
Use of External Fixator Device for Mandible Fracture Related to War Injury: A Systematic Review

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Protocol
2.2. Search Strategies
2.3. Eligibility Criteria
2.4. Study Selection
2.5. Data Extraction and Analysis
2.6. Risk of Bias
3. Results
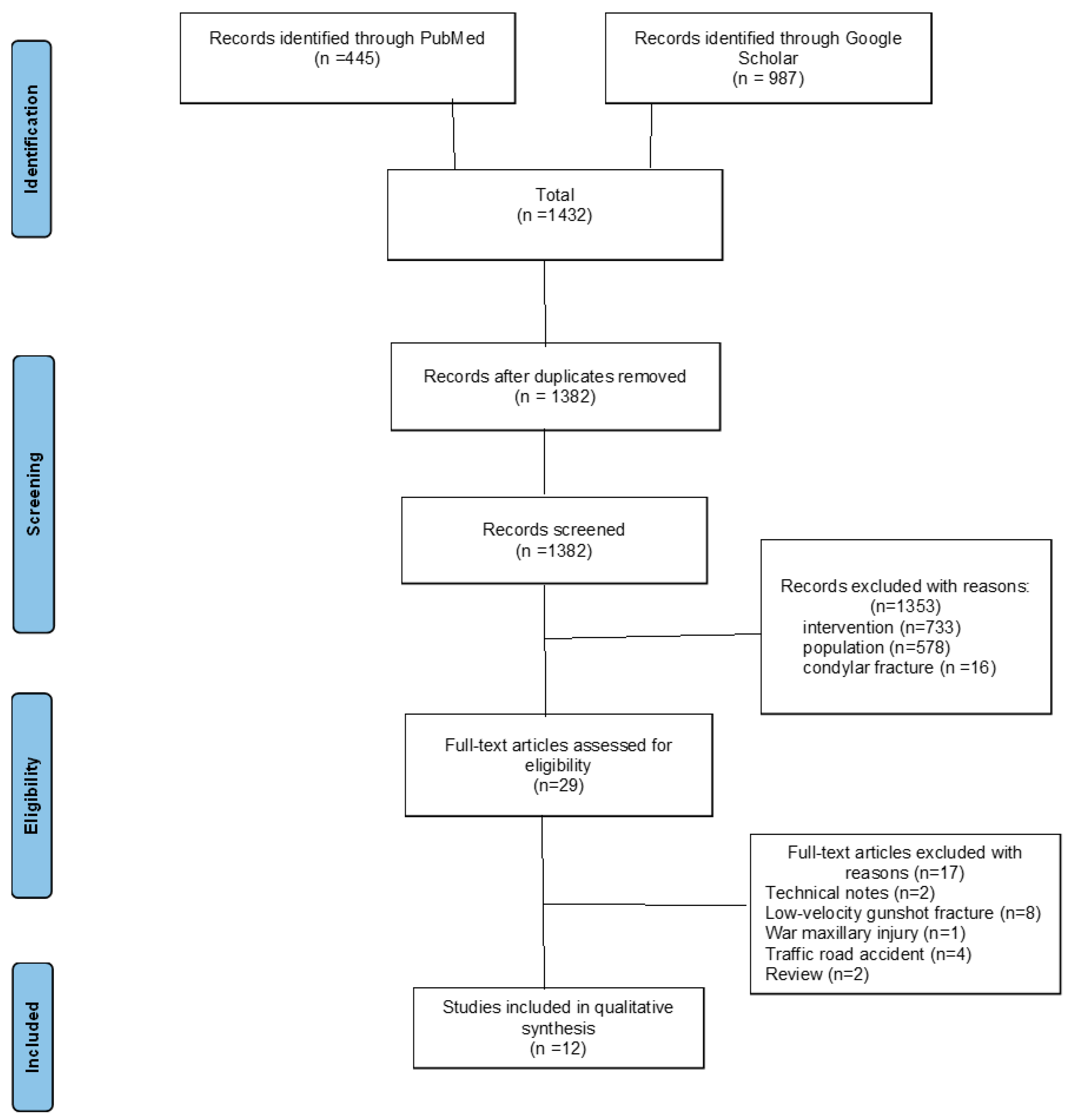
3.1. Study Selections
3.2. Study Characteristics

{kind=link}
| Authors (Year) | Study Design | Country | N. Patients | Type of External Fixator | Mechanism | Indication | Fracture Details | Outcome | Complications |
|---|---|---|---|---|---|---|---|---|---|
| Gibbons, 2011 [33] | Case report | UK | 1 | Custom II | High-velocity bullet | Definitive | Comminuted fracture | Bone healing, correct occlusion | None |
| Carvalho, 2019 [14] | Case series | NA | 3 | Orthopedic wrist | High-velocity bullet | 2 Definitive, 1 Initial | Comminuted, 1 w/bone loss | Functional recovery, aesthetics restored | None |
| Zorman, 1990 [34] | Case series | NA | 4 | Orthopedic (Hoffman) | Missile injury | NA | NA | Good/excellent result | NA |
| Mc Millian, 2016 [30] | Case report | NA | 1 | NA | Explosive device | Definitive | Comminuted, large soft tissue defect | Excellent | None |
| Breeze, 2016 [28] | Case report | NA | 1 | NA | High-velocity bullet | Definitive | Comminuted, soft tissue maceration | Successful | Not reported |
| Elbir, 2023 [6] | Case series | Libya | 2 | Custom II | High-velocity bullet | Initial | Multifragmented | NA | None |
| Mc Veigh, 2010 [23] | Case series | UK | 3 | Custom II | Explosive device | Definitive | Comminuted, periosteal damage | Primary bone healing | NA |
| Marti-Flich, 2020 [5] | Retrospective cohort | France | 24 | Self-crafted | High-velocity bullet | 5 Definitive, 19 Initial | NA | NA | Non-union (2 cases) |
| Venugopal 2011 [32] | Retrospective cohort | NA | 10 | NA | Explosive device | 8 Definitive, 2 Initial | Comminuted | NA | NA |
| Maghalaes, 2020 [13] | Case report | NA | 1 | Orthopedic | High-velocity bullet | Definitive | Comminuted w/infection | Function and contour preserved | None |
| Breeze, 2011 [27] | Retrospective cohort | UK | 22 | NA | Explosive device | Definitive | NA | NA | NA |
| Ellis, 2003 [2] | Retrospective cohort | NA | 17 | NA | High-velocity bullet | NA | Comminuted | NA | Non-union (4 cases 23.5%) |
| Authors (Year) | Follow-Up/Duration of External Fixator (Week) | Associated Bone Treatment | Associated Soft Tissue Treatment |
|---|---|---|---|
| Gibbon, 2011 [33] | 7 weeks | NA | NA |
| Carvalho 2019 [14] | 14 weeks | Osteochondral bone graft and reconstruction with plate and screw: 1 patient | |
| Zorman, 1990 [34] | NA | NA | NA |
| McMillian, 2016 [30] | NA | NA | NA |
| Breeze, 2019 [28] | NA | Iliac bone graft | NA |
| Elbir, 2023 [6] | 8 weeks (2 months) | Iliac bone graft and reconstruction plate | NA |
| Mc Veigh, 2010 [23] | NA | Miniplate osteosynthesis of substantial dentoalveolar fragments | NA |
| Marti-Flich, 2020 [5] | NA | NA | NA |
