1. Introduction
Since the Danish surgeon Henrik Kehlet introduced the fast-track concept in the 1990s, it has been incorporated with increasing acceptance by all healthcare professionals involved directly or indirectly in the surgical process. The perioperative changes introduced by this concept have allowed for better postoperative outcomes, which ultimately translate to quicker recovery to the patient’s basal state [
1]. This application of fast-tracking brings evident benefits, but, currently, the concept alone is insufficient due to the increased number of comorbidities, greater frailty, and increased life expectancy of the population. For these reasons, we need better preoperative optimization of patients’ basal state, beyond minimizing possible surgical complications. To achieve this, it is necessary to improve their functional state (physical, nutritional, and psychological), as this is one of the factors involved in poor postoperative evolutions and one on which we can act [
2].
Factors such as malnutrition, frailty, sarcopenia, and anemia are particularly relevant in patients with head and neck cancer, pancreatic neoplasms, and other digestive tumors, significantly impacting surgical tolerance and prognosis. Severe malnutrition, common in these malignancies, increases the risk of infections, delays wound healing, and results in poorer response to adjuvant therapy. Sarcopenia and frailty impair the response to surgical stress, contributing to the loss of functional independence and prolonged hospital stays. Preoperative assessments, such as muscle mass measurement and physical performance tests, can help identify high-risk patients. Preoperative anemia, frequently observed in oncologic patients, is associated with an increased need for transfusions, perioperative fatigue, and worse postoperative outcomes. Strategies such as iron supplementation or erythropoietin administration can be key in its management.
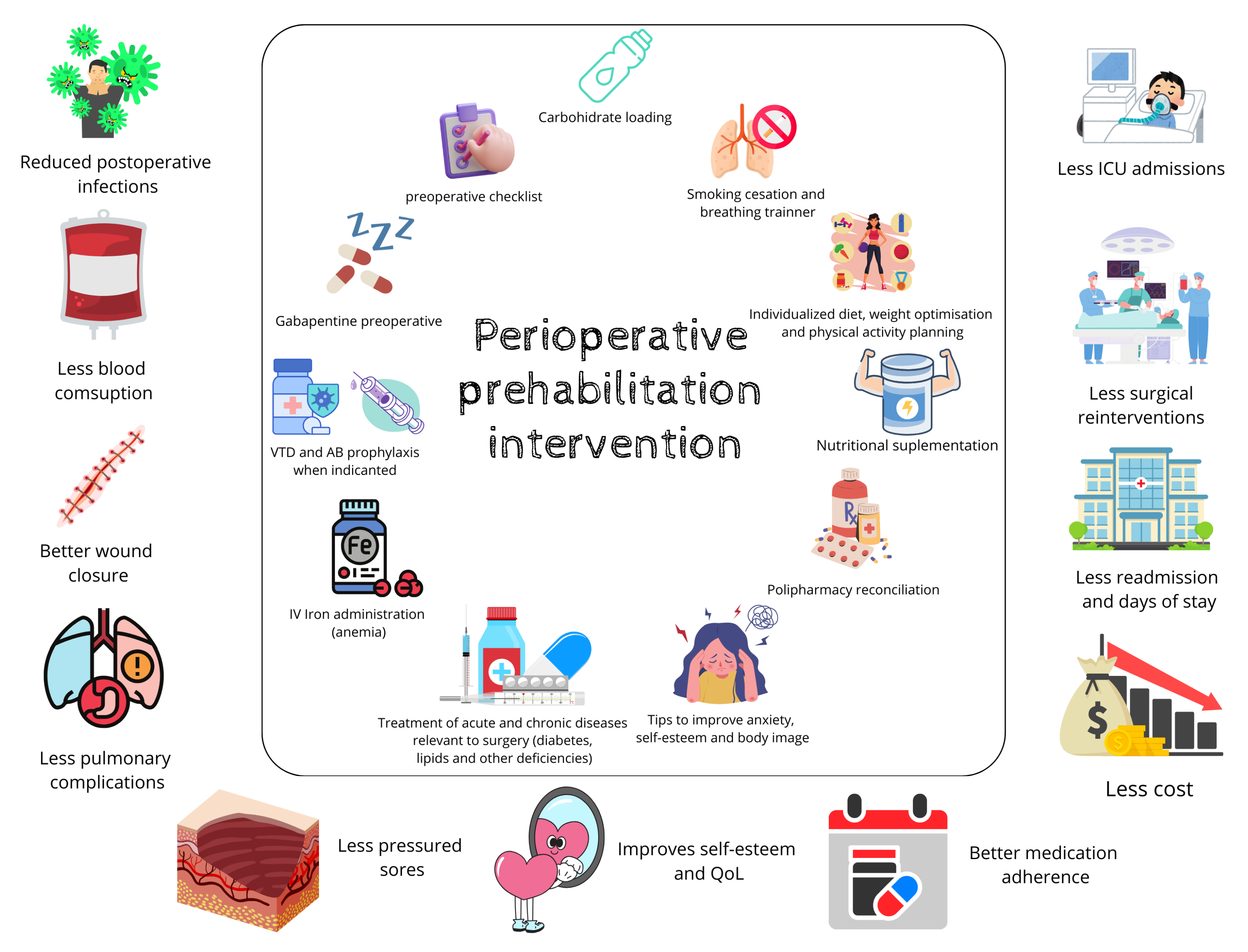
Based on these factors, prehabilitation is a program designed to improve the patient’s functional capacity before surgery by addressing three aspects: physical activity, proper nutrition, and reduction in anxiety and frustration. Several published studies support the improvement in presurgical functional condition with prehabilitation programs, which may include specific interventions such as exercise, education, smoking cessation, nutritional assessment and education, psychological support, as well as optimization of comorbidities and their treatments [
3,
4,
5,
6,
7,
8].
This preparation requires active participation from the patient, and, for this, it is necessary for them to understand the significance of their effort [
9,
10].
