Prognostic Factors in High Grade Osteosarcoma Patients Who Received Neoadjuvant Therapy and Subsequently Underwent Surgery: Data from the Turkish Oncology Group

 , , , , , , , , , , add
Show full author list
, , , , , , , , , , add
Show full author list
Abstract
1. Introduction
2. Material and Methods
Statistical Analysis
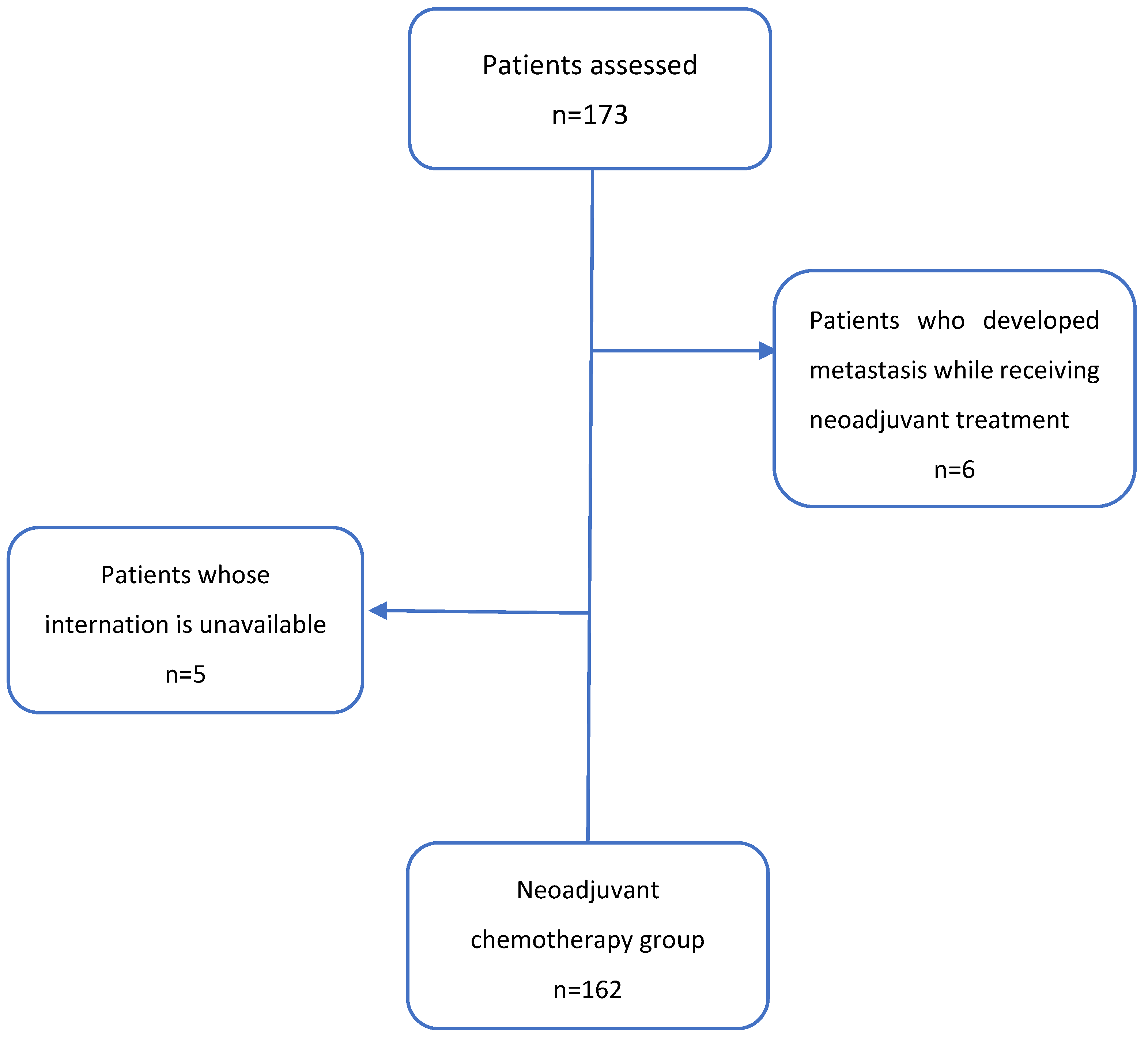
3. Results
3.1. The Study Population’s Demographic and Clinical Characteristics
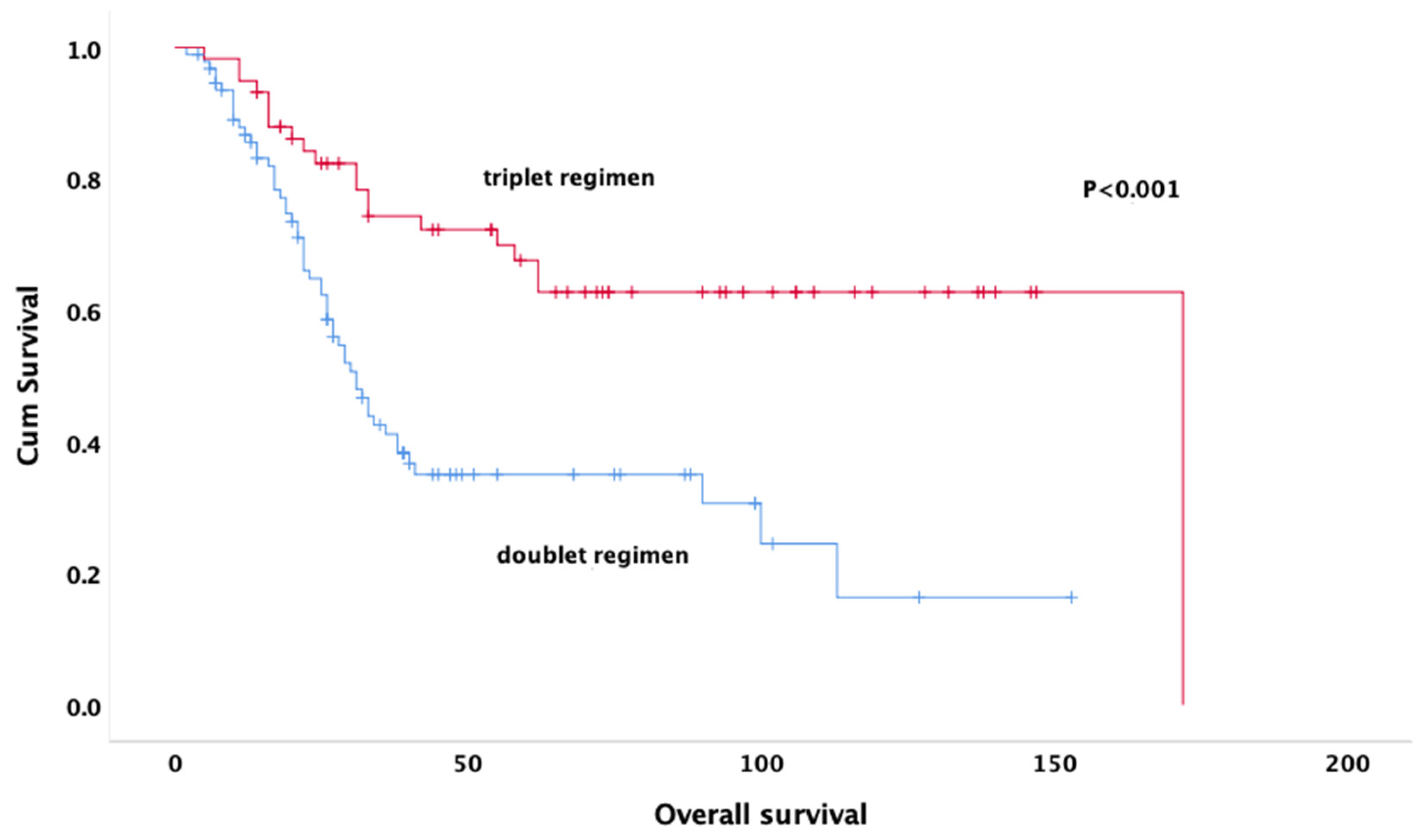
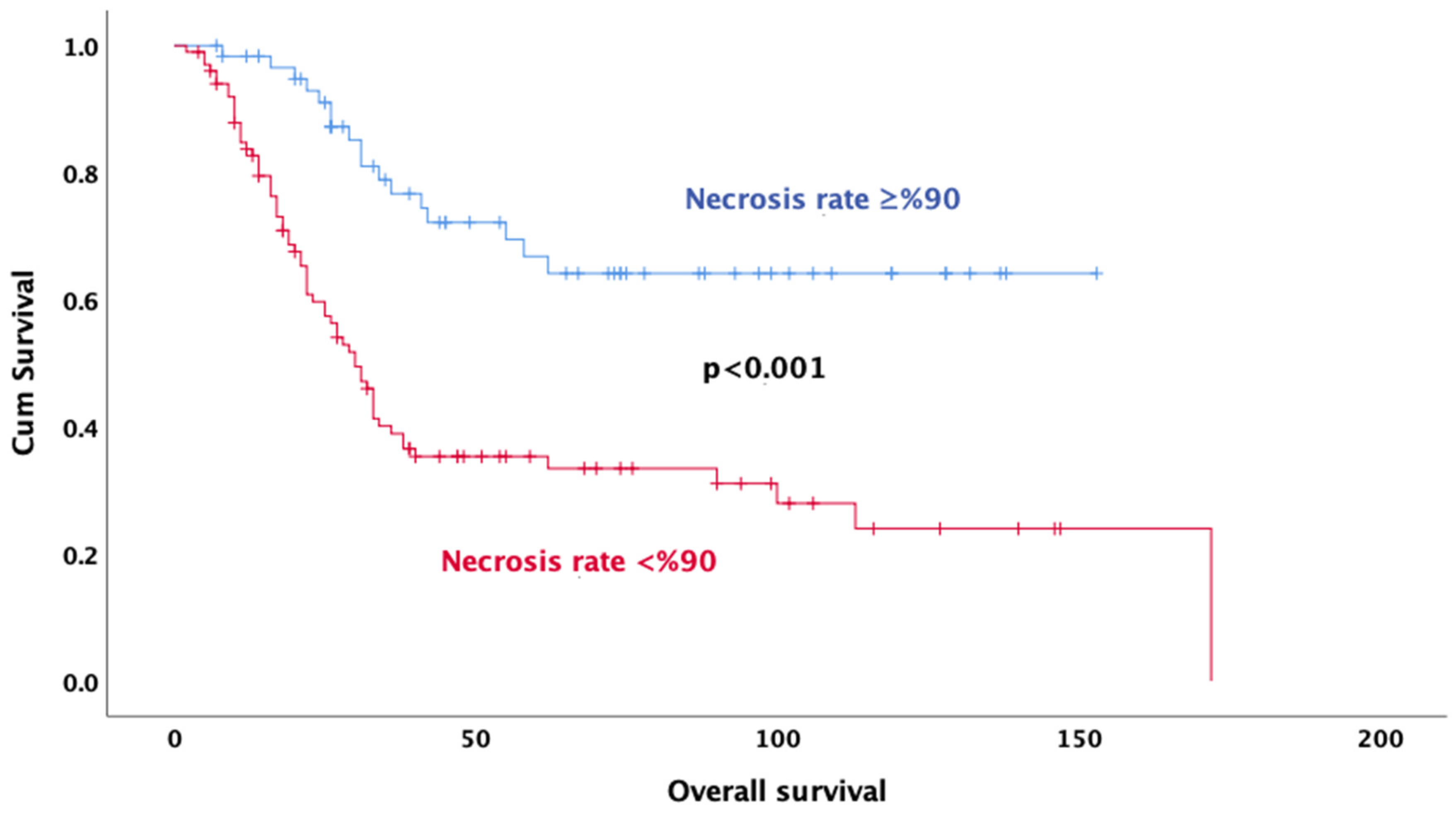
3.2. Survival Analysis
3.3. Univariable and Multivariable Cox Proportional Hazards Models
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- SEER Cancer Statistics Fact Sheets: Bone and Joint Cancer; National Cancer Institute: Bethesda, MD, USA, 2021. Available online: http://seer.cancer.gov/statfacts/html/bones.html (accessed on 8 September 2021).
