
Effectiveness of Transcranial Stimulation on Cognitive Abilities of Older Adults with Mild Cognitive Impairment
 ,
,  ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Sources of Information
2.2. Search Strategy
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Study Selection Process
2.6. Data Extraction
2.7. Assessment of Methodological Quality
2.8. Analytic Decisions for Meta-Analysis
3. Results
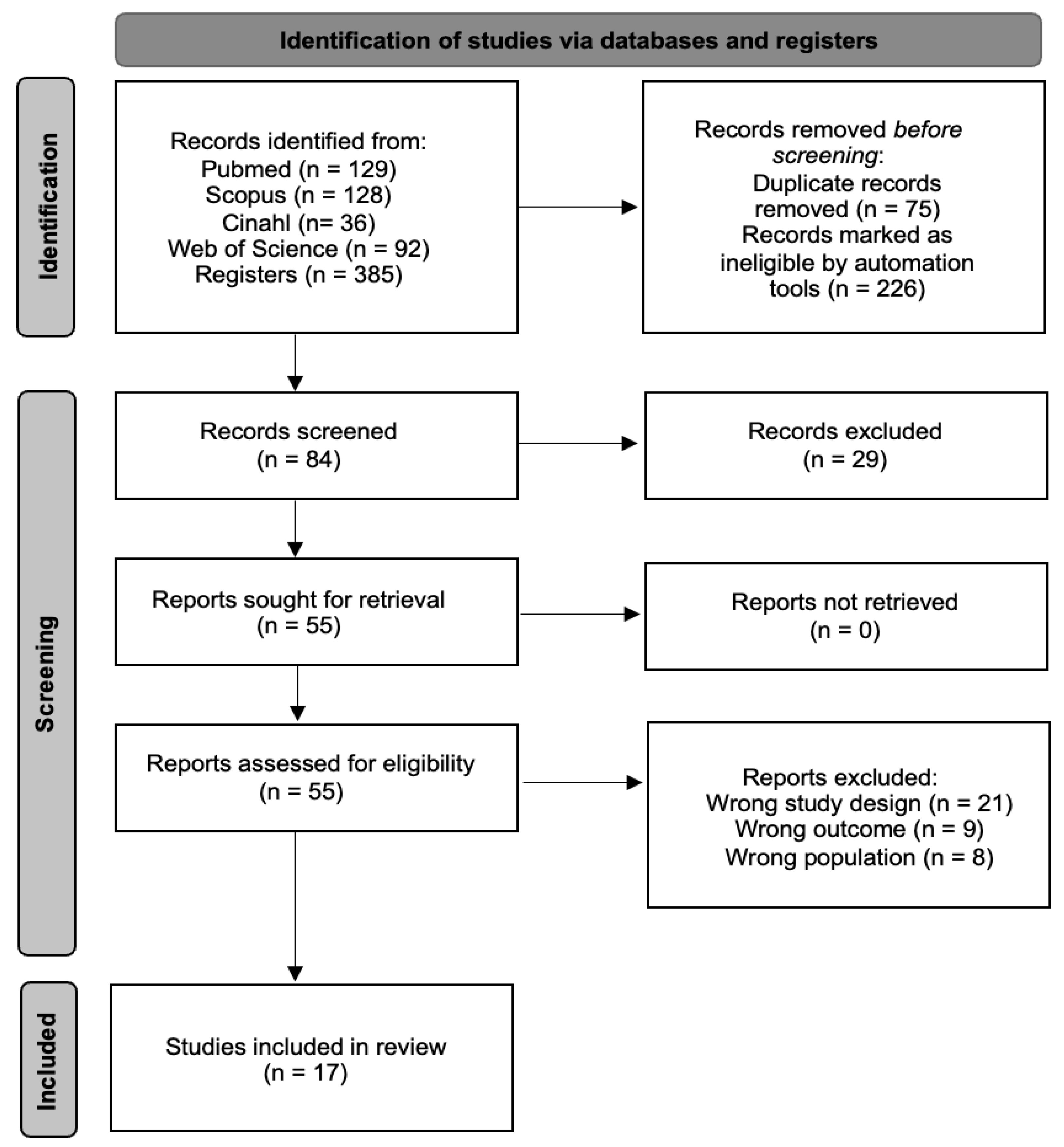
3.1. Study Selection Process
3.2. Methodological Quality
3.3. Characteristics of the Studies
3.4. Study Results
3.5. Meta-Analysis
3.5.1. Subgroup Analysis
3.5.2. Global Cognitive Function
3.5.3. Visual Attention
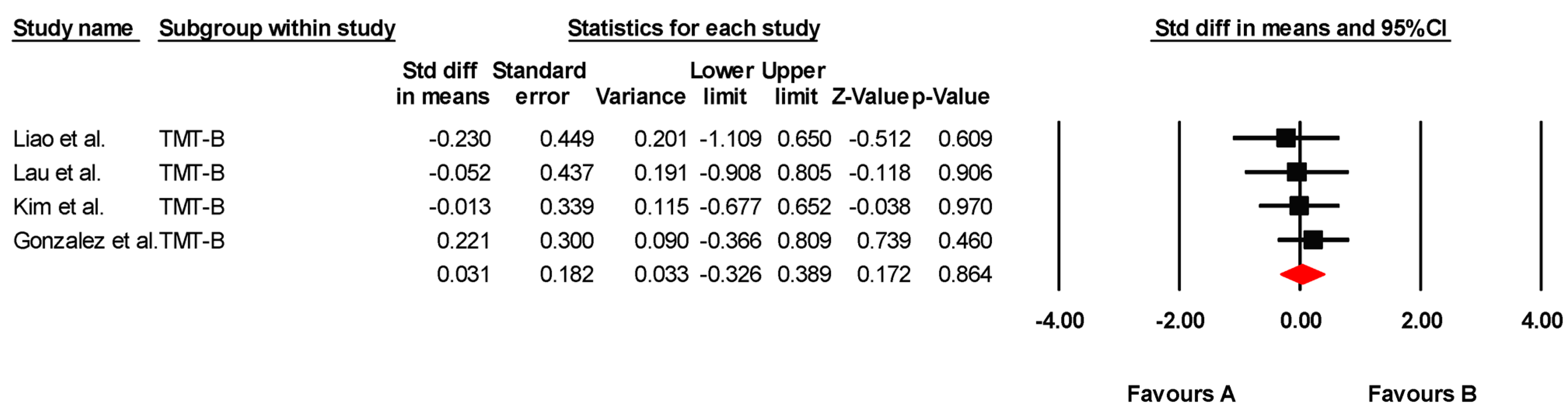
3.5.4. Mental Flexibility
3.5.5. Selective Attention
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| tDCS | transcranial direct current stimulation |
| MCI | mild cognitive impairment |
| WOS | Web of Science |
| RCTs | randomized controlled trials |
| MoCA | Montreal Cognitive Assessment |
| MMSE | Mini-Mental State Examination |
| CT | cognitive training |
| OLM | associative Object-Location Memory |
| atDCS | anodal transcranial direct current stimulation |
| HD-tDCS | high-definition transcranial direct current stimulation |
| fALFF | fractional Amplitude of Low-Frequency Fluctuation |
| ReHo | Regional Homogenity |
| CCT | Cognitive Control Training |
| ICCT | Interactive Computerized Cognitive Training |
| MRS | Magnetic Resonance Spectroscopy |
| GABA | Glutamate and Gamma-aminobutyric Acid |
| TUG | Timed Up-and-Go test |
| TMT-A | Trail Making Test-A |
| DLPFC | dorsolateral prefrontal cortex |
| DATL | Dominal Anterior Temporal Lobe |
| PFC-tDCS | prefrontal cortex transcranial direct current stimulation |
| tDCS-cog | transcranial direct current stimulation combined with cognitive training |
| VOMT | Visual Object Matching Task |
| CANTAB | Cambridge Neuropsychological Test Automated Battery |
| VSA | Visual Sustained Attention |
| SWM | Spatial Working Memory |
| VM | Visual Memory |
| SCWT | Stroop Color Word Test |
| rsFCNPS | functional connectivity Neuropsychiatric Symptoms |
| F | frequency |
| #S | number of sessions |
| D | duration |
References
- Ismail, Z.; Ahmad, W.I.W.; Hamjah, S.H.; Astina, I.K. The Impact of Population Ageing: A Review. Iran. J. Public Health 2021, 50, 2451–2460. [Google Scholar] [PubMed]
- Langa, K.M. Cognitive Aging, Dementia, and the Future of an Aging Population. In National Academies of Sciences, Engineering, and Medicine; Division of Behavioral and Social Sciences and Education; Committee on Population; Majmundar, M.K., Hayward, M.D., Eds.; Future Directions for the Demography of Aging: Proceedings of a Workshop; National Academies Press (US): Washington, DC, USA, 2018; Volume 9. Available online: https://www.ncbi.nlm.nih.gov/books/NBK513075/ (accessed on 15 January 2025).
- Murman, D.L. The Impact of Age on Cognition. Semin. Hear. 2015, 36, 111–121. [Google Scholar]
- Lee, P.L.; Huang, C.K.; Chen, Y.Y.; Chang, H.H.; Cheng, C.H.; Lin, Y.C.; Lin, C.-L. Enhancing Cognitive Function in Older Adults through Processing Speed Training: Implications for Cognitive Health Awareness. Healthcare 2024, 12, 532. [Google Scholar] [CrossRef]
- National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Health Sciences Policy; Committee on Preventing Dementia and Cognitive Impairment. Preventing Cognitive Decline and Dementia: A Way Forward; Downey, A., Stroud, C., Landis, S., Leshner, A.I., Eds.; National Academies Press (US): Washington, DC, USA, 2017. [Google Scholar] [PubMed]