There are many models of how to carry out surgical prehabilitation. In some hospitals, such as the Clinic of Barcelona, this program is led by anesthesiologists and includes nursing staff from anesthesia, physiotherapists, nutritionists, and psychologists. Additionally, it is supported by other specialists like surgeons, pulmonologists, and cardiologists, who are involved throughout the surgical process. In these programs, the initial assessment is performed by the anesthesiologist, and the patient is referred to different professionals as needed [
11]. Other models are managed by the surgery department and refer the patient to various specialists according to their needs [
12]. With these models and others, the patient’s condition optimized, but this requires multiple consultations.
The results of prehabilitation in abdominal surgery are also diverse. Authors like Boden I. et al. [
13] and Martin D. et al. [
7,
14] have asserted that these programs reduce postoperative complications and hospital stays, in addition to being reliable and safe, significantly reducing annual hospital costs [
7,
13,
14,
15]. Another study conducted at the Infanta Cristina University Hospital, where prehabilitation consultation was led by nurses and internists, evidenced that, with this model, the quality of life and functionality of patients were improved, and postoperative complications, readmissions, hospital stays, and healthcare costs were reduced [
16].
Within this framework, the main goal of the present study was to evaluate cost savings at a tertiary hospital following the presented prehabilitation model. As secondary objectives, postoperative complications, length of hospital stay after the surgical intervention, and blood requirements used in the immediate and distant postoperative periods were analyzed.
2. Materials and Methods
2.1. Study Design
An observational, descriptive, comparative pre–post study was conducted at the University Hospital Infanta Cristina in Parla (Community of Madrid, Spain) on patients over 18 years old who underwent scheduled major surgery. The surgical prehabilitation program, led by an advanced practice nurse and supported by an internist, was applied to the intervention group (which received functional, clinical, and psychological interventions) and compared with the group receiving standard preoperative care.
2.2. Inclusion—Exclusion Criteria
The surgical prehabilitation program began in early 2020 for all patients on the surgical waiting list scheduled for major surgery, except those undergoing emergency surgery, hospitalized patients, or patients of the Department of Otolaryngology.
