

Relearning Upper Limb Proprioception After Stroke Through Robotic Therapy: A Feasibility Analysis

 ,
,  , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
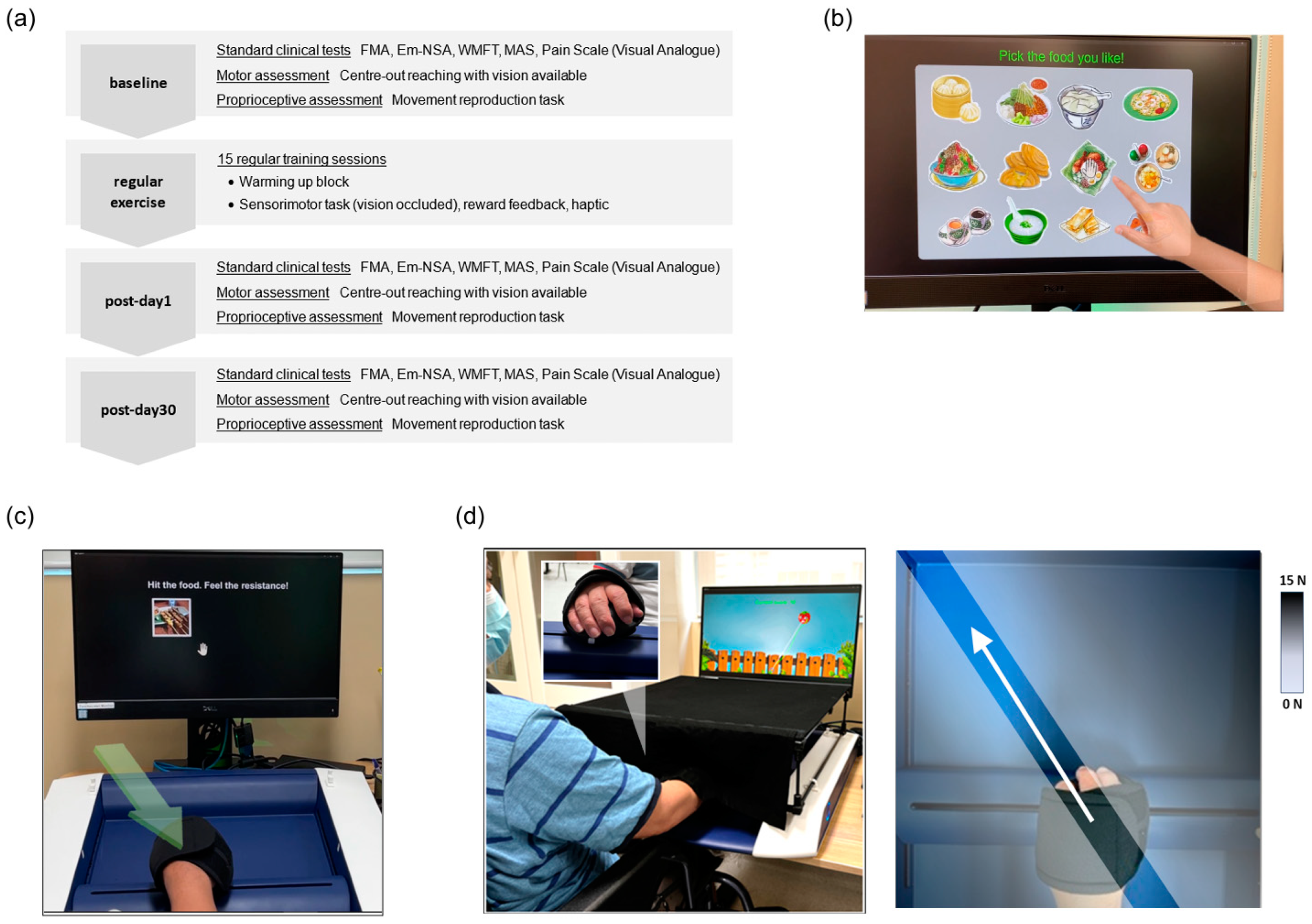
2.1. Study Design
2.2. Study Participants
2.3. Study Protocol
- (1)
- Warm-up and resistive exercise
- (2)
- Sensorimotor training task
- (3)
- Augmented feedback
2.4. Assessment Outcomes
- (1)
- Robotic-based assessments
- (2)
- Standard clinical scales
2.5. Data Analyses and Statistical Tests
2.6. Analysis of Feasibility
3. Results
3.1. Assessment Outcomes
- (1)
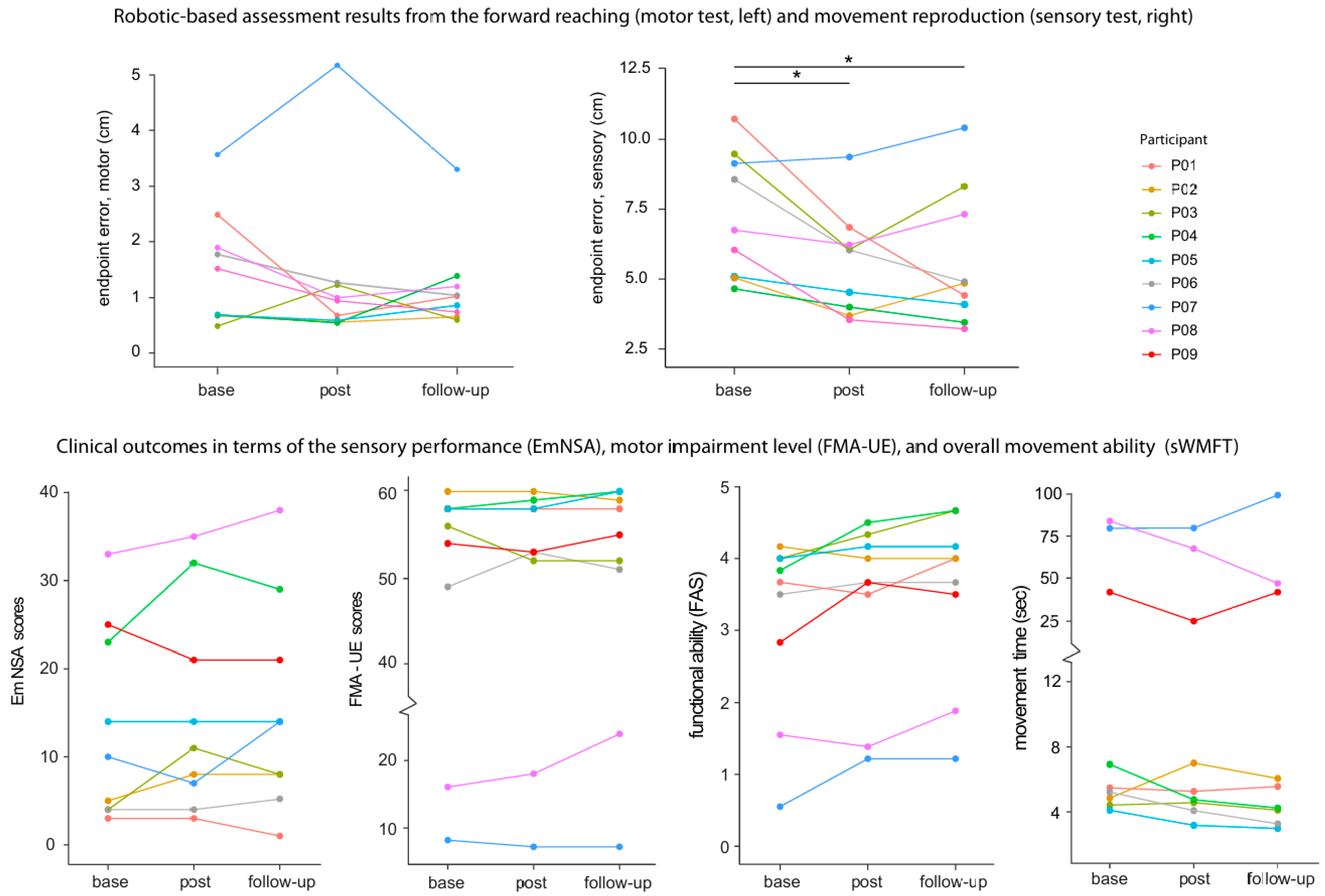
- Robotic Assessments
- (2)
- Standard Clinical Scales
3.2. Training Performance
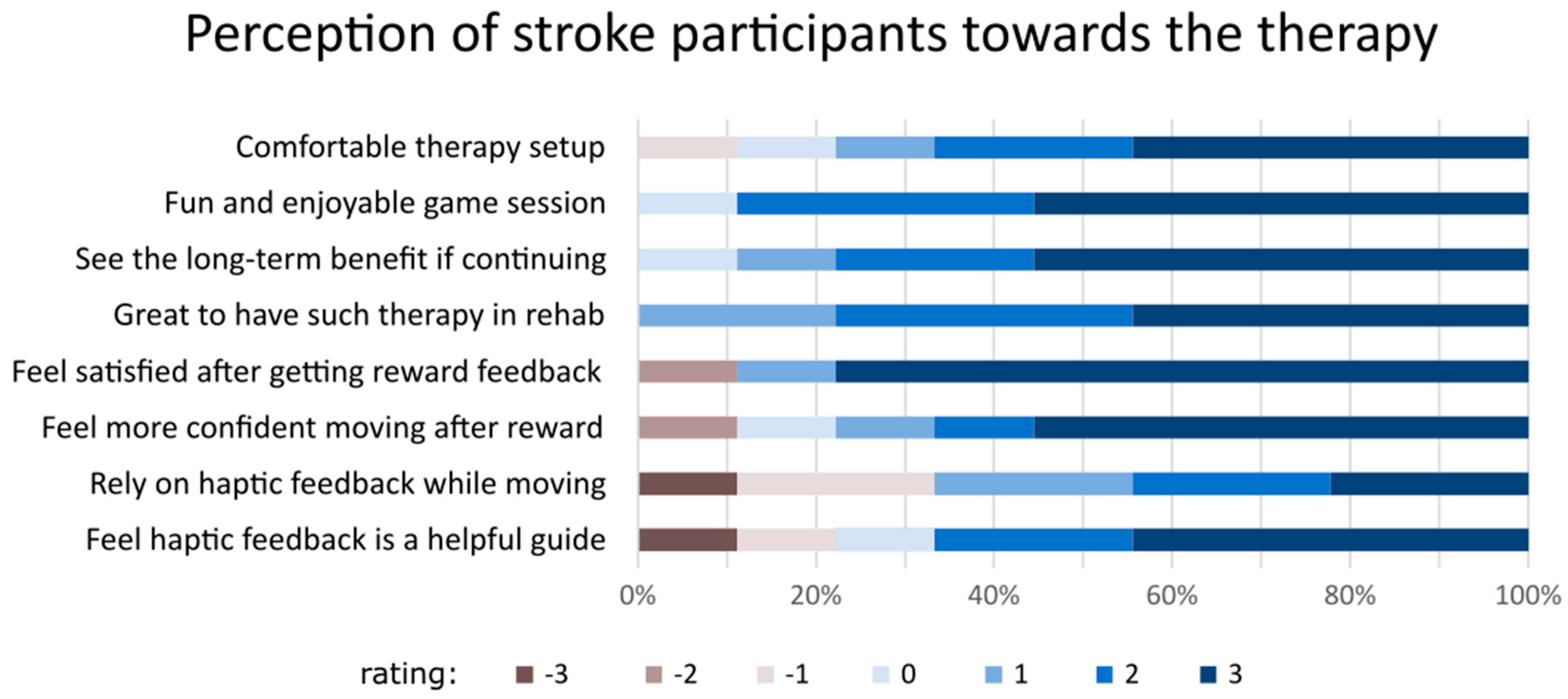
3.3. Acceptability and Feasibility Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Carey, L.M. Somatosensory Loss after Stroke. CRP 1995, 7, 51–91. [Google Scholar] [CrossRef]
- Bolognini, N.; Russo, C.; Edwards, D.J. The sensory side of post-stroke motor rehabilitation. Restor. Neurol. Neurosci. 2016, 34, 571–586. [Google Scholar] [CrossRef]
- Proske, U.; Gandevia, S.C. The Proprioceptive Senses: Their Roles in Signaling Body Shape, Body Position and Movement, and Muscle Force. Physiol. Rev. 2012, 92, 1651–1697. [Google Scholar] [CrossRef] [PubMed]
- Herter, T.M.; Scott, S.H.; Dukelow, S.P. Vision does not always help stroke survivors compensate for impaired limb position sense. J. Neuroeng. Rehabil. 2019, 16, 129. [Google Scholar] [CrossRef] [PubMed]
- Scheidt, R.A.; Stoeckmann, T. Reach adaptation and final position control amid environmental uncertainty after stroke. J. Neurophysiol. 2007, 97, 2824–2836. [Google Scholar] [CrossRef]
- Carlsson, H.; Gard, G.; Brogårdh, C. Upper-limb sensory impairments after stroke: Self-reported experiences of daily life and rehabilitation. J. Rehabil. Med. 2018, 50, 45–51. [Google Scholar] [CrossRef]
- Carey, L.M.; Matyas, T.A.; Baum, C. Effects of Somatosensory Impairment on Participation After Stroke. Am. J. Occup. Ther. 2018, 72, 7203205100p1–7203205100p10. [Google Scholar] [CrossRef] [PubMed]
- Boccuni, L.; Meyer, S.; Kessner, S.S.; De Bruyn, N.; Essers, B.; Cheng, B.; Thomalla, G.; Peeters, A.; Sunaert, S.; Duprez, T.; et al. Is There Full or Proportional Somatosensory Recovery in the Upper Limb After Stroke? Investigating Behavioral Outcome and Neural Correlates. Neurorehabilit. Neural Repair 2018, 32, 691–700. [Google Scholar] [CrossRef]