- Ottaviani, G.; Jaffe, N. The etiology of osteosarcoma. Cancer Treat Res. 2009, 152, 1532. [Google Scholar]
- Mirabello, L.; Troisi, R.J.; Savage, S.A. Osteosarcoma incidence and survival rates from 1973 to 2004: Data from the Sur-veillance, Epidemiology, and End Results Program. Cancer 2009, 115, 1531–1543. [Google Scholar] [CrossRef] [PubMed]
- Xu, G.; Wu, H.; Zhang, Y.; Xu, Y.; Guo, X.; Baklaushev, V.P.; Chekhonin, V.P.; Peltzer, K.; Wang, J.; Lu, F.; et al. Risk and Prognostic Factors for Different Organ Metastasis in Primary Osteosarcoma: A Large Population-Based Analysis. Orthop. Surg. 2022, 14, 714–719. [Google Scholar] [CrossRef] [PubMed]
- Inwards, C.Y.; Unni, K.K. Classification and Grading of Bone Sarcomas. Hematol. Clin. N. Am. 1995, 9, 545–569. [Google Scholar] [CrossRef]
- WHO Classification of Tumours Editorial Board (Ed.) Soft tissue and bone tumours. In WHO Classification of Tumours, 5th ed.; IARC Press: Lyon, France, 2020. [Google Scholar]
- Isakoff, M.S.; Bielack, S.S.; Meltzer, P.; Gorlick, R. Osteosarcoma: Current Treatment and a Collaborative Pathway to Success. J. Clin. Oncol. 2015, 33, 3029–3035. [Google Scholar] [CrossRef]
- Bramwell, V.H.; Steward, W.P.; Nooij, M.; Whelan, J.; Craft, A.W.; Grimer, R.J.; Taminau, A.H.; Cannon, S.R.; Malcolm, A.J.; Hogendoorn, P.C.; et al. Neoadjuvant chemotherapy with doxorubicin and cisplatin in malignant fibrous histiocytoma of bone: A European Osteosarcoma Intergroup study. J. Clin. Oncol. 1999, 17, 3260–3269. [Google Scholar] [CrossRef]
- Souhami, R.L.; Craft, A.W.; Van der Eijken, J.W.; Nooij, M.; Spooner, D.; Bramwell, V.H.; Wierzbicki, R.; Malcolm, A.J.; Kirkpatrick, A.; Uscinska, B.M.; et al. Randomised trial of two regimens of chemotherapy in operable osteosarcoma: A study of the European Osteosarcoma Intergroup. Lancet 1997, 350, 911–917. [Google Scholar] [CrossRef]
- Bacci, G.; Forni, C.; Longhi, A.; Ferrari, S.; Donati, D.A.V.I.D.E.; De Paolis, M.; Barbieri, E.; Pignotti, E.; Rosito, P.; Versari, M. Long-term outcome for patients with non-metastatic Ewing’s sarcoma treated with adjuvant and neoadjuvant chemotherapies. 402 patients treated at Rizzoli between 1972 and 1992. Eur. J. Cancer 2004, 40, 73–83. [Google Scholar] [CrossRef]
- Goorin, A.M.; Schwartzentruber, D.J.; Devidas, M.; Gebhardt, M.C.; Ayala, A.G.; Harris, M.B.; Helman, L.J.; Grier, H.E.; Link, M.P. Presurgical chemotherapy compared with immediate surgery and adjuvant chemotherapy for non-metastatic osteosarcoma: Pediatric Oncology Group Study POG8651. J. Clin. Oncol. 2003, 21, 1574–1580. [Google Scholar] [CrossRef]
- Bacci, G.; Bertoni, F.; Longhi, A.; Ferrari, S.; Forni, C.; Biagini, R.; Bacchini, P.; Donati, D.; Manfrini, M.; Bernini, G.; et al. Neoadjuvant chemotherapy for high-grade central osteosarcoma of the extremity: Histologic response to preoperative chemotherapy correlates with histologic subtype of the tumor. Cancer 2003, 97, 3068–3075. [Google Scholar] [CrossRef]