- Xu, Y.; Huang, H.; Wu, M.; Zhuang, Z.; Liu, H.; Hou, M.; Chen, C. Transcranial Direct Current Stimulation for Cognitive Impairment Rehabilitation: A Bibliometric Analysis. Arch. Med. Res. 2025, 56, 103086. [Google Scholar] [PubMed]
- Chen, J.; Wang, Z.; Chen, Q.; Fu, Y.; Zheng, K. Transcranial Direct Current Stimulation Enhances Cognitive Function in Patients with Mild Cognitive Impairment and Early/Mid Alzheimer’s Disease: A Systematic Review and Meta-Analysis. Brain Sci. 2022, 12, 562. [Google Scholar] [CrossRef] [PubMed]
- Reed, T.; Cohen Kadosh, R. Transcranial electrical stimulation (tES) mechanisms and its effects on cortical excitability and connectivity. J. Inherit. Metab. Dis. 2018, 41, 1123–1130. [Google Scholar]
- Grider, M.H.; Jessu, R.; Kabir, R. Physiology, Action Potential. [Updated 2023 May 8]. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2025. Available online: https://www.ncbi.nlm.nih.gov/books/NBK538143/ (accessed on 16 January 2025).
- Bennabi, D.; Pedron, S.; Haffen, E.; Monnin, J.; Peterschmitt, Y.; Van Waes, V. Transcranial direct current stimulation for memory enhancement: From clinical research to animal models. Front. Syst. Neurosci. 2014, 8, 159. [Google Scholar]
- Au, J.; Katz, B.; Moon, A.; Talati, S.; Abagis, T.R.; Jonides, J.; Jaeggi, S.M. Post-training stimulation of the right dorsolateral prefrontal cortex impairs working memory training performance. J. Neurosci. Res. 2021, 99, 2351–2363. [Google Scholar]
- Goldthorpe, R.A.; Rapley, J.M.; Violante, I.R. A Systematic Review of Non-invasive Brain Stimulation Applications to Memory in Healthy Aging. Front. Neurol. 2020, 11, 575075. [Google Scholar] [CrossRef]
- Šimko, P.; Pupíková, M.; Gajdoš, M.; Rektorová, I. Cognitive Aftereffects of Acute tDCS Coupled with Cognitive Training: An fMRI Study in Healthy Seniors. Neural Plast. 2021, 2021, 6664479. [Google Scholar]
- Moshfeghinia, R.; Shekouh, D.; Mostafavi, S.; Hosseinzadeh, M.; Bahadori, A.R.; Abdollahifard, S.; Razmkon, A. The effects of transcranial direct-current stimulation (tDCS) on pain intensity of patients with fibromyalgia: A systematic review and meta-analysis. BMC Neurol. 2023, 23, 395. [Google Scholar] [CrossRef] [PubMed]
- Prathum, T.; Chantanachai, T.; Vimolratana, O.; Laksanaphuk, C.; Apiworajirawit, I.; Aneksan, B.; Latthirun, K.; Yang, C.-T.; Klomjai, W. A systematic review and meta-analysis of the impact of transcranial direct current stimulation on cognitive function in older adults with cognitive impairments: The influence of dosage parameters. Alzheimer’s Res. Ther. 2025, 17, 37. [Google Scholar]
- Antonioni, A.; Baroni, A.; Fregna, G.; Ahmed, I.; Straudi, S. The effectiveness of home-based transcranial direct current stimulation on chronic pain: A systematic review and meta-analysis. Digit. Health 2024, 10, 20552076241292677. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.J.; Cho, Y.; Lee, J.H. Transcranial Direct Current Stimulation for Global Cognition in Mild Cognitive Impairment. Chonnam Med. J. 2025, 61, 1–8. [Google Scholar] [CrossRef]
- Phipps, C.J.; Murman, D.L.; Warren, D.E. Stimulating Memory: Reviewing Interventions Using Repetitive Transcranial Magnetic Stimulation to Enhance or Restore Memory Abilities. Brain Sci. 2021, 11, 1283. [Google Scholar] [CrossRef]