- Doyle, S.D.; Bennett, S.; Dudgeon, B. Upper limb post-stroke sensory impairments: The survivor’s experience. Disabil. Rehabil. 2014, 36, 993–1000. [Google Scholar] [CrossRef]
- Connell, L.A.; McMahon, N.E.; Adams, N. Stroke survivors’ experiences of somatosensory impairment after stroke: An Interpretative Phenomenological Analysis. Physiotherapy 2014, 100, 150–155. [Google Scholar] [CrossRef]
- Zandvliet, S.; Kwakkel, G.; Nijland, R.; van Wegen, E.V.; Meskers, C. Is Recovery of Somatosensory Impairment Conditional for Upper-Limb Motor Recovery Early After Stroke? Neurorehabilit. Neural Repair 2020, 34, 403–416. [Google Scholar] [CrossRef]
- Hoh, J.E.; Semrau, J.A. The Role of Sensory Impairments on Recovery and Rehabilitation After Stroke. Curr. Neurol. Neurosci. Rep. 2025, 25, 22. [Google Scholar] [CrossRef]
- Byrne, D.; Cahill, L.S.; Barr, C.; George, S. Assessment of sensory impairment of the upper limb post-stroke by occupational therapists within the acute setting: A mixed methods study exploring current clinical practice. Br. J. Occup. Ther. 2023, 86, 830–838. [Google Scholar] [CrossRef]
- Ingemanson, M.L.; Rowe, J.R.; Chan, V.; Wolbrecht, E.T.; Reinkensmeyer, D.J.; Cramer, S.C. Somatosensory system integrity explains differences in treatment response after stroke. Neurology 2019, 92, e1098–e1108. [Google Scholar] [CrossRef]
- Cahill, L.S.; Carey, L.M.; Mak-Yuen, Y.; McCluskey, A.; Neilson, C.; O’Connor, D.A.; Lannin, N.A. Factors influencing allied health professionals’ implementation of upper limb sensory rehabilitation for stroke survivors: A qualitative study to inform knowledge translation. BMJ Open 2021, 11, e042879. [Google Scholar] [CrossRef] [PubMed]
- Sidarta, A.; Lim, Y.; Wong, R.A.; Tan, I.O.; Kuah, C.; Ang, W.T. Current clinical practice in managing somatosensory impairments and the use of technology in stroke rehabilitation. PLoS ONE 2022, 17, e0270693. [Google Scholar] [CrossRef] [PubMed]
- Cahill, L.S.; Lannin, N.A.; Purvis, T.; Cadilhac, D.A.; Mak-Yuen, Y.; O’Connor, D.A.; Carey, L.M. What is “usual care” in the rehabilitation of upper limb sensory loss after stroke? Results from a national audit and knowledge translation study. Disabil. Rehabil. 2022, 44, 6462–6470. [Google Scholar] [CrossRef] [PubMed]
- Seo, H.G.; Yun, S.J.; Farrens, A.J.; Johnson, C.A.; Reinkensmeyer, D.J. A Systematic Review of the Learning Dynamics of Proprioception Training: Specificity, Acquisition, Retention, and Transfer. Neurorehabilit. Neural Repair 2023, 37, 744–757. [Google Scholar] [CrossRef]