| Venugopal, 2011 [32] | 24 months of follow-up | NA | NA |
| Maghalaes, 2020 [13] | NA | no | Intraoral and extraoral wound healed in second intention |
| Breeze, 2011 [27] | NA | NA | NA |
| Ellis, 2003 [2] | NA | NA | NA |
3.3. External Fixator Device Available
3.4. Outcome and Fracture Union Duration
3.5. Complications
Quality Assessment of Studies
4. Discussion
Strength and Study Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| IMF | Intermaxillary fixation |
| ORIF | Open reduction and internal fixation |
| MMF | Maxillomandibular fixation |
| NA | Not available |
| UK | United Kingdom |
| NOS | Newcastle–Ottawa Scale |
| EF | External fixation |
References
- Kazi, A.A.; Lee, T.S.; Vincent, A.; Sokoya, M.; Sheen, D.; Ducic, Y. The role of external fixation in trauma and reconstruction of the mandible in the age of rigid fixation. Facial Plast. Surg. 2019, 35, 614–622. [Google Scholar] [CrossRef] [PubMed]
- Ellis, E., 3rd; Muniz, O.; Anand, K. Treatment considerations for comminuted mandibular fractures. J. Oral Maxillofac. Surg. 2003, 61, 861–870. [Google Scholar] [CrossRef] [PubMed]
- Chrcanovic, B.R. Open versus closed reduction: Comminuted mandibular fractures. Oral Maxillofac. Surg. 2013, 17, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Fleming, I.D.; Morris, J.H. Use of acrylic external splint after mandibular resection. Am. J. Surg. 1969, 118, 708–711. [Google Scholar] [CrossRef]
- Marti-Flich, L.; Schlund, M.; Raoul, G.; Maes, J.-M.; Ferri, J.; Wojcik, T.; Nicot, R. Twenty-four years of experience in management of complex mandibular fractures with low cost, custom-made mandibular external fixation: A 65-patient series. J. Stomatol. Oral Maxillofac. Surg. 2020, 121, 242–247. [Google Scholar] [CrossRef]
- Elbir, B.; Kolsuz, N.; Varol, A. External mandibular fixation for gunshot fractures: Report of 2 cases. Ulus. Travma. Acil. Cerrahi. Derg. 2023, 29, 741–745. [Google Scholar] [CrossRef]
- Torres, L.H.S.; Uchoa, C.P.; Cavalcante, M.B.; Jardim, V.B.F.; Rodrigues, É.D.R.; Pereira, R.V.S.; Côvre, L.M.; do Egito Vasconcelos, B.C.; e Silva, E.D.D.O.; Pereira Filho, V.A. Colles external fixator as alternative in comminuted mandibular fractures treatment. Res. Soc. Dev. 2020, 9, e1879108030. [Google Scholar] [CrossRef]
- Cornelius, C.-P.; Augustin, J.B.; Sailer, L.-K. External pin fixation for stabilization of the mandible—Comeback of a method: Historical review and first experiences with the ‘mandible external fixator’. Oral Maxillofac. Surg. 2009, 13, 1–14. [Google Scholar] [CrossRef]
- Braidy, H.F.; Ziccardi, V.B. External fixation for mandible fractures. Atlas Oral Maxillofac. Surg. Clin. 2009, 17, 45–53. [Google Scholar] [CrossRef]
- Holmes, S.; Hardee, P.; Anand, P. Use of an orthopaedic fixator for external fixation of the mandible. Br. J. Oral Maxillofac. Surg. 2002, 40, 238–240. [Google Scholar] [CrossRef]
- de Alencar, M.G.M.; De Bortoli, M.M.; da Silva, T.C.G.; e Silva, E.D.d.O.; Laureano Filho, J.R. Suitability of wrist external fixator for treatment of mandibular fracture. J. Craniofacial Surg. 2018, 29, e371–e372. [Google Scholar] [CrossRef] [PubMed]