- Patel, S.J.; Lynch, J.W.; Johnson, T.; Carroll, R.R.; Schumacher, C.; Spanier, S.; Scarborough, M. Dose-intense ifosfamide/doxorubicin/cisplatin based chemotherapy for osteosarcoma in adults. Am. J. Clin. Oncol. 2002, 25, 489–495. [Google Scholar] [CrossRef] [PubMed]
- Yu, D.; Zhang, S.; Feng, A.; Xu, D.; Zhu, Q.; Mao, Y.; Zhao, Y.; Lv, Y.; Han, C.; Liu, R.; et al. Methotrexate, doxorubicin, and cisplatinum regimen is still the preferred option for osteosarcoma chemotherapy: A meta-analysis and clinical observation. Medicine 2019, 98, e15582. [Google Scholar] [CrossRef] [PubMed]
- Marina, N.M.; Smeland, S.; Bielack, S.S.; Bernstein, M.; Jovic, G.; Krailo, M.D.; Hook, J.M.; Arndt, C.; van den Berg, H.; Brennan, B.; et al. Comparison of MAPIE versus MAP in patients with a poor response to preoperative chemotherapy for newly diagnosed high-grade osteosarcoma (EURAMOS-1): An open-label, international, randomised controlled trial. Lancet Oncol. 2016, 17, 1396–1408. [Google Scholar] [CrossRef]
- Hogendoorn, P.C.W.; Athanasou, N.; Bielack, S.; De Alava, E.; Dei Tos, A.P.; Ferrari, S.; Gelderblom, H.; Grimer, R.; Hall, K.S.; Hassan, B.; et al. Bone sarcomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2010, 21, 204–213. [Google Scholar] [CrossRef]
- Benjamin, R.S. Regional chemotherapy for osteosarcoma. Semin. Oncol. 1989, 16, 323–327. [Google Scholar] [PubMed]
- Benjamin, R.S.; Patel, S.R. Pediatric and adult osteosarcoma: Comparisons and contrasts in presentation andtherapy. In Pediatric and Adolescent Osteosarcoma; Jaffe, N., Bruland, O.S., Bielack, S.S., Eds.; Springer: Berlin/Heidelberg, Germany, 2010; pp. 355–363. [Google Scholar]
- Anninga, J.K.; Gelderblom, H.; Fiocco, M.; Kroep, J.R.; Taminiau, A.H.; Hogendoorn, P.C.; Egeler, R.M. Chemotherapeutic adjuvant treatment for osteosarcoma: Where do we stand? Eur. J. Cancer 2011, 47, 2431–2445. [Google Scholar] [CrossRef]
- Xin, S.; Wei, G. Prognostic factors in osteosarcoma: A study level meta-analysis and systematic review of current practice. J. Bone Oncol. 2020, 21, 100281. [Google Scholar] [CrossRef]
- Bacci, G.; Longhi, A.; Versari, M.; Mercuri, M.; Briccoli, A.; Picci, P. Prognostic factors for osteosarcoma of the extremity treated withneoadjuvant chemotherapy: 15-year experience in 789 patients treated at a single institution. Cancer 2006, 106, 1154–1161. [Google Scholar] [CrossRef]
- Salzer-Kuntschik, M.; Brand, G.; Delling, G. Determination of the degree of morphological regression following chemotherapy in malignant bone tumors. Pathologe 1983, 4, 135–141. (In German) [Google Scholar]
- Kushnir, I.; Kolander, Y.; Bickels, J.; Gortzak, Y.; Flusser, G.; Issakov, J.; Merimsky, O. Is it important to maintain high-dose intensity chemotherapy in the treatment of adults with osteosarcoma? Med. Oncol. 2014, 31, 1–6. [Google Scholar] [CrossRef]
- Harting, M.T.; Lally, K.P.; Andrassy, R.J.; Vaporciyan, A.A.; Cox, C.S., Jr.; Hayes-Jordan, A.; Blakely, M.L. Age as a prognostic factor for patients with osteosarcoma: An analysis of 438 patients. J. Cancer Res. Clin. Oncol. 2011, 136, 561–570. [Google Scholar] [CrossRef] [PubMed]