- Brunoni, A.R.; Nitsche, M.A.; Bolognini, N.; Bikson, M.; Wagner, T.; Merabet, L.; Edwards, D.J.; Valero-Cabre, A.; Rotenberg, A.; Pascual-Leone, A.; et al. Clinical research with transcranial direct current stimulation (tDCS): Challenges and future directions. Brain Stimul. 2012, 5, 175–195. [Google Scholar] [CrossRef]
- Sanderson-Cimino, M.; Elman, J.A.; Tu, X.M.; Gross, A.L.; Panizzon, M.S.; Gustavson, D.E.; Bondi, M.W.; Edmonds, E.C.; Eglit, G.M.L.; Eppig, J.S.; et al. Cognitive practice effects delay diagnosis of MCI: Implications for clinical trials. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2022, 8, e12228. [Google Scholar]
- Xiao, Z.; Wu, W.; Ma, X.; Wu, J.; Liang, X.; Zhou, X.; Cao, Y.; Zhao, Q.; Ding, D. Plasma p-tau217, p-tau181, and NfL as early indicators of dementia risk in a community cohort: The Shanghai Aging Study. Alzheimers Dement. 2023, 15, e12514. [Google Scholar] [CrossRef]
- Kang, J.H.; Korecka, M.; Lee, E.B.; Cousins, K.A.Q.; Tropea, T.F.; Chen-Plotkin, A.A.; Irwin, D.J.; Wolk, D.; Brylska, M.; Wan, Y.; et al. Alzheimer Disease Biomarkers: Moving from CSF to Plasma for Reliable Detection of Amyloid and tau Pathology. Clin. Chem. 2023, 69, 1247–1259. [Google Scholar] [CrossRef]
- Dubois, B.; von Arnim, C.A.F.; Burnie, N.; Bozeat, S.; Cummings, J. Biomarkers in Alzheimer’s disease: Role in early and differential diagnosis and recognition of atypical variants. Alzheimers Res. Ther. 2023, 15, 175. [Google Scholar] [CrossRef]
- Leuzy, A.; Mattsson-Carlgren, N.; Palmqvist, S.; Janelidze, S.; Dage, J.L.; Hansson, O. Blood-based biomarkers for Alzheimer’s disease EMBO Mol Med. 2022, 14, e14408.
- Hansson, O. Biomarkers for neurodegenerative diseases. Nat. Med. 2023, 29, 761–773. [Google Scholar] [CrossRef]
- Janelidze, S.; Stomrud, E.; Smith, R.; Palmqvist, S.; Mattsson, N.; Airey, D.; Proctor, N.; Chai, X.; Shcherbinin, S.; Triana-Baltzer, G.; et al. Plasma P-tau217 performs better than P-tau181 as a biomarker of Alzheimer’s disease Nat Commun. 2020, 11, 1683.
- Palmqvist, S.; Janelidze, S.; Quiroz, Y.T.; Zetterberg, H.; Lopera, F.; Stomrud, E.; Su, Y.; Chen, Y.; Serrano, G.E.; Leuzy, A.; et al. Discriminative Accuracy of Plasma Phospho-tau217 for Alzheimer Disease vs Other Neurodegenerative Disorders. JAMA 2020, 324, 772–781. [Google Scholar] [CrossRef]
- Albishi, A.M. How does combining physical therapy with transcranial direct stimulation improve upper-limb motor functions in patients with stroke? A theory perspective. Ann. Med. Surg. 2024, 86, 4601–4607. [Google Scholar]
- Sanches, C.; Stengel, C.; Godard, J.; Mertz, J.; Teichmann, M.; Migliaccio, R.; Valero-Cabré, A. Past, Present, and Future of Non-invasive Brain Stimulation Approaches to Treat Cognitive Impairment in Neurodegenerative Diseases: Time for a Comprehensive Critical Review. Front. Aging Neurosci. 2021, 12, 578339. [Google Scholar]
- Fregni, F.; Nitsche, M.A.; Loo, C.K.; Brunoni, A.R.; Marangolo, P.; Leite, J.; Carvalho, S.; Bolognini, N.; Caumo, W.; Paik, N.J.; et al. Regulatory Considerations for the Clinical and Research Use of Transcranial Direct Current Stimulation (tDCS): Review and recommendations from an expert panel. Clin. Res. Regul. Aff. 2015, 32, 22–35. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The prisma 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions Version 6.4 (Updated August 2023). Cochrane. 2023. Available online: www.training.cochrane.org/handbook (accessed on 22 November 2023).