- Alpert, B.; Tiwana, P.S.; Kushner, G.M. Management of comminuted fractures of the mandible. Oral Maxillofac. Surg. Clin. N. Am. 2009, 21, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Magalhães, G.P.; de Carvalho, M.L.; Ingryd, J.; de Sousa, T.; dos Santos, J.Z.L.V. Mandibula Fracture by Fire Weapon Projectile: Surgical Treatment Through the Use of External Fixers: Case Report. IOSR J. Dent. Med. Sci. (IOSR-JDMS) 2020, 19, 1–4. [Google Scholar]
- Carvalho, P.H.R.; da Hora Sales, P.H.; da Rocha, S.S.; Cavalcanti, A.M.M.; de Jesus Rodrigues Mello, M.; Junior, J.M.S.M. Treatment of comminutive fractures by firearm projectiles with adapted wrist external fixator. Oral Maxillofac. Surg. 2019, 23, 501–505. [Google Scholar] [CrossRef]
- Barreda Hale, M.; Romero-Araya, P.; Cea Herrera, M.; Espinoza, D.; Castro, N.; Castro, J.; Serandour, G. Computer-assisted planning with 3D printing for mandibular reconstruction caused by a mandibular fracture with secondary osteomyelitis: A Case Report. Clin. Case Rep. 2021, 9, e04410. [Google Scholar] [CrossRef]
- Mahdian, N.; Onderková, A.; Brizman, E.; Pavlíková, G.; Vlachopulos, V.; Drahoš, M.; Foltán, R. External fixation greatly improves outcomes in the surgical treatment of osteoradionecrosis of the jaws without affecting quality of life: A five-year retrospective study. Br. J. Oral Maxillofac. Surg. 2020, 58, e45–e50. [Google Scholar] [CrossRef]
- Cascone, P.; Spallaccia, F.; Arangio, P.; Vellone, V.; Gualtieri, M. A modified external fixator system in treatment of mandibular condylar fractures. J. Craniofacial Surg. 2017, 28, 1230–1235. [Google Scholar] [CrossRef]
- Iannetti, G.; Cascone, P. Use of rigid external fixation in fractures of the mandibular condyle. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1995, 80, 394–397. [Google Scholar] [CrossRef]
- Cascone, P.; Marcozzi, M.M.; Ramieri, V.; Bosco, G.; Vellone, V.; Spallaccia, F. Mandibular Condylar Fractures in Children: Morphofunctional Results After Treatment with External Fixation. J. Craniofac. Surg. 2017, 28, 1742–1745. [Google Scholar] [CrossRef]
- Hernigou, P. History of external fixation for treatment of fractures. Int. Orthop. 2017, 41, 845–853. [Google Scholar] [CrossRef]
- Mohamed, A.; Mepani, V.; Sharma, V. Use of an endotracheal tube in the biphasic fixation of a mandibular fracture. Br. J. Oral Maxillofac. Surg. 2020, 58, 484–485. [Google Scholar] [CrossRef]
- Mukerji, R.; Mukerji, G.; McGurk, M. Mandibular fractures: Historical perspective. Br. J. Oral Maxillofac. Surg. 2006, 44, 222–228. [Google Scholar] [CrossRef]
- McVeigh, K.; Breeze, J.; Jeynes, P.; Martin, T.; Parmar, S.; Monaghan, A.M. Clinical strategies in the management of complex maxillofacial injuries sustained by British military personnel. BMJ Mil. Health 2010, 156, 110–113. [Google Scholar] [CrossRef] [PubMed]