- Richardson, S.M.; Wurtz, L.D.; Collier, C.D. Ninety Percent or Greater Tumor Necrosis Is Associated with Survival and Social Determinants of Health in Patients with Osteosarcoma in the National Cancer Database. Clin. Orthop. Relat. Res. 2023, 481, 512–522. [Google Scholar] [CrossRef]
- Misaghi, A.; Goldin, A.; Awad, M.; Kulidjian, A.A. Osteosarcoma: A comprehensive review. SICOT J. 2018, 4, 12. [Google Scholar] [CrossRef]
- Bacci, G.; Ferrari, S.; Longhi, A.; Perin, S.; Forni, C.; Fabbri, N.; Salduca, N.; Versari, M.; Smith, K.V.J. Pattern of relapse in patients with osteosarcoma of the extremities treated with neo-adjuvant chemotherapy. Eur. J. Cancer 2001, 37, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Zeng, Y.; Liu, B.; Lu, G.; Xiang, Z.; Chen, J.; Yu, Y.; Zuo, Z.; Lin, Y.; Ma, J. Risk Factors, Prognostic Factors, and Nomograms for Distant Metastasis in Patients with Newly Diagnosed Osteosarcoma: A Population-Based Study. Front. Endocrinol. 2021, 12, 672024. [Google Scholar] [CrossRef] [PubMed]
- Erdoğan, F.; Çinka, H.; Akman, B.Ç.; Coşkun, H.S.; Dabak, N. Analysis of prognostic factors and histopathological response to neoadjuvant chemotherapy in osteosarcoma. Jt. Dis. Relat. Surg. 2023, 34, 196–206. [Google Scholar] [CrossRef]
- Bertrand, T.E.; Cruz, A.; Binitie, O.; Cheong, D.; Letson, D.G. Do Surgical Margins Affect Local Recurrence and Survival in Extremity, Nonmetastatic, High-grade Osteosarcoma? Clin. Orthop. Relat. Res. 2016, 474, 677–683. [Google Scholar] [CrossRef]
- Bispo, R.Z., Jr.; de Camargo, O.P. Prognostic factors in the survival of patients diagnosed with primary non-metastatic osteosarcoma with a poor response to neoadjuvant chemotherapy. Clinics 2009, 64, 1177–1186. [Google Scholar]
- Li, X.; Moretti, V.M.; Ashana, A.O.; Lackman, R.D. Impact of close surgical margin on local recurrence and survival in osteosarcoma. Int. Orthop. 2012, 36, 131–137. [Google Scholar] [CrossRef]
- Stein, G.S.; Lian, J.B.; Owen, T.A. Relationship of cell growth to the regulation of tissue-specific gene expression during osteoblast differentiation. FASEB J. 1990, 4, 3111–3123. [Google Scholar] [CrossRef]
- Ambroszkiewicz, J.; Gajewska, J.; Klepacka, T.; Chełchowska, M.; Laskowska-Klita, T.; Woz, W. Clinical utility of bio-chemical bone turnover markers in children and adolescents with osteosarcoma. Adv. Med. Sci. 2010, 55, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Ren, H.Y.; Sun, L.L.; Li, H.Y.; Ye, Z.M. Prognostic significance of serum alkaline phosphatase level in osteo- sarcoma: A meta-analysis of published data. BioMed Res. Int. 2015, 2015, 160835. [Google Scholar] [CrossRef] [PubMed]
- Kamal, A.F.; Abubakar, I.; Salamah, T. Alkaline phosphatase, lactic dehidrogenase, inflammatory variables and apparent diffusion coefficients from MRI for prediction of chemotherapy response in osteosarcoma. A cross sectional study. Ann. Med. Surg. 2021, 64, 102228. [Google Scholar] [CrossRef] [PubMed]
- Saeter, G.; Elomaa, I.; Wahlqvist, Y.; Alvegård, T.A.; Wiebe, T.; Monge, O.; Forrestier, E.; Solheim, Ø.P. Prognostic factors in bone sarcomas. Acta Orthop. Scand. 1997, 273, 156–160. [Google Scholar] [CrossRef]