This retrospective review of patient records covered surgeries performed between 1 January 2019, and 31 December 2023. All participants had previously been included on the surgical waiting list for major surgery, including oncological procedures (digestive, urological, and gynecological surgeries) and non-oncological procedures such as orthopedic surgeries (primary hip and knee arthroplasty) and gynecological surgeries (hysterectomies). Patients who were transferred to other hospitals or canceled their surgery were excluded from this study.
2.3. Sample Size
Regarding patient recruitment, the control group included patients who underwent surgery in 2019, while the intervention group included patients who participated in the prehabilitation program and underwent surgery between 2020 (with an interruption due to COVID-19), 2021, 2022, and 2023.
2.4. Studied Variables
The following clinical and demographic variables were collected: sex, age, and oncological disease (yes or no).
In addition, descriptive variables were recorded before surgery, such as the number of consultations performed to optimize the patient. Postoperative variables related to clinical outcomes, including complications, the number of red blood cell units required, and the average hospital stay duration until discharge, were also analyzed.
Another key aspect of data collection was the cost savings generated following the implementation of the surgical prehabilitation program.
2.5. Intervention
The intervention group followed the preoperative intervention program for between 15 and 30 days before the procedure.
The process began at the moment the responsible surgeon placed the patient on the surgical waiting list, generating a referral to the Surgical Prehabilitation Unit, along with laboratory tests associated with the program to detect deficiencies, anemia, and other conditions such as diabetes and dyslipidemia, which may affect the perioperative and late postoperative periods.
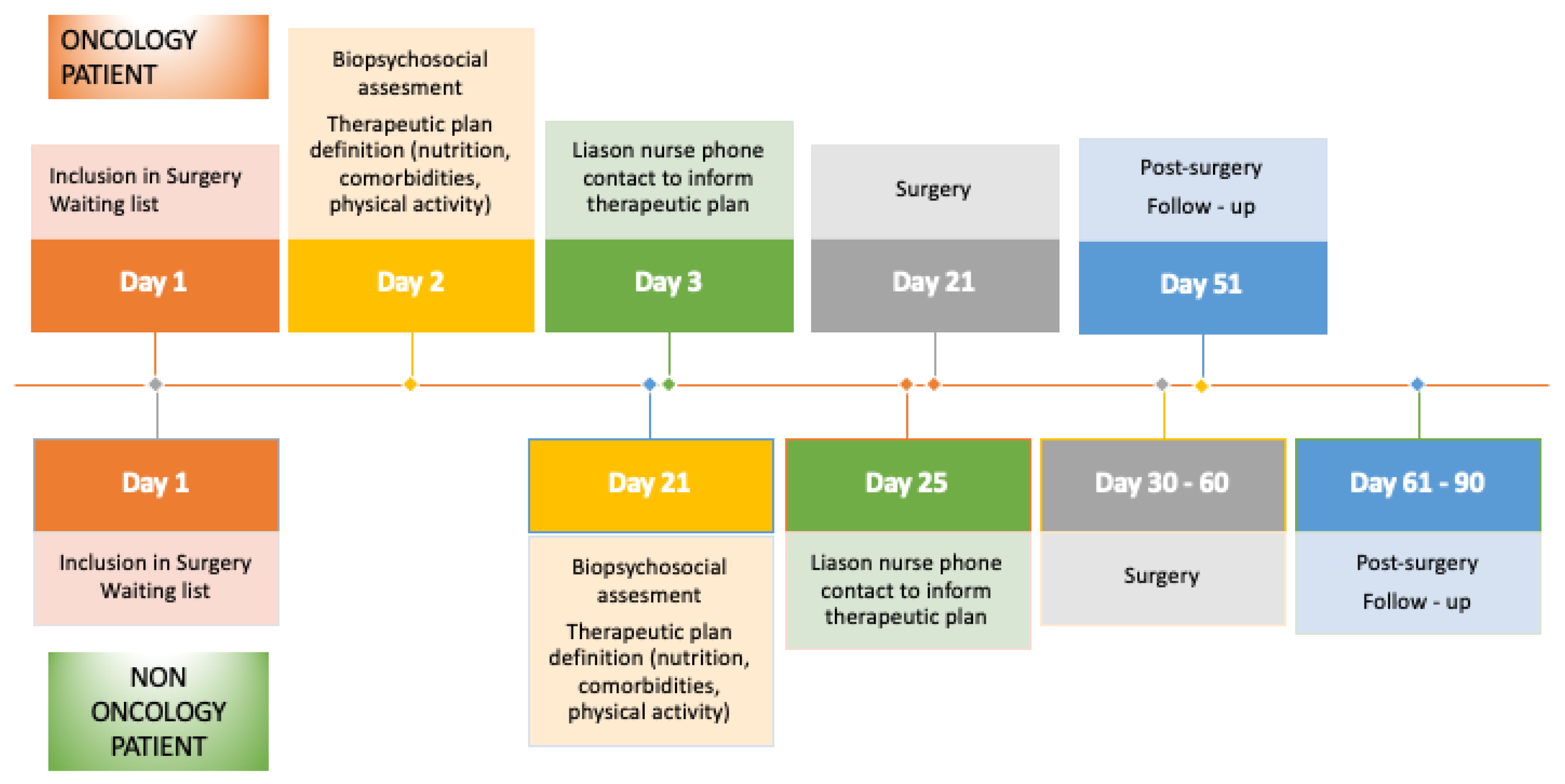
If the patient had an oncological condition, they were evaluated by an advanced practice nurse (APN) within 48 h of inclusion, prior to the anesthesia assessment, to allow for maximum optimization time, given that surgery occurred within 30 days. If the patient was scheduled to receive neoadjuvant therapy before surgery, the evaluation took place at the beginning of the treatment to prevent the deterioration caused by oncological therapy before surgery. This was due to the limited time frame available before the surgical intervention. For non-oncological surgeries, the timeline was more flexible, and evaluations were conducted 21 to 30 days before surgery (
Figure 1).
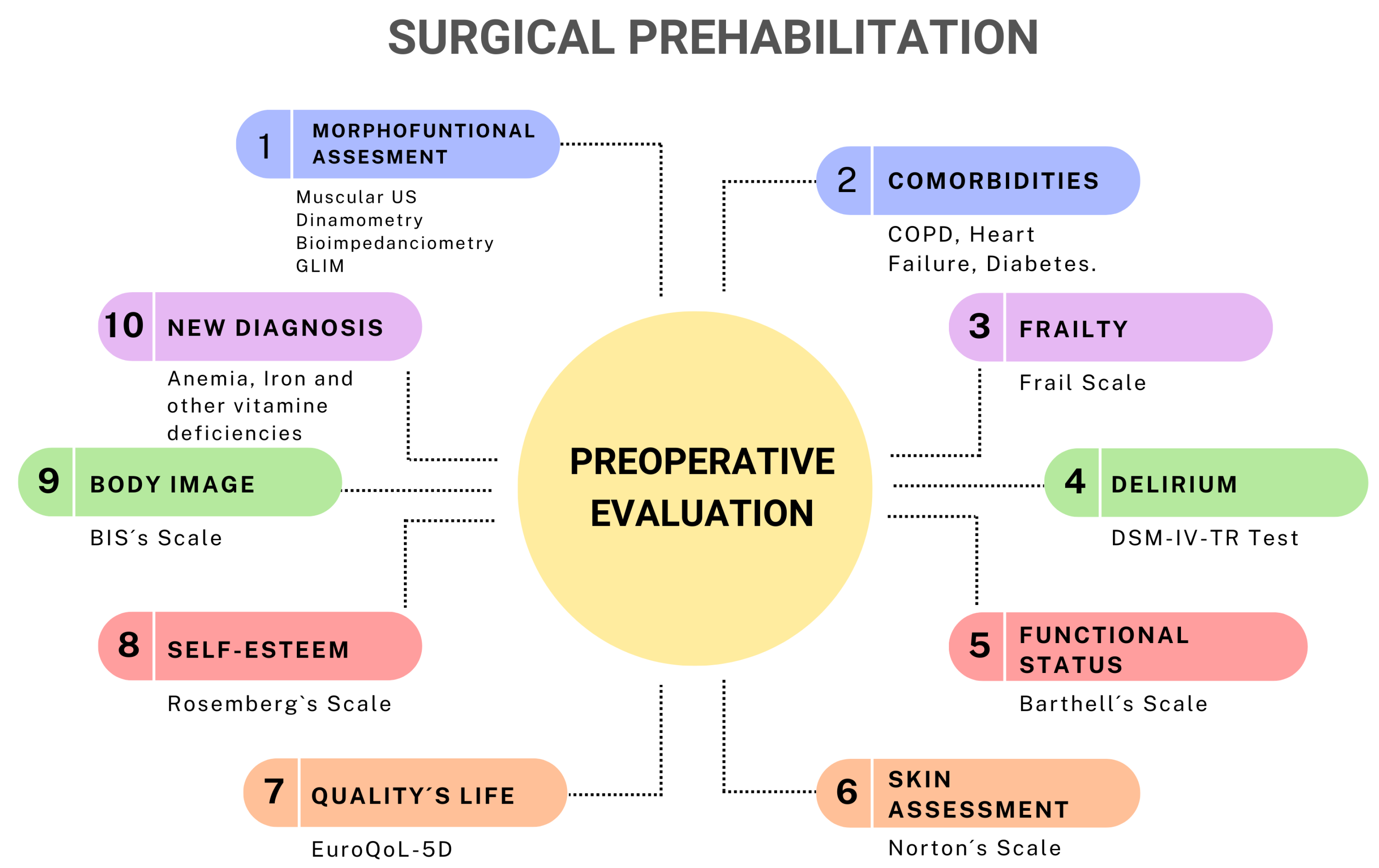
Once the patient was assessed in the prehabilitation program, they underwent comprehensive screening, including a bio-psychosocial assessment (
Figure 2), which consisted of
Nutritional assessment using GLIM criteria.
