
A Multidisciplinary Approach of Type 1 Diabetes: The Intersection of Technology, Immunotherapy, and Personalized Medicine

 , , , ,
, , , ,
Abstract
1. Introduction
2. The Role of Smart Technology in T1D: CGM, Insulin Pumps, and AI Systems
- Fasting glucose levels should be maintained between 3.9 and 7.8 mmol/L (70–140 mg/dL) [40].
- For children under 7 years of age, a tighter time interval is recommended, ensuring that at least 50% of CGM readings fall within 3.9–7.8 mmol/L (70–140 mg/dL) or 70% within the range of 3.9–10 mmol/L (70–180 mg/dL) [41].
- ISPAD recommends maintaining HbA1c levels below 53 mmol/mol (<7.0%) to prevent long-term microvascular and macrovascular complications [40].
2.1. Continuous Glucose Monitoring (CGM) Systems
- Professional CGM: data are recorded over several days and can be accessed only by healthcare providers, typically for retrospective analysis [46].
- Personal CGM: Users can view glucose levels in real time, allowing for immediate intervention. This category includes the following:
2.2. Continuous Subcutaneous Insulin Delivery (CSII) Systems
- Basal insulin infusion: a continuous supply of small amounts of rapid-acting insulin throughout the day and night to maintain stable glucose levels;
- Bolus insulin delivery: a single, larger dose of insulin given at mealtimes or to correct high blood glucose levels [51].
- Traditional tube pumps: these pumps feature an insulin reservoir connected to the body via a thin tube, which leads to a cannula (needle or catheter) inserted under the skin.
- Patch pumps: These devices are directly attached to the skin and do not require tubing. Insulin is delivered via a short cannula that penetrates the skin.
- Closed-loop pumps (artificial pancreas systems): these fully automated systems combine an insulin pump with a CGM sensor, continuously adjusting insulin doses based on real-time glucose data.
- Integrated CGM pumps: while not entirely automated, these pumps work in conjunction with CGM sensors and can suggest insulin dose adjustments based on glucose trends.
- Mechanical pumps: these are simpler devices that provide fixed and programmable insulin delivery, often used in specific clinical scenarios [46].
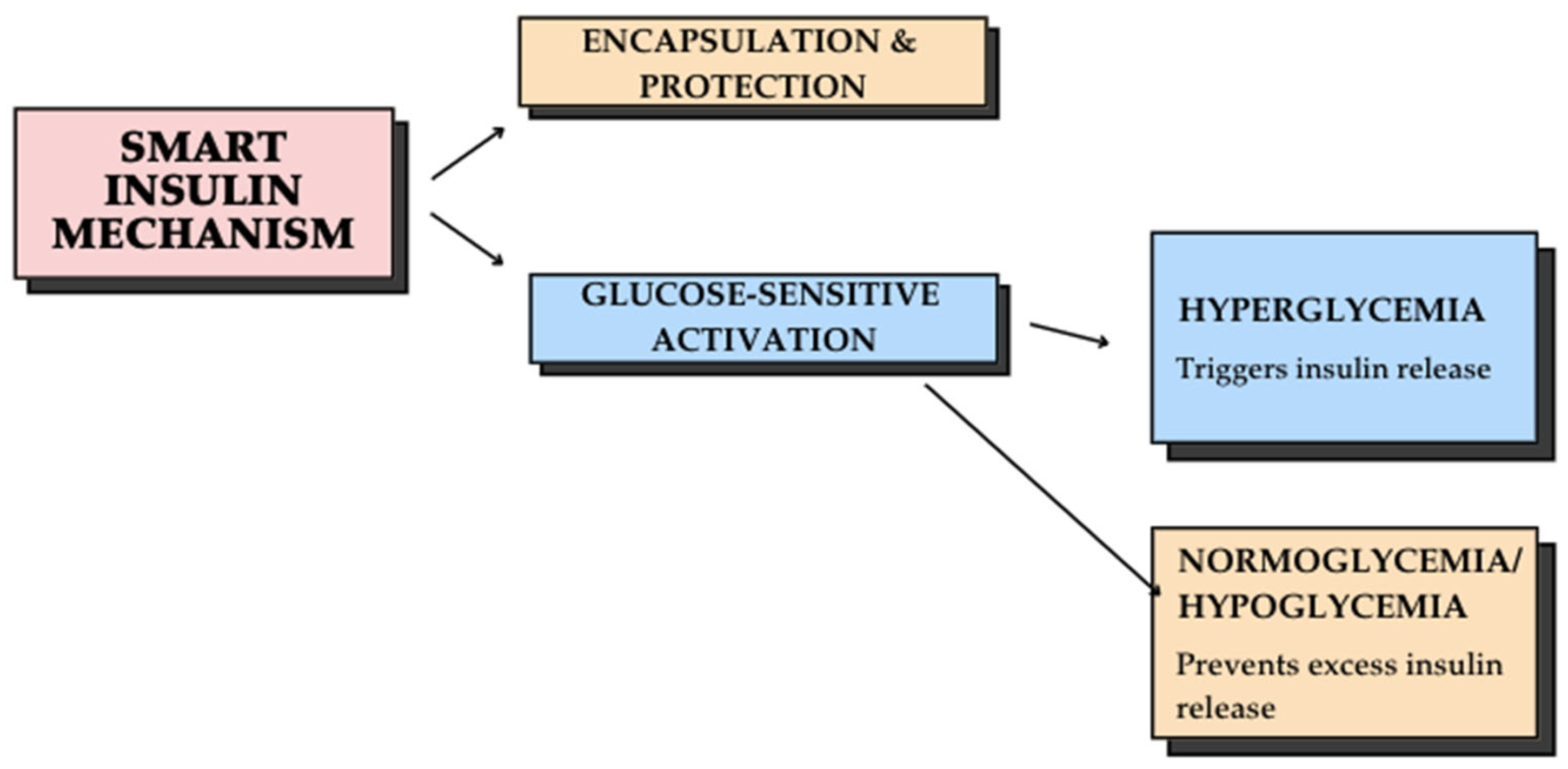
2.3. Glucose-Responsive Insulin Delivery System and Artificial Intelligence (AI) in Diabetes Management
2.4. Supporting Adolescents in T1D Self-Management: Education and Digital Tools
2.4.1. The Role of Digital Storytelling in Diabetes Education
2.4.2. Mobile Technology and IT Innovations in T1D Management
2.4.3. The Role of Telemedicine in T1D Management
- Reduced patient-physician interaction: personal contact is a key element in establishing trust and improving patient adherence, which may be compromised in virtual care settings [124].
- Technological barriers: some patients and healthcare providers struggle with limited digital literacy, affecting their ability to effectively utilize telemedicine platforms [123].
2.5. Expanding Diabetes Technology Worldwide: Challenges and Opportunities
3. Future Solutions in the Therapy of T1D
3.1. Wearable Biosensors: Non-Invasive Continuous Monitoring
- Real-time glucose tracking via smartphone applications;
- Automated alerts when glucose levels exceed pre-set thresholds;
- Data storage and analysis to enhance long-term glycemic management.
3.2. Optical Coherence Tomography (OCT) for Glucose Monitoring
- Completely non-invasive, eliminating the need for needles or skin punctures;
- High imaging precision enables real-time tracking of glucose fluctuations;
- Enhanced patient comfort is particularly beneficial for pediatric patients [142].
3.3. Bioimpedance-Based Glucose Monitoring
- Bioimpedance offers a stable and precise estimation of glucose levels, particularly within an optimal frequency range below 40 kHz [145].
- CGM devices based on bioimpedance include sensors, analytical algorithms, and measurement circuits, offering a potential alternative to traditional CGM systems [138].
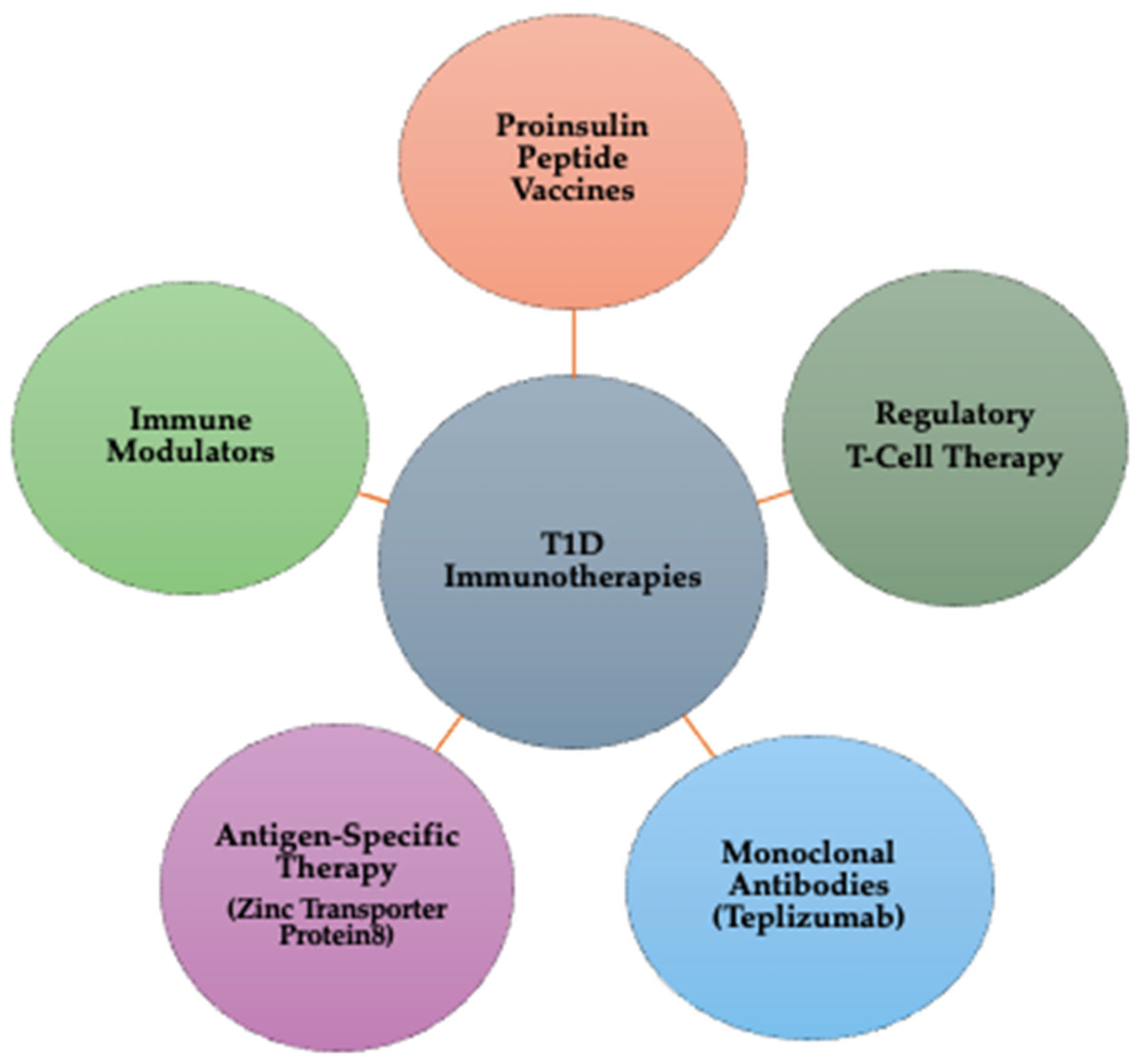
3.4. Immunotherapy: Modulating the Immune Response in T1D
- Proinsulin peptide (PPI) vaccines: Proinsulin peptide vaccines train the immune system to tolerate beta cells instead of attacking them. By exposing the immune system to proinsulin fragments, these vaccines help induce immune tolerance, potentially preventing or delaying T1D onset. Clinical stage: phase I/II trials are ongoing to assess efficacy and safety [17].