- Bielack, S.S.; Kempf-Bielack, B.; Delling, G.; Exner, G.U.; Flege, S.; Helmke, K.; Kotz, R.; Salzer-Kuntschik, M.; Werner, M.; Winkelmann, W.; et al. Prognostic factors in high-grade osteosarcoma of the extremities or trunk: An analysis of 1702 patients treated on neoadjuvant cooperative osteosarcoma study group protocols. J. Clin. Oncol. 2002, 20, 776–790. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age, Year | |
|---|---|
| Median (IQR) | 20 (18–29) |
| Gender, n (%) Female Male | 76 (46.9) 86 (53.1) |
| ECOG-PS, n (%) 0–1 ≥2 | 160 (98.8) 2 (1.2) |
| Histology, n (%) Osteoblastic Chondroblastic Fibroblastic Telangiectatic NOS | 66(40.7) 46(28.4) 16 (9.9 12 (7.4) 22 (13.6) |
| Tumor size <8 cm ≥8 cm | 49 (30.2) 113 (69.8) |
| Location, n (%) Lower extremity Upper extremity Axial/vertebra | 135 (83.3) 18 (11.1) 9 (5.6) |
| Neoadjuvant treatment, n (%) Cisplatin + doxorubicin (doublet regimen) PEI (Triplet regimen) MAP (Triplet regimen) Others | 94 (58) 32 (19.8) 27 (16.7) 9 (5.5) |
| Type of surgery, n (%) Limb-sparing surgery Amputation | 147 (90.7) 15 (9.3) |
| Pathologic response, n (%) Complete response Presence of residual | 18 (11.1) 144 (88.9) |
| Rate of necrosis ≥%90, n (%) Doublet Treatment Triplet Treatment | 25 (43.85) 32 (56.15) |
| Surgical margin, n (%) R0 R1/2 | 150 (92.6) 12 (7.4) |
| Adjuvant therapy, n (%) Yes No | 143 (88.3) 19 (11.7) |
| LDH, n (%) Elevated levels Normal levels | 72 (44.4) 90 (55.6) |
| ALP, n (%) Elevated levels Normal levels | 105 (64.8) 57 (35.2) |
| Metastases at diagnosis, n (%) No metastasis Skip metastasis (Bone only) Distant metastasis (lung) | 136 (84) 8 (4.9) 18 (11.1) |
| Progression in follow-up, n (%) Local recurrence Distant metastasis Local recurrence + distant metastasis | 17 (17.0) 65 (65.0) 18 (18.0) |
| Univariate | Multivariate | |||
|---|---|---|---|---|
| Median DFS | p | HR (%95 CI) | p | |
| Age <65 ≥65 | 4.0 (2.1–5.9) 4.0 (2.8–5.1) | 0.697 | Ref 0.50 (0.27–0.92) | 0.024 |
| Gender Female Male | 3.0 (2.3–3.7) 4.0 (2.8–5.1) | 0.955 | ||
| Tumor size <8 cm ≥8 cm | 9.4 (2.1–16.7) 9.7 (7.9–11.5) | 0.717 | ||
| Neoadjuvant treatment Triplet regimen Doublet regimen | 12.7 (9.9–15.6) 8.6 (6.4–10.8) | 0.091 | ||
| Pathologic response Complete response Presence of residual | 4.1 (1.4–6.7) 3.4 (2.5–4.2) | 0.340 | ||
| Rate of necrosis %90 and above <90 | 13.7 (11.2–16.1) 8.6 (6.8–10.5) | 0.063 | ||
| Alkaline phosphatase Normal levels Elevated levels | 12.8 (10.5–15.2) 8.6 (6.3–10.9) | 0.301 | ||
| Lactate dehydrogenase Normal levels Elevated levels | 12.4 (8.8–16.0) 8.6 (6.1–11.1) | 0.292 | ||
| Surgical margin R1/2 R0 | 2.7 (0.1–5.3) 10.4 (7.5–13.2) | 0.040 | Ref 0.62 (0.32–1.21) | 0.163 |
| Adjuvant therapy Yes No | 12.3 (9.5–15.0) 3.4 (1.0–5.6) | <0.001 | Ref 2.37 (1.38–4.06) | <0.001 |
| Pathological fracture No Yes | 10.0 (6.9–12.9) 8.6 (4.6–12.7) | 0.320 | ||
| Pelvic location Yes No | 5.5 (1.9–9.1) 10.6 (7.2–14.0) | 0.094 | ||
| Metastases at diagnosis Yes No | 7.1 (2.5–11.6) 10.4 (7.3–13.4) | 0.363 | ||