Laboratory tests including C-reactive protein (CRP), albumin, prealbumin, lymphocytes, and cholesterol.
Multifunctional assessment, including BMI, and rectus femoris muscle measurements via ultrasound, along with complete bioelectrical impedance analysis (BIA) including fat mass, muscle mass, and total body water using phase angle (PA) estimation.
Additional laboratory tests assessed hemoglobin levels, iron profile, vitamin B12, and folic acid to identify anemia (preoperative hemoglobin < 13 g/dL) and vitamin D levels, which correlate with muscle contraction.
The functional assessment included the following:
Six-meter walk test and handgrip dynamometry to evaluate muscle contraction;
Degree of dependence and frailty assessed using the Barthel index and, later, the FRAIL scale;
Pulmonary capacity assessment and optimization using a respiratory incentive device, which was provided directly during consultation to increase pulmonary capacity.
Additionally, psychological evaluation was performed by
Measuring self-esteem using the Rosenberg Self-Esteem Scale;
Assessing body image perception using the Body Image Scale (BIS) questionnaire;
Determining quality of life with the EuroQoL 5D test.
If the patient presented with low self-esteem (Rosenberg < 25 points) and/or poor quality of life (EuroQoL 5D > 5 points), they were referred to a psycho-oncologist for further assessment and intervention.
2.6. Cost-Saving Estimation
To estimate the cost savings in euros for the hospital resulting from the implementation of the program between 1 January 2020, and 30 December 2022, the inclusion visit, the visit the day before surgery, and the visit one month after surgery were considered. For the effectiveness/efficiency analysis in this study, the following cost-saving indicators were selected: hospital stay savings, the number of consultations saved (due to avoided referrals to other specialists), the number of complications prevented (including re-operation), and, finally, the number of red blood cell concentrate units saved. This allowed us to calculate the corresponding economic savings.
Complications often result in additional surgical intervention or pharmacological treatment. Taking this into consideration, the estimated cost per complication was based on DRGs 252.2 (abdominal/gastrointestinal procedure complications).
These unit prices in euros are based on Order 1975/2023 of 29 December from the Madrid Health Department, which establishes the public prices for healthcare services and activities in the Community of Madrid [
17].
2.7. Statistical Analysis
A descriptive analysis was performed for all study variables to examine their distribution. Categorical variables are described using the percentage associated with each possible response option, while quantitative variables are summarized using the mean, standard deviation, and range.
To assess the normality of the data, the Kolmogorov–Smirnov test for a single sample was applied to the quantitative variables. For comparisons between variables and hypothesis testing, the following statistical methods were used: the chi-square test for categorical variables; Student’s t-test or ANOVA for normally distributed quantitative variables; and the Mann–Whitney U test or Kruskal–Wallis test for quantitative variables that did not follow a normal distribution. Additionally, odds ratios (ORs) were calculated to estimate the relationships between binary dichotomous variables.
3. Results
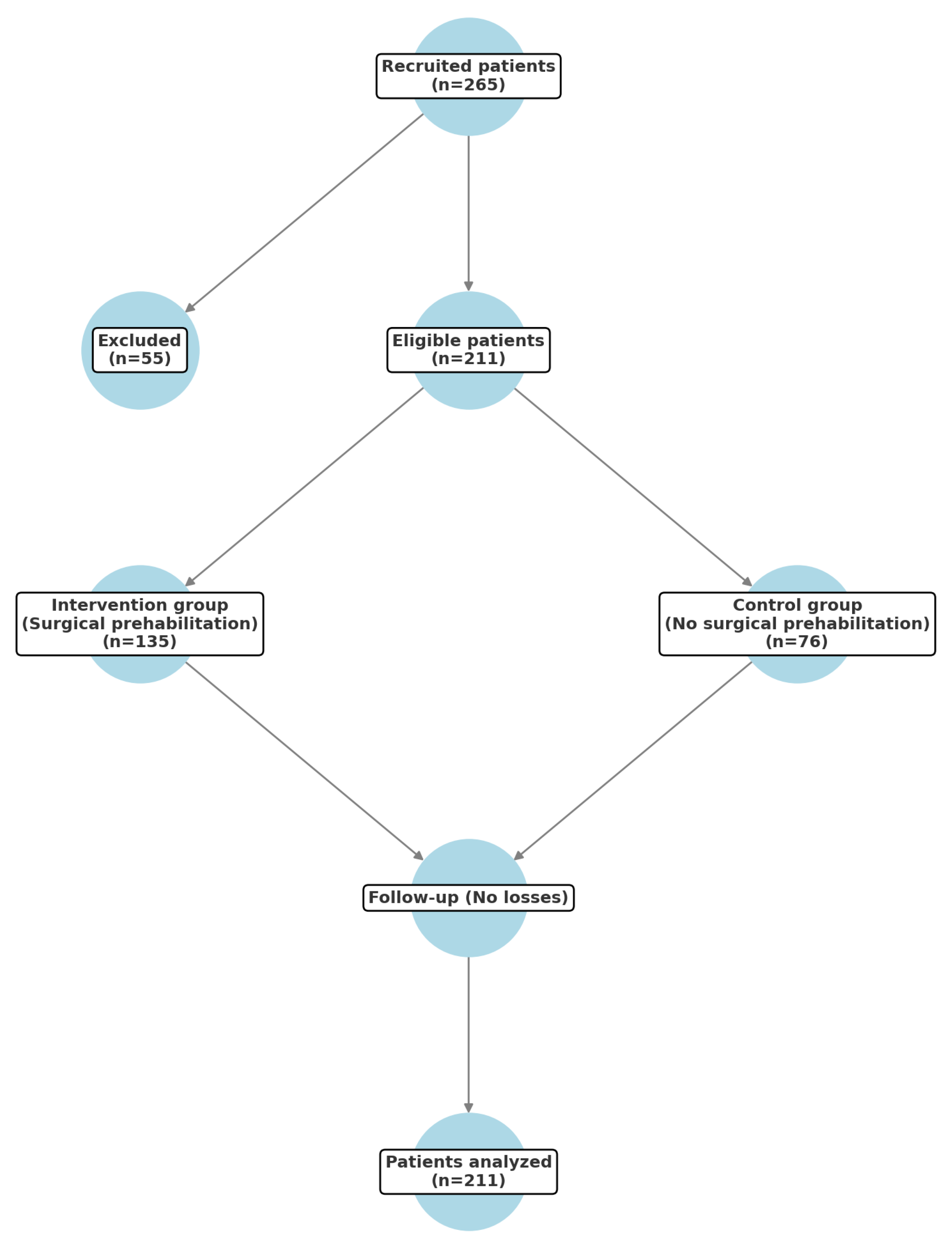
A total of 265 patients were recruited for this study, of whom 55 were excluded because they were transferred to other hospitals to expedite their surgery due to administrative reasons. The remaining 211 patients were randomized: 135 to the group that received optimization before surgery (intervention group) and 76 to the group who did not receive it (control group) (
Figure 3).