- Regulatory T-cell (Treg) therapy: Tregs are a specialized subset of immune cells responsible for suppressing autoimmune reactions. In Treg therapy, patient-derived Tregs are extracted, expanded in a laboratory, and reinfused to restore immune balance. This approach reduces beta cell destruction and modulates immune responses, helping preserve endogenous insulin production. Clinical stage: multiple Phase I/II clinical trials are investigating Treg therapy in newly diagnosed T1D patients [147].
- Monoclonal antibodies (teplizumab therapy): Teplizumab is a monoclonal antibody therapy that targets CD3 on T-cells, effectively by blocking key immune pathways involved in the attack on beta cells, delaying disease progression in newly diagnosed individuals, and reducing inflammation and modulating the immune system’s response to beta cells. Clinical stage: Teplizumab has received FDA approval for delaying the onset of T1D in at-risk individuals. Ongoing studies continue evaluating long-term efficacy [16,148].
- Antigen-specific therapy— Zinc Transporter Protein 8 (ZnT8) targeting: ZnT8 is an autoantigen present in prediabetic and diabetic patients, making it a critical target for immunotherapy. ZnT8-based treatments help regulate immune responses, potentially protecting beta cells from further autoimmune damage. Early diagnosis strategies using ZnT8 autoantibodies can also improve predictive screening for T1D risk. Clinical stage: preclinical and early-stage Phase I trials [149,150];
- Immune modulators: Immune modulation aims to modify the immune response to maintain beta cell function and prevent or delay the onset of the disease. Abatacept, a T-cell co-stimulation blocker, reduces inflammation and lowers the likelihood of autoimmune destruction. Other immunomodulatory drugs are currently being tested to improve beta cell survival and enhance long-term glycemic control. Clinical stage: phase II/III trials are evaluating the efficacy in delaying T1D progression [151].
3.5. Stem Cell Therapy
- Embryonic stem cells (ESCs) are pluripotent cells capable of differentiating into any cell type, including beta cells. These cells have shown great potential for beta cell regeneration but raise ethical concerns and a risk of immune rejection [153];
- Induced pluripotent stem cells (iPSCs) are reprogrammed adult cells that mimic ESCs, offering a patient-specific approach. These cells are generated from the patient’s own cells, reducing the risk of immune system rejection and provide an ethically viable alternative to embryonic stem cells [154];
- Mesenchymal stem cells (MSCs) are found in bone marrow, adipose tissue, and umbilical cord blood. These cells exhibit anti-inflammatory and immunomodulatory properties, making them valuable in autoimmune diseases like T1D. Also, they differentiate into multiple cell types, including insulin-producing beta cells [155,156].
3.6. Gene Therapy
- Gene transfer for beta-cell regeneration uses viral vectors (e.g., adenoviruses, lentiviruses) to introduce essential transcription factors like PDX1 and MAFA. These factors play a critical role in beta cell development and regeneration, restoring insulin production in individuals with T1D [135].
- CRISPR-Cas9 gene editing is a revolutionary gene-editing technique that enables precise genetic modifications. This gene can correct mutations in the insulin gene to ensure proper insulin production. Also, it allows the introduction of protective sequences to shield beta cells from autoimmune destruction [157].
- Gene therapy for localized immunosuppression delivers therapeutic genes that produce immunosuppressive proteins (e.g., IL-10 and TGF-beta). Also, it protects beta cells from autoimmune attacks without compromising the body’s immune defense against infections [157].
- Alpha-to-beta cell conversion introduces specific genes like ARX and PDX1 to reprogram glucagon-producing alpha cells into insulin-producing beta cells. This technique offers an alternative source of functional beta cells, restoring natural insulin production [18].
3.7. Contact Lenses for CGM
3.8. Microbiome and Personalized Medicine
3.9. The Role of Probiotics in T1D Management
3.10. Nanomedicines Based on Trace Elements in Diabetes Management
- Blood glucose regulation: trace element nanoparticles help lower blood glucose levels, reducing hyperglycemia.
- Improved insulin sensitivity: these nanoparticles enhance cellular responsiveness to insulin, allowing for better glucose uptake and utilization.
- Enhanced insulin secretion: certain trace element-based nanomedicines stimulate pancreatic β-cells to produce and release insulin more efficiently.
- Alleviation of glucose intolerance: by modulating glucose absorption and utilization, these nanoparticles help prevent postprandial glucose spikes.
- Lipid profile improvement: studies have shown that trace element nanoparticles can positively influence lipid metabolism, reducing the risk of dyslipidemia in diabetes.
- Anti-inflammatory and antioxidant properties: nanoparticles derived from trace elements exhibit anti-inflammatory and antioxidant effects, which are crucial in preventing β-cell damage and mitigating diabetes-related oxidative stress [137].
4. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| T1D | Type 1 diabetes |
| CGM | Continuous glucose monitoring |
| AI | Artificial intelligence |
| CRISPR | Clustered Regularly Interspaced Short Palindromic Repeats |
| WHO | World Health Organization |
| IDF | International Diabetes Federation |
| ISPAD | International Society for Pediatric and Adolescent Diabetes |
| CSII | Continuous subcutaneous insulin infusion |
| FDA | Food and Drug Administration |
| IT | Information technology |
| MAFA | Musculoaponeurotic fibrosarcoma oncogene homolog A |
| PDX1 | Pancreatic and duodenal homeobox 1 |
| ARX | Aristaless-related homeobox |
| DKA | Diabetic ketoacidosis |
| SGLT2 | Sodium-Glucose Co-Transporter 2 |
| TREG | Regulatory T-cell |
| GDPR | General Data Protection Regulation |
| HIPAA | Health Insurance Portability and Accountability Act |
References
- World Health Organization. Global Report on Diabetes; World Health Organization: Geneva, Switzerland, 2016; ISBN 9789241565257. [Google Scholar]
- Kavakiotis, I.; Tsave, O.; Salifoglou, A.; Maglaveras, N.; Vlahavas, I.; Chouvarda, I. Machine Learning and Data Mining Methods in Diabetes Research. Comput. Struct. Biotechnol. J. 2017, 15, 104–116. [Google Scholar] [CrossRef] [PubMed]
- Aldaghi, T.; Muzik, J. Multicriteria Decision-Making in Diabetes Management and Decision Support: Systematic Review. JMIR Med. Inform. 2024, 12, e47701. [Google Scholar] [CrossRef]
- Chiang, Y.; Tsay, P.; Chen, C.; Hsu, C.; Yu, H.; Chang, C.; Lo, F.; Moons, P. A Delphi Study on the Healthcare Needs of Patients with Type 1 Diabetes during the Transition from Adolescence to Adulthood: Consensus among Patients, Primary Caregivers, and Healthcare Providers. Int. J. Environ. Res. Public Health 2021, 18, 7149. [Google Scholar] [CrossRef]
- Goyal, S.; Nunn, C.A.; Rotondi, M.; Couperthwaite, A.B.; Reiser, S.; Simone, A.; Katzman, D.K.; Cafazzo, J.A.; Palmert, M.R. A Mobile App for the Self-Management of Type 1 Diabetes Among Adolescents: A Randomized Controlled Trial. JMIR mHealth uHealth 2017, 5, e82. [Google Scholar] [CrossRef] [PubMed]
- Petersmann, A.; Nauck, M.; Müller-Wieland, D.; Kerner, W.; Müller, U.; Landgraf, R.; Freckmann, G.; Heinemann, L. Definition, Classification and Diagnosis of Diabetes Mellitus. Exp. Clin. Endocrinol. Diabetes 2018, 126, 406–410. [Google Scholar] [CrossRef]
- Urbano, F.; Farella, I.; Brunetti, G.; Faienza, M.F. Pediatric Type 1 Diabetes: Mechanisms and Impact of Technologies on Comorbidities and Life Expectancy. Int. J. Mol. Sci. 2023, 24, 11980. [Google Scholar] [CrossRef]
- Krzewska, A.; Ben-Skowronek, I. Effect of Associated Autoimmune Diseases on Type 1 Diabetes Mellitus Incidence and Metabolic Control in Children and Adolescents. Biomed. Res. Int. 2016, 2016, 6219730. [Google Scholar] [CrossRef]
- García-Chapa, E.G.; Leal-Ugarte, E.; Peralta-Leal, V.; Durán-González, J.; Meza-Espinoza, J.P. Genetic Epidemiology of Type 2 Diabetes in Mexican Mestizos. Biomed. Res. Int. 2017, 2017, 3937893. [Google Scholar] [CrossRef]
- International Diabetes Federation. IDF Diabetes Atlas, 10th ed; International Diabetes Federation: Brussels, Belgium, 2021. [Google Scholar]
- Atkinson, M.A.; Eisenbarth, G.S.; Michels, A.W. Type 1 Diabetes. Lancet 2014, 383, 69–82. [Google Scholar] [CrossRef]
