.A. Increased rates of bipolar disorder diagnoses among U.S. child, adolescent, and adult inpatients, 1996–2004. Biol. Psychiatry 2007, 62, 107–114. [Google Scholar] [CrossRef]
- Moreno, C.L.; Blanco, C.; Jiang, H.; Schmidt, A.B.; Olfson, M. National trends in the outpatient diagnosis and treatment of bipolar disorder in youth. Arch. Gen. Psychiatry 2007, 64, 1032–1039. [Google Scholar] [CrossRef]
- Parens, E.; Johnston, J. Controversies concerning the diagnosis and treatment of bipolar disorder in children. Child. Adolesc. Psychiatry Ment. Health 2010, 4. [Google Scholar] [CrossRef]
- Kent, L.; Craddock, N. Is there a relationship between attention deficit hyperactivity disorder and bipolar disorder? J. Affect. Disord. 2003, 73, 211–221. [Google Scholar] [CrossRef]
- Milberger, S.; Biederman, J.; Faraone, S.V.; Murphy, J.; Tsuang, M.T. Attention deficit hyperactivity disorder and comorbid disorders: Issues of overlapping symptoms. Am. J. Psychiatry 1995, 152, 1793–1799. [Google Scholar]
- Dusetzina, S.B.; Weinberger, M.; Gaynes, B.N.; Farley, J.F.; Sleath, B.; Hansen, R.A. Prevalence of bipolar disorder diagnoses and psychotropic drug therapy among privately insured children and adolescents. Pharmacotherapy 2012, 32, 1085–1094. [Google Scholar] [CrossRef]
- Crystal, S.; Olfson, M.; Huang, C.; Pincus, H.; Gerhard, T. Broadened use of atypical antipsychotics: Safety, effectiveness, and policy challenges. Health Aff. 2009, 28, 770–781. [Google Scholar] [CrossRef]
- Zito, J.M.; Burcu, M.; Ibe, A.; Safer, D.J.; Magder, L.S. Antipsychotic use by Medicaid-insured youths: Impact of eligibility and psychiatric diagnosis across a decade. Psychiatr. Serv. 2013, 64, 223–229. [Google Scholar]
- Comer, J.S.; Olfson, M.; Mojtabai, R. National trends in child and adolescent psychotropic polypharmacy in office-based practice, 1996–2007. J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 1001–1010. [Google Scholar] [CrossRef]
- Dziegielewski, S.F. DSM-IV-TR in Action; John Wiley & Sons: New York, NY, USA, 2002; pp. 52–55. [Google Scholar]
- Turner, S.; Nunn, A.J.; Choonara, I. Unlicensed drug use in children in the UK. Int. J. Pharm. Pharm. Available online: http://www.priory.com/pharmol/uduiciuk.htm (accessed on 10 December 2013).
- National Center for Health Statistics. National Ambulatory Medical Care Survey. Available online: http://www.cdc.gov/nchs/ahcd/about_ahcd.htm (accessed on 10 December 2013).
- National Center for Health Statistics. NAMCS Estimation Procedures. Available online: http://www.cdc.gov/nchs/ahcd/ahcd_estimation_procedures.htm (accessed on 10 December 2013).