The sample consisted mostly of men (58.5%), with a mean age of 65.67 years (
Table 1). A total of 88.6% were oncology patients, and only 14.4% had received neoadjuvant therapy. On the other hand, 11.4% were non-oncological patients.
Regarding complications, statistically significant results were obtained (p < 0.001), with the control group experiencing more complications after surgery (52.6% versus 25.0% in the intervention group). The OR for complications based on whether optimization was received before surgery was 3.434 (95% CI (1.890; 6.241).
The intervention group required fewer blood transfusions than the control group (90.1% versus 75%,
p = 0.014) [OR = 3.128; 95% CI (1.445; 6.772)]. Similarly, the intervention group received fewer red blood cell concentrates than the control group (0.80 versus 2.24,
p < 0.001). The length of hospital stay and readmissions were higher in the control group compared to the intervention group (
p = 0.004,
p = 0.014, respectively) (
Table 2).
3.1. Costs
For this study, the calculation included the 135 patients in the intervention group and the 76 patients in the control group.
3.1.1. Hospital Stay Savings
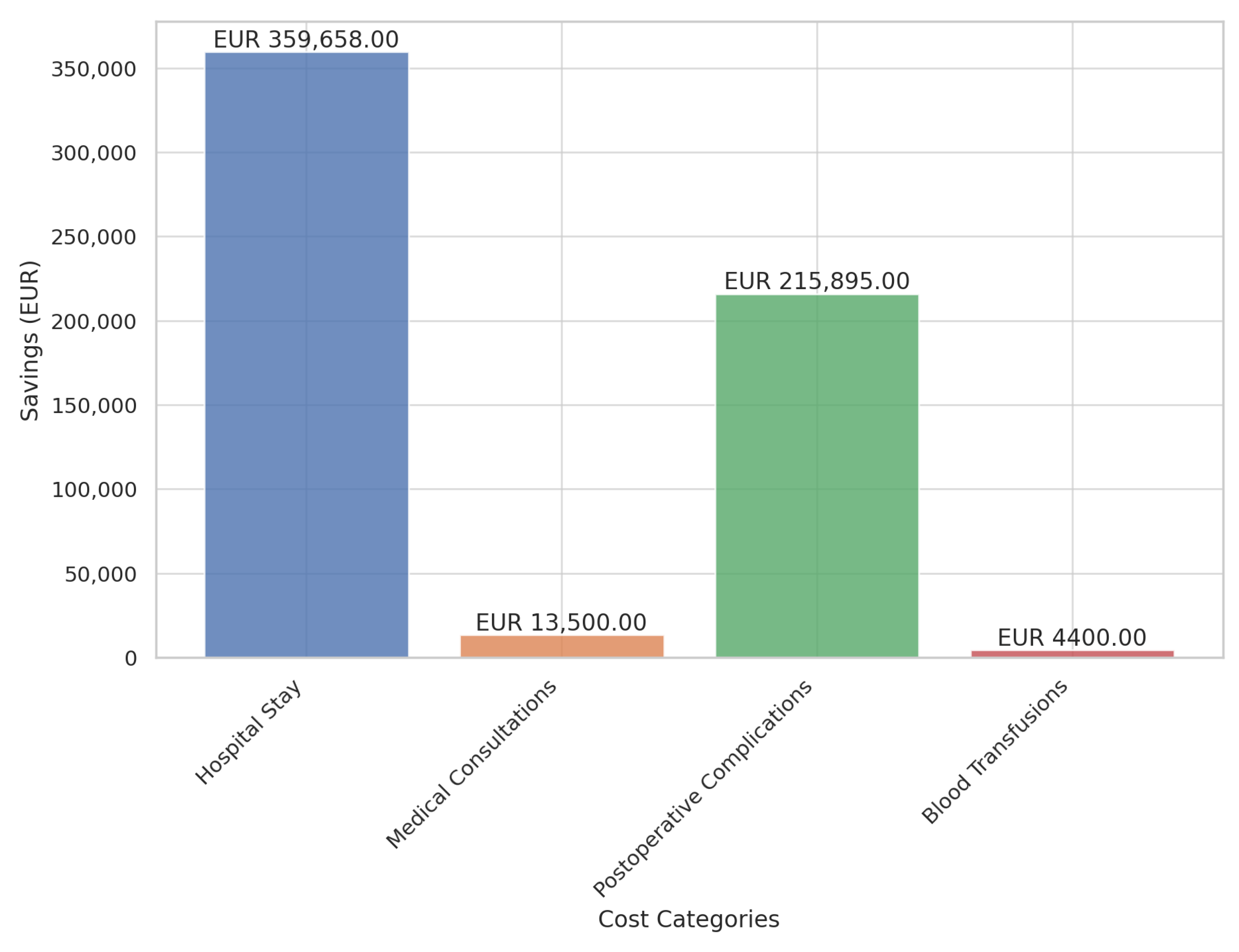
Based on the obtained data, the average hospital stay was 8.34 days for patients who participated in the prehabilitation program versus 11.63 days for those in the control. This results in a total savings of 444.15 hospital stay days, which was equivalent to 53 potential admissions for gastrointestinal, urological, gynecological, hepatobiliary, or pancreatic surgery, with an average cost per admission of EUR 6786.00. Therefore, the total savings amounted to 53 potential discharges/admissions × EUR 6786.00 per discharge, totaling EUR 359,658.00 (
Figure 4).
