
Comparison of Open Abdominal and Laparoscopic Bilateral Uterosacral Ligament Replacement: A One-Year Follow-Up Study

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Methods
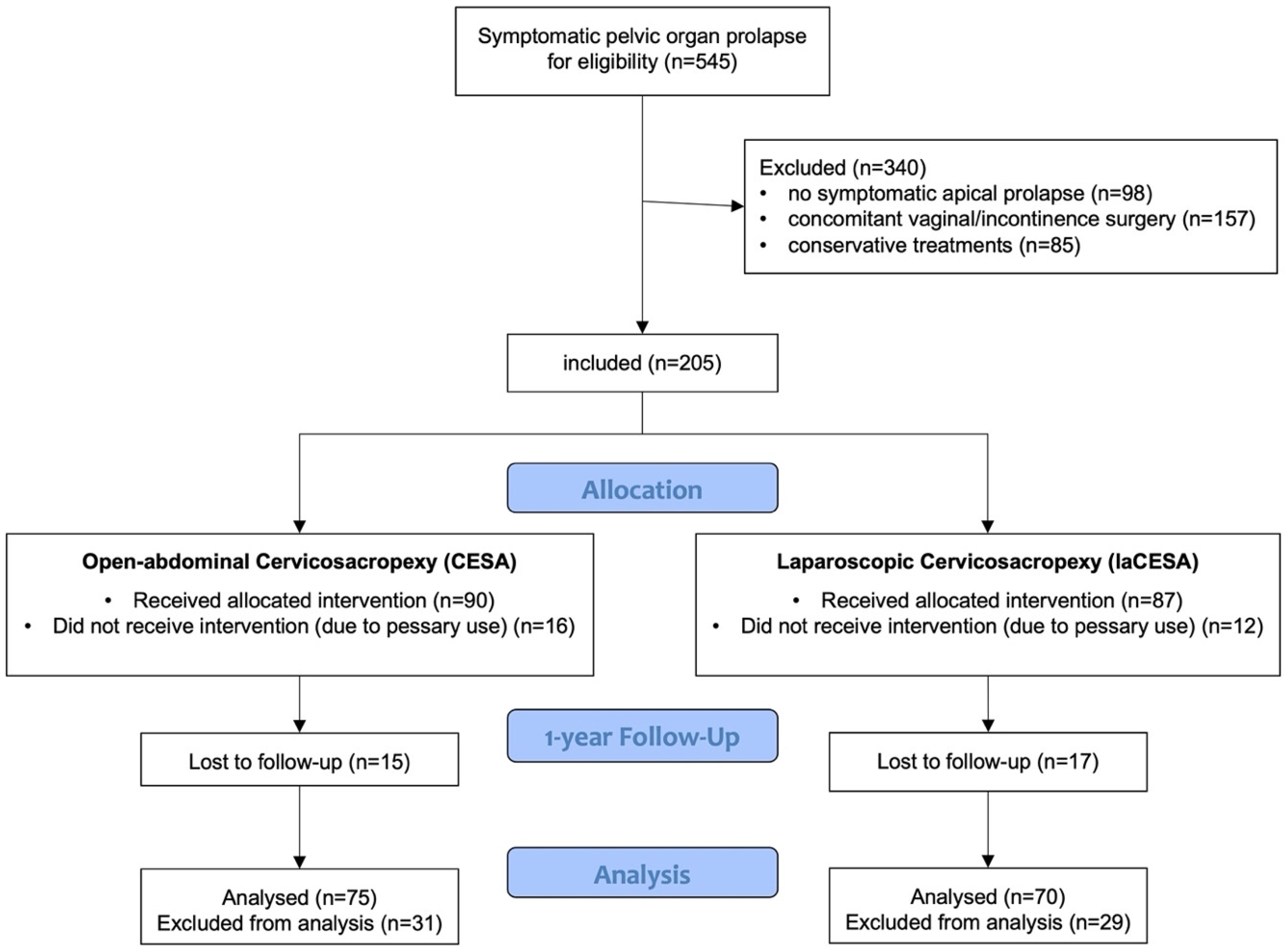
2.1. Patient Inclusion and Exclusion Criteria
2.2. Preoperative and Postoperative Assessments
2.3. Outcome Measures
2.4. Surgical Techniques
2.5. Statistical Analysis
3. Results
3.1. Preoperative Characteristics
3.2. Operative and Postoperative Findings
3.3. Intraoperative and Postoperative Complications
3.4. Urinary Continence Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CESA | Cervicosacropexy |
| ICIQ-UI SF | International Consultation on Incontinence Questionnaire—Urinary Incontinence |
| laCESA | Laparoscopic cervicosacropexy |
| MUI | Mixed urinary incontinence |
| POP | Pelvic organ prolapse |
| POP-Q | Pelvic organ prolapse quantification system |
| PVDF | Polyvinylidene-fluoride |
| UI | Urinary incontinence |
| UUI | Urgency urinary incontinence |
| USL | Uterosacral ligament |
| SCP | Sacrocolpopexy |
| SUI | Stress urinary incontinence |
| TOT | Transobturator tape |
References
- Olsen, A.L.; Smith, V.J.; Bergstrom, J.O.; Colling, J.C.; Clark, A.L. Epidemiology of surgically managed pelvic organ prolapse and urinary incontinence. Obstet. Gynecol. 1997, 89, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Spanknebel, B.; Dimpfl, T. Descensus genitalis—Klassische operative Konzepte. Gynakologe 2013, 46, 458–462. [Google Scholar] [CrossRef]
- Maher, C.; Feiner, B.; Baessler, K.; Christmann-Schmid, C.; Haya, N.; Brown, J. Surgery for women with apical vaginal prolapse. Cochrane Database Syst. Rev. 2016, 2017, CD012376. [Google Scholar] [CrossRef]
- Ganatra, A.M.; Rozet, F.; Sanchez-Salas, R.; Barret, E.; Galiano, M.; Cathelineau, X.; Vallancien, G. The Current Status of Laparoscopic Sacrocolpopexy: A Review. Eur. Urol. 2009, 55, 1089–1105. [Google Scholar] [CrossRef] [PubMed]
- Wagner, L.; Meurette, G.; Vidart, A.; Warembourg, S.; Terassa, J.B.; Berrogain, N.; Ragni, E.; Le Normand, L. Laparoscopic sacrocolpopexy for pelvic organ prolapse: Guidelines for clinical practice. Prog. Urol. 2016, 26, S27–S37. [Google Scholar] [CrossRef]
- Wong, V.; Guzman Rojas, R.; Shek, K.L.; Chou, D.; Moore, K.H.; Dietz, H.P. Laparoscopic sacrocolpopexy: How low does the mesh go? Ultrasound Obstet. Gynecol. 2017, 49, 404–408. [Google Scholar] [CrossRef]
- Manodoro, S.; Werbrouck, E.; Veldman, J.; Haest, K.; Corona, R.; Claerhout, F.; Coremans, G.; De Ridder, D.; Spelzini, F.; Deprest, J. Laparoscopic approach in the pelvic floor surgery. Ceska Gynekol. 2011, 76, 418–424. [Google Scholar] [CrossRef]
- De Boer, T.A.; Kluivers, K.B.; Withagen, M.I.J.; Milani, A.L.; Vierhout, M.E. Predictive factors for overactive bladder symptoms after pelvic organ prolapse surgery. Int. Urogynecol. J. 2010, 21, 1143–1149. [Google Scholar] [CrossRef]