- Wilkening, M.W.; Patel, P.A.; Gordon, C.B. External fixation in a low-velocity gunshot wound to the mandible. J. Craniofacial Surg. 2012, 23, e418–e419. [Google Scholar] [CrossRef] [PubMed]
- Bazerbachi, F.; Haffar, S.; Hussain, M.T.; Vargas, E.J.; Watt, K.D.; Murad, M.H.; Chari, S.; Dayyeh, B.K.A. Systematic review of acute pancreatitis associated with interferon-α or pegylated interferon-α: Possible or definitive causation? Pancreatology 2018, 18, 691–699. [Google Scholar] [CrossRef] [PubMed]
- Haffar, S.; Bazerbachi, F.; Prokop, L.; Watt, K.D.; Murad, M.H.; Chari, S.T. Frequency and prognosis of acute pancreatitis associated with fulminant or non-fulminant acute hepatitis A: A systematic review. Pancreatology 2017, 17, 166–175. [Google Scholar] [CrossRef]
- Breeze, J.; Gibbons, A.J.; Hunt, N.C.; Monaghan, A.M.; Gibb, I.; Hepper, A.; Midwinter, M. Mandibular fractures in British military personnel secondary to blast trauma sustained in Iraq and Afghanistan. Br. J. Oral. Maxillofac. Surg. 2011, 49, 607–611. [Google Scholar] [CrossRef]
- Breeze, J.; Parmar, S.; Monaghan, A. 71 High-energy ballistic injuries to the face. In Challenging Concepts in Oral and Maxillofacial Surgery: Cases with Expert Commentary; Idle, M.R., Monaghan, A.M., Eds.; Oxford University Press: Oxford, UK, 2016. [Google Scholar]
- Tonn, C.R.; Ward, M.L.; Abadie, W.M.; Lally, J.W.; Bevans, S.E.; Henry, L.R. Military Injuries to the Head and Neck—Implications for Practice in Resource Constrained Environments. Oper. Tech. Otolaryngol. Head Neck Surg. 2020, 31, 339–352. [Google Scholar] [CrossRef]
- McMillan, K.; Martin, T. 77 Reconstructive challenges following blast injuries to the facial soft tissue and skeleton. In Challenging Concepts in Oral and Maxillofacial Surgery: Cases with Expert Commentary; Idle, M.R., Monaghan, A.M., Eds.; Oxford University Press: Oxford, UK, 2016. [Google Scholar]
- Tucker, D.I.; Zachar, M.R.; Chan, R.K.; Hale, R.G. Characterization and management of mandibular fractures: Lessons learned from Iraq and Afghanistan. Atlas Oral Maxillofac. Surg. Clin. N. Am. 2013, 21, 61–68. [Google Scholar] [CrossRef]
- Venugopal, A.; Bhatt, V.; Williams, R.; Sharp, I.; Parmar, S.; Monaghan, A. The use of external fixators and intermaxillary fixation in comminuted fractures of the facial skeleton. Br. J. Oral Maxillofac. Surg. 2011, 49, S111. [Google Scholar] [CrossRef]
- Gibbons, A.J.; Mackenzie, N.; Breederveld, R.S. Use of a custom designed external fixator system to treat ballistic injuries to the mandible. Int. J. Oral Maxillofac. Surg. 2011, 40, 103–105. [Google Scholar] [CrossRef] [PubMed]
- Zorman, D.; Godart, P.A.; Kovacs, B.; Andrianne, Y.; Daelemans, P.; Burny, F. Treatment of mandibular fractures by external fixation. Oral Surg. Oral Med. Oral Pathol. 1990, 69, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Gibbons, A.J.; Mackenzie, N. Lessons learned in oral and maxillofacial surgery from British military deployments in Afghanistan. J. R. Army. Med. Corps. 2010, 156, 113–116. [Google Scholar] [CrossRef] [PubMed]
