
Impact of Diabetes Duration on Major Adverse Cardiac Events in Patients with Non-Obstructive Coronary Artery Disease

 , , , , , and
, , , , , and
Abstract
1. Introduction
2. Methods
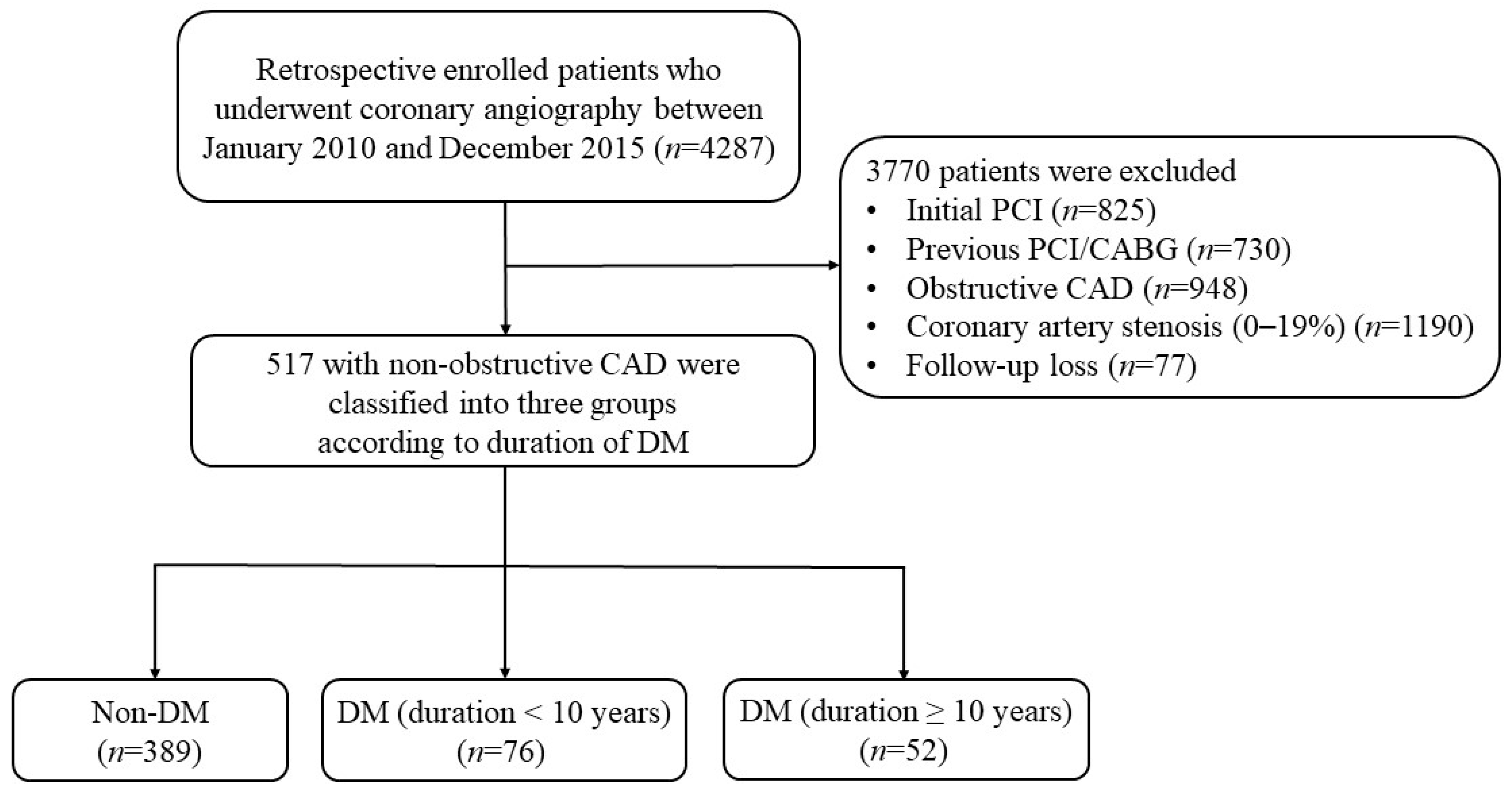
2.1. Study Design and Population
2.2. Study Endpoint and Definition
2.3. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Clinical Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Einarson, T.R.; Acs, A.; Ludwig, C.; Panton, U.H. Prevalence of cardiovascular disease in type 2 diabetes: A systematic literature review of scientific evidence from across the world in 2007-2017. Cardiovasc. Diabetol. 2018, 17, 83. [Google Scholar] [CrossRef] [PubMed]
- Magliano, D.J.; Boyko, E.J.; Scientific Committee, IDF Diabetes Atlas. Idf Diabetes Atlas, 10th ed.; International Diabetes Federation © Interna-tional Diabetes Federation: Brussels, Belgium, 2021. [Google Scholar]
- Liu, Y.; Yang, Y.M.; Zhu, J.; Tan, H.Q.; Liang, Y.; Li, J.D. Prognostic significance of hemoglobin A1c level in patients hospitalized with coronary artery disease. A systematic review and meta-analysis. Cardiovasc. Diabetol. 2011, 10, 98. [Google Scholar] [CrossRef]
- Beckman, J.A.; Creager, M.A.; Libby, P. Diabetes and atherosclerosis: Epidemiology, pathophysiology, and management. JAMA 2002, 287, 2570–2581. [Google Scholar] [CrossRef] [PubMed]
- Esper, R.B.; Farkouh, M.E.; Ribeiro, E.E.; Hueb, W.; Domanski, M.; Hamza, T.H.; Siami, F.S.; Godoy, L.C.; Mathew, V.; French, J.; et al. SYNTAX Score in Patients With Diabetes Undergoing Coronary Revascularization in the FREEDOM Trial. J. Am. Coll. Cardiol. 2018, 72, 2826–2837. [Google Scholar] [CrossRef]
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. Heart disease and stroke statistics—2013 update: A report from the American Heart Association. Circulation 2013, 127, e6–e245. [Google Scholar] [CrossRef]
- Silbernagel, G.; Rosinger, S.; Grammer, T.B.; Kleber, M.E.; Winkelmann, B.R.; Boehm, B.O.; März, W. Duration of type 2 diabetes strongly predicts all-cause and cardiovascular mortality in people referred for coronary angiography. Atherosclerosis 2012, 221, 551–557. [Google Scholar] [CrossRef]
- Barr, E.L.; Zimmet, P.Z.; Welborn, T.A.; Jolley, D.; Magliano, D.J.; Dunstan, D.W.; Cameron, A.J.; Dwyer, T.; Taylor, H.R.; Tonkin, A.M.; et al. Risk of cardiovascular and all-cause mortality in individuals with diabetes mellitus, impaired fasting glucose, and impaired glucose tolerance: The Australian Diabetes, Obesity, and Lifestyle Study (AusDiab). Circulation 2007, 116, 151–157. [Google Scholar] [CrossRef]