- De Boer, T.A.; Hove MCPSTen Burger, C.W.; Vierhout, M.E. The prevalence and risk factors of overactive bladder symptoms and its relation to pelvic organ prolapse symptoms in a general female population. Int. Urogynecol. J. 2011, 22, 569–575. [Google Scholar] [CrossRef]
- Rajshekhar, S.; Mukhopadhyay, S.; Morris, E. Early safety and efficacy outcomes of a novel technique of sacrocolpopexy for the treatment of apical prolapse. Int. J. Gynecol. Obstet. 2016, 135, 182–186. [Google Scholar] [CrossRef]
- Joukhadar, R.; Meyberg-Solomayer, G.; Hamza, A.; Radosa, J.; Bader, W.; Barski, D.; Ismaeel, F.; Schneider, G.; Solomayer, E.; Baum, S. A novel operative procedure for pelvic organ prolapse utilizing a MRI-visible mesh implant: Safety and outcome of modified laparoscopic bilateral sacropexy. BioMed Res. Int. 2015, 2015, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Rexhepi, S.; Rexhepi, E.; Stumm, M.; Mallmann, P.; Ludwig, S. Laparoscopic Bilateral Cervicosacropexy and Vaginosacropexy: New Surgical Treatment Option in Women with Pelvic Organ Prolapse and Urinary Incontinence. J. Endourol. 2018, 32, 1058–1064. [Google Scholar] [CrossRef]
- Ludwig, S.; Morgenstern, B.; Mallmann, P.; Jäger, W. Laparoscopic bilateral cervicosacropexy: Introduction to a new tunneling technique. Int. Urogynecol. J. 2019, 30, 1215–1217. [Google Scholar] [CrossRef]
- Alkatout, I.; Mettler, L. Hysterectomy: A Comprehensive Surgical Approach. In Hysterectomy: A Comprehensive Surgical Approach; Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar] [CrossRef]
- Cassis, C.; Mukhopadhyay, S.; Morris, E. Standardizing abdominal sacrocolpopexy for the treatment of apical prolapse: One year on. Int. J. Gynecol. Obstet. 2019, 147, 49–53. [Google Scholar] [CrossRef]
- Jäger, W.; Brakat, A.; Ludwig, S.; Mallmann, P. Effects of the apical suspension of the upper vagina by cervicosacropexy or vaginosacropexy on stress and mixed urinary incontinence. Pelviperineology 2021, 40, 32–38. [Google Scholar] [CrossRef]
- Veit-Rubin, N.; Dubuisson, J.B.; Gayet-Ageron, A.; Lange, S.; Eperon, I.; Dubuisson, J. Patient satisfaction after laparoscopic lateral suspension with mesh for pelvic organ prolapse: Outcome report of a continuous series of 417 patients. Int. Urogynecol. J. 2017, 28, 1685–1693. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Li, Z.; Si, K.; Dai, Q.; Qiao, Y.; Li, D.; Zhang, L.; Wu, F.; He, J.; Wu, G. Effectiveness of Laparoscopic Pectopexy for Pelvic Organ Prolapse Compared with Laparoscopic Sacrocolpopexy. J. Minim Invasive Gynecol. 2023, 30, 833–840.e2. [Google Scholar] [CrossRef]