- Weisman, A.; Bai, J.-W.; Cardinez, M.; Kramer, C.K.; Perkins, B.A. Effect of Artificial Pancreas Systems on Glycaemic Control in Patients with Type 1 Diabetes: A Systematic Review and Meta-Analysis of Outpatient Randomised Controlled Trials. Lancet Diabetes Endocrinol. 2017, 5, 501–512. [Google Scholar] [CrossRef]
- Pescovitz, M.D.; Greenbaum, C.J.; Bundy, B.; Becker, D.J.; Gitelman, S.E.; Goland, R.; Gottlieb, P.A.; Marks, J.B.; Moran, A.; Raskin, P.; et al. B-Lymphocyte Depletion with Rituximab and β-Cell Function: Two-Year Results. Diabetes Care 2014, 37, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Sui, T.; Song, Y.; Liu, Z.; Chen, M.; Deng, J.; Xu, Y.; Lai, L.; Li, Z. CRISPR-Induced Exon Skipping Is Dependent on Premature Termination Codon Mutations. Genome Biol. 2018, 19, 2–6. [Google Scholar] [CrossRef]
- Herkert, D.; Vijayakumar, P.; Luo, J.; Schwartz, J.I.; Rabin, T.L.; DeFilippo, E.; Lipska, K.J. Cost-Related Insulin Underuse Among Patients with Diabetes. JAMA Intern. Med. 2019, 179, 112–114. [Google Scholar] [CrossRef] [PubMed]
- Herold, K.C.; Gitelman, S.E.; Ehlers, M.R.; Gottlieb, P.A.; Greenbaum, C.J.; Hagopian, W.; Boyle, K.D.; Keyes-Elstein, L.; Aggarwal, S.; Phippard, D.; et al. Teplizumab (Anti-CD3 MAb) Treatment Preserves C-Peptide Responses in Patients with New-Onset Type 1 Diabetes in a Randomized Controlled Trial. Diabetes 2013, 62, 3766–3774. [Google Scholar] [CrossRef]
- Huang, M.; Chen, W.; Wang, M.; Huang, Y.; Liu, H.; Ming, Y.; Chen, Y.; Tang, Z.; Jia, B. Advanced Delivery Strategies for Immunotherapy in Type I Diabetes Mellitus. BioDrugs 2023, 37, 331–352. [Google Scholar] [CrossRef]
- Allemailem, K.S.; Alsahli, M.A.; Almatroudi, A.; Alrumaihi, F.; Alkhaleefah, F.K.; Rahmani, A.H.; Khan, A.A. Current Updates of CRISPR/Cas9-mediated Genome Editing and Targeting within Tumor Cells: An Innovative Strategy of Cancer Management. Cancer Commun. 2022, 42, 1257–1287. [Google Scholar] [CrossRef]
- Gregory, G.A.; Robinson, T.I.G.; Linklater, S.E.; Wang, F.; Colagiuri, S.; de Beaufort, C.; Donaghue, K.C.; Magliano, D.J.; Maniam, J.; Orchard, T.J.; et al. Global Incidence, Prevalence, and Mortality of Type 1 Diabetes in 2021 with Projection to 2040: A Modelling Study. Lancet Diabetes Endocrinol. 2022, 10, 741–760. [Google Scholar] [CrossRef]
- Ogle, G.D.; James, S.; Dabelea, D.; Pihoker, C.; Svennson, J.; Maniam, J.; Klatman, E.L.; Patterson, C.C. Global Estimates of Incidence of Type 1 Diabetes in Children and Adolescents: Results from the International Diabetes Federation Atlas, 10th Edition. Diabetes Res. Clin. Pract. 2022, 183, 109083. [Google Scholar] [CrossRef]
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.N.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, Regional and Country-Level Diabetes Prevalence Estimates for 2021 and Projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef]
- Klaassen, R.; Bul, K.; Op den Akker, R.; Van der Burg, G.; Kato, P.; Di Bitonto, P. Design and Evaluation of a Pervasive Coaching and Gamification Platform for Young Diabetes Patients. Sensors 2018, 18, 402. [Google Scholar] [CrossRef]
- Holtz, B.; Mitchell, K.M.; Holmstrom, A.J.; Cotten, S.R.; Dunneback, J.K.; Jimenez-Vega, J.; Ellis, D.A.; Wood, M.A. An MHealth-Based Intervention for Adolescents with Type 1 Diabetes and Their Parents: Pilot Feasibility and Efficacy Single-Arm Study. JMIR mHealth uHealth 2021, 9, e23916. [Google Scholar] [CrossRef] [PubMed]
- Bitar, H.; Alfahid, A.; Alrige, M.; Abogazah, W.; Alsanbi, N. Ana Alsukary: An Android Mobile Application to Support Diabetic Children and Parents in Saudi Arabia. Rev. Română Informatică Autom. 2022, 32, 73–86. [Google Scholar] [CrossRef]
- Bashir, M.; Ahluwalia, H.; Sayeed, S.I.; Kapoor, R. A Comparative Study of Anxiety Levels and Its Relation with Heart Rate Variability (HRV) Indices in Adolescents with Type 1 Diabetes Mellitus. Medeni. Med. J. 2018, 33, 22–27. [Google Scholar] [CrossRef]
- Ashraff, S.; Siddiqui, M.A.; Carline, T.E. The Psychosocial Impact of Diabetes in Adolescents: A Review. Oman Med. J. 2013, 28, 159–162. [Google Scholar] [CrossRef]
- Christie, D.; Thompson, R.; Sawtell, M.; Allen, E.; Cairns, J.; Smith, F.; Jamieson, E.; Hargreaves, K.; Ingold, A.; Brooks, L.; et al. Structured, Intensive Education Maximising Engagement, Motivation and Long-Term Change for Children and Young People with Diabetes: A Cluster Randomised Controlled Trial with Integral Process and Economic Evaluation—The CASCADE Study. Health Technol. Assess. 2014, 18, 1–202. [Google Scholar] [CrossRef]
- Datye, K.; Bonnet, K.; Schlundt, D.; Jaser, S. Experiences of Adolescents and Emerging Adults Living with Type 1 Diabetes. Diabetes Educ. 2019, 45, 194–202. [Google Scholar] [CrossRef]
- Anghel, L.; Boev, M.; Stanescu, C.; Caramfil, S.M.; Luca, L.; Musat, C.L.; Ciubara, A. Depression in the Diabetic Patient. BRAIN Broad Res. Artif. Intell. Neurosci. 2023, 14, 658–672. [Google Scholar] [CrossRef]
- Cengiz, E.; Danne, T.; Ahmad, T.; Ayyavoo, A.; Beran, D.; Ehtisham, S.; Fairchild, J.; Jarosz-Chobot, P.; Ng, S.M.; Paterson, M.; et al. ISPAD: Clinical Practice Consensus Guidelines 2022. Insulin Treatment in Children and Adolescents with Diabetes. Pediatr. Diabetes 2022, 23, 1277–1296. [Google Scholar] [CrossRef]
- Adolfsson, P.; Taplin, C.E.; Zaharieva, D.P.; Pemberton, J.; Davis, E.A.; Riddell, M.C.; McGavock, J.; Moser, O.; Szadkowska, A.; Lopez, P.; et al. ISPAD Clinical Practice Consensus Guidelines 2022: Exercise in Children and Adolescents with Diabetes. Pediatr. Diabetes 2022, 23, 1341–1372. [Google Scholar] [CrossRef]
- Passanisi, S.; Salzano, G.; Basile, P.; Bombaci, B.; Caime, F.; Rulli, I.; Valenzise, M.; Gitto, E.; Lombardo, F. Prevalence and Clinical Features of Severe Diabetic Ketoacidosis Treated in Pediatric Intensive Care Unit: A 5-Year Monocentric Experience. Ital. J. Pediatr. 2023, 49, 58. [Google Scholar] [CrossRef]
- Passanisi, S.; Galletta, F.; Bombaci, B.; Cherubini, V.; Tiberi, V.; Minuto, N.; Bassi, M.; Iafusco, D.; Piscopo, A.; Mozzillo, E.; et al. Device-Related Skin Reactions Increase Emotional Burden in Youths with Type 1 Diabetes and Their Parents. J. Diabetes Sci. Technol. 2024, 18, 1293–1299. [Google Scholar] [CrossRef]
- Ledwoń, E.; Zemła-Szten, P.; von dem Berge, T.; Nalewajko, K.; Passanisi, S.; Piona, C.; dos Santos, T.; Svensson, J.; Korsgaard Berg, A.; Chobot, A. Skin Reactions in Children with Type 1 Diabetes Associated with the Use of New Diabetes Technologies—An Observational Study from a Regional Polish Pediatric Diabetes Center. Children 2024, 11, 740. [Google Scholar] [CrossRef]
- Gregory, J.W.; Cameron, F.J.; Joshi, K.; Eiswirth, M.; Garrett, C.; Garvey, K.; Agarwal, S.; Codner, E. ISPAD Clinical Practice Consensus Guidelines 2022: Diabetes in Adolescence. Pediatr. Diabetes 2022, 23, 857–871. [Google Scholar] [CrossRef]
- Gomes, M.B.; Calliari, L.E.; Conte, D.; Correa, C.L.; Drummond, K.R.G.; Mallmann, F.; Pinheiro, A.A.; Muniz, L.H.; Leal, F.S.L.; Morales, P.H.; et al. Diabetes-Related Chronic Complications in Brazilian Adolescents with Type 1 Diabetes. A Multicenter Cross-Sectional Study. Diabetes Res. Clin. Pract. 2021, 177, 108895. [Google Scholar] [CrossRef]
- Mayya, V.; Kandala, R.N.V.P.S.; Gurupur, V.; King, C.; Vu, G.T.; Wan, T.T.H. Need for an Artificial Intelligence-Based Diabetes Care Management System in India and the United States. Health Serv. Res. Manag. Epidemiol. 2024, 11, 23333928241275292. [Google Scholar] [CrossRef]
- Anandhakrishnan, A.; Hussain, S. Automating Insulin Delivery through Pump and Continuous Glucose Monitoring Connectivity: Maximizing Opportunities to Improve Outcomes. Diabetes Obes. Metab. 2024, 26, 27–46. [Google Scholar] [CrossRef]
- Mackenzie, S.C.; Sainsbury, C.A.R.; Wake, D.J. Diabetes and Artificial Intelligence beyond the Closed Loop: A Review of the Landscape, Promise and Challenges. Diabetologia 2024, 67, 223–235. [Google Scholar] [CrossRef]
- de Bock, M.; Codner, E.; Craig, M.E.; Huynh, T.; Maahs, D.M.; Mahmud, F.H.; Marcovecchio, L.; DiMeglio, L.A. ISPAD: Clinical Practice Consensus Guidelines 2022: Glycemic Targets and Glucose Monitoring for Children, Adolescents, and Young People with Diabetes. Pediatr. Diabetes 2022, 23, 1270–1276. [Google Scholar] [CrossRef]
- Sundberg, F.; DeBeaufort, C.; Krogvold, L.; Patton, S.; Piloya, T.; Smart, C.; Van Name, M.; Weissberg-Benchell, J.; Silva, J.; DiMeglio, L.A. ISPAD Clinical Practice Consensus Guidelines 2022: Managing Diabetes in Preschoolers. Pediatr. Diabetes 2022, 23, 1496–1511. [Google Scholar] [CrossRef]