- Venuraju, S.M.; Lahiri, A.; Jeevarethinam, A.; Cohen, M.; Darko, D.; Nair, D.; Rosenthal, M.; Rakhit, R.D. Duration of type 2 diabetes mellitus and systolic blood pressure as determinants of severity of coronary stenosis and adverse events in an asymptomatic diabetic population: PROCEED study. Cardiovasc. Diabetol. 2019, 18, 51. [Google Scholar] [CrossRef] [PubMed]
- Finck, T.; Hardenberg, J.; Will, A.; Hendrich, E.; Haller, B.; Martinoff, S.; Hausleiter, J.; Hadamitzky, M. 10-Year Follow-Up After Coronary Computed Tomography Angiography in Patients With Suspected Coronary Artery Disease. JACC Cardiovasc. Imaging 2019, 12, 1330–1338. [Google Scholar] [CrossRef]
- Safdar, B.; Spatz, E.S.; Dreyer, R.P.; Beltrame, J.F.; Lichtman, J.H.; Spertus, J.A.; Reynolds, H.R.; Geda, M.; Bueno, H.; Dziura, J.D.; et al. Presentation, Clinical Profile, and Prognosis of Young Patients with Myocardial Infarction with Nonobstructive Coronary Arteries (MINOCA): Results From the VIRGO Study. J. Am. Heart Assoc. 2018, 7, e009174. [Google Scholar] [CrossRef]
- Rodríguez-Capitán, J.; Sánchez-Pérez, A.; Ballesteros-Pradas, S.; Millán-Gómez, M.; Cardenal-Piris, R.; Oneto-Fernández, M.; Gutiérrez-Alonso, L.; Rivera-López, R.; Guisado-Rasco, A.; Cano-García, M.; et al. Prognostic Implication of Non-Obstructive Coronary Lesions: A New Classification in Different Settings. J. Clin. Med. 2021, 10, 1863. [Google Scholar] [CrossRef] [PubMed]
- Kemp, H.G.; Kronmal, R.A.; Vlietstra, R.E.; Frye, R.L. Seven year survival of patients with normal or near normal coronary arteriograms: A CASS registry study. J. Am. Coll. Cardiol. 1986, 7, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Maddox, T.M.; Stanislawski, M.A.; Grunwald, G.K.; Bradley, S.M.; Ho, P.M.; Tsai, T.T.; Patel, M.R.; Sandhu, A.; Valle, J.; Magid, D.J.; et al. Nonobstructive coronary artery disease and risk of myocardial infarction. JAMA 2014, 312, 1754–1763. [Google Scholar] [CrossRef]
- Nakazato, R.; Arsanjani, R.; Achenbach, S.; Gransar, H.; Cheng, V.Y.; Dunning, A.; Lin, F.Y.; Al-Mallah, M.; Budoff, M.J.; Callister, T.Q.; et al. Age-related risk of major adverse cardiac event risk and coronary artery disease extent and severity by coronary CT angiography: Results from 15 187 patients from the International Multisite CONFIRM Study. Eur. Heart J. Cardiovasc. Imaging 2014, 15, 586–594. [Google Scholar] [CrossRef]
- Ouellette, M.L.; Löffler, A.I.; Beller, G.A.; Workman, V.K.; Holland, E.; Bourque, J.M. Clinical Characteristics, Sex Differences, and Outcomes in Patients With Normal or Near-Normal Coronary Arteries, Non-Obstructive or Obstructive Coronary Artery Disease. J. Am. Heart Assoc. 2018, 7, e007965. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.R.; Peterson, E.D.; Dai, D.; Brennan, J.M.; Redberg, R.F.; Anderson, H.V.; Brindis, R.G.; Douglas, P.S. Low diagnostic yield of elective coronary angiography. N. Engl. J. Med. 2010, 362, 886–895. [Google Scholar] [CrossRef]