| Univariate | Multivariate | |||
|---|---|---|---|---|
| Median OS | p | HR (%95 CI) | p | |
| Age <18 ≥18 | 172.0 (NR) 33.0 (27.1–38.9) | <0.001 | Ref 0.53 (0.22–1.3) | 0.163 |
| Gender Male Female | 33.0 (23.0–42.9) 113.0 (NR) | 0.032 | Ref 0.59(0.35–0.98) | 0.040 |
| Tumor size <8 cm ≥8 cm | NR 38.0 (18.7–57.2) | 0.048 | Ref 1.20 (0.71–2.03) | 0.490 |
| Neoadjuvant treatment Triplet regimen Doublet regimen | 172.0 (NR) 31.0 (25.6–36.4) | <0.001 | Ref 1.87 (1.07–3.20) | 0.021 |
| Pathologic response Complete response Presence of residual | NR 36.0 (18.0–54.0) | 0.011 | Ref 0.86 (0.26–2.78) | 0.812 |
| Rate of necrosis <90% ≥90% | 30.0 (25.2–34.8) NR | <0.001 | Ref 0.36 (0.20–0.64) | <0.001 |
| Alkaline phosphatase Elevated levels Normal levels | 31.0 (26.0–35.9) NR | 0.001 | Ref 0.35 (0.20–0.64) | <0.001 |
| Lactate dehydrogenase Normal levels Elevated levels | 62.0 (10.4–113.5) 33.0 (23.2–42.7) | 0.091 | ||
| Surgical margin R1/R2 R0 | 17.0 (8.5–25.4) 55.0 (14.3–95.7) | 0.012 | Ref 0.34 (0.14–0.82) | 0.010 |
| Pathological fracture No Yes | 58 (10.2–105.8) 33 (25.8–40.2) | 0.272 | ||
| Pelvic location No Yes | 55.0 (3.9–106.0) 22.0 (11.7–32.2) | 0.013 | Ref 0.79 (0.38–1.62) | 0.523 |
| Metastases at diagnosis Yes No | 31.0 (17.2–44.8) 62.0 (6.0–117.9) | <0.001 | Ref 0.37 (0.21–0.67) | 0.010 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sever, N.; Şimşek, F.; Onur, İ.D.; Arvas, H.; Guliyev, T.; Şakalar, T.; Çiçek, C.M.; Orman, S.; Çetin, E.B.; Kayaş, K.; et al. Prognostic Factors in High Grade Osteosarcoma Patients Who Received Neoadjuvant Therapy and Subsequently Underwent Surgery: Data from the Turkish Oncology Group. J. Clin. Med. 2025, 14, 2024. https://doi.org/10.3390/jcm14062024
Sever N, Şimşek F, Onur İD, Arvas H, Guliyev T, Şakalar T, Çiçek CM, Orman S, Çetin EB, Kayaş K, et al. Prognostic Factors in High Grade Osteosarcoma Patients Who Received Neoadjuvant Therapy and Subsequently Underwent Surgery: Data from the Turkish Oncology Group. Journal of Clinical Medicine. 2025; 14(6):2024. https://doi.org/10.3390/jcm14062024
Chicago/Turabian StyleSever, Nadiye, Fatih Şimşek, İlknur Deliktaş Onur, Hayati Arvas, Tural Guliyev, Teoman Şakalar, Ceren Mordağ Çiçek, Seval Orman, Emine Bihter Çetin, Kamil Kayaş, and et al. 2025. "Prognostic Factors in High Grade Osteosarcoma Patients Who Received Neoadjuvant Therapy and Subsequently Underwent Surgery: Data from the Turkish Oncology Group" Journal of Clinical Medicine 14, no. 6: 2024. https://doi.org/10.3390/jcm14062024
APA StyleSever, N., Şimşek, F., Onur, İ. D., Arvas, H., Guliyev, T., Şakalar, T., Çiçek, C. M., Orman, S., Çetin, E. B., Kayaş, K., Akbaş, S., Ağyol, Y., Güren, A. K., Erel, P., Kocaaslan, E., Paçacı, B., Tunç, M. A., Çelebi, A., Majidova, N., ... Bayoğu, İ. V. (2025). Prognostic Factors in High Grade Osteosarcoma Patients Who Received Neoadjuvant Therapy and Subsequently Underwent Surgery: Data from the Turkish Oncology Group. Journal of Clinical Medicine, 14(6), 2024. https://doi.org/10.3390/jcm14062024