3.1.2. Reduction in Preoperative Consultations
The reduction in the number of consultations following the establishment of the surgical prehabilitation unit was estimated at 21.3%. This translated to a savings of 59 consultations for the 135 patients in the intervention group compared to the control group. Given that each consultation costed EUR 75.00, the total savings amounted to EUR 4425.00.
3.1.3. Reduction in Postoperative Complications
In the control group, 52.6% of patients experienced postoperative complications compared to 25.0% in the intervention (prehabilitation) group. This corresponded to avoiding postoperative complications in 37 patients. The estimated cost per complication, based on DRG 252.2 (abdominal/gastrointestinal procedure complications), was EUR 5835.00. Calculated over 37 patients, this resulted in a total savings of EUR 215,895.00 (
Figure 4).
3.1.4. Savings on Blood Transfusion Requirements
Regarding the need for red blood cell transfusions, 25.0% of the control group required transfusions compared to 9.9% in the intervention (prehabilitation group). This meant that transfusions were avoided in 20 patients, with an average of two blood-derived units per patient (costing EUR 110.00 per unit), resulting in total savings of EUR 4400.00 (
Figure 4).
3.1.5. Total Program Savings
The total savings from the program amounted to EUR 593,453.00 for the sample of 135 patients (
Table 3). See percentage at
Figure 5.
4. Discussion
Patient preparation before major surgery for people with cancer between 10 and 21 days prior to the operation and patients without cancer between 30 to 60 days prior (
Figure 2) had many beneficial effects, including enhancing nutritional status with hyperproteical supplements and carbohydrate-rich shakes for those with malnutrition, increasing lung capacity using an incentive spirometer, a physical exercise program, and reducing anemia and comorbidities through medical treatment [
18,
19,
20,
21,
22]. This study showed that adequate preoperative preparation significantly reduced the complication rate in oncological interventions (
p < 0.001). Patients undergoing this regimen not only had shorter hospital stays (
p = 0.004) but also fewer readmissions (
p = 0.014) compared to the control group. Thanks to this system, a total of 53 potential admissions were avoided, resulting in savings of EUR 359,658.
A relevant aspect is the number of visits required before surgery. National prehabilitation models (GERM Group) require intervention from multiple specialists (hematologists, endocrinologists, cardiologists, pulmonologists, physiotherapists, etc.) and a higher number of consultations, increasing systemic costs and impacting patient quality of life due to time spent on multiple appointments, averaging five visits per patient and delaying prehabilitation start. At the Hospital Infanta Cristina of Parla, the model we implemented, following IMPRICA and belonging to the GERM group, centralizes the coordination of advanced practice nursing with an internist, allowing optimization to begin within 48 h from inclusion in a surgery waiting list, requiring only one patient visit, thus improving quality of life and reducing hospital costs. This represents a reduction of 59 consultations, translating into a benefit of EUR 4425.00.
According to evidence from Schack et al. and the Spanish multimodal rehabilitation group, the risks of mortality and complications are higher for patients with untreated anemia [
23]. As suggested in the study, early optimization of patients’ hemoglobin levels reduced postoperative complications. Our study showed that those who did not undergo surgical prehabilitation had a 3.43 times lower risk of experiencing postoperative complications compared to those who did. This led to postoperative complications being avoided in 37 patients, resulting in savings of EUR 215,895.00.
With optimal hemoglobin levels, although the patient could experience bleeding during surgery, postoperative hemoglobin levels were higher than if blood products were not administered when levels are below 13 g/dL. This helped prevent decompensation in patients with heart failure, exacerbation of chronic kidney disease, or delays in postoperative rehabilitation caused by acute anemic syndrome (
Figure 6). Additionally, delayed hospital discharge could increase the risk of nosocomial infection. In summary, this translated into a reduced need for blood (25.0% in the control group versus 9.9% in the intervention group), shorter postoperative stays, fewer complications for the patient, and cost savings for the system. This resulted in savings of 40 units of blood products, generating a benefit of EUR 4400.00.
This was reflected in improved 30-day mortality rates, as described by Schack et al. in their series [
23].
The aforementioned surgical prehabilitation program, in terms of cost-effectiveness, translated into savings of EUR 593,453.00 (savings of EUR 4395.95 per patient), as evidenced in this article. This study indicates the increase in savings and supports the findings of Rombey et al. [
24]. Despite the positive results in the meta-analysis, our program at the Infanta Cristina University Hospital yielded even greater savings.
Advanced practice nurses in surgical prehabilitation clinics play a fundamental role in optimizing patients’ health status before surgery, ensuring individualized and evidence-based care. Their competencies include leadership in care planning, resource management, and coordination of the multidisciplinary team, ensuring continuity of care and patient safety, as described by Mudarra et al. [
16] Through comprehensive assessment, they identify specific needs, optimize comorbidity management, and promote self-care to improve functionality and quality of life. Additionally, they provide personalized health education, monitor treatment adherence, and facilitate communication between different levels of care. Their work contributes to the sustainability of the healthcare system by reducing hospitalization time, postoperative complications, and readmissions, thereby optimizing resource utilization. Prehabilitation clinics enhance patient and caregiver satisfaction while strengthening professional training through continuous education and the generation of knowledge via research. Their positive impact on cost reductions, improved safety, and the efficiency of surgical care highlights the importance of their role within a multidisciplinary team. In this way, advanced practice nurses not only improve clinical and economic outcomes but also foster more effective, patient-centered, and humanized healthcare, in line with what was stated by Assolari et al. [
25].