- Cashin, A.G.; McAuley, J.H. Clinimetrics: Physiotherapy evidence database (pedro) scale. J. Physiother. 2020, 66, 59. [Google Scholar]
- de Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar]
- Higgins, J.P.T.; Savović, J.; Page, M.; Elbers, R.; Sterne, J.A.C. Assessing risk of bias in a randomized trial. In Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Higgins, J.P.T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M.J., Welch, V.A., Eds.; Wiley-Blackwell: Chichester, UK, 2019; pp. 205–228. [Google Scholar] [CrossRef]
- de Sousa, A.V.C.; Grittner, U.; Rujescu, D.; Külzow, N.; Flöel, A. Impact of 3-Day Combined Anodal Transcranial Direct Current Stimulation-Visuospatial Training on Object-Location Memory in Healthy Older Adults and Patients with Mild Cognitive Impairment. J. Alzheimers Dis. 2020, 75, 223–244. [Google Scholar] [CrossRef] [PubMed]
- Fileccia, E.; Di Stasi, V.; Poda, R.; Rizzo, G.; Stanzani-Maserati, M.; Oppi, F.; Avoni, P.; Capellari, S.; Liguori, R. Effects on cognition of 20-day anodal transcranial direct current stimulation over the left dorsolateral prefrontal cortex in patients affected by mild cognitive impairment: A case-control study. Neurol. Sci. 2019, 40, 1865–1872. [Google Scholar] [CrossRef]
- Gonzalez, P.C.; Fong, K.N.K.; Brown, T. Transcranial direct current stimulation as an adjunct to cognitive training for older adults with mild cognitive impairment: A randomized controlled trial. Ann. Phys. Rehabil. Med. 2021, 64, 101536. [Google Scholar]
- He, F.; Li, Y.; Li, C.; Fan, L.; Liu, T.; Wang, J. Repeated anodal high-definition transcranial direct current stimulation over the left dorsolateral prefrontal cortex in mild cognitive impairment patients increased regional homogeneity in multiple brain regions. PLoS ONE 2021, 16, e0256100. [Google Scholar]
- Kim, J.; Park, S.; Kim, H.; Roh, D.; Kim, D.H. Home-based, Remotely Supervised, 6-Week tDCS in Patients With Both MCI and Depression: A Randomized Double-Blind Placebo-Controlled Trial. Clin. EEG Neurosci. 2024, 55, 531–542. [Google Scholar] [PubMed]
- Lau, C.I.; Liu, M.N.; Cheng, F.Y.; Wang, H.C.; Walsh, V.; Liao, Y.Y. Can transcranial direct current stimulation combined with interactive computerized cognitive training boost cognition and gait performance in older adults with mild cognitive impairment? a randomized controlled trial. J. Neuroeng. Rehabil. 2024, 21, 26. [Google Scholar] [CrossRef]
- Lengu, K.; Ryan, S.; Peltier, S.J.; Tyszkowski, T.; Kairys, A.; Giordani, B.; Hampstead, B.M. Effects of High Definition-Transcranial Direct Current Stimulation on Local GABA and Glutamate Levels Among Older Adults with and without Mild Cognitive Impairment: An Exploratory Study. J. Alzheimers Dis. 2021, 84, 1091–1102. [Google Scholar] [CrossRef]
- Liao, Y.Y.; Liu, M.N.; Wang, H.C.; Walsh, V.; Lau, C.I. Combining Transcranial Direct Current Stimulation With Tai Chi to Improve Dual-Task Gait Performance in Older Adults With Mild Cognitive Impairment: A Randomized Controlled Trial. Front. Aging Neurosci. 2021, 13, 766649. [Google Scholar]
- Manenti, R.; Sandrini, M.; Gobbi, E.; Binetti, G.; Cotelli, M. Effects of Transcranial Direct Current Stimulation on Episodic Memory in Amnestic Mild Cognitive Impairment: A Pilot Study. J. Gerontol. B Psychol. Sci. Soc. Sci. 2020, 75, 1403–1413. [Google Scholar] [CrossRef]
- Manor, B.; Zhou, J.; Harrison, R.; Lo, O.Y.; Travison, T.G.; Hausdorff, J.M.; Pascual-Leone, A.; Lipsitz, L. Transcranial Direct Current Stimulation May Improve Cognitive-Motor Function in Functionally Limited Older Adults. Neurorehabil. Neural Repair. 2018, 32, 788–798. [Google Scholar] [CrossRef]
- Martin, D.M.; Mohan, A.; Alonzo, A.; Gates, N.; Gbadeyan, O.; Meinzer, M.; Sachdev, P.; Brodaty, H.; Loo, C. A Pilot Double-Blind Randomized Controlled Trial of Cognitive Training Combined with Transcranial Direct Current Stimulation for Amnestic Mild Cognitive Impairment. J. Alzheimers Dis. 2019, 71, 503–512. [Google Scholar] [CrossRef] [PubMed]
- Rezakhani, S.; Amiri, M.; Hassani, A.; Esmaeilpour, K.; Sheibani, V. Anodal HD-tDCS on the dominant anterior temporal lobe and dorsolateral prefrontal cortex: Clinical results in patients with mild cognitive impairment. Alzheimers Res. Ther. 2024, 16, 27. [Google Scholar] [CrossRef]
- Sandrini, M.; Manenti, R.; Brambilla, M.; Cobelli, C.; Cohen, L.G.; Cotelli, M. Older adults get episodic memory boosting from noninvasive stimulation of prefrontal cortex during learning. Neurobiol. Aging 2016, 39, 210–216. [Google Scholar] [CrossRef]
- Šimko, P.; Pupíková, M.; Gajdoš, M.; Klobušiaková, P.; Vávra, V.; Šimo, A.; Rektorová, I. Exploring the impact of intensified multiple session tDCS over the left DLPFC on brain function in MCI: A randomized control trial. Sci. Rep. 2024, 14, 1512. [Google Scholar] [CrossRef] [PubMed]
- Stonsaovapak, C.; Hemrungroj, S.; Terachinda, P.; Piravej, K. Effect of Anodal Transcranial Direct Current Stimulation at the Right Dorsolateral Prefrontal Cortex on the Cognitive Function in Patients with Mild Cognitive Impairment: A Randomized Double-Blind Controlled Trial. Arch. Phys. Med. Rehabil. 2020, 101, 1279–1287. [Google Scholar] [CrossRef] [PubMed]
- Turnbull, A.; Anthony, M.; Tadin, D.; Porsteinsson, A.P.; Heffner, K.; Lin, F.V. Effect of online tDCS to left somatomotor cortex on neuropsychiatric symptoms among older adults at risk for dementia. Cortex 2023, 159, 131–141. [Google Scholar] [CrossRef]
- Yun, K.; Song, I.U.; Chung, Y.A. Changes in cerebral glucose metabolism after 3 weeks of noninvasive electrical stimulation of mild cognitive impairment patients. Alzheimers Res. Ther. 2016, 8, 49. [Google Scholar] [CrossRef]
- Shin, Y.I.; Foerster, Á.; Nitsche, M.A. Transcranial direct current stimulation (tDCS)—Application in neuropsychology. Neuropsychologia 2015, 69, 154–175. [Google Scholar] [CrossRef]
- Meinzer, M.; Lindenberg, R.; Antonenko, D.; Flaisch, T.; Flöel, A. Anodal transcranial direct current stimulation temporarily reverses age-associated cognitive decline and functional brain activity changes. J. Neurosci. 2013, 33, 12470–12478. [Google Scholar] [CrossRef]