- Breeze, J.; Gibbons, A.J.; Opie, N.J.; Monaghan, A. Maxillofacial injuries in military personnel treated at the Royal Centre for Defence Medicine June 2001 to December 2007. Br. J. Oral Maxillofac. Surg. 2010, 48, 613–616. [Google Scholar] [CrossRef]
- Gibbons, A.J.; Breeze, A.F. The face of war: The initial management of modern battlefield ballistic facial injuries. J. Mil. Veterans’ Health 2011, 19, 15. [Google Scholar]
- Breeze, J.; Monaghan, A.M.; Williams, M.D.; Clark, R.N.W.; Gibbons, A.J. Five months of surgery in the multinational field hospital in Afghanistan with an emphasis on oral and maxillofacial injuries. J. R. Army Med. Corps. 2010, 156, 125–128. [Google Scholar] [CrossRef]
- Breeze, J.; Gibbons, A.J.; Combes, J.G.; Monaghan, A.M. Oral and maxillofacial surgical contribution to 21 months of operating theatre activity in Kandahar Field Hospital: 1 February 2007–31 October 2008. Br. J. Oral. Maxillofac. Surg. 2011, 49, 464–468. [Google Scholar] [CrossRef]
- Breeze, J.; Tong, D.; Gibbons, A. Contemporary management of maxillofacial ballistic trauma. Br. J. Oral Maxillofac. Surg. 2017, 55, 661–665. [Google Scholar] [CrossRef]
- Breeze, J.; Blanch, R.; Baden, J.; Monaghan, A.M.; Evriviades, D.; Harrisson, S.E.; Roberts, S.; Gibson, A.; MacKenzie, N.; Baxter, D.; et al. Skill sets required for the management of military head, face and neck trauma: A multidisciplinary consensus statement. J. R. Army Med. Corps. 2018, 164, 133–138. [Google Scholar] [CrossRef]
- Peleg, K.; Aharonson-Daniel, L.; Stein, M.; Michaelson, M.; Kluger, Y.; Simon, D.; Noji, E.K.; Israeli Trauma Group. Gunshot and explosion injuries: Characteristics, outcomes, and implications for care of terror-related injuries in Israel. Ann. Surg. 2004, 239, 311–318. [Google Scholar] [CrossRef]
- Deininger, C.; Hofmann, V.; Necchi, M.; Deininger, S.; Wichlas, F. Off-Label Treatment for Severe Craniomaxillofacial Fractures in Low-Income Countries—A Novel Operation Method with the External Face Fixator. J. Clin. Med. 2022, 11, 1488. [Google Scholar] [CrossRef] [PubMed]
- Breeze, J.; Bryant, D. Current concepts in the epidemiology and management of battlefield head, face and neck trauma. BMJ Mil. Health 2009, 155, 274–278. [Google Scholar] [CrossRef]
- Will, M.J.; Goksel, T.; Stone, C.G., Jr.; Doherty, M.J. Oral and maxillofacial injuries experienced in support of Operation Iraqi Freedom I and II. Oral Maxillofac. Surg. Clin. N. Am. 2005, 17, 331–339. [Google Scholar] [CrossRef]
- Neupert, E.A., 3rd; Boyd, S.B. Retrospective analysis of low-velocity gunshot wounds to the mandible. Oral Surg. Oral Med. Oral Pathol. 1991, 72, 383–387. [Google Scholar] [CrossRef]
- Louis, P.J.; Fernandes, R. Temporary stabilization of the mandible with an external fixation device. J. Oral Maxillofac. Surg. 2001, 59, 1374–1375. [Google Scholar] [CrossRef]
- Shuker, S.T. Interrami intraoral fixation technique for severe mandibular rifle fragmented bullet injury management. J. Craniofac. Surg. 2013, 24, 1168–1174. [Google Scholar] [CrossRef]