5. Study Limitations and Future Perspectives
The main limitations of our study are related to the external validity of the findings. First, the cost-savings analysis was conducted in a single hospital within the Spanish public healthcare network, which may limit the generalizability of the results to other centers with different organizational structures, care protocols, or funding sources.
Additionally, our study did not include certain surgical pathologies, such as head and neck neoplasms or cardiac surgery, among others. The exclusion of these groups prevented us from assessing the impact of surgical prehabilitation in people with different recovery profiles and preoperative needs, which may affect the applicability of our findings to a broader population.
Future studies should expand the analysis to multiple hospital centers not only within Spain but also in other countries with different healthcare financing models, including those with non-public or unsubsidized healthcare systems. This would allow for an evaluation of the economic and clinical feasibility of surgical prehabilitation in contexts with differences in funding structures and treatment accessibility, providing a more global perspective on its impact on healthcare system efficiency.
6. Conclusions
This study confirmed that implementing a surgical prehabilitation model led by an advanced practice nurse and an internist significantly reduced postoperative complications, decreased hospital length of stay, and optimized healthcare resource utilization in a tertiary hospital. Patients who participated in the prehabilitation program had a 3.43 times lower risk of postoperative complications, a reduced need for blood transfusions, and a significant decrease in hospital readmissions compared to those who did not undergo prehabilitation.
From an economic perspective, this model proved to be highly efficient by reducing unnecessary preoperative consultations and optimizing the care process, allowing for better coordination across different levels of care. Additionally, the improved preoperative preparation facilitated a faster return to patients’ baseline functionality, leading to more efficient postoperative recovery and reducing the overall impact of surgery on quality of life.
Moreover, this model reinforces the crucial role of advanced practice nursing in perioperative care management, highlighting its leadership in interdisciplinary coordination, patient education, and evidence-based decision making.
Author Contributions
Conceptualization, N.M.-G. and F.J.G.-S.; methodology, N.M.-G.; validation, N.M.-G., F.R.-R. and F.J.G.-S.; formal analysis, V.I.-I.; investigation, V.I.-I. and F.R.-R.; resources, F.J.G.-S.; data curation, N.M.-G.; writing—original draft preparation, N.M.-G.; writing—review and editing, F.J.G.-S.; visualization, F.R-R.; supervision, N.M.-G.; project administration, N.M.-G. and F.J.G.-S. All authors have read and agreed to the published version of this manuscript.
Funding
This research was funded through the funds of the IDIPHISA Foundation (Research Institute of the Puerta de Hierro University Hospital), with which the Infanta Cristina University Hospital in Madrid was affiliated, grant number [00101600007].
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee Segovia—Arana Biomedical Research Institute of Universitary Hospital Puerta de Hierro (protocol code ACT 15.18) in 19 October 2018.
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| APN | Advanced practice nurse |
| BIS | Body Image Scale |
| BMI | Body mass index |
| GERM | Grupo Español de Rehabilitación Multimodal |
| DRG | Diagnosis-related group |
| GLIM | Global Leadership Initiative on Malnutrition |
| IMPRICA | Implementación Nacional de la Vía RICA |
References
- Zargar-Shoshtari, K.; Hill, A.G. Postoperative Fatigue: A Review. World J. Surg. 2009, 33, 738. [Google Scholar] [CrossRef] [PubMed]
- Buchner, D.M.; Wagner, E.H. Preventing Frail Health. Clin. Geriatr. Med. 1992, 8, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Lorca Parraguez, L.A.; Leao-Ribeiro, I.; Martínez-Mardones, M.B.; Plasser-Troncoso, J.; Vivallos González, J.; Salas Ocaranza, R.; Torres-Castro, R. Resultados funcionales de un programa de prehabilitación en cirugía electiva de cáncer colorrectal. Rev. Cirugía 2022, 74, 276–282. [Google Scholar] [CrossRef]
- Van Rooijen, S.; Carli, F.; Dalton, S.; Thomas, G.; Bojesen, R.; Le Guen, M.; Barizien, N.; Awasthi, R.; Minnella, E.; Beijer, S.; et al. Multimodal prehabilitation in colorectal cancer patients to improve functional capacity and reduce postoperative complications: The first international randomized controlled trial for multimodal prehabilitation. BMC Cancer 2019, 19, 98. [Google Scholar] [CrossRef]
- Barberan-Garcia, A.; Ubre, M.; Pascual-Argente, N.; Risco, R.; Faner, J.; Balust, J.; Lacy, A.; Puig-Junoy, J.; Roca, J.; Martinez-Palli, G. Post-discharge impact and cost-consequence analysis of prehabilitation in high-risk patients undergoing major abdominal surgery: Secondary results from a randomised controlled trial. Br. J. Anaesth. 2019, 123, 450–456. [Google Scholar] [CrossRef]
- Jin, S.; Li, S.; Zhang, Q.; Pang, D. Preoperative physical exercise strategies for patients undergoing major abdominal cancer surgery: A scoping review. Support. Care Cancer 2021, 29, 7057–7071. [Google Scholar] [CrossRef]
- Martin, D.; Besson, C.; Pache, B.; Michel, A.; Geinoz, S.; Gremeaux-Bader, V.; Larcinese, A.; Benaim, C.; Kayser, B.; Demartines, N.; et al. Feasibility of a prehabilitation program before major abdominal surgery: A pilot prospective study. J. Int. Med. Res. 2021, 49, 03000605211060196. [Google Scholar] [CrossRef]
- Mayo, N.E.; Feldman, L.; Scott, S.; Zavorsky, G.; Kim, D.J.; Charlebois, P.; Stein, B.; Carli, F. Impact of preoperative change in physical function on postoperative recovery: Argument supporting prehabilitation for colorectal surgery. Surgery 2011, 150, 505–514. [Google Scholar] [CrossRef]
- Lawrence, V.A.; Hazuda, H.P.; Cornell, J.E.; Pederson, T.; Bradshaw, P.T.; Mulrow, C.D.; Page, C.P. Functional independence after major abdominal surgery in the elderly. J. Am. Coll. Surg. 2004, 199, 762–772. [Google Scholar] [CrossRef]
- Balagué, C.; Arroyo, A. Prehabilitation: Another Step Towards the Optimization of Surgical Patients. Cirugía Española (Engl. Ed.) 2020, 98, 175–177. [Google Scholar] [CrossRef]
- El Clínic Aplica un Programa de Prehabilitación que Reduce al 50% las Complicaciones Post-Quirúrgicas. Available online: https://www.clinicbarcelona.org/noticias/el-clinic-aplica-un-programa-de-prehabilitacion-que-reduce-al-50-las-complicaciones-en-pacientes-quirurgicos-de-alto-riesgo (accessed on 16 February 2025).