- Schoelwer, M.J.; DeBoer, M.D.; Breton, M.D. Use of Diabetes Technology in Children. Diabetologia 2024, 67, 2075–2084. [Google Scholar] [CrossRef]
- Cardona-Hernandez, R.; Schwandt, A.; Alkandari, H.; Bratke, H.; Chobot, A.; Coles, N.; Corathers, S.; Goksen, D.; Goss, P.; Imane, Z.; et al. Glycemic Outcome Associated with Insulin Pump and Glucose Sensor Use in Children and Adolescents with Type 1 Diabetes. Data From the International Pediatric Registry SWEET. Diabetes Care 2021, 44, 1176–1184. [Google Scholar] [CrossRef] [PubMed]
- Johnson, S.R.; Holmes-Walker, D.J.; Chee, M.; Earnest, A.; Jones, T.W. Universal Subsidized Continuous Glucose Monitoring Funding for Young People with Type 1 Diabetes: Uptake and Outcomes Over 2 Years, a Population-Based Study. Diabetes Care 2022, 45, 391–397. [Google Scholar] [CrossRef]
- Prahalad, P.; Hardison, H.; Odugbesan, O.; Lyons, S.; Alwazeer, M.; Neyman, A.; Miyazaki, B.; Cossen, K.; Hsieh, S.; Eng, D.; et al. Benchmarking Diabetes Technology Use Among 21 U.S. Pediatric Diabetes Centers. Clin. Diabetes 2024, 42, 27–33. [Google Scholar] [CrossRef]
- Elian, V.; Popovici, V.; Ozon, E.A.; Musuc, A.M.; Fița, A.C.; Rusu, E.; Radulian, G.; Lupuliasa, D. Current Technologies for Managing Type 1 Diabetes Mellitus and Their Impact on Quality of Life—A Narrative Review. Life 2023, 13, 1663. [Google Scholar] [CrossRef]
- Franceschi, R.; Micheli, F.; Mozzillo, E.; Cauvin, V.; Liguori, A.; Soffiati, M.; Giani, E. Intermittently Scanned and Continuous Glucose Monitor Systems: A Systematic Review on Psychological Outcomes in Pediatric Patients. Front. Pediatr. 2021, 9, 660173. [Google Scholar] [CrossRef]
- Visser, M.M.; Charleer, S.; Fieuws, S.; De Block, C.; Hilbrands, R.; Van Huffel, L.; Maes, T.; Vanhaverbeke, G.; Dirinck, E.; Myngheer, N.; et al. Comparing Real-Time and Intermittently Scanned Continuous Glucose Monitoring in Adults with Type 1 Diabetes (ALERTT1): A 6-Month, Prospective, Multicentre, Randomised Controlled Trial. Lancet 2021, 397, 2275–2283. [Google Scholar] [CrossRef]
- Cappon, G.; Acciaroli, G.; Vettoretti, M.; Facchinetti, A.; Sparacino, G. Wearable Continuous Glucose Monitoring Sensors: A Revolution in Diabetes Treatment. Electronics 2017, 6, 65. [Google Scholar] [CrossRef]
- Zafar, H.; Channa, A.; Jeoti, V.; Stojanović, G.M. Comprehensive Review on Wearable Sweat-Glucose Sensors for Continuous Glucose Monitoring. Sensors 2022, 22, 638. [Google Scholar] [CrossRef]
- Nagy, G.; Szekely, T.E.; Somogyi, A.; Herold, M.; Herold, Z. New Therapeutic Approaches for Type 1 Diabetes: Disease-Modifying Therapies. World J. Diabetes 2022, 13, 835–850. [Google Scholar] [CrossRef]
- Sperling, M.A.; Laffel, L.M. Current Management of Glycemia in Children with Type 1 Diabetes Mellitus. N. Engl. J. Med. 2022, 386, 1155–1164. [Google Scholar] [CrossRef]
- Bailey, T.S.; Alva, S. Landscape of Continuous Glucose Monitoring (CGM) and Integrated CGM: Accuracy Considerations. Diabetes Technol. Ther. 2021, 23, S5–S11. [Google Scholar] [CrossRef]
- Mansour, M.; Saeed Darweesh, M.; Soltan, A. Wearable Devices for Glucose Monitoring: A Review of State-of-the-Art Technologies and Emerging Trends. Alex. Eng. J. 2024, 89, 224–243. [Google Scholar] [CrossRef]
- Wang, J.; Wang, Z.; Yu, J.; Kahkoska, A.R.; Buse, J.B.; Gu, Z. Glucose-Responsive Insulin and Delivery Systems: Innovation and Translation. Adv. Mater. 2020, 32, e1902004. [Google Scholar] [CrossRef]
- Moroșan, E.; Popovici, V.; Elian, V.; Dărăban, A.M.; Rusu, A.I.; Licu, M.; Mititelu, M.; Karampelas, O. The Impact of Medical Nutrition Intervention on the Management of Hyperphosphatemia in Hemodialysis Patients with Stage 5 Chronic Kidney Disease: A Case Series. Int. J. Environ. Res. Public Health 2023, 20, 5049. [Google Scholar] [CrossRef]
- Stankute, I.; Radzeviciene, L.; Monstaviciene, A.; Dobrovolskiene, R.; Danyte, E.; Verkauskiene, R. Serum Cystatin C as a Biomarker for Early Diabetic Kidney Disease and Dyslipidemia in Young Type 1 Diabetes Patients. Medicina 2022, 58, 218. [Google Scholar] [CrossRef]
- Eliasson, B.; Lyngfelt, L.; Strömblad, S.-O.; Franzén, S.; Eeg-Olofsson, K. The Significance of Chronic Kidney Disease, Heart Failure and Cardiovascular Disease for Mortality in Type 1 Diabetes: Nationwide Observational Study. Sci. Rep. 2022, 12, 17950. [Google Scholar] [CrossRef]
- Da Silva de Sousa, G.G.; Yamamura, M.; Moura de Araújo, M.F.; Vieira Ramos, A.C.; Arcêncio, R.A.; Pereira de Jesus Costa, A.C.; Maia Pascoal, L.; Stabnow Santos, F.; Alves de Oliveira Serra, M.A.; Graepp Fontoura, I.; et al. Vulnerable Territories to Tuberculosis-Diabetes Mellitus Comorbidity in a Northeastern Brazilian Scenario. J. Infect. Dev. Ctries. 2022, 16, 813–820. [Google Scholar] [CrossRef]
- Ingley, M.; Quebedeaux, P.; Schmidbauer, K.; Amghaiab, I.A.; Chan, J. PMON315 Hyperglycemia Dilemma: Concomitant Type 1 Diabetes Mellitus and Cushing’s Disease. J. Endocr. Soc. 2022, 6, A624–A625. [Google Scholar] [CrossRef]
- Ilie, I. The Multifarious Cushing’s—Lessons from a Case Series. Acta Endocrinol. 2019, 15, 261–269. [Google Scholar] [CrossRef]
- Kaur, N.; Bhadada, S.K.; Minz, R.W.; Dayal, D.; Kochhar, R. Interplay between Type 1 Diabetes Mellitus and Celiac Disease: Implications in Treatment. Dig. Dis. 2018, 36, 399–408. [Google Scholar] [CrossRef]
- O’Donnell, H.K.; Vigers, T.; Johnson, S.B.; Pyle, L.; Wright, N.; Deeb, L.C.; Driscoll, K.A. Pump It Up! A Randomized Clinical Trial to Optimize Insulin Pump Self-Management Behaviors in Adolescents with Type 1 Diabetes. Contemp. Clin. Trials 2021, 102, 106279. [Google Scholar] [CrossRef]
- Ersig, A.L.; Tsalikian, E.; Coffey, J.; Williams, J.K. Stressors in Teens with Type 1 Diabetes and Their Parents: Immediate and Long-Term Implications for Transition to Self-Management. J. Pediatr. Nurs. 2016, 31, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Downing, J.; Gleeson, H.K.; Clayton, P.E.; Davis, J.R.E.; Wales, J.K.; Callery, P. Transition in Endocrinology: The Challenge of Maintaining Continuity. Clin. Endocrinol. 2013, 78, 29–35. [Google Scholar] [CrossRef]
- Herbert, L.; Owen, V.; Pascarella, L.; Streisand, R. Text Message Interventions for Children and Adolescents with Type 1 Diabetes: A Systematic Review. Diabetes Technol. Ther. 2013, 15, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Monaghan, M.; Hilliard, M.; Sweenie, R.; Riekert, K. Transition Readiness in Adolescents and Emerging Adults with Diabetes: The Role of Patient-Provider Communication. Curr. Diab. Rep. 2013, 13, 900–908. [Google Scholar] [CrossRef]
- Glycemic Targets: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44, S73–S84. [CrossRef]
- Chen, L.; Chuang, L.-M.; Chang, C.-H.; Wang, C.-S.; Wang, I.-C.; Chung, Y.; Peng, H.-Y.; Chen, H.-C.; Hsu, Y.-L.; Lin, Y.-S.; et al. Evaluating Self-Management Behaviors of Diabetic Patients in a Telehealthcare Program: Longitudinal Study Over 18 Months. J. Med. Internet Res. 2013, 15, e266. [Google Scholar] [CrossRef]
- Jackson, C.C.; Albanese-O’Neill, A. Supporting the Student’s Graduated Independence in Diabetes Care. NASN Sch. Nurse 2016, 31, 202–204. [Google Scholar] [CrossRef]
- Zarifsaniey, N.; Shirazi, M.O.; Mehrabi, M.; Bagheri, Z. Promoting Self-Management Behaviors in Adolescents with Type 1 Diabetes, Using Digital Storytelling: A Pilot Randomized Controlled Trial. BMC Endocr. Disord. 2022, 22, 74. [Google Scholar] [CrossRef]
- Abrar, E.A.; Yusuf, S.; Sjattar, E.L.; Rachmawaty, R. Development and Evaluation Educational Videos of Diabetic Foot Care in Traditional Languages to Enhance Knowledge of Patients Diagnosed with Diabetes and Risk for Diabetic Foot Ulcers. Prim. Care Diabetes 2020, 14, 104–110. [Google Scholar] [CrossRef]
- Jahanbakhsh, M.; Ehteshami, A.; Afkhami, S. Developing “Aryan”: Diabetes Self-Care Mobile Application. Int. J. Prev. Med. 2019, 10, 59. [Google Scholar] [CrossRef] [PubMed]
- Samimi, Z.; Talakoub, S.; Ghazavi, Z. Effect of Telephone Follow-up by Nurses on Self-Care in Children with Diabetes. Iran. J. Nurs. Midwifery Res. 2018, 23, 26. [Google Scholar] [CrossRef] [PubMed]
- Swift, A.; Etherton, J.; Twycross, A. Keeping the Patient Front and Central: The Role of Storytelling. Evid. Based Nurs. 2019, 22, 31–32. [Google Scholar] [CrossRef]
- Moghimian, M.; Akbari, M.; Moghaddasi, J.; Niknajad, R. Effect of Digital Storytelling on Anxiety in Patients Who Are Candidates for Open-Heart Surgery. J. Cardiovasc. Nurs. 2019, 34, 231–235. [Google Scholar] [CrossRef] [PubMed]