- Aman, J.E.; Elangovan, N.; Yeh, I.-L.; Konczak, J. The effectiveness of proprioceptive training for improving motor function: A systematic review. Front. Hum. Neurosci. 2015, 8, 1075. [Google Scholar] [CrossRef]
- Serrada, I.; Hordacre, B.; Hillier, S.L. Does Sensory Retraining Improve Sensation and Sensorimotor Function Following Stroke: A Systematic Review and Meta-Analysis. Front. Neurosci. 2019, 13, 402. [Google Scholar] [CrossRef]
- Yeh, I.-L.; Holst-Wolf, J.; Elangovan, N.; Cuppone, A.V.; Lakshminarayan, K.; Capello, L.; Masia, L.; Konczak, J. Effects of a robot-aided somatosensory training on proprioception and motor function in stroke survivors. J. Neuroeng. Rehabil. 2021, 18, 77. [Google Scholar] [CrossRef] [PubMed]
- De Santis, D.; Zenzeri, J.; Casadio, M.; Masia, L.; Riva, A.; Morasso, P.; Squeri, V. Robot-Assisted Training of the Kinesthetic Sense: Enhancing Proprioception after Stroke. Front. Hum. Neurosci. 2015, 8, 1037. [Google Scholar] [CrossRef]
- Casadio, M.; Morasso, P.; Sanguineti, V.; Giannoni, P. Minimally assistive robot training for proprioception enhancement. Exp. Brain Res. 2009, 194, 219–231. [Google Scholar] [CrossRef]
- Gopaul, U.; Carey, L.; Callister, R.; Nilsson, M.; Vliet, P. van Combined somatosensory and motor training to improve upper limb function following stroke: A systematic scoping review. Phys. Ther. Rev. 2018, 23, 355–375. [Google Scholar] [CrossRef]
- Campolo, D.; Tommasino, P.; Gamage, K.; Klein, J.; Hughes, C.M.L.; Masia, L. H-Man: A planar, H-shape cabled differential robotic manipulandum for experiments on human motor control. J. Neurosci. Methods 2014, 235, 285–297. [Google Scholar] [CrossRef]
- Widmer, M.; Held, J.P.O.; Wittmann, F.; Valladares, B.; Lambercy, O.; Sturzenegger, C.; Palla, A.; Lutz, K.; Luft, A.R. Reward During Arm Training Improves Impairment and Activity After Stroke: A Randomized Controlled Trial. Neurorehabilit. Neural Repair 2022, 36, 140–150. [Google Scholar] [CrossRef]
- Stolk-Hornsveld, F.; Crow, J.L.; Hendriks, E.P.; van der Baan, R.; Harmeling-van der Wel, B.C. The Erasmus MC modifications to the (revised) Nottingham Sensory Assessment: A reliable somatosensory assessment measure for patients with intracranial disorders. Clin Rehabil. 2006, 20, 160–172. [Google Scholar] [CrossRef]
- Bogard, K.; Wolf, S.; Zhang, Q.; Thompson, P.; Morris, D.; Nichols-Larsen, D. Can the Wolf Motor Function Test be streamlined? Neurorehabil. Neural. Repair 2009, 23, 422–428. [Google Scholar] [CrossRef] [PubMed]