- Sharaf, B.; Wood, T.; Shaw, L.; Johnson, B.D.; Kelsey, S.; Anderson, R.D.; Pepine, C.J.; Bairey Merz, C.N. Adverse outcomes among women presenting with signs and symptoms of ischemia and no obstructive coronary artery disease: Findings from the National Heart, Lung, and Blood Institute-sponsored Women’s Ischemia Syndrome Evaluation (WISE) angiographic core laboratory. Am. Heart J. 2013, 166, 134–141. [Google Scholar] [CrossRef]
- Redfors, B.; Furer, A.; Selker, H.P.; Thiele, H.; Patel, M.R.; Chen, S.; Udelson, J.E.; Ohman, E.M.; Eitel, I.; Granger, C.B.; et al. Effect of Smoking on Outcomes of Primary PCI in Patients With STEMI. J. Am. Coll. Cardiol. 2020, 75, 1743–1754. [Google Scholar] [CrossRef]
- Matsuo, S.; Imai, E.; Horio, M.; Yasuda, Y.; Tomita, K.; Nitta, K.; Yamagata, K.; Tomino, Y.; Yokoyama, H.; Hishida, A. Revised equations for estimated GFR from serum creatinine in Japan. Am. J. Kidney Dis. 2009, 53, 982–992. [Google Scholar] [CrossRef]
- Bugiardini, R.; Bairey Merz, C.N. Angina with “normal” coronary arteries: A changing philosophy. JAMA 2005, 293, 477–484. [Google Scholar] [CrossRef]
- Shah, P.K. Molecular mechanisms of plaque instability. Curr. Opin. Lipidol. 2007, 18, 492–499. [Google Scholar] [CrossRef] [PubMed]
- Libby, P.; Theroux, P. Pathophysiology of coronary artery disease. Circulation 2005, 111, 3481–3488. [Google Scholar] [CrossRef] [PubMed]
- Tebaldi, M.; Campo, G.; Biscaglia, S. Fractional flow reserve: Current applications and overview of the available data. World J. Clin. Cases 2015, 3, 678–681. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.J.; Hwang, B.H.; Choi, I.J.; Choo, E.H.; Lim, S.; Kim, J.K.; Koh, Y.S.; Kim, D.B.; Jang, S.W.; Cho, E.J.; et al. Impact of diabetes duration on the extent and severity of coronary atheroma burden and long-term clinical outcome in asymptomatic type 2 diabetic patients: Evaluation by Coronary CT angiography. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 1065–1073. [Google Scholar] [CrossRef]
- Wannamethee, S.G.; Shaper, A.G.; Whincup, P.H.; Lennon, L.; Sattar, N. Impact of diabetes on cardiovascular disease risk and all-cause mortality in older men: Influence of age at onset, diabetes duration, and established and novel risk factors. Arch. Intern. Med. 2011, 171, 404–410. [Google Scholar] [CrossRef]
- Kim, Y.; Shin, M.S.; Kim, Y.S.; Kang, W.C.; Kim, B.R.; Moon, J.; Chung, W.J.; Ahn, T.H.; Shin, E.K. The impact of diabetes duration on left ventricular diastolic function and cardiovascular disease. Postgrad. Med. J. 2012, 88, 189–193. [Google Scholar] [CrossRef]