- Lisenbee, P.S.; Ford, C.M. Engaging Students in Traditional and Digital Storytelling to Make Connections Between Pedagogy and Children’s Experiences. Early Child. Educ. J. 2018, 46, 129–139. [Google Scholar] [CrossRef]
- Kory-Westlund, J.M.; Jeong, S.; Park, H.W.; Ronfard, S.; Adhikari, A.; Harris, P.L.; DeSteno, D.; Breazeal, C.L. Flat vs. Expressive Storytelling: Young Children’s Learning and Retention of a Social Robot’s Narrative. Front. Hum. Neurosci. 2017, 11, 295. [Google Scholar] [CrossRef]
- Wilson, D.K.; Hutson, S.P.; Wyatt, T.H. Exploring the Role of Digital Storytelling in Pediatric Oncology Patients’ Perspectives Regarding Diagnosis. Sage Open 2015, 5, 2158244015572099. [Google Scholar] [CrossRef]
- Papacharissi, Z. Affective Publics and Structures of Storytelling: Sentiment, Events and Mediality. Inf. Commun. Soc. 2016, 19, 307–324. [Google Scholar] [CrossRef]
- Järvelä-Reijonen, E.; Karhunen, L.; Sairanen, E.; Muotka, J.; Lindroos, S.; Laitinen, J.; Puttonen, S.; Peuhkuri, K.; Hallikainen, M.; Pihlajamäki, J.; et al. The Effects of Acceptance and Commitment Therapy on Eating Behavior and Diet Delivered through Face-to-Face Contact and a Mobile App: A Randomized Controlled Trial. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 22. [Google Scholar] [CrossRef]
- Morawski, K.; Ghazinouri, R.; Krumme, A.; Lauffenburger, J.C.; Lu, Z.; Durfee, E.; Oley, L.; Lee, J.; Mohta, N.; Haff, N.; et al. Association of a Smartphone Application with Medication Adherence and Blood Pressure Control. JAMA Intern. Med. 2018, 178, 802. [Google Scholar] [CrossRef]
- Patel, M.L.; Hopkins, C.M.; Brooks, T.L.; Bennett, G.G. Comparing Self-Monitoring Strategies for Weight Loss in a Smartphone App: Randomized Controlled Trial. JMIR mHealth uHealth 2019, 7, e12209. [Google Scholar] [CrossRef]
- Greer, J.A.; Jacobs, J.M.; Pensak, N.; Nisotel, L.E.; Fishbein, J.N.; MacDonald, J.J.; Ream, M.E.; Walsh, E.A.; Buzaglo, J.; Muzikansky, A.; et al. Randomized Trial of a Smartphone Mobile App to Improve Symptoms and Adherence to Oral Therapy for Cancer. J. Natl. Compr. Canc. Netw. 2020, 18, 133–141. [Google Scholar] [PubMed]
- Mascarenhas, M.N.; Chan, J.M.; Vittinghoff, E.; Van Blarigan, E.L.; Hecht, F. Increasing Physical Activity in Mothers Using Video Exercise Groups and Exercise Mobile Apps: Randomized Controlled Trial. J. Med. Internet Res. 2018, 20, e179. [Google Scholar] [CrossRef] [PubMed]
- Berndt, R.-D.; Takenga, C.; Preik, P.; Kuehn, S.; Berndt, L.; Mayer, H.; Kaps, A.; Schiel, R. Impact of Information Technology on the Therapy of Type-1 Diabetes: A Case Study of Children and Adolescents in Germany. J. Pers. Med. 2014, 4, 200–217. [Google Scholar] [CrossRef]
- Klee, P.; Bussien, C.; Castellsague, M.; Combescure, C.; Dirlewanger, M.; Girardin, C.; Mando, J.-L.; Perrenoud, L.; Salomon, C.; Schneider, F.; et al. An Intervention by a Patient-Designed Do-It-Yourself Mobile Device App Reduces HbA1c in Children and Adolescents with Type 1 Diabetes: A Randomized Double-Crossover Study. Diabetes Technol. Ther. 2018, 20, 797–805. [Google Scholar] [CrossRef]
- Castensøe-Seidenfaden, P.; Reventlov Husted, G.; Teilmann, G.; Hommel, E.; Olsen, B.S.; Kensing, F. Designing a Self-Management App for Young People with Type 1 Diabetes: Methodological Challenges, Experiences, and Recommendations. JMIR mHealth uHealth 2017, 5, e124. [Google Scholar] [CrossRef] [PubMed]
- Albanese-O’Neill, A.; Schatz, D.A.; Thomas, N.; Bernhardt, J.M.; Cook, C.L.; Haller, M.J.; Bernier, A.V.; Silverstein, J.H.; Westen, S.C.; Elder, J.H. Designing Online and Mobile Diabetes Education for Fathers of Children with Type 1 Diabetes: Mixed Methods Study. JMIR Diabetes 2019, 4, e13724. [Google Scholar] [CrossRef]
- Andersen, N.S.; Haugaard, L.H.; Pedersen, S.B.; Pedersen, M.S.; Bygholm, A. Digital Support for Self-Management in Children with Diabetes: Understanding Their Needs and Developing a Design Concept. In Digital Personalized Health and Medicine; IOS Press: Amsterdam, The Netherlands, 2020. [Google Scholar]
- McCulloch, V.; Hope, S.; Loranger, B.; Rea, P. How to Effectively Design and Create a Concept Mobile Application to Aid in the Management of Type 1 Diabetes in Adolescents. J. Vis. Commun. Med. 2017, 40, 101–108. [Google Scholar] [CrossRef]
- Castensøe-Seidenfaden, P.; Husted, G.R.; Jensen, A.K.; Hommel, E.; Olsen, B.; Pedersen-Bjergaard, U.; Kensing, F.; Teilmann, G. Testing a Smartphone App (Young with Diabetes) to Improve Self-Management of Diabetes Over 12 Months: Randomized Controlled Trial. JMIR mHealth uHealth 2018, 6, e141. [Google Scholar] [CrossRef]
- Schmidt, M.; Lu, J.; Luo, W.; Cheng, L.; Lee, M.; Huang, R.; Weng, Y.; Kichler, J.C.; Corathers, S.D.; Jacobsen, L.M.; et al. Learning Experience Design of an MHealth Self-Management Intervention for Adolescents with Type 1 Diabetes. Educ. Technol. Res. Dev. 2022, 70, 2171–2209. [Google Scholar] [CrossRef]
- Alsalman, D.M.; Ali, Z.B.; Alnosaier, Z.; Alotaibi, N.; Alanzi, T.M. Caregiver’s Opinions on the Design of the Screens of a Future Gamified Mobile Application for Self-Management of Type 1 Diabetes in Children in Saudi Arabia. Int. J. Telemed. Appl. 2021, 2021, 8822676. [Google Scholar] [CrossRef] [PubMed]
- Kitsiou, S.; Paré, G.; Jaana, M.; Gerber, B. Effectiveness of MHealth Interventions for Patients with Diabetes: An Overview of Systematic Reviews. PLoS ONE 2017, 12, e0173160. [Google Scholar] [CrossRef]
- Markowitz, J.T.; Cousineau, T.; Franko, D.L.; Schultz, A.T.; Trant, M.; Rodgers, R.; Laffel, L.M.B. Text Messaging Intervention for Teens and Young Adults with Diabetes. J. Diabetes Sci. Technol. 2014, 8, 1029–1034. [Google Scholar] [CrossRef] [PubMed]
- Cafazzo, J.A.; Casselman, M.; Hamming, N.; Katzman, D.K.; Palmert, M.R. Design of an MHealth App for the Self-Management of Adolescent Type 1 Diabetes: A Pilot Study. J. Med. Internet Res. 2012, 14, e70. [Google Scholar] [CrossRef]
- Holtz, B.E.; Murray, K.M.; Hershey, D.D.; Dunneback, J.K.; Cotten, S.R.; Holmstrom, A.J.; Vyas, A.; Kaiser, M.K.; Wood, M.A. Developing a Patient-Centered MHealth App: A Tool for Adolescents with Type 1 Diabetes and Their Parents. JMIR mHealth uHealth 2017, 5, e53. [Google Scholar] [CrossRef]
- Husted, G.R.; Weis, J.; Teilmann, G.; Castensøe-Seidenfaden, P. Exploring the Influence of a Smartphone App (Young with Diabetes) on Young People’s Self-Management: Qualitative Study. JMIR mHealth uHealth 2018, 6, e43. [Google Scholar] [CrossRef]
- Ledderer, L.; Møller, A.; Fage-Butler, A. Adolescents’ Participation in Their Healthcare: A Sociomaterial Investigation of a Diabetes App. Digit. Health 2019, 5, 2055207619845448. [Google Scholar] [CrossRef]
- Stanger, C.; Kowatsch, T.; Xie, H.; Nahum-Shani, I.; Lim-Liberty, F.; Anderson, M.; Santhanam, P.; Kaden, S.; Rosenberg, B. A Digital Health Intervention (SweetGoals) for Young Adults with Type 1 Diabetes: Protocol for a Factorial Randomized Trial. JMIR Res. Protoc. 2021, 10, e27109. [Google Scholar] [CrossRef]
- Frøisland, D.H.; Årsand, E. Integrating Visual Dietary Documentation in Mobile-Phone-Based Self-Management Application for Adolescents with Type 1 Diabetes. J. Diabetes Sci. Technol. 2015, 9, 541–548. [Google Scholar] [CrossRef]
- Krmpotic, K.; Gallant, J.R.; Zufelt, K.; Zuijdwijk, C. User-Centred Development of an MHealth App for Youth with Type 1 Diabetes: The Challenge of Operationalizing Desired Features and Feasibility of Offering Financial Incentives. Health Technol. 2022, 12, 499–513. [Google Scholar] [CrossRef]
- Alfonsi, J.E.; Choi, E.E.Y.; Arshad, T.; Sammott, S.-A.S.; Pais, V.; Nguyen, C.; Maguire, B.R.; Stinson, J.N.; Palmert, M.R. Carbohydrate Counting App Using Image Recognition for Youth with Type 1 Diabetes: Pilot Randomized Control Trial. JMIR mHealth uHealth 2020, 8, e22074. [Google Scholar] [CrossRef] [PubMed]
- Chatzakis, C.; Floros, D.; Papagianni, M.; Tsiroukidou, K.; Kosta, K.; Vamvakis, A.; Koletsos, N.; Hatziagorou, E.; Tsanakas, I.; Mastorakos, G. The Beneficial Effect of the Mobile Application Euglyca in Children and Adolescents with Type 1 Diabetes Mellitus: A Randomized Controlled Trial. Diabetes Technol. Ther. 2019, 21, 627–634. [Google Scholar] [CrossRef] [PubMed]
- den Akker, R.O.; Klaassen, R.; Bul, K.; Kato, P.M.; van der Burg, G.-J.; di Bitonto, P. Let Them Play. In Proceedings of the 11th EAI International Conference on Pervasive Computing Technologies for Healthcare, New York, NY, USA, 23 May 2017; pp. 409–418. [Google Scholar]