- Fugl-Meyer, A.R.; Jääskö, L.; Leyman, I.; Olsson, S.; Steglind, S. The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scand. J. Rehabil. Med. 1975, 7, 13. [Google Scholar] [CrossRef]
- Lin, K.; Hsieh, Y.; Wu, C.; Chen, C.; Jang, Y.; Liu, J. Minimal detectable change and clinically important difference of the Wolf Motor Function Test in stroke patients. Neurorehabilit. Neural Repair 2009, 23, 429–434. [Google Scholar] [CrossRef]
- Wu, C.; Fu, T.; Lin, K.; Feng, C.; Hsieh, K.; Yu, H.; Lin, C.; Hsieh, C.; Ota, H. Assessing the streamlined Wolf motor function test as an outcome measure for stroke rehabilitation. Neurorehabilit. Neural Repair 2011, 25, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Page, S.J.; Fulk, G.D.; Boyne, P. Clinically Important Differences for the Upper-Extremity Fugl-Meyer Scale in People With Minimal to Moderate Impairment Due to Chronic Stroke. Phys. Ther. 2012, 92, 791–798. [Google Scholar] [CrossRef]
- Balasubramanian, S.; Melendez-Calderon, A.; Roby-Brami, A.; Burdet, E. On the analysis of movement smoothness. J. NeuroEng. Rehabil. 2015, 12, 112. [Google Scholar] [CrossRef] [PubMed]
- Balasubramanian, S.; Melendez-Calderon, A.; Burdet, E. A robust and sensitive metric for quantifying movement smoothness. IEEE Trans. Biomed. Eng. 2012, 59, 2126–2136. [Google Scholar] [CrossRef]
- Mohamed Refai, M.I.; Saes, M.; Scheltinga, B.L.; van Kordelaar, J.; Bussmann, J.B.J.; Veltink, P.H.; Buurke, J.H.; Meskers, C.G.M.; van Wegen, E.E.H.; Kwakkel, G.; et al. Smoothness metrics for reaching performance after stroke. Part 1: Which one to choose? J. NeuroEng. Rehabil. 2021, 18, 154. [Google Scholar] [CrossRef]
- Wobbrock, J.O.; Findlater, L.; Gergle, D.; Higgins, J.J. The aligned rank transform for nonparametric factorial analyses using only anova procedures. In CHI'11: Proceedings of the SIGCHI Conference on Human Factors in Computing Systems; Association for Computing Machinery: New York, NY, USA, 2011; pp. 143–146. [Google Scholar] [CrossRef]
- Elkin, L.A.; Kay, M.; Higgins, J.J.; Wobbrock, J.O. An Aligned Rank Transform Procedure for Multifactor Contrast Tests. In UIST'21: Proceedings of the 34th Annual ACM Symposium on User Interface Software and Technology; Association for Computing Machinery: New York, NY, USA, 2021; pp. 754–768. [Google Scholar] [CrossRef]
- Canty, A.J. Resampling methods in R: The boot package. Newsl. R Proj. Vol. 2002, 2, 2–7. [Google Scholar]