- Reis, J.P.; Allen, N.B.; Bancks, M.P.; Carr, J.J.; Lewis, C.E.; Lima, J.A.; Rana, J.S.; Gidding, S.S.; Schreiner, P.J. Duration of Diabetes and Prediabetes During Adulthood and Subclinical Atherosclerosis and Cardiac Dysfunction in Middle Age: The CARDIA Study. Diabetes Care 2018, 41, 731–738. [Google Scholar] [CrossRef]
- Fox, C.S.; Sullivan, L.; D’Agostino, R.B., Sr.; Wilson, P.W. The significant effect of diabetes duration on coronary heart disease mortality: The Framingham Heart Study. Diabetes Care 2004, 27, 704–708. [Google Scholar] [CrossRef]
- Gerstein, H.C.; Mann, J.F.; Pogue, J.; Dinneen, S.F.; Hallé, J.P.; Hoogwerf, B.; Joyce, C.; Rashkow, A.; Young, J.; Zinman, B.; et al. Prevalence and determinants of microalbuminuria in high-risk diabetic and nondiabetic patients in the Heart Outcomes Prevention Evaluation Study. The HOPE Study Investigators. Diabetes Care 2000, 23 (Suppl. S2), B35–B39. [Google Scholar]
- Tuomilehto, J.; Borch-Johnsen, K.; Molarius, A.; Forsén, T.; Rastenyte, D.; Sarti, C.; Reunanen, A. Incidence of cardiovascular disease in Type 1 (insulin-dependent) diabetic subjects with and without diabetic nephropathy in Finland. Diabetologia 1998, 41, 784–790. [Google Scholar] [CrossRef]
- Clarkson, P.; Celermajer, D.S.; Donald, A.E.; Sampson, M.; Sorensen, K.E.; Adams, M.; Yue, D.K.; Betteridge, D.J.; Deanfield, J.E. Impaired vascular reactivity in insulin-dependent diabetes mellitus is related to disease duration and low density lipoprotein cholesterol levels. J. Am. Coll. Cardiol. 1996, 28, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Keaney, J.F., Jr.; Larson, M.G.; Vasan, R.S.; Wilson, P.W.; Lipinska, I.; Corey, D.; Massaro, J.M.; Sutherland, P.; Vita, J.A.; Benjamin, E.J. Obesity and systemic oxidative stress: Clinical correlates of oxidative stress in the Framingham Study. Arter. Thromb. Vasc. Biol. 2003, 23, 434–439. [Google Scholar] [CrossRef] [PubMed]
- Boudina, S.; Abel, E.D. Diabetic cardiomyopathy revisited. Circulation 2007, 115, 3213–3223. [Google Scholar] [CrossRef] [PubMed]
- Meigs, J.B.; Mittleman, M.A.; Nathan, D.M.; Tofler, G.H.; Singer, D.E.; Murphy-Sheehy, P.M.; Lipinska, I.; D’Agostino, R.B.; Wilson, P.W. Hyperinsulinemia, hyperglycemia, and impaired hemostasis: The Framingham Offspring Study. JAMA 2000, 283, 221–228. [Google Scholar] [CrossRef]
- Kannel, W.B.; D’Agostino, R.B.; Wilson, P.W.; Belanger, A.J.; Gagnon, D.R. Diabetes, fibrinogen, and risk of cardiovascular disease: The Framingham experience. Am. Heart J. 1990, 120, 672–676. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Non-DM | DM_Duration < 10 Years | DM_Duration ≥ 10 Years | p-Value | |