- Kessler, R.C.; Avenevoli, S.; Green, J.; Gruber, M.J.; Guyer, M.; He, Y.; Jin, R.; Kaufman, J.; Sampson, N.A.; Zaslavsky, A.M. National comorbidity survey replication adolescent supplement (NCS-A): III. Concordance of DSM-IV/CIDI diagnoses with clinical reassessments. J. Am. Acad. Child Adolesc. Psychiatry 2009, 48, 386–399. [Google Scholar] [CrossRef]
- Findling, R.L.; Youngstrom, E.A.; Fristad, M.A.; Birmaher, B.; Kowatch, R.A.; Arnold, L.E.; Frazier, T.W.; Axelson, D.; Ryan, N.; Demeter, C.; et al. Characteristics of children with elevated symptoms of mania: The Longitudinal Assessment of Manic Symptoms (LAMS) study. J. Clin. Psychiatry 2010, 71, 1664–1672. [Google Scholar] [CrossRef]
- Youngstrom, E.; Youngstrom, J.; Algorta, G.P.; Fine, E.M. Pediatric bipolar disorder and mixed mood symptoms: Moderately prevalent in community mental health and underdiagnosed by practitioners. Neuropsychopharmacol 2012, 38, 399–400. [Google Scholar]
- Stringaris, A.; Santosh, P.; Leibenluft, E.; Goodman, R. Youth meeting symptom and impairment criteria for mania-like episodes lasting less than four days: An epidemiological enquiry. J. Child Psychol. Psychiatry 2009, 51, 31–38. [Google Scholar]
- Geller, B.; Craney, J.L.; Bolhofner, K.; DelBello, M.P.; Williams, M.; Zimmerman, B. One-year recovery and relapse rates of children with a prepubertal and early adolescent bipolar disorder phenotype. Am. J. Psychiatry 2001, 158, 303–305. [Google Scholar] [CrossRef]
- National Institute of Mental Health. Bipolar Disorder Research at the National Institute of Mental Health. Available online: http://www.nimh.nih.gov/publicat/bipolarresfact.cfm (accessed on 31 August 2002).
- National Institute of Mental Health. National Institute of Mental Health research roundtable on prepubertal bipolar disorder. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 871–878. [Google Scholar] [CrossRef]
- Olfson, M.; Crystal, S.; Gerhard, T.; Huang, C.S.; Carlson, G.A. Mental health treatment received by youths in the year before and after a new diagnosis of bipolar disorder. Psychiatr. Serv. 2009, 60, 1098–1106. [Google Scholar]
- Holtmann, M.; Bolte, S.; Poustka, F. Rapid increase in rates of bipolar diagnosis in youth: “True” bipolarity or misdiagnosed severe disruptive behavior disorders? Arch. Gen. Psychiatry 2008, 65. [Google Scholar] [CrossRef]
- Grohol, J. Temper dysregulation disorder with dysphoria. Available online: http://psychcentral.com/lib/temper-dysregulation-disorder-with-dysphoria/0002892 (accessed on 26 September 2013).
- Pataki, C.; Carlson, G.A. The comorbidity of ADHD and bipolar disorder: Any less confusion? Curr. Psychiatry Rep. 2013, 15. [Google Scholar] [CrossRef]
- Carucci, S.; Atzori, P.; Alia, C.; Danjou, F.; Zuddas, A. Phenomenology and 24 month treatment outcome of pediatric bipolar disorder (Poster). Eur. Neuropsychopharmacol. 2010, 20, 90–91. [Google Scholar] [CrossRef]
- Weber, N.S.; Fisher, J.A.; Cowan, D.N.; Niebuhr, D.W. Psychiatric and general medical conditions comorbid with bipolar disorder in the National Hospital Discharge Survey. Psychiatr. Serv. 2011, 62, 1152–1158. [Google Scholar]
- Miller, S.; Chang, K.D.; Ketter, T.A. Bipolar disorder and attention-deficit/hyperactivity disorder comorbidity in children and adolescents: Evidence-based approach to diagnosis and treatment. J. Clin. Psychiatry 2013, 74, 628–629. [Google Scholar] [CrossRef]
- Bhangoo, R.K.; Lowe, C.H.; Myers, F.S.; Treland, J.; Curran, J.; Towbin, K.E.; Leibenluft, E. Medication use in children and adolescents treated in the community for bipolar disorder. J. Child Adolesc. Psychopharmacol. 2003, 13, 515–522. [Google Scholar] [CrossRef]