- Teresi, J.A.; Yu, X.; Stewart, A.L.; Hays, R.D. Guidelines for Designing and Evaluating Feasibility Pilot Studies. Med. Care 2022, 60, 95. [Google Scholar] [CrossRef] [PubMed]
- Cambier, D.C.; De Corte, E.; Danneels, L.A.; Witvrouw, E.E. Treating sensory impairments in the post-stroke upper limb with intermittent pneumatic compression. Results of a preliminary trial. Clin. Rehabil. 2003, 17, 14–20. [Google Scholar] [CrossRef]
- Cuppone, A.V.; Squeri, V.; Semprini, M.; Masia, L.; Konczak, J. Robot-Assisted Proprioceptive Training with Added Vibro-Tactile Feedback Enhances Somatosensory and Motor Performance. PLoS ONE 2016, 11, e0164511. [Google Scholar] [CrossRef]
- Sim, S.-M.; Oh, D.-W.; Chon, S. Immediate effects of somatosensory stimulation on hand function in patients with poststroke hemiparesis: A randomized cross-over trial. Int. J. Rehabil. Res. 2015, 38, 306. [Google Scholar] [CrossRef]
- Derakhshanfar, M.; Raji, P.; Bagheri, H.; Jalili, M.; Tarhsaz, H. Sensory interventions on motor function, activities of daily living, and spasticity of the upper limb in people with stroke: A randomized clinical trial. J. Hand Ther. 2021, 34, 515–520. [Google Scholar] [CrossRef]
- Galea, M.P. Physical modalities in the treatment of neurological dysfunction. Clin. Neurol. Neurosurg. 2012, 114, 483–488. [Google Scholar] [CrossRef] [PubMed]
- Carey, L.M.; Matyas, T.A. Training of Somatosensory Discrimination After Stroke: Facilitation of Stimulus Generalization. Am. J. Phys. Med. Rehabil. 2005, 84, 428–442. [Google Scholar] [CrossRef]
- Carey, L.; Macdonell, R.; Matyas, T.A. SENSe: Study of the Effectiveness of Neurorehabilitation on Sensation: A Randomized Controlled Trial. Neurorehabilit. Neural Repair 2011, 25, 304–313. [Google Scholar] [CrossRef]
- Zbytniewska-Mégret, M.; Salzmann, C.; Ranzani, R.; Kanzler, C.M.; Gassert, R.; Liepert, J.; Lambercy, O. Design and Preliminary Evaluation of a Robot-assisted Assessment-driven Finger Proprioception Therapy. In Proceedings of the 2022 International Conference on Rehabilitation Robotics (ICORR), Rotterdam, The Netherlands, 25–29 July 2022; pp. 1–6. [Google Scholar] [CrossRef]
- Singh, N.; Saini, M.; Kumar, N.; Srivastava, M.V.P.; Mehndiratta, A. Evidence of neuroplasticity with robotic hand exoskeleton for post-stroke rehabilitation: A randomized controlled trial. J. NeuroEng. Rehabil. 2021, 18, 76. [Google Scholar] [CrossRef]