- Neinstein, A.; Wong, J.; Look, H.; Arbiter, B.; Quirk, K.; McCanne, S.; Sun, Y.; Blum, M.; Adi, S. A Case Study in Open Source Innovation: Developing the Tidepool Platform for Interoperability in Type 1 Diabetes Management. J. Am. Med. Inform. Assoc. 2016, 23, 324–332. [Google Scholar] [CrossRef]
- Bin-Abbas, B.; Jabbari, M.; Al-Fares, A.; El-Dali, A.; Al-Orifi, F. Effect of Mobile Phone Short Text Messages on Glycaemic Control in Children with Type 1 Diabetes. J. Telemed. Telecare 2014, 20, 153–156. [Google Scholar] [CrossRef] [PubMed]
- Trnka, P.; Aldaghi, T.; Muzik, J. Categorization of MHealth Coaching Technologies for Children or Adolescents with Type 1 Diabetes: Systematic Review. JMIR Pediatr. Parent. 2024, 7, e50370. [Google Scholar] [CrossRef]
- Nkhoma, D.E.; Soko, C.J.; Bowrin, P.; Manga, Y.B.; Greenfield, D.; Househ, M.; Li, Y.-C.; Iqbal, U. Digital Interventions Self-Management Education for Type 1 and 2 Diabetes: A Systematic Review and Meta-Analysis. Comput. Methods Programs Biomed. 2021, 210, 106370. [Google Scholar] [CrossRef]
- Garner, K.; Boggiss, A.; Jefferies, C.; Serlachius, A. Digital Health Interventions for Improving Mental Health Outcomes and Wellbeing for Youth with Type 1 Diabetes: A Systematic Review. Pediatr. Diabetes 2022, 23, 258–269. [Google Scholar] [CrossRef]
- Stevens, S.; Gallagher, S.; Andrews, T.; Ashall-Payne, L.; Humphreys, L.; Leigh, S. The Effectiveness of Digital Health Technologies for Patients with Diabetes Mellitus: A Systematic Review. Front. Clin. Diabetes Healthc. 2022, 3, 936752. [Google Scholar] [CrossRef]
- Giani, E.; Dovc, K.; Dos Santos, T.J.; Chobot, A.; Braune, K.; Cardona-Hernandez, R.; De Beaufort, C.; Scaramuzza, A.E. Telemedicine and COVID 19 Pandemic: The Perfect Storm to Mark a Change in Diabetes Care. Results from a World-wide Cross-sectional Web-based Survey. Pediatr. Diabetes 2021, 22, 1115–1119. [Google Scholar] [CrossRef]
- Buggs-Saxton, C. Care of Pediatric Patients with Diabetes During the Coronavirus Disease 2019 (COVID-19) Pandemic. Pediatr. Clin. N. Am. 2021, 68, 1093–1101. [Google Scholar] [CrossRef]
- Cornea, D. Local Therapy Management of Oral Pathology in Patients with Local Therapy Management of Oral Pathology in Patients with Fixed Orthodontic Appliances During the COVID-19 Pandemic. Rom. J. Oral Rehabil. 2022, 14, 200–206. [Google Scholar]
- Crossen, S.S.; Bruggeman, B.S.; Haller, M.J.; Raymond, J.K. Challenges and Opportunities in Using Telehealth for Diabetes Care. Diabetes Spectr. 2022, 35, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, D.A.; Gee, P.M.; Fatkin, K.J.; Peeples, M. A Systematic Review of Reviews Evaluating Technology-Enabled Diabetes Self-Management Education and Support. J. Diabetes Sci. Technol. 2017, 11, 1015–1027. [Google Scholar] [CrossRef] [PubMed]
- Guljas, R.; Ahmed, A.; Chang, K.; Whitlock, A. Impact of Telemedicine in Managing Type 1 Diabetes Among School-Age Children and Adolescents: An Integrative Review. J. Pediatr. Nurs. 2014, 29, 198–204. [Google Scholar] [CrossRef]
- von Sengbusch, S.; Eisemann, N.; Mueller-Godeffroy, E.; Lange, K.; Doerdelmann, J.; Erdem, A.; Menrath, I.; Bokelmann, J.; Krasmann, M.; Kaczmarczyk, P.; et al. Outcomes of Monthly Video Consultations as an Add-on to Regular Care for Children with Type 1 Diabetes: A 6-Month Quasi-Randomized Clinical Trial Followed by an Extension Phase. Pediatr. Diabetes 2020, 21, 1502–1515. [Google Scholar] [CrossRef]
- Negreiros, F.D.d.S.; Araújo, A.L.d.; Mattos, S.M.; Moreira, T.R.; Cestari, V.R.F.; da Silva, L.M.S.; Moreira, T.M.M. Digital Technologies in the Care of People with Diabetes during the COVID-19 Pandemic: A Scoping Review. Rev. Esc. Enferm. USP 2021, 55, e20210295. [Google Scholar] [CrossRef]
- d’Annunzio, G.; Maffeis, C.; Cherubini, V.; Rabbone, I.; Scaramuzza, A.; Schiaffini, R.; Minuto, N.; Piccolo, G.; Maghnie, M. Caring for Children and Adolescents with Type 1 Diabetes Mellitus: Italian Society for Pediatric Endocrinology and Diabetology (ISPED) Statements during COVID-19 Pandemia. Diabetes Res. Clin. Pract. 2020, 168, 108372. [Google Scholar] [CrossRef]
- Plachy, L.; Neuman, V.; Velichova, K.; Slavenko, M.G.; Santova, A.; Anne Amaratunga, S.; Obermannova, B.; Kolouskova, S.; Pruhova, S.; Sumnik, Z.; et al. Telemedicine Maintains Good Glucose Control in Children with Type 1 Diabetes but Is Not Time Saving for Healthcare Professionals: KITES Randomized Study. Diabetes Res. Clin. Pract. 2024, 209, 111602. [Google Scholar] [CrossRef]
- Gajarawala, S.N.; Pelkowski, J.N. Telehealth Benefits and Barriers. J. Nurse Pract. 2021, 17, 218–221. [Google Scholar] [CrossRef]
- Taras, M.A.; Tonolo, G. Psychological Aspects in the Use of Telemedicine in Diabetes Mellitus. J. Diabetes Treat. 2022, 7, 1098. [Google Scholar] [CrossRef]
- Tyler, N.S.; Jacobs, P.G. Artificial Intelligence in Decision Support Systems for Type 1 Diabetes. Sensors 2020, 20, 3214. [Google Scholar] [CrossRef]
- Tanenbaum, M.L.; Commissariat, P.V. Barriers and Facilitators to Diabetes Device Adoption for People with Type 1 Diabetes. Curr. Diab. Rep. 2022, 22, 291–299. [Google Scholar] [CrossRef]
- Addala, A.; Suttiratana, S.C.; Wong, J.J.; Lanning, M.S.; Barnard, K.D.; Weissberg-Benchell, J.; Laffel, L.M.; Hood, K.K.; Naranjo, D. Cost Considerations for Adoption of Diabetes Technology Are Pervasive: A Qualitative Study of Persons Living with Type 1 Diabetes and Their Families. Diabet. Med. 2021, 38, e14575. [Google Scholar] [CrossRef]
- Forlenza, G.P. Use of Artificial Intelligence to Improve Diabetes Outcomes in Patients Using Multiple Daily Injections Therapy. Diabetes Technol. Ther. 2019, 21, S24–S28. [Google Scholar] [CrossRef]
- Bertolazzi, A.; Marzęda-Młynarska, K.; Kięczkowska, J.; Zanier, M.L. Datafication of Care: Security and Privacy Issues with Health Technology for People with Diabetes. Societies 2024, 14, 163. [Google Scholar] [CrossRef]
- Ware, J.; Hovorka, R. Closed-Loop Insulin Delivery: Update on the State of the Field and Emerging Technologies. Expert Rev. Med. Devices 2022, 19, 859–875. [Google Scholar] [CrossRef] [PubMed]
- Abrahamson, M.J.; Barzilay, J.I.; Blonde, L.; Bloomgarden, Z.T.; Bush, M.A.; Dagogo-Jack, S.; Davidson, M.B.; Einhorn, D.; Timothy Garvey, W.; Grunberger, G.; et al. Aace Comprehensive Diabetes Management Algorithm 2013. Endocr. Pract. 2013, 19, 327–336. [Google Scholar] [CrossRef] [PubMed]
- Children and Adolescents: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44, S180–S199. [CrossRef]
- Keymeulen, B.; De Groot, K.; Jacobs-Tulleneers-Thevissen, D.; Thompson, D.M.; Bellin, M.D.; Kroon, E.J.; Daniels, M.; Wang, R.; Jaiman, M.; Kieffer, T.J.; et al. Encapsulated Stem Cell–Derived β Cells Exert Glucose Control in Patients with Type 1 Diabetes. Nat. Biotechnol. 2023, 42, 1507–1514. [Google Scholar] [CrossRef]
- Karpov, D.S.; Sosnovtseva, A.O.; Pylina, S.V.; Bastrich, A.N.; Petrova, D.A.; Kovalev, M.A.; Shuvalova, A.I.; Eremkina, A.K.; Mokrysheva, N.G. Challenges of CRISPR/Cas-Based Cell Therapy for Type 1 Diabetes: How Not to Engineer a “Trojan Horse”. Int. J. Mol. Sci. 2023, 24, 17320. [Google Scholar] [CrossRef]
- Cheng, Y.; Wang, H.; Li, M. The Promise of CRISPR/Cas9 Technology in Diabetes Mellitus Therapy: How Gene Editing Is Revolutionizing Diabetes Research and Treatment. J. Diabetes Complicat. 2023, 37, 108524. [Google Scholar] [CrossRef]
- Basile, G.; Qadir, M.M.F.; Mauvais-Jarvis, F.; Vetere, A.; Shoba, V.; Modell, A.E.; Pastori, R.L.; Russ, H.A.; Wagner, B.K.; Dominguez-Bendala, J. Emerging Diabetes Therapies: Bringing Back the β-Cells. Mol. Metab. 2022, 60, 101477. [Google Scholar] [CrossRef] [PubMed]
- Ruan, S.; Guo, X.; Ren, Y.; Cao, G.; Xing, H.; Zhang, X. Nanomedicines Based on Trace Elements for Intervention of Diabetes Mellitus. Biomed. Pharmacother. 2023, 168, 115684. [Google Scholar] [CrossRef]
- Huang, J.; Zhang, Y.; Wu, J. Review of Non-Invasive Continuous Glucose Monitoring Based on Impedance Spectroscopy. Sens. Actuators A Phys. 2020, 311, 112103. [Google Scholar] [CrossRef]
- Humulescu, I.; Flutur, M.M.; Cioancă, O.; Mircea, C.; Robu, S.; Marin-Batir, D.; Spac, A.; Corciova, A.; Hăncianu, M. Comparative Chemical and Biological Activity of Selective Herbal Extracts. Farmacia 2021, 69, 861–866. [Google Scholar] [CrossRef]
- Wang, M.; Yang, Y.; Min, J.; Song, Y.; Tu, J.; Mukasa, D.; Ye, C.; Xu, C.; Heflin, N.; McCune, J.S.; et al. A Wearable Electrochemical Biosensor for the Monitoring of Metabolites and Nutrients. Nat. Biomed. Eng. 2022, 6, 1225–1235. [Google Scholar] [CrossRef] [PubMed]
- Peng, X.; Yan, Y.-X.; Liu, H. On the Use of Fiber Lasers in Non-Invasive Blood Glucose Monitoring. Opt. Fiber Technol. 2022, 68, 102822. [Google Scholar] [CrossRef]