- Hsu, W.Y.; Ku, Y.; Zanto, T.P.; Gazzaley, A. Effects of noninvasive brain stimulation on cognitive function in healthy aging and Alzheimer’s disease: A systematic review and meta-analysis. Neurobiol. Aging 2015, 36, 2348–2359. [Google Scholar] [CrossRef]
- Hill, A.T.; Fitzgerald, P.B.; Hoy, K.E. Effects of Anodal Transcranial Direct Current Stimulation on Working Memory: A Systematic Review and Meta-Analysis of Findings From Healthy and Neuropsychiatric Populations. Brain Stimul. 2016, 9, 197–208. [Google Scholar] [CrossRef] [PubMed]
- Chung, S.W.; Hill, A.T.; Rogasch, N.C.; Hoy, K.E.; Fitzgerald, P.B. Use of theta-burst stimulation in changing excitability of motor cortex: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2016, 63, 43–64. [Google Scholar] [PubMed]
- Pope, P.A.; Brenton, J.W.; Miall, R.C. Task-Specific Facilitation of Cognition by Anodal Transcranial Direct Current Stimulation of the Prefrontal Cortex. Cereb. Cortex 2015, 25, 4551–4558. [Google Scholar]
- Uddin, L.Q. Cognitive and behavioural flexibility: Neural mechanisms and clinical considerations. Nat. Rev. Neurosci. 2021, 22, 167–179. [Google Scholar] [PubMed]
- Manenti, R.; Sandrini, M.; Gobbi, E.; Cobelli, C.; Brambilla, M.; Binetti, G.; Cotelli, M. Strengthening of Existing Episodic Memories Through Non-invasive Stimulation of Prefrontal Cortex in Older Adults with Subjective Memory Complaints. Front. Aging Neurosci. 2017, 9, 401. [Google Scholar]
- Smith, J.Q.; Jones, M.R.; Brown, C.D. The Future of Work: Implications for Managerial Innovation and Resource Management. Bus. Horiz. 2018, 61, 1–12. [Google Scholar]
- Antonenko, D.; Fromm, A.E.; Thams, F.; Kuzmina, A.; Backhaus, M.; Knochenhauer, E.; Li, S.C.; Grittner, U.; Flöel, A. Cognitive training and brain stimulation in patients with cognitive impairment: A randomized controlled trial. Alzheimer’s Res. Ther. 2024, 16, 6. [Google Scholar] [CrossRef]
- Talsma, L.J.; Kroese, H.A.; Slagter, H.A. Boosting Cognition: Effects of Multiple-Session Transcranial Direct Current Stimulation on Working Memory. J. Cogn. Neurosci. 2017, 29, 755–768. [Google Scholar]
- Lindenberger, U.; Lövdén, M. Brain Plasticity in Human Lifespan Development: The Exploration-Selection-Refinement Model. Annu. Rev. Dev. Psychol. 2019, 1, 197–222. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total Score | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| De Sousa et al. [36] | 1 | 1 | 0 | 1 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 6 |
| Fileccia et al. [37] | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 8 |
| González et al. [38] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 9 |
| He et al. [39] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 9 |
| Kim et al. [40] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 9 |
| Lau et al. [41] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 9 |
| Lengu et al. [42] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 9 |
| Liao et al. [43] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 9 |
| Manenti et al. [44] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 9 |
| Manor et al. [45] | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 7 |
| Martin et al. [46] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 9 |
| Rezakhani et al. [47] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 9 |
| Sandrini et al. [48] | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 8 |
| Šimko et al. [49] | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 8 |
| Stonsaovapak et al. [50] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 9 |
| Turnbull et al. [51] | 1 | 1 | 0 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 8 |
| Yun et al. [52] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 8 |
| Sum of column scores. | 17 | 17 | 12 | 17 | 16 | 2 | 14 | 17 | 15 | 17 | 15 | - |
| Bias | Bias in Randomization | Bias Due to Deviations from the Intervention. | Bias Due to Missing Data | Bias in the Measurement of Outcomes | Bias in the Selection of Reports | Overall Assessment of the Risk Bias |
|---|---|---|---|---|---|---|
| De Sousa et al. [36] | Low risk of bias | Low risk of bias | Unclear risk of bias | Unclear risk of bias | Low risk of bias | Low or unclear |
| Fileccia et al. [37] | Low risk of bias | Low risk of bias | Unclear risk of bias | Unclear risk of bias | Low risk of bias | Low or unclear |
| González et al. [38] | Low risk of bias | Low risk of bias | Unclear risk of bias | Low risk of bias | Low risk of bias | Low or unclear |
| He et al. [39] | Low risk of bias | Low risk of bias | Low risk of bias | Low risk of bias | Low risk of bias | Low |
| Kim et al. [40] | Low risk of bias | Unclear risk of bias | Unclear risk of bias | Low risk of bias | Low risk of bias | Low or unclear |
| Lau et al. [41] | Low risk of bias | Unclear risk of bias | Unclear risk of bias | Low risk of bias | Low risk of bias | Low or unclear |
| Lengu et al. [42] | Low risk of bias | Unclear risk of bias | Unclear risk of bias | Low risk of bias | Low risk of bias | Low or unclear |
| Liao et al. [43] | Low risk of bias | Unclear risk of bias | Unclear risk of bias | Low risk of bias | Low risk of bias | Low or unclear |
| Manenti et al. [44] | Low risk of bias | Unclear risk of bias | Unclear risk of bias | Low risk of bias | Low risk of bias | Low or unclear |
| Manor et al. [45] | Low risk of bias | Unclear risk of bias | Low risk of bias | Low risk of bias | Low risk of bias | Low or unclear |
| Martin et al. [46] | Low risk of bias | Low risk of bias | Low risk of bias | Low risk of bias | Low risk of bias | Low |
| Rezakhani et al. [47] | Low risk of bias | Low risk of bias | Low risk of bias | Low risk of bias | Low risk of bias | Low |
| Sandrini et al. [48] | Low risk of bias | Low risk of bias | Low risk of bias | Low risk of bias | Low risk of bias | Low |
| Šimko et al. [49] | Low risk of bias | Unclear risk of bias | Unclear risk of bias | Low risk of bias | Low risk of bias | Low or unclear |
| Stonsaovapak et al. [50] | Low risk of bias | Low risk of bias | Low risk of bias | Low risk of bias | Low risk of bias | Low |
| Turnbull et al. [51] | Low risk of bias | Low risk of bias | Unclear risk of bias | Low risk of bias | Low risk of bias | Low or unclear |
| Yun et al. [52] | Unclear risk of bias | Low risk of bias | Low risk of bias | Low risk of bias | Low risk of bias | Low or unclear |