- Vahdat, S.; Darainy, M.; Thiel, A.; Ostry, D.J. A Single Session of Robot-Controlled Proprioceptive Training Modulates Functional Connectivity of Sensory Motor Networks and Improves Reaching Accuracy in Chronic Stroke. Neurorehabilit. Neural Repair 2019, 33, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Sidarta, A.; Vahdat, S.; Bernardi, N.F.; Ostry, D.J. Somatic and Reinforcement-Based Plasticity in the Initial Stages of Human Motor Learning. J. Neurosci. 2016, 36, 11682–11692. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, N.F.; Darainy, M.; Ostry, D. Somatosensory Contribution to the Initial Stages of Human Motor Learning. J. Neurosci. Off. J. Soc. Neurosci. 2015, 35, 14316–14326. [Google Scholar] [CrossRef]
- Maier, M.; Ballester, B.R.; Verschure, P.F.M.J. Principles of Neurorehabilitation After Stroke Based on Motor Learning and Brain Plasticity Mechanisms. Front. Syst. Neurosci. 2019, 13, 74. [Google Scholar]
- Kager, S.; Hussain, A.; Budhota, A.; Dailey, W.D.; Hughes, C.M.; Deshmukh, V.A.; Kuah, C.W.; Ng, C.Y.; Yam, L.H.; Xiang, L.; et al. Work with me, not for me: Relationship between robotic assistance and performance in subacute and chronic stroke patients. J. Rehabil. Assist. Technol. Eng. 2020, 6, 2055668319881583. [Google Scholar] [CrossRef]
- Rosenthal, O.; Wing, A.M.; Wyatt, J.L.; Punt, D.; Brownless, B.; Ko-Ko, C.; Miall, R.C. Boosting robot-assisted rehabilitation of stroke hemiparesis by individualized selection of upper limb movements—A pilot study. J. NeuroEng. Rehabil. 2019, 16, 42. [Google Scholar] [CrossRef]
- Giang, C.; Pirondini, E.; Kinany, N.; Pierella, C.; Panarese, A.; Coscia, M.; Miehlbradt, J.; Magnin, C.; Nicolo, P.; Guggisberg, A.; et al. Motor improvement estimation and task adaptation for personalized robot-aided therapy: A feasibility study. BioMed. Eng. OnLine 2020, 19, 33. [Google Scholar] [CrossRef] [PubMed]
- Maura, R.M.; Rueda Parra, S.; Stevens, R.E.; Weeks, D.L.; Wolbrecht, E.T.; Perry, J.C. Literature review of stroke assessment for upper-extremity physical function via EEG, EMG, kinematic, and kinetic measurements and their reliability. J NeuroEng. Rehabil. 2023, 20, 21. [Google Scholar] [CrossRef] [PubMed]
- Dukelow, S.P.; Herter, T.M.; Moore, K.D.; Demers, M.J.; Glasgow, J.I.; Bagg, S.D.; Norman, K.E.; Scott, S.H. Quantitative Assessment of Limb Position Sense Following Stroke. Neurorehabilit. Neural Repair 2010, 24, 178–187. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case No. | Gender | Age | Duration of Stroke | Nature of Stroke | Affected Limb |