- Zhang, Y.; Wu, G.; Wei, H.; Guo, Z.; Yang, H.; He, Y.; Xie, S.; Liu, Y. Continuous Noninvasive Monitoring of Changes in Human Skin Optical Properties during Oral Intake of Different Sugars with Optical Coherence Tomography. Biomed. Opt. Express 2014, 5, 990. [Google Scholar] [CrossRef]
- Zhu, F.; Abbas, S.R.; Bologa, R.; Levin, N.W.; Kotanko, P. Effect of Decrease in Glucose Gradient on Change in Intraperitoneal Volume Using Segmental Bioimpedance During PET. Nephrol. Dial. Transplant. 2020, 35 (Suppl. S3), gfaa142-P1183. [Google Scholar] [CrossRef]
- Jose, P.S.H.; Rajasekaran, K.; Rajalakshmy, P.; Jebastina, B. A Non-Invasive Method for Measurement of Blood Glucose Using Bio Impedance Technique. In Proceedings of the 2019 2nd International Conference on Signal Processing and Communication (ICSPC), Coimbatore, India, 29–30 March 2019; pp. 138–142. [Google Scholar]
- Takamatsu, R.; Higuchi, K.; Muramatsu, D. Measurement Frequency Evaluation for Bioimpedance-Based Blood-Glucose Estimation. In Proceedings of the 2021 IEEE 3rd Global Conference on Life Sciences and Technologies (LifeTech), Nara, Japan, 9–11 March 2021; pp. 309–310. [Google Scholar]
- Pearson, J.A.; McKinney, E.F.; Walker, L.S.K. 100 Years Post-Insulin: Immunotherapy as the next Frontier in Type 1 Diabetes. Immunother. Adv. 2021, 1, ltab024. [Google Scholar] [CrossRef]
- Bluestone, J.A.; Buckner, J.H.; Fitch, M.; Gitelman, S.E.; Gupta, S.; Hellerstein, M.K.; Herold, K.C.; Lares, A.; Lee, M.R.; Li, K.; et al. Type 1 Diabetes Immunotherapy Using Polyclonal Regulatory T Cells. Sci. Transl. Med. 2015, 7, 315ra189. [Google Scholar] [CrossRef]
- Liu, Y.; Li, W.; Chen, Y.; Wang, X. Anti-CD3 Monoclonal Antibodies in Treatment of Type 1 Diabetes: A Systematic Review and Meta-Analysis. Endocrine 2023, 83, 322–329. [Google Scholar] [CrossRef]
- Zhang, X.; Dong, Y.; Liu, D.; Yang, L.; Xu, J.; Wang, Q. Antigen-Specific Immunotherapies in Type 1 Diabetes. J. Trace Elem. Med. Biol. 2022, 73, 127040. [Google Scholar] [CrossRef] [PubMed]
- Lungu, I.-I. Catechin-Zinc-Complex: Synthesis, Characterization and Biological Assessment. Farmacia 2023, 71, 755–763. [Google Scholar] [CrossRef]
- Zarei, M.; Sheikholeslami, M.A.; Mozaffari, M.; Mortada, Y. Innovative Immunotherapies and Emerging Treatments in Type 1 Diabetes Management. Diabetes Epidemiol. Manag. 2025, 17, 100247. [Google Scholar] [CrossRef]
- Pagliuca, F.W.; Millman, J.R.; Gürtler, M.; Segel, M.; Van Dervort, A.; Ryu, J.H.; Peterson, Q.P.; Greiner, D.; Melton, D.A. Generation of Functional Human Pancreatic β Cells in vitro. Cell 2014, 159, 428–439. [Google Scholar] [CrossRef] [PubMed]
- Diane, A.; Mu-U-Min, R.B.A.; Al-Siddiqi, H.H. Epigenetic Memory as Crucial Contributing Factor in Directing the Differentiation of Human IPSC into Pancreatic β-Cells in vitro. Cell Tissue Res. 2025, 399, 267–276. [Google Scholar] [CrossRef]
- Silva, I.B.B.; Kimura, C.H.; Colantoni, V.P.; Sogayar, M.C. Stem Cells Differentiation into Insulin-Producing Cells (IPCs): Recent Advances and Current Challenges. Stem Cell Res. Ther. 2022, 13, 309. [Google Scholar] [CrossRef]
- von Scholten, B.J.; Kreiner, F.F.; Gough, S.C.L.; von Herrath, M. Current and Future Therapies for Type 1 Diabetes. Diabetologia 2021, 64, 1037–1048. [Google Scholar] [CrossRef]
- Rezania, A.; Bruin, J.E.; Arora, P.; Rubin, A.; Batushansky, I.; Asadi, A.; O’Dwyer, S.; Quiskamp, N.; Mojibian, M.; Albrecht, T.; et al. Reversal of Diabetes with Insulin-Producing Cells Derived in vitro from Human Pluripotent Stem Cells. Nat. Biotechnol. 2014, 32, 1121–1133. [Google Scholar] [CrossRef]
- Yin, H.; Xue, W.; Chen, S.; Bogorad, R.L.; Benedetti, E.; Grompe, M.; Koteliansky, V.; Sharp, P.A.; Jacks, T.; Anderson, D.G. Genome Editing with Cas9 in Adult Mice Corrects a Disease Mutation and Phenotype. Nat. Biotechnol. 2014, 32, 551–553. [Google Scholar] [CrossRef]
- Kazanskiy, N.L.; Khonina, S.N.; Butt, M.A. Smart Contact Lenses—A Step towards Non-Invasive Continuous Eye Health Monitoring. Biosensors 2023, 13, 933. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Yang, K.; Fan, H.; Wei, M.; Xiong, Q. Targeting the Gut Microbiota and Its Metabolites for Type 2 Diabetes Mellitus. Front. Endocrinol. 2023, 14, 1114424. [Google Scholar] [CrossRef]
- Takeuchi, T.; Kubota, T.; Nakanishi, Y.; Tsugawa, H.; Suda, W.; Kwon, A.T.J.; Yazaki, J.; Ikeda, K.; Nemoto, S.; Mochizuki, Y.; et al. Gut Microbial Carbohydrate Metabolism Contributes to Insulin Resistance. Nature 2023, 621, 389–395. [Google Scholar] [CrossRef]
- Guo, Q. Bioinformatics Analysis of the Diversity of Gut Microbiota and Different Microbiota on Insulin Resistance in Diabetes Mellitus Patients. Heliyon 2023, 9, e22117. [Google Scholar] [CrossRef]
- Homayouni-Rad, A.; Soroush, A.-R.; Khalili, L.; Norouzi-Panahi, L.; Kasaie, Z.; Ejtahed, H.-S. Diabetes Management by Probiotics: Current Knowledge and Future Pespective. Int. J. Vitam. Nutr. Res. 2016, 86, 216–228. [Google Scholar] [CrossRef]
- Popoviciu, M.S.; Kaka, N.; Sethi, Y.; Patel, N.; Chopra, H.; Cavalu, S. Type 1 Diabetes Mellitus and Autoimmune Diseases: A Critical Review of the Association and the Application of Personalized Medicine. J. Pers. Med. 2023, 13, 422. [Google Scholar] [CrossRef]
- Bibbò, S.; Dore, M.P.; Pes, G.M.; Delitala, G.; Delitala, A.P. Is There a Role for Gut Microbiota in Type 1 Diabetes Pathogenesis? Ann. Med. 2017, 49, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Mokhtari, P.; Metos, J.; Anandh Babu, P.V. Impact of Type 1 Diabetes on the Composition and Functional Potential of Gut Microbiome in Children and Adolescents: Possible Mechanisms, Current Knowledge, and Challenges. Gut Microbes 2021, 13, 1–18. [Google Scholar] [CrossRef]
- Neiva, L.P.; Lopez, L.C.; Pasiani, R.O.; Serra, M.J.R.; Rullo, V.E.V. Use of Probiotics and Similar in Pediatric Patients with Type 1 Diabetes Mellitus: A Systematic Review. Rev. Paul. Pediatr. 2024, 42, e2023097. [Google Scholar] [CrossRef]
- Zikou, E.; Dovrolis, N.; Dimosthenopoulos, C.; Gazouli, M.; Makrilakis, K. The Effect of Probiotic Supplements on Metabolic Parameters of People with Type 2 Diabetes in Greece—A Randomized, Double-Blind, Placebo-Controlled Study. Nutrients 2023, 15, 4663. [Google Scholar] [CrossRef]
- Sahhaf Ebrahimi, F.; Homayouni Rad, A.; Mosen, M.; Abbasalizadeh, F.; Tabrizi, A.; Khalili, L. Effect of L. Acidophilus and B. Lactis on Blood Glucose in Women with Gestational Diabetes Mellitus: A Randomized Placebo-Controlled Trial. Diabetol. Metab. Syndr. 2019, 11, 75. [Google Scholar] [CrossRef] [PubMed]
- Groele, L.; Szajewska, H.; Szalecki, M.; Świderska, J.; Wysocka-Mincewicz, M.; Ochocińska, A.; Stelmaszczyk-Emmel, A.; Demkow, U.; Szypowska, A. Lack of Effect of Lactobacillus Rhamnosus GG and Bifidobacterium Lactis Bb12 on Beta-Cell Function in Children with Newly Diagnosed Type 1 Diabetes: A Randomised Controlled Trial. BMJ Open Diabetes Res. Care 2021, 9, e001523. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhang, Y.; Luo, L.; Le, Y.; Li, Y.; Yuan, F.; Wu, Y.; Xu, P. The Beneficial Effects of a Multispecies Probiotic Supplement on Glycaemic Control and Metabolic Profile in Adults with Type 1 Diabetes: A Randomised, Double-Blinded, Placebo-Controlled Pilot-Study. Diabetes Metab. Syndr. Obes. 2023, 16, 829–840. [Google Scholar] [CrossRef]
- Moravejolahkami, A.R.; Shakibaei, M.; Fairley, A.M.; Sharma, M. Probiotics, Prebiotics, and Synbiotics in Type 1 Diabetes Mellitus: A Systematic Review and Meta-analysis of Clinical Trials. Diabetes. Metab. Res. Rev. 2024, 40, e3655. [Google Scholar] [CrossRef]
- Li, X.; Atkinson, M.A. The Role for Gut Permeability in the Pathogenesis of Type 1 Diabetes—A Solid or Leaky Concept? Pediatr. Diabetes 2015, 16, 485–492. [Google Scholar] [CrossRef]
- Ang, Z.; Ding, J.L. GPR41 and GPR43 in Obesity and Inflammation—Protective or Causative? Front. Immunol. 2016, 7, 28. [Google Scholar] [CrossRef]
- Priyadarshini, M.; Navarro, G.; Layden, B.T. Gut Microbiota: FFAR Reaching Effects on Islets. Endocrinology 2018, 159, 2495–2505. [Google Scholar] [CrossRef]
- Psichas, A.; Sleeth, M.L.; Murphy, K.G.; Brooks, L.; Bewick, G.A.; Hanyaloglu, A.C.; Ghatei, M.A.; Bloom, S.R.; Frost, G. The Short Chain Fatty Acid Propionate Stimulates GLP-1 and PYY Secretion via Free Fatty Acid Receptor 2 in Rodents. Int. J. Obes. 2015, 39, 424–429. [Google Scholar] [CrossRef]