|---|---|---|---|---|
| N | 389 | 76 | 52 | - |
| DM duration (years) | 3 (2–6) | 15 (10–20) | ||
| Age (years) | 62.2 ± 11.5 | 64.0 ± 9.9 | 68.1 ± 9.8 | 0.001 |
| Male | 208 (53.5) | 34 (44.7) | 28 (53.9) | 0.557 |
| BMI (kg/m2) | 24.3 ± 3.0 | 25.7 ± 3.6 | 24.0 ± 3.2 | 0.002 |
| Hypertension | 192 (49.4) | 53 (69.7) | 35 (67.3) | <0.001 |
| Dyslipidemia | 78 (20.1) | 20 (26.3) | 8 (15.4) | 0.292 |
| Smoking | 133 (34.2) | 20 (26.3) | 13 (25.0) | 0.207 |
| CKD | 2 (0.5) | 3 (4.0) | 5 (9.6) | <0.001 |
| Previous CVA | 26 (6.7) | 6 (7.9) | 3 (5.8) | 0.887 |
| Aspirin | 213 (54.8) | 39 (51.3) | 22 (42.3) | 0.228 |
| Thienophyridine | 26 (6.7) | 7 (9.2) | 3 (5.8) | 0.686 |
| Cilostazol | 10 (2.6) | 2 (2.6) | 8 (15.4) | <0.001 |
| Statin | 138 (35.5) | 26 (34.2) | 15 (28.9) | 0.639 |
| Beta blocker | 62 (15.9) | 15 (19.7) | 11 (21.2) | 0.510 |
| ACEi/ARB | 69 (17.7) | 20 (26.3) | 14 (26.9) | 0.095 |
| Vasodilator | 157 (40.4) | 27 (35.5) | 17 (32.7) | 0.459 |
| LV EF (%) | 61.5 ± 8.5 | 60.7 ± 9.8 | 56.7 ± 11.4 | 0.008 |
| Fasting glucose (mg/dL) | 113.4 ± 34.2 | 153.5 ± 51.5 | 183.7 ± 96.6 | <0.001 |
| HbA1c (%) | 5.9 ± 0.6 | 7.3 ± 1.2 | 7.9 ± 1.7 | <0.001 |
| Creatinine (mg/dL) | 0.8 (0.7–1.0) | 0.8 (0.7–1.0) | 0.9 (0.7–1.3) | 0.018 |
| Hemoglobin (g/dL) | 13.7 ± 1.8 | 13.6 ± 1.9 | 12.8 ± 1.8 | 0.005 |
| Hematocrit (%) | 40.1 ± 4.5 | 39.6 ± 5.2 | 37.3 ± 5.0 | <0.001 |
| Platelet (×109/L) | 237.6 ± 60.7 | 254.4 ± 72.6 | 231.8 ± 64.3 | 0.078 |
| White blood cell (×109/L) | 7.7 ± 2.8 | 7.7 ± 3.1 | 7.5 ± 2.3 | 0.886 |
| Total cholesterol (mg/dL) | 188.4 ± 37.4 | 174.7 ± 47.7 | 160.9 ± 40.3 | <0.001 |
| Triglycerides (mg/dL) | 125.1 ± 75.8 | 157.0 ± 92.3 | 129.4 ± 94.5 | 0.013 |
| HDL-cholesterol (mg/dL) | 44.2 ± 12.1 | 41.2 ± 10.3 | 37.6 ± 11.2 | 0.002 |
| LDL-cholesterol (mg/dL) | 114.6 ± 32.9 | 99.6 ± 40.9 | 96.0 ± 32.0 | <0.001 |
| C-Reactive protein (mg/dL) | 0.13 (0.06–0.34) | 0.18 (0.08–0.42) | 0.28 (0.09–1.53) | 0.031 |
| Albumin (g/dL) | 4.3 ± 0.4 | 4.2 ± 0.5 | 4.1 ± 0.4 | 0.007 |
| Non-DM (n = 389) | DM_Duration < 10 Years (n = 76) | DM_Duration ≥ 10 Years (n = 52) | p-Value | |
|---|---|---|---|---|
| MACCEs | 18 (4.6) | 8 (10.5) | 12 (23.1) | <0.001 |
| All-cause death | 25 (6.4) | 5 (6.6) | 13 (25.0) | <0.001 |
| Cardiovascular death | 3 (0.8) | 2 (2.6) | 5 (9.6) | <0.001 |
| Non-fatal MI | 4 (1.0) | 1 (1.3) | 0 (0.0) | 0.734 |
| Non-fatal stroke | 11 (2.8) | 5 (6.6) | 7 (13.5) | <0.001 |
| Unadjusted HR (95% CI) | p-Value | Model 1 | p-Value | Model 2 | p-Value | |
|---|---|---|---|---|---|---|
| MACCEs | ||||||
| non-DM | 1.00 | - | 1.00 | - | 1.00 | |