|---|---|---|---|---|---|
| P01 | Male | 65 | 4 years | Haemorrhagic | Right |
| P02 | Male | 61 | 4 years | Haemorrhagic | Right |
| P03 | Male | 71 | 3 years | Haemorrhagic | Left |
| P04 | Female | 38 | 3 years | Haemorrhagic | Right |
| P05 | Male | 39 | 2 years | Haemorrhagic | Right |
| P06 | Male | 57 | 1 year | Haemorrhagic | Right |
| P07 | Male | 63 | 7 years | Ischemic | Left |
| P08 | Female | 74 | 6 years | Ischemic | Right |
| P09 | Male | 58 | 2 years | Ischemic | Left |
| Case No. | Sensory (Post) | Sensory (Follow-Up) | Functions (Post) | Functions (Follow-Up) | Task Time (Post) | Task Time (Follow-Up) | Impairment (Post) | Impairment (Post) |
|---|---|---|---|---|---|---|---|---|
| P01 | 0 | −2 | −0.17 | 0.33 | −0.22 | 0.08 | 0 | 0 |
| P02 | 3 | 3 | −0.17 | −0.17 | 2.17 | 1.21 | 0 | −1 |
| P03 | 7 | 4 | 0.33 | 0.67 | 0.15 | −0.32 | −4 | −4 |
| P04 | 9 | 6 | 0.67 | 0.83 | −2.18 | −2.70 | 1 | 2 |
| P05 | 0 | 0 | 0.17 | 0.17 | −0.93 | −1.13 | 0 | 2 |
| P06 | 0 | 1 | 0.17 | 0.17 | −1.14 | −1.96 | 4 | 2 |
| P07 | −3 | 4 | 0.67 | 0.67 | 0.15 | 19.78 | −1 | −1 |
| P08 | 2 | 5 | −0.17 | 0.33 | −16.44 | −37.12 | 2 | 8 |
| P09 | −4 | −4 | 0.83 | 0.67 | −17.22 | 0 | −1 | 1 |
| Mean diff | 1.56 (−1.22, 4.11) | 1.89 (−0.11, 4.11) | 0.26 (0.02, 0.50) | 0.41 (0.22, 0.61) | −3.96 (−7.92, 1.08) | −2.46 (−10.93, 7.63) | 0.22 (−1.11, 1.56) | 1.00 (−1.00, 2.89) |
| MCID | 0.20 | 0.20 | −1.50 | −1.50 | 7.25 | 7.25 |
| Indicator | Information |
|---|---|
| Recruitment | Screening was subject to COVID-19 restrictions. Of the 24 stroke clients, only 10 (41.66%) met the inclusion criteria, though 1 declined to enrol. Among those ineligible, 14 (58.33%) either did not exhibit any sensory deficits or were excluded due to excessive shoulder pain, insufficient muscle strength, or poor cognitive function. |
| Trial scheduling | All participants made their best effort to attend therapy sessions three times per week. However, as community-dwelling clients, their schedules were occasionally disrupted by routine commitments. Sessions were rescheduled due to factors such as vaccinations, medical checkups, or feeling unwell. |
| Tolerability and adherence | The study procedures were well tolerated by all participants. No adjustment to the therapy protocol was necessary, as each of the 10 blocks was sufficiently brief and manageable. One participant (P05) experienced frustration with failed trials early in training and reported some sleep disturbances. However, all participants successfully completed all sessions without any dropouts. |