| Author | Study Design | Sample CG/IG and Sex | Control Group | Age CG/IG | Treatment | Adverse Events or Side Effects | Placement of the Electrodes | Parameters Intervention Group | Results |
|---|---|---|---|---|---|---|---|---|---|
| De Sousa et al. [36] | RCT Single-blind cross-over, placebo controlled | 24/24 F: 56.25% M: 43.75% | visuospatial OLM training plus sham atDCS | 69 (7)/70 (6) | visuospatial OLM training plus atDCS | No adverse events | Anode: right temporoparietal cortex Catode: left supraorbital region | F: 3 times/week #S: 3 sessions D: 20 min CI: 1 mA | OLM training combined with atDCS improved training success only in MCI patients. The relative performance improvement was similar between MCI patients and HE participants with atDCS. No positive effect was observed after one month. Exploratory analyses indicated a positive effect on online performance but a negative effect on offline performance in MCI patients. In both groups, post hoc exploratory analyses revealed that individuals with initially low performance showed a greater benefit from atDCS. |
| Fileccia et al. [37] | RCT, single-blind, parallel, placebo-controlled | 17/17 F: 29.4% M: 70.6% | Sham tDCS | 69.7 (1.6)/71.6 (1.4) | tDCS | Slight itching sensation | Anode: left DLPFC Catode: right deltoid muscle | F: 5 times/week #S: 20 sessions D: 20 min CI: 2 mA | At follow-up, patients who received anodal stimulation demonstrated improvements in episodic verbal memory (p < 0.001), figure naming (p < 0.01), overall cognitive function (Brief Mental Deterioration Battery) (p < 0.0001), and mood (Beck Depression Inventory) (p < 0.01). |
| González et al. [38] | RCT, double-blind, parallel, placebo-controlled | 45/22 F: 72.7% M: 27.3% | Sham tDCS combined with CT | 71 (6.2)/69.8 (5.3) | tDCS combined with CT | Discomfort in two patients | Anode: left DLPFC Catode: contraleral braquioradialis muscle | F: 3 time/week #S: 9 sessions D: 30 min CI: 1.5 mA | All three groups showed improvements in global cognition and everyday memory (p < 0.017) both after the intervention and at follow-up, with the tDCS + CT group showing larger effect sizes (d > 0.94) compared to the other groups, though no significant differences were found between the groups. Regarding CT outcomes, significant differences were observed in favor of the tDCS + CT group, particularly in reducing the completion and reaction times for working memory and attention tasks (p < 0.017). |
| He et al. [39] | RCT, double-blind, parallel, placebo-controlled | 19/24 F: 74.4% M: 25.6% | Sham tDCS | 65.63 (3.53)/63.5 (4.8) | HD-tDCS | Headache, scalp pain, tingling, itching, burning, skin redness, difficulty concentrating, skin lesions, and drowsiness | Anode: left DLPFC Cathode: surrounding the anode in a 4 × 1 montage | F: 5 times/week #S: 10 sessions D: 20 min CI: 1 mA | The findings revealed that the fALFF and ReHo values were altered in various brain areas following HD-tDCS. Significant decreases in fALFF values were observed in the right Insula, right Precuneus, left Thalamus, and right Superior Parietal regions, while the right Inferior Temporal, left Fusiform, left Superior Occipital, right Calcarine, and right Angular regions exhibited notable increases in fALFF values. Significant increases in ReHo values were found in the right Inferior Temporal, left Putamen, left Middle Frontal, right Precentral, left Medial Superior Frontal, right Superior Frontal, and left Precentral regions. These results suggest that HD-tDCS can modify both the intensity and synchronization of brain activity, and that fALFF and ReHo analyses are effective tools for detecting changes in spontaneous brain activity following HD-tDCS. |
| Kim et al. [40] | RCT, double-blind, parallel, placebo-controlled | 23/14 F: 64.9% M: 35.1% | Sham stimulation | 73.1 (6.3)/76.1 (7.4) | Home-based and remotely monitored tDCS | Discomfort in some patients | Anode: left DLPFC Cathode: right DLPFC | F: 5 times/week #S: 30 sessions D: 30 min CI: 2 mA | In terms of the effects on both depressive symptoms and cognitive functions, active tDCS did not show a significant difference compared to sham tDCS. However, when compared to sham stimulation, active tDCS resulted in a decrease in delta frequency activation and an increase in beta frequency activation. Additionally, the increase in beta activity was linked to cognitive improvement, but only in the active group. |
| Lau et al. [41] | RCT, double-blind, parallel, placebo-controlled | 10/11 F: 66.7% M: 33.3% | Sham tDCS and ICCT | 69 (4.9)/72 (17.3) | tDCS and ICCT | No adverse events | Anode: left DLPFC Cathode: right supraorbital region | F: 3 times/week #S: 15 sessions D: 20 min, 40 min with cognitive training CI: 2 mA | Both groups showed improvements in global cognition, executive function, and working memory scores, but no significant interaction effects were found on cognitive outcomes. Furthermore, the group × time interactions revealed that tDCS + ICCT significantly improved dual-task gait performance, specifically in gait speed (p = 0.045), variability (p = 0.016), and dual-task cost (p = 0.039), when compared to sham + ICCT. |
| Lengu et al. [42] | RCT, double-blind, cross-over, placebo-controlled | 19/13 F: 37.5% M: 62.5% | Sham HD-tDCS | 69.26 (6.73)/71.15 (5.26) | Active HD-tDCS | No adverse events | Anode: RSPC Cathode: 4 × 1 montage | F: 2 times/week #S: 2 sessions D: 20 min CI: 2 mA | Compared to the sham condition, and after adjusting for MRS voxel overlap and right superior parietal volume, active HD-tDCS significantly increased GABA levels and decreased the glutamate-to-GABA ratio. No changes were noted in the left prefrontal control MRS voxel. While no significant correlation was found between the strength of the delivered current (measured through MRI-based computational modeling) and changes in neurometabolites, a strong positive relationship was observed between the volume of the right superior parietal cortex and changes in neurometabolites. |