- Bhowmik, D.; Aparasu, R.R.; Rajan, S.S.; Sherer, J.T.; Ochoa-Perez, M.; Chen, H. The utilization of psychopharmacological treatment and medication adherence among Medicaid enrolled children and adolescents with bipolar depression. J. Affect. Disord. 2013, 150, 424–429. [Google Scholar] [CrossRef]
- Zito, J.M. Pharmacoepidemiology: Recent findings and challenges for child and adolescent psychopharmacology (commentary). J. Clin. Psychiatry 2007, 68, 966–967. [Google Scholar] [CrossRef]
- Correll, C.U. Clinical psychopharmacology of pediatric mood stabilizer and antipsychotic treatment, Part 1: Challenges and developments (commentary). J. Clin. Psychiatry 2007, 68, 1301–1302. [Google Scholar] [CrossRef]
- Wagner, W.D.; Weller, E.B.; Carlson, G.A.; Sachs, G.; Biederman, J.; Frazier, J.A.; Wozniak, P.; Tracy, K.; Weller, R.A.; Bowden, C. An open-label trial of divalproex in children and adolescents with bipolar disorder. J. Am. Acad. Child Adolesc. Psychiatry 2002, 41, 1224–1230. [Google Scholar] [CrossRef]
- West, A.E.; Weinstein, S.M.; Celio, C.I.; Henry, D.; Pavuluri, M.N. Co-morbid disruptive behavior disorder and aggression predict functional outcomes and differential response to risperidone versus divalproex in pharmacotherapy for pediatric bipolar disorder. J. Child Adolesc. Psychopharmacol. 2011, 21, 545–553. [Google Scholar] [CrossRef]
- Yanofski, J. The dopamine dilemma: Using stimulants and antipsychotics concurrently. Psychiatry (Edgmont) 2010, 7, 18–23. [Google Scholar]
- American Academy of Child and Adolescent Psychiatry. Practice parameter for the assessment and treatment of children and adolescents with bipolar disorder. J. Am. Acad. Child Adolesc. Psychiatry 2004, 46, 107–125. [Google Scholar]
- ito, J.M.; Derivan, A.T.; Kratochvil, C.J.; Safer, D.J.; Fegert, J.M.; Greenhill, L.L. Off-label psychopharmacologic prescribing for children: History supports close clinical monitoring. Child Adolesc. Psychiatry Ment. Health 2008, 2. [Google Scholar] [CrossRef]
- Friedman, A.R. A dry pipeline for psychiatric drugs. New York Times. Available online: http://www.nytimes.com/2013/08/20/health/a-dry-pipeline-for-psychiatric-drugs.html?_r=0 (accessed on 20 August 2013).
- Duke Evidence Synthesis Group. Future research prioritization: Bipolar disorder and antipsychotic use in adolescents and young adults. Unpublished work. 2013. [Google Scholar]
- Shah, E.H.; Galanter, C.A.; Zito, J.M. AACAP’s toolbox for clinical practice and outcomes: A resource for practicing clinicians and trainees. AACAP News 2013, 44, 242–243. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Rajakannan, T.; Zito, J.M.; Burcu, M.; Safer, D.J. Pediatric Bipolar Disorder: Subtype Trend and Impact of Behavioral Comorbidities. J. Clin. Med. 2014, 3, 310-322. https://doi.org/10.3390/jcm3010310
Rajakannan T, Zito JM, Burcu M, Safer DJ. Pediatric Bipolar Disorder: Subtype Trend and Impact of Behavioral Comorbidities. Journal of Clinical Medicine. 2014; 3(1):310-322. https://doi.org/10.3390/jcm3010310
Chicago/Turabian StyleRajakannan, Thiyagu, Julie M. Zito, Mehmet Burcu, and Daniel J. Safer. 2014. "Pediatric Bipolar Disorder: Subtype Trend and Impact of Behavioral Comorbidities" Journal of Clinical Medicine 3, no. 1: 310-322. https://doi.org/10.3390/jcm3010310
APA StyleRajakannan, T., Zito, J. M., Burcu, M., & Safer, D. J. (2014). Pediatric Bipolar Disorder: Subtype Trend and Impact of Behavioral Comorbidities. Journal of Clinical Medicine, 3(1), 310-322. https://doi.org/10.3390/jcm3010310