| Manpower | Two personnel were required for the study. During training, the study team noted that participants occasionally failed to notice their hands slipping off the handle. To manage this, the accompanying therapist checked the grip through the side gap of the arm cover after each training block, ensuring proper hand positioning. This shows that a minimum of one trained personnel was necessary for the intervention. A separate therapist not involved in the training conducted the baseline, post-training, and follow-up assessments. |
| Adverse events | No adverse events, physical injury, or death were reported. |
| Training gain | A positive training gain was seen in each individual (see main text and Figure 3), except for P05. |
| Assessment outcomes | The clinical data showed a degree of variability, where not all participants improved beyond the MCID. In contrast, the robotic-based measure of sensory performance, considered to be more sensitive, showed a significant difference after training (see main text and Figure 2). These improvements were not observed in the motor test, suggesting that the primary benefit of the training is sensory rather than motor. |
| Perception of participants | This is reflected in the result of the acceptability questionnaire (see main text and Figure 4 below). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sidarta, A.; Lim, Y.C.; Kuah, C.W.K.; Chua, K.S.G.; Ang, W.T. Relearning Upper Limb Proprioception After Stroke Through Robotic Therapy: A Feasibility Analysis. J. Clin. Med. 2025, 14, 2189. https://doi.org/10.3390/jcm14072189
Sidarta A, Lim YC, Kuah CWK, Chua KSG, Ang WT. Relearning Upper Limb Proprioception After Stroke Through Robotic Therapy: A Feasibility Analysis. Journal of Clinical Medicine. 2025; 14(7):2189. https://doi.org/10.3390/jcm14072189
Chicago/Turabian StyleSidarta, Ananda, Yu Chin Lim, Christopher Wee Keong Kuah, Karen Sui Geok Chua, and Wei Tech Ang. 2025. "Relearning Upper Limb Proprioception After Stroke Through Robotic Therapy: A Feasibility Analysis" Journal of Clinical Medicine 14, no. 7: 2189. https://doi.org/10.3390/jcm14072189
APA StyleSidarta, A., Lim, Y. C., Kuah, C. W. K., Chua, K. S. G., & Ang, W. T. (2025). Relearning Upper Limb Proprioception After Stroke Through Robotic Therapy: A Feasibility Analysis. Journal of Clinical Medicine, 14(7), 2189. https://doi.org/10.3390/jcm14072189