| Liao et al. [43] | RCT, double-blind, parallel, placebo-controlled | 10/10 F: 65% M: 35% | Sham tDCS and Tai Chi | 73.1 (4.6)/72.6 (4.1) | Anodal tDCS and Tai Chi | No adverse events | Anode: left DLPFC Cathode: right supraorbital region | F: 3 times/week #S: 36 sessions D: 20 min, 40 min with Tai Chi CI: 2 mA | Significant interaction effects between groups were observed in the cognitive dual-task walking. The anodal tDCS group showed a greater improvement in cadence and dual-task cost of speed compared to the sham group. Combining tDCS with Tai Chi may provide additional benefits over TC alone in improving dual-task gait performance in patients with MCI. |
| Manenti et al. [44] | RCT, double-blind, parallel, placebo-controlled | 9/9 F: 45.5% M: 55.5% | Sham tDCS | 75.3 (2.2)/75.3 (4.8) | Active tDCS | Itching and irritation with light to moderate intensity | Anode: left LPFC Cathode: right supraorbital region | F: 3 times/week #S: 3 sessions D: 15 min CI: 1.5 mA | There were no significant differences in word recall performance between the active and sham groups after the last learning trial on Day 1 (p = 0.17), indicating similar baseline performance. However, the recognition task analysis showed a significant “Group” effect (p = 0.044), with the active tDCS group performing better than the sham group, and a significant “Time” effect (p = 0.020), showing decreased performance from Day 3 to Day 30. The interaction between “Group” and “Time” was not significant (p = 0.922). No significant effects were found for the “Group” (p = 0.563), “Time” (p = 0.826), or their interaction (p = 0.293) on the C criterion of the recognition task. Finally, the word recall analysis showed a significant “Time” effect (p = 0.041), indicating performance decline from Day 3 to Day 30, while “Group” (p = 0.626) and the interaction between “Group” and “Time” (p = 0.553) were not significant. |
| Manor et al. [45] | RCT, double-blind, parallel, placebo-controlled | 10/9 F: 52.6% M: 47.4% | Sham tDCS | 79 (4)/82 (4) | tDCS | Sensations under the electrode, skin redness, drowsiness and headache | Anode: left DLPFC (Brodmann Area 46) Cathode: right supraorbital region | F: 5 times/week #S: 10 sessions D: 20 min CI: 2 mA | Compared to sham, tDCS led to improvements in the total MoCA score (p = 0.03), particularly in the executive function sub-score (p = 0.002), as well as in several dual-task standing and walking metrics (p < 0.05). These effects lasted for two weeks. tDCS had no impact on the TUG for mobility or the Geriatric Depression Scale. Participants who showed greater improvements in dual-task standing posture after the first tDCS session also demonstrated larger cognitive-motor improvements after two weeks of tDCS (p < 0.04). |
| Martin et al. [46] | RCT, double-blind, parallel, placebo-controlled | 35/33 F: 66.2% M: 33.8% | CT + sham tDCS | 71.6 (6.35)/71.8 (6.39) | CT + active tDCS | Tingling, redness, mild burning and itching | Anode: left DLPFC Catode: right VLPFC | F: 3 times/week #S: 15 sessions D: 30 min CI: 2 mA | The CT + active tDCS group showed significant improvement post-treatment (p = 0.033), whereas the CT + sham tDCS group did not (p = 0.050), although there was no difference between the groups. At the 3-month follow-up, both groups exhibited significant memory improvements compared to pre-treatment (CT + active tDCS: p < 0.01; CT + sham tDCS: p < 0.01), but no significant difference was found between the groups. |
| Rezakhani et al. [47] | RCT, double-blind, parallel, placebo-controlled | 20/40 F: 36.7% M: 63.3% | Sham HD-tDCS | 69.35 (9.94)/68.65 (10.09) | Left DLPFC or DATL HD-tDCS | No adverse events | Anode group 1: left DLPFC Anode group 2: DATL Cathode both groups: right prefrontal region | F: 5 times/week #S: 10 sessions D: 20 min CI: 2 mA | MCI patients showed the highest MoCA mean scores in both the left DLPFC and DATL groups compared to the study baseline, 2 weeks after the intervention. Additionally, the MoCA mean scores for MCI patients were higher in both intervention groups than in the sham group up to 3 months post-stimulation (p ≤ 0.05). However, a decreasing trend in MoCA mean scores was observed as time progressed from the initial stimulation. Furthermore, higher QoLAD mean scores were seen in the left DLPFC and DATL groups 3 months post-stimulation, emphasizing the effectiveness of anodal HD-tDCS in enhancing the quality of life in MCI patients. |
| Sandrini et al. [48] | RCT, double-blind, parallel, placebo-controlled | 14/14 F: 60.7% M: 39.3% | Sham tDCS | 69.1 (3.4)/68.6 (4.2) | Anodal tDCS | Itching and irritation with light to moderate intensity | Anode: left LPFC Cathode: right supraorbital region | F: 3 times/week #S: 3 sessions D: 15 min CI: 1.5 mA | The results demonstrated that anodal tDCS enhanced episodic memory, as evidenced by improved delayed recall (48 h) compared to placebo stimulation. The finding that PFC-tDCS during learning can improve verbal episodic memory in the elderly suggests the potential for designing targeted neurorehabilitation protocols for conditions that impact episodic memory, such as mild cognitive impairment. |
| Šimko et al. [49] | RCT, double-blind, parallel, placebo-controlled | 18/17 F: - M: - | Sham stimulation | 72.4 (4.96) both groups | tDCS-cog | No adverse events | Anode: left DLPFC Cathode: left Middle Frontal gyrus | F: 5 times/week #S: 10 sessions D: 20 min CI: 2 mA | Our main finding showed that tDCS-cog did not produce superior after-effects compared to the sham on VOMT in individuals with MCI, as indicated by insignificant immediate and long-lasting effects. Moreover, tDCS-cog did not enhance honline training as expected. The fMRI analysis revealed changes in brain activity in the left insula, which may be associated with the tDCS-cog intervention. |
| Stonsaovapak et al. [50] | RCT, double-blind, parallel, placebo-controlled | 22/23 F: 91.1% M: 8.9% | Placebo stimulation | 69.68 (7.6)/68.39 (8.37) | atDCS | Tingling and itching sensation | Anode: left DLPFC Cathode: right supraorbital region | F: 3 times/week #S: 12 sessions D: 20 min CI: 2 mA | CANTAB results showed a significant improvement in VSA accuracy in the atDCS group at all three time points, as well as improvements in SWM and VM immediately after the first stimulation, along with a reduced VM reaction time after 12 sessions. Long-lasting effects on VSA and VM were observed 4 weeks post-treatment. |