- Christiansen, C.B.; Gabe, M.B.N.; Svendsen, B.; Dragsted, L.O.; Rosenkilde, M.M.; Holst, J.J. The Impact of Short-Chain Fatty Acids on GLP-1 and PYY Secretion from the Isolated Perfused Rat Colon. Am. J. Physiol. Liver Physiol. 2018, 315, G53–G65. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Company Name | Country | Example of CGM Device | Functional Principle | Clinical Relevance and Mechanism |
|---|---|---|---|---|
| F. Hoffmann-La Roche | Switzerland | Accu-Chek CGM System | Utilizes a subcutaneous sensor to measure glucose in interstitial fluid, transmitting data wirelessly to a receiver or smartphone. | Provides real-time glucose tracking and alerts users to prevent hypo- or hyperglycemia. |
| A. Menarini Diagnostics | Italy | GlucoMen Day CGM | Employs a minimally invasive continuous glucose sensor that connects via Bluetooth for real-time monitoring. | Enhances glucose control by reducing the frequency of blood glucose finger sticks. |
| B. Braun Melsungen AG | Germany | Omnitest CGM | Uses an enzymatic biosensor to detect glucose levels in the interstitial fluid, providing continuous data. | Supports proactive insulin adjustments by offering trend insights. |
| Echo Therapeutics, Inc. | USA | Symphony CGM | Implements a transdermal biosensor for non-invasive glucose measurement. | Aims to eliminate discomfort associated with invasive CGM devices. |
| Johnson & Johnson | USA | Animas Vibe CGM | Integrates a real-time glucose sensor with an insulin pump for automated insulin adjustments. | Improves glycemic control through a semi-automated insulin delivery system. |
| Medtronic plc | USA | Guardian Connect CGM | Uses a thin subcutaneous sensor to provide continuous glucose readings to a linked device. | Provides predictive alerts for hypo- and hyperglycemia, improving glycemic stability. |
| GlySens Incorporated | USA | GlySens ICGM System | Features a fully implantable CGM that transmits glucose data continuously. | Reduces the need for sensor replacements, allowing long-term glucose monitoring. |
| Senseonics Holdings, Inc. | USA | Eversense Implantable CGM | Utilizes an implantable fluorescence-based glucose sensor that communicates with a wearable transmitter. | Offers extended wear time (up to 6 months) for reduced device maintenance. |
| Abbott Laboratories | USA | FreeStyle Libre | Uses a filament sensor placed under the skin that is scanned manually for glucose readings. | Eliminates routine fingerstick testing while providing retrospective glucose data. |
| LifeScan IP Holdings LLC | USA | OneTouch CGM System | Employs a subcutaneous electrochemical sensor that transmits glucose levels to a connected app. | Facilitates real-time glucose monitoring with digital tracking for better self-management. |
| Terumo Corporation | Japan | Terumo CGM | Implements an enzymatic reaction-based sensor for continuous glucose tracking. | Ensures high accuracy in glucose detection, aiding in insulin dosing decisions. |
| Application Name | Key Benefits | References |
|---|---|---|
| Bant app | Enhances blood glucose monitoring and self-management. | [5,97] |
| Webdia app | Reduces HbA1c levels in children. | [87] |
| MyT1DHero app | Improves communication between parents and adolescents; enhances adherence to self-care. | [23,98] |
| Ana Alsukary app created in Saudi Arabia | Helps children understand their diabetes and adjust their lifestyle. | [24] |
| Young with Diabetes app (YWD) | Reduces feelings of loneliness; enhances T1D knowledge and self-management skills. | [88,92,99] |
| Diapplo app | Partially meets children’s educational needs. | [100] |
| Mobile Diabetes Advice for Dads (mDAD) | Assists fathers in understanding and supporting diabetes management. | [89] |
| SweetGoals app | Supports young adults in complying with their medical regimen. | [101] |
| Mobile Diab | Aids in T1D treatment for adolescents. | [86,102,103] |
| CanDIT (Canadian Diabetes Incentives and Technology) app | Highly accepted tool for providing diabetes-related information. | [103] |
| iSpy app and glycemic control tools | Encourages glucose monitoring, assists with data collection, and supports healthy nutrition and medication dosing. | [104,105] |
| Category | Therapy | Development Stage | Key Benefits | Challenges/Risks | Reference |
|---|---|---|---|---|---|
| Emerging Therapies (In Clinical Trials, Awaiting Approval) | Beta Cell Regeneration Therapies (Stem Cell-Derived β-Cells) | Phase 1/2 clinical trials | Potential to restore natural insulin production | Risk of immune rejection, ethical concerns | [133] |
| Advanced Artificial Pancreas (Next-Gen Hybrid Closed-Loop Systems) | Late-stage development | AI-driven glucose prediction, dual hormone systems | Requires extensive validation, high costs | [125] | |
| Combination Immunotherapy Approaches | Phase 1/2 trials | Aims to protect β-cells from autoimmune destruction | Long-term effects and patient selection still uncertain | [134] | |
| Experimental Therapies (Preclinical or Early Research) | CRISPR Gene Editing for T1D Cure | Preclinical stage | Potential to correct genetic predisposition to autoimmunity | Ethical and technical challenges, long-term safety unknown | [135] |
| Bioartificial Pancreas (Encapsulated Insulin-Secreting Cells) | Animal models | Implantable alternative to insulin therapy | Durability and immune rejection issues | [12] | |
| Gut Microbiome Modulation for Autoimmune Prevention | Early human studies | May prevent autoimmune response and preserve β-cells | Needs further validation, long-term effects unknown | [136] | |
| Nanomedicine-Based Insulin Delivery | Preclinical stage | More efficient insulin absorption, reduced injections | No human trials yet, safety concerns | [137] |
| Probiotic Type | Key Details | Type of Study (Participants) | Duration of Treatment | Key Findings | Reference |
|---|---|---|---|---|---|
| Multispecies Probiotic (Lactobacillus acidophilus, Lactobacillus plantarum, Bifidobacterium lactis, Saccharomyces boulardii) | Commonly found in fermented foods; supports gut health and immune modulation. | Randomized, double-blind, placebo-controlled clinical trial (91) | 6 months | Significant reduction in HbA1c, fasting glucose, and total cholesterol | [167,168] |
| Multispecies Probiotic (Lactobacillus casei, Bifidobacterium bifidum) | Frequently used in probiotic supplements; aids in gut microbiome stability. | Randomized controlled trial (60) | 12 weeks | Significant improvement in glycemic control and lipid profile. | [166] |
| Lactobacillus rhamnosusGG | Well-researched strain for gut health; found in dairy-based probiotic products. | Randomized controlled trial (33) | 6 months | No significant effect on β-cell function or HbA1c levels. | [169] |
| Multispecies Probiotic (Bifidobacterium longum, Lactobacillus bulgaricus, Streptococcus thermophilus) | Used in dairy products and probiotic formulations; supports digestion and metabolism. | Randomized, double-blinded, placebo-controlled pilot study (50) | 12 weeks | Significant reduction in fasting blood glucose levels. | [170] |
| Synbiotic Supplement (Probiotics + Prebiotics) | Combination of beneficial bacteria and dietary fibers for gut health. | Randomized controlled trial (130) | 6 months | Study protocol; results pending. | [171] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Batir-Marin, D.; Ștefan, C.S.; Boev, M.; Gurău, G.; Popa, G.V.; Matei, M.N.; Ursu, M.; Nechita, A.; Maftei, N.-M. A Multidisciplinary Approach of Type 1 Diabetes: The Intersection of Technology, Immunotherapy, and Personalized Medicine. J. Clin. Med. 2025, 14, 2144. https://doi.org/10.3390/jcm14072144
Batir-Marin D, Ștefan CS, Boev M, Gurău G, Popa GV, Matei MN, Ursu M, Nechita A, Maftei N-M. A Multidisciplinary Approach of Type 1 Diabetes: The Intersection of Technology, Immunotherapy, and Personalized Medicine. Journal of Clinical Medicine. 2025; 14(7):2144. https://doi.org/10.3390/jcm14072144
Chicago/Turabian StyleBatir-Marin, Denisa, Claudia Simona Ștefan, Monica Boev, Gabriela Gurău, Gabriel Valeriu Popa, Mădălina Nicoleta Matei, Maria Ursu, Aurel Nechita, and Nicoleta-Maricica Maftei. 2025. "A Multidisciplinary Approach of Type 1 Diabetes: The Intersection of Technology, Immunotherapy, and Personalized Medicine" Journal of Clinical Medicine 14, no. 7: 2144. https://doi.org/10.3390/jcm14072144
APA StyleBatir-Marin, D., Ștefan, C. S., Boev, M., Gurău, G., Popa, G. V., Matei, M. N., Ursu, M., Nechita, A., & Maftei, N.-M. (2025). A Multidisciplinary Approach of Type 1 Diabetes: The Intersection of Technology, Immunotherapy, and Personalized Medicine. Journal of Clinical Medicine, 14(7), 2144. https://doi.org/10.3390/jcm14072144