- Naumann, G.; Börner, C.; Naumann, L.J.; Schröder, S.; Hüsch, T. A novel bilateral anterior sacrospinous hysteropexy technique for apical pelvic organ prolapse repair via the vaginal route: A cohort study. Arch. Gynecol. Obstet. 2022, 306, 141–149. [Google Scholar] [CrossRef]
- DeLancey, J.O.L. Anatomy and biomechanics of genital prolapse. Clin. Obstet. Gynecol. 1993, 36, 897–909. [Google Scholar] [CrossRef]
- Ashton-Miller, J.A.; DeLancey, J.O.L. Functional anatomy of the female pelvic floor. In Evidence-Based Physical Therapy for the Pelvic Floor: Bridging Science and Clinical Practice, 2nd ed.; Elsevier: Amsterdam, The Netherlands, 2015. [Google Scholar] [CrossRef]
- Summers, A.; Winkel, L.A.; Hussain, H.K.; DeLancey, J.O.L. The relationship between anterior and apical compartment support. Am. J. Obstet. Gynecol. 2006, 194, 1438–1443. [Google Scholar] [CrossRef]
- Bump, R.C.; Mattiasson, A.; Bo, K.; Brubaker, L.P.; DeLancey, J.O.L.; Klarskov, P.; Shull, B.L.; Smith, A.R.B. The standardization of terminology of female pelvic organ prolapse and pelvic floor dysfunction. Am. J. Obstet. Gynecol. 1996, 175, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Bump, R.C. The POP-Q system: Two decades of progress and debate. Int. Urogynecol. J. 2014, 25, 441–443. [Google Scholar] [CrossRef] [PubMed]
- Barber, M.D.; Brubaker, L.; Nygaard, I.; Wheeler, T.L.; Schaffer, J.; Chen, Z.; Spino, C. Defining success after surgery for pelvic organ prolapse. Obstet. Gynecol. 2009, 114, 600–609. [Google Scholar] [CrossRef]
- Nygaard, I.E.; McCreery, R.; Brubaker, L.; Connolly, A.M.; Cundiff, G.; Weber, A.M.; Zyczynski, H. Abdominal sacrocolpopexy: A comprehensive review. Obstet. Gynecol. 2004, 104, 805–823. [Google Scholar] [CrossRef]
- Costantini, E.; Brubaker, L.; Cervigni, M.; Matthews, C.A.; O’Reilly, B.A.; Rizk, D.; Giannitsas, K.; Maher, C.F. Sacrocolpopexy for pelvic organ prolapse: Evidence-based review and recommendations. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 205, 60–65. [Google Scholar] [CrossRef]
- Jäger, W.; Mirenska, O.; Brügge, S. Surgical treatment of mixed and urge urinary incontinence in women. Gynecol. Obstet. Investig. 2012, 74, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, S.; Becker, I.; Mallmann, P.; Jäger, W. Comparison of solifenacin and bilateral apical fixation in the treatment of mixed and urgency urinary incontinence in women: URGE 1 study, a randomized clinical trial. In Vivo 2019, 33, 1949–1957. [Google Scholar] [CrossRef]
- Zhao, X.; Chen, G.; Lei, L.; Wu, X.; Liu, S.; Wang, J.; Hu, B.; Lyu, W. Key anatomies of DeLancey’s three levels of vaginal support theory: An observation in laparoscopic surgery. Zhejiang Da Xue Xue Bao Yi Xue Ban 2018, 47, 329–337. [Google Scholar] [CrossRef]
- Frigerio, M.; Barba, M.; Marino, G.; Volontè, S.; Cola, A. Intraoperative ultrasound assessment of ureteral patency after uterosacral ligaments apical suspension for prolapse surgical repair: A feasibility study. Int. J. Gynecol. Obstet. 2023, 163, 103–107. [Google Scholar] [CrossRef]
- Mihai, I.; Dura, H.; Teodoru, C.A.; Todor, S.B.; Ichim, C.; Grigore, N.; Mohor, C.I.; Mihetiu, A.; Oprinca, G.; Bacalbasa, N.; et al. Intraoperative Ultrasound: Bridging the Gap between Laparoscopy and Surgical Precision during 3D Laparoscopic Partial Nephrectomies. Diagnostics 2024, 14, 942. [Google Scholar] [CrossRef]
- Klinge, U.; Klosterhalfen, B.; Öttinger, A.P.; Junge, K.; Schumpelick, V. PVDF as a new polymer for the construction of surgical meshes. Biomaterials 2002, 23, 3487–3493. [Google Scholar] [CrossRef] [PubMed]
- Kolberg, H.; Liedl, B.; Göretzlehner, U.; Klinge, U.; Stephanou, M.; Klosterhalfen, B. PVDF als biokompatibler Implantatwerkstoff im Beckenboden. Geburtshilfe Frauenheilkd 2008, 68, PO_Gyn_04_30. [Google Scholar] [CrossRef]
- Junge, K.; Klinge, U.; Rosch, R.; Stumpf, M.; Klosterhalfen, B.; Schumpelick, V. PVDF: A New Alternative. In Meshes: Benefits and Risks; Springer: Berlin/Heidelberg, Germany, 2004. [Google Scholar] [CrossRef]
- Klink, C.D.; Junge, K.; Binnebösel, M.; Alizai, H.P.; Otto, J.; Neumann, U.P.; Klinge, U. Comparison of long-term biocompability of PVDF and PP meshes. J. Investig. Surg. 2011, 24, 292–299. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | CESA a (n = 75) | laCESA a (n = 70) | p-Value |
|---|---|---|---|
| Age, mean years (range) | 59 (32–82) | 58 (28–81) | 0.714 b |
| Body mass index (BMI) c | 27 (18–42) | 26 (18–37) | 0.215 b |
| Parity, mean (range) | 2 (0–7) | 2 (0–5) | 0.467 b |
| Pelvic organ prolapse d | |||
| apical POP-Q stage 0 | 0 (0%) | 0 (0%) | 1.000 e |
| apical POP-Q stage 1 | 33 (44%) | 23 (33%) | 0.177 e |
| apical POP-Q stage 2 | 37 (49%) | 36 (51%) | 0.869 e |
| apical POP-Q stage 3–4 | 5 (7%) | 11 (16%) | 0.112 e |
| Type of urinary incontinence f | |||
| Urinary incontinent | 58 (77%) | 48 (69%) | 0.264 e |
| Stress urinary incontinence (SUI) | 7 (12%) | 8 (17%) | 0.788 e |
| Urgency urinary incontinence (UUI) | 11 (19%) | 12 (25%) | 1.000 e |
| Mixed urinary incontinence (MUI) | 40 (69%) | 28 (28%) | 0.021 e |
| History of previous surgery g | |||
| Sacrocolpopexy | 2 (3%) h | 0 (0%) | 0.170 e |
| Laparoscopic subtotal hysterectomy | 6 (8%) i | 5 (7%) | 0.846 e |
| Anterior colporrhaphy | 3 (4%) | 1 (1%) | 0.602 e |
| Anterior colporrhaphy with mesh | 0 (0%) | 1 (1%) | 0.301 e |
| Colposuspension (Burch) | 1 (1%) | 0 (0%) | 0.334 e |
| Tension-free vaginal tape (TVT) | 4 (5%) | 0 (0%) | 0.092 e |
| Transobturator tape insertion (TOT) | 1 (1%) | 0 (0%) | 0.334 e |
| Surgical Steps | Abdominal CESA | Laparoscopic CESA |
|---|---|---|
| Surgical access path | Pfannenstiel incision | Establishment of CO2 peritoneum a Four trocars (Figure 3):
|