| Turnbull et al. [51] | RCT, double-blind, parallel, placebo-controlled | 20/20 F: 60% M: 40% | Sham tDCS | 73 (7.1)/70 (6.6) | Anodal tDCS | Tingling and itching | Anode: left SMC Cathode: right orbitofrontal region | F: 5 times/week #S: 14 sessions D: 20 min CI: 1.5 mA | Generalized Estimating Equations showed no significant group-by-time interactions for either NPS measure. However, there was evidence of a reduction in patient-reported NPS (p = 0.051), decreased LSMC activation during visual attention (p = 0.087), and increased LSMC-amygdala resting-state functional connectivity (p = 0.077) in the intervention group from pre- to post-intervention. The decrease in LSMC activation (p = 0.002) and the increase in LSMC-amygdala rsFC (p = 0.030) were associated with the reduction in patient-reported NPS. Additionally, increased positive valence across sessions was significantly linked to NPS improvement related to the intervention (p < 0.001). No findings were observed for caregiver-reported NPS. The effects were more pronounced in the left postcentral gyrus compared to the left Precentral gyrus. |
| Yun et al. [52] | RCT, double-blind, parallel, placebo-controlled | 18/17 F: 68.7% M: 31.3% | Sham tDCS | 73.12 (4.25)/74.75 (7.47) | tDCS | No adverse events | Anode: left DLPFC Cathode: right DLPFC | F: 3 times/week #S: 9 sessions D: 30 min CI: 2 mA | We demonstrated that consistent and prolonged use of tDCS significantly boosted regional cerebral metabolism in MCI patients. Additionally, improvements in subjective memory satisfaction and memory strategies were only seen in the real tDCS group after 3 weeks of stimulation. |
| Effect Size | Heterogeneity | Publication Bias | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | K | N | Ns | SMD | 95% CI | p | Q (df) | I2 (p) | Funnel Plot (Egger p) | Trim and Fill | |
| Adj SMD | % var | ||||||||||
| Global cognitive function | 7 | 214 | 30.6 | 0.477 | 0.200 to 0.754 | 0.001 | 6 | 57.96 | 0.88 | 0.48 | 14.27% |
| Visual attention | 4 | 123 | 30.8 | −0.200 | −0.559 to 0.158 | 0.274 | 3 | 0.000 | 0.15 | −0.20 | 1.25% |
| Mental flexibility | 4 | 123 | 30.8 | 0.031 | −0.326 to 0.389 | 0.864 | 7 | 0.000 | 0.11 | 0.03 | 0.79% |
| Selective attention | 3 | 91 | 30.3 | 0.682 | −1.418 to 0.054 | 0.069 | 5 | 81.540 | 0.32 | −0.81 | 37.84% |
| Study Name | Subgroup Within Study | Experimental Group | Control Group | Heterogeneity | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | M | SD | n | M | SD | Q-Value | df (Q) | p-Value | I2 | ||
| Fileccia et al. [37] | MMSE | 17 | 26.6 | 0.50 | 17 | 17.0 | 25.1 | 14.27 | 6 | 0.0027 | 57.96 |
| Liao et al. [43] | MoCa | 10 | 24.9 | 3.62 | 10 | 25.3 | 3.19 | ||||
| Lau et al. [41] | MoCa | 11 | 26.6 | 17.0 | 10 | 26.7 | 2.20 | ||||
| He et al. [39] | MoCa | 20 | 26.7 | 4.10 | 15 | 24.0 | 3.10 | ||||
| Rezakhani et al. [47] | MoCa | 20 | 27.0 | 2.55 | 20 | 23.7 | 2.36 | ||||
| González et al. [38] | MoCa | 21 | 26.2 | 2.00 | 24 | 26.4 | 2.60 | ||||
| Manor et al. [45] | MoCa | 9 | 25.0 | 4.00 | 10 | 22.0 | 1.76 | ||||
| Study Name | Subgroup Within Study | Experimental Group | Control Group | Heterogeneity | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | M | SD | n | M | SD | Q-Value | df (Q) | p-Value | I2 | ||
| Liao et al. [43] | TMT-A | 10 | 44.8 | 8.99 | 10 | 51.8 | 17.0 | 1.25 | 3 | 0.740 | 0.000 |
| Lau et al. [41] | TMT-A | 11 | 48.3 | 8.90 | 10 | 52.5 | 10.3 | ||||
| Kim et al. [40] | TMT-A | 14 | 42.3 | 25.8 | 23 | 41.8 | 22.1 | ||||
| González et al. [38] | TMT-A | 21 | 45.5 | 18.1 | 24 | 48.4 | 26.0 | ||||
| Study Name | Subgroup Within Study | Experimental Group | Control Group | Heterogeneity | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | M | SD | n | M | SD | Q-Value | df (Q) | p-Value | I2 | ||
| Liao et al. [43] | TMT-B | 10 | 88.3 | 35.6 | 10 | 95.9 | 30.4 | 0.79 | 3 | 0.851 | 0.000 |
| Lau et al. [41] | TMT-B | 11 | 91.4 | 32.5 | 10 | 92.8 | 19.4 | ||||
| Kim et al. [40] | TMT-B | 14 | 86.0 | 34.7 | 23 | 86.4 | 28.8 | ||||
| González et al. [38] | TMT-B | 21 | 72.5 | 34.1 | 24 | 66.0 | 24.5 | ||||
| Study Name | Subgroup Within Study | Experimental Group | Control Group | Heterogeneity | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| n | M | SD | n | M | SD | Q-Value | df (Q) | p-Value | I2 | ||
| Liao et al. [43] | SCWT (number) | 10 | 32.2 | 5.34 | 10 | 32.4 | 9.53 | 27.09 | 5 | 0.001 | 81.5 |
| Liao et al. [43] | SCWT (time’s) | 10 | 67.3 | 11.70 | 10 | 74.2 | 18.50 | ||||
| Kim et al. [40] | Stroop test word | 14 | 96.5 | 25.80 | 23 | 91.1 | 28.20 | ||||
| Kim et al. [40] | Stroop test color | 14 | 52.1 | 26.70 | 23 | 63.4 | 27.80 | ||||
| Fileccia et al. [37] | Stroop test time | 17 | 22.1 | 4.50 | 17 | 28.7 | 9.10 | ||||
| Fileccia et al. [37] | Stroop test errors | 17 | 0.3 | 0.70 | 17 | 6.2 | 3.10 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muñoz-Perete, J.M.; Cano-Sánchez, J.; Castellote-Caballero, Y.; Vico-Rodríguez, P.; Cano-Orihuela, M.; Sánchez-Alcalá, M.; Carcelén-Fraile, M.d.C. Effectiveness of Transcranial Stimulation on Cognitive Abilities of Older Adults with Mild Cognitive Impairment. J. Clin. Med. 2025, 14, 2472. https://doi.org/10.3390/jcm14072472
Muñoz-Perete JM, Cano-Sánchez J, Castellote-Caballero Y, Vico-Rodríguez P, Cano-Orihuela M, Sánchez-Alcalá M, Carcelén-Fraile MdC. Effectiveness of Transcranial Stimulation on Cognitive Abilities of Older Adults with Mild Cognitive Impairment. Journal of Clinical Medicine. 2025; 14(7):2472. https://doi.org/10.3390/jcm14072472
Chicago/Turabian StyleMuñoz-Perete, Juan Miguel, Javier Cano-Sánchez, Yolanda Castellote-Caballero, Paulino Vico-Rodríguez, Marta Cano-Orihuela, Marcelina Sánchez-Alcalá, and María del Carmen Carcelén-Fraile. 2025. "Effectiveness of Transcranial Stimulation on Cognitive Abilities of Older Adults with Mild Cognitive Impairment" Journal of Clinical Medicine 14, no. 7: 2472. https://doi.org/10.3390/jcm14072472
APA StyleMuñoz-Perete, J. M., Cano-Sánchez, J., Castellote-Caballero, Y., Vico-Rodríguez, P., Cano-Orihuela, M., Sánchez-Alcalá, M., & Carcelén-Fraile, M. d. C. (2025). Effectiveness of Transcranial Stimulation on Cognitive Abilities of Older Adults with Mild Cognitive Impairment. Journal of Clinical Medicine, 14(7), 2472. https://doi.org/10.3390/jcm14072472