- Herrero Martín, L. Rehabilitación Multimodal en Cirugía Bariátrica: Actualización en la Prevención y Tratamiento de las Náuseas y los Vómitos Postoperatorios. 2024. Volume XIX. p. 89. Available online: https://www.revista-portalesmedicos.com/revista-medica/rehabilitacion-multimodal-en-cirugia-bariatrica-actualizacion-en-la-prevencion-y-tratamiento-de-las-nauseas-y-los-vomitos-postoperatorios/ (accessed on 16 February 2025).
- Boden, I.; Skinner, E.H.; Browning, L.; Reeve, J.; Anderson, L.; Hill, C.; Robertson, I.K.; Story, D.; Denehy, L. Preoperative physiotherapy for the prevention of respiratory complications after upper abdominal surgery: Pragmatic, double blinded, multicentre randomised controlled trial. BMJ 2018, 360, j5916. [Google Scholar] [CrossRef] [PubMed]
- Boukili, I.E.; Flaris, A.N.; Mercier, F.; Cotte, E.; Kepenekian, V.; Vaudoyer, D.; Glehen, O.; Passot, G. Prehabilitation before major abdominal surgery: Evaluation of the impact of a perioperative clinical pathway, a pilot study. Scand. J. Surg. 2022, 111, 14574969221083394. [Google Scholar] [CrossRef] [PubMed]
- Martínez, P. Prehabilitación. Un posible nuevo enfoque en la cirugía. Ocronos 2022, 5, 278. [Google Scholar]
- García, N.M.; Sánchez, F.J.G. Enfermera de práctica avanzada en Programa de Prehabilitación Quirúrgica. Metas Enfermería 2023, 26, 71. [Google Scholar] [CrossRef]
- BOCM(2023) Orden 1975/2023 de 29 de Diciembre de la Consejería de Sanidad, por la que se fijan los Precios Públicos por la Prestación de los Servicios y Actividades de Naturaleza Sanitaria de la Comunidad de Madrid. Consejería de Sanidad. BOCM [Boletin Oficial de la Comunidad de Madrid]. 30 December 2023. Available online: https://gestiona.comunidad.madrid/wleg_pub/secure/normativas/contenidoNormativa.jsf?opcion=VerHtml&nmnorma=13510&eli=true#no-back-button (accessed on 31 March 2025).
- Okam, M.M.; Koch, T.A.; Tran, M.H. Iron Supplementation, Response in Iron-Deficiency Anemia: Analysis of Five Trials. Am. J. Med. 2017, 130, 991.e1–991.e8. [Google Scholar] [CrossRef]
- Muñoz, M.; Gómez-Ramírez, S.; Besser, M.; Pavía, J.; Gomollón, F.; Liumbruno, G.M.; Bhandari, S.; Cladellas, M.; Shander, A.; Auerbach, M. Current misconceptions in diagnosis and management of iron deficiency. Blood Transfus. 2017, 15, 422. [Google Scholar] [CrossRef]
- Trasobares, M.J.; Ruiz, M.R.; Miedes, M.B.; Lagunas, M.L. Bases de la terapia de prehabilitación. Rev. Sanit. Investig. 2023, 4, 221. [Google Scholar]
- López Rodríguez-Arias, F.; Sánchez-Guillén, L.; Armañanzas Ruiz, L.I.; Díaz Lara, C.; Lacueva Gómez, F.J.; Balagué Pons, C.; Ramírez Rodríguez, J.M.; Arroyo, A. A Narrative Review About Prehabilitation in Surgery: Current Situation and Future Perspectives. Cirugía Española (Engl. Ed.) 2020, 98, 178–186. [Google Scholar] [CrossRef]
- de Luis, D.A.; Culebras, J.M.; Aller, R.; Eiros-Bouza, J.M. Surgical infection and malnutrition. Nutr. Hosp. 2014, 30, 509–513. [Google Scholar] [CrossRef]
- Schack, A.; Berkfors, A.A.; Ekeloef, S.; Gögenur, I.; Burcharth, J. The Effect of Perioperative Iron Therapy in Acute Major Non-cardiac Surgery on Allogenic Blood Transfusion and Postoperative Haemoglobin Levels: A Systematic Review and Meta-analysis. World J. Surg. 2019, 43, 1677–1691. [Google Scholar] [CrossRef]
- Rombey, T.; Eckhardt, H.; Kisilev, J.; Silzle, T.M.; Quentin, W. Cost-Effectiveness of Prehabilitation Prior to Elective Surgery: A Systematic Review of Economic Evaluations. BMC Med. 2023, 21, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Assolari, F.; Stefano, M.; Diego, L.; Alessandra, D.; Chiara, C.; Giuseppina, T.; Daniela, C.; Morales-Palomares, S.; Cangelosi, G.; Mazzoleni, B. Advanced Practice Nursing in Surgery: A Scoping Review of Roles and Educational Programs. Int. Nurs. Rev. 2024, 1–14. [Google Scholar] [CrossRef]
| Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).



 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}