- Rose, M.J.; Shanti, R.M.; Iocca, O.; Rasa, M.; Ziccardi, V.B. Retrospective analysis of external pin fixation of mandibular fractures: A 25-year single institution experience. J. Craniomaxillofac. Surg. 2025, 53, 624–631. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, J.; Lew, F.; Agarwal, V.; Cho, B. Gunshot Wounds to the Mandible: A 21-Year Urban Trauma Center’s Experience. Plast. Surg. Mod. Tech. 2017, 2, 124. [Google Scholar] [CrossRef]
| Reference | Question 1 | Question 2 | Question 3 | Question 4 | Question 5 | Overall Quality | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Gibbon, 2011 Case report [33] | ☺ | ☺ | ☺ | ☺ | ☺ | Good | |||||
| Carvalho 2019, case series [14] | ☺ | ☺ | ☺ | ☺ | ☺ | Good | |||||
| Zorman 1990, case series [34] | ☺ | ☺ | ☺ | ☺ | ☺ | Low | |||||
| McMillian 2016, case report [30] | ☺ | ☺ | ☺ | ☺ | ☺ | Low | |||||
| Breeze 2016, case report [28] | ☺ | ☺ | ☺ | ☺ | ☺ | Moderate | |||||
| Elbir 2023, case series [6] | ☺ | ☺ | ☺ | ☺ | ☺ | Good | |||||
| Mc Veigh 2010, case series [23] | ☺ | ☺ | ☺ | ☺ | ☺ | Good | |||||
| Maghalaes 2020, case report [13] | ☺ | ☺ | ☺ | ☺ | ☺ | Moderate | |||||
| Reference | Selection | Comparability | Outcome | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Representativeness of the Cases | Ascertainment of Exposure | Selection of Non-Exposed | Outcome Was Not Present at the Start of Study | Comparability of Cohorts | Assessment of Outcome | Sufficient Follow-Up Time | Adequacy of Follow-Up of Cohorts | Overall Quality | |
| Marti-Flich 2020, retrospective cohort study [5] | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 5 |
| Venugopal 2011, retrospective cohort study [32] | 1 | 1 | 0 | 1 | 2 | 1 | 1 | 1 | 8 |
| Breeze 2011, Retrospective cohort study [27] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 |
| Ellis 2003, retrospective cohort study [2] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masumbuko, F.; Reychler, G.; Cornu, O.; Huart, C.; Yombi, J.C.; Olszewski, R. Use of External Fixator Device for Mandible Fracture Related to War Injury: A Systematic Review. J. Clin. Med. 2025, 14, 3061. https://doi.org/10.3390/jcm14093061
Masumbuko F, Reychler G, Cornu O, Huart C, Yombi JC, Olszewski R. Use of External Fixator Device for Mandible Fracture Related to War Injury: A Systematic Review. Journal of Clinical Medicine. 2025; 14(9):3061. https://doi.org/10.3390/jcm14093061
Chicago/Turabian StyleMasumbuko, Franck, Gregory Reychler, Olivier Cornu, Caroline Huart, Jean Cyr Yombi, and Raphael Olszewski. 2025. "Use of External Fixator Device for Mandible Fracture Related to War Injury: A Systematic Review" Journal of Clinical Medicine 14, no. 9: 3061. https://doi.org/10.3390/jcm14093061
APA StyleMasumbuko, F., Reychler, G., Cornu, O., Huart, C., Yombi, J. C., & Olszewski, R. (2025). Use of External Fixator Device for Mandible Fracture Related to War Injury: A Systematic Review. Journal of Clinical Medicine, 14(9), 3061. https://doi.org/10.3390/jcm14093061