| DM_duration < 10 years | 2.45 (1.07–5.64) | 0.035 | 2.48 (1.08–5.71) | 0.033 | 2.34 (0.98–5.55) | 0.055 |
| DM_duration ≥ 10 years | 5.39 (2.59–11.20) | <0.001 | 5.52 (2.58–11.81) | <0.001 | 4.61 (2.04–10.40) | <0.001 |
| All-cause death | ||||||
| non-DM | 1.00 | - | 1.00 | - | 1.00 | |
| DM_duration < 10 years | 1.05 (0.40–2.74) | 0.923 | 0.97 (0.37–2.53) | 0.946 | 0.88 (0.33–2.37) | 0.796 |
| DM_duration ≥ 10 years | 4.16 (2.13–8.14) | <0.001 | 3.38 (1.70–6.74) | <0.001 | 2.09 (0.94–4.64) | 0.069 |
| Cardiovascular death | ||||||
| non-DM | 1.00 | - | 1.00 | - | 1.00 | |
| DM_duration < 10 years | 3.57 (0.60–21.34) | 0.164 | 3.60 (0.60–21.58) | 0.162 | 3.01 (0.41–22.16) | 0.281 |
| DM_duration ≥ 10 years | 13.19 (3.15–55.24) | <0.001 | 13.57 (3.07–60.04) | <0.001 | 12.42 (2.33–66.22) | 0.003 |
| Non-fatal MI | ||||||
| non-DM | 1.00 | - | 1.00 | - | 1.00 | |
| DM_duration < 10 years | 1.31 (0.15–11.74) | 0.808 | 1.54 (0.17–14.12) | 0.703 | 1.14 (0.11–12.04) | 0.911 |
| DM_duration ≥ 10 years | - | - | - | - | - | |
| Non-fatal stroke | ||||||
| non-DM | 1.00 | - | 1.00 | - | 1.00 | |
| DM_duration < 10 years | 2.54 (0.88–7.31) | 0.084 | 2.49 (0.86–7.18) | 0.091 | 2.21 (0.74–6.62) | 0.158 |
| DM_duration ≥ 10 years | 6.10 (2.45–15.18) | <0.001 | 5.53 (2.15–14.23) | <0.001 | 4.97 (1.88–13.19) | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.-A.; Song, S.-W.; Kim, S.-H.; Jung, J.; Jang, W.-Y.; Moon, D.; Her, S.-H.; Yoo, K.-D.; Moon, K.-W.; Lee, S.N. Impact of Diabetes Duration on Major Adverse Cardiac Events in Patients with Non-Obstructive Coronary Artery Disease. J. Clin. Med. 2025, 14, 2797. https://doi.org/10.3390/jcm14082797
Lee Y-A, Song S-W, Kim S-H, Jung J, Jang W-Y, Moon D, Her S-H, Yoo K-D, Moon K-W, Lee SN. Impact of Diabetes Duration on Major Adverse Cardiac Events in Patients with Non-Obstructive Coronary Artery Disease. Journal of Clinical Medicine. 2025; 14(8):2797. https://doi.org/10.3390/jcm14082797
Chicago/Turabian StyleLee, Yun-Ah, Sang-Wook Song, Se-Hong Kim, Jin Jung, Won-Young Jang, Donggyu Moon, Sung-Ho Her, Ki-Dong Yoo, Keon-Woong Moon, and Su Nam Lee. 2025. "Impact of Diabetes Duration on Major Adverse Cardiac Events in Patients with Non-Obstructive Coronary Artery Disease" Journal of Clinical Medicine 14, no. 8: 2797. https://doi.org/10.3390/jcm14082797
APA StyleLee, Y.-A., Song, S.-W., Kim, S.-H., Jung, J., Jang, W.-Y., Moon, D., Her, S.-H., Yoo, K.-D., Moon, K.-W., & Lee, S. N. (2025). Impact of Diabetes Duration on Major Adverse Cardiac Events in Patients with Non-Obstructive Coronary Artery Disease. Journal of Clinical Medicine, 14(8), 2797. https://doi.org/10.3390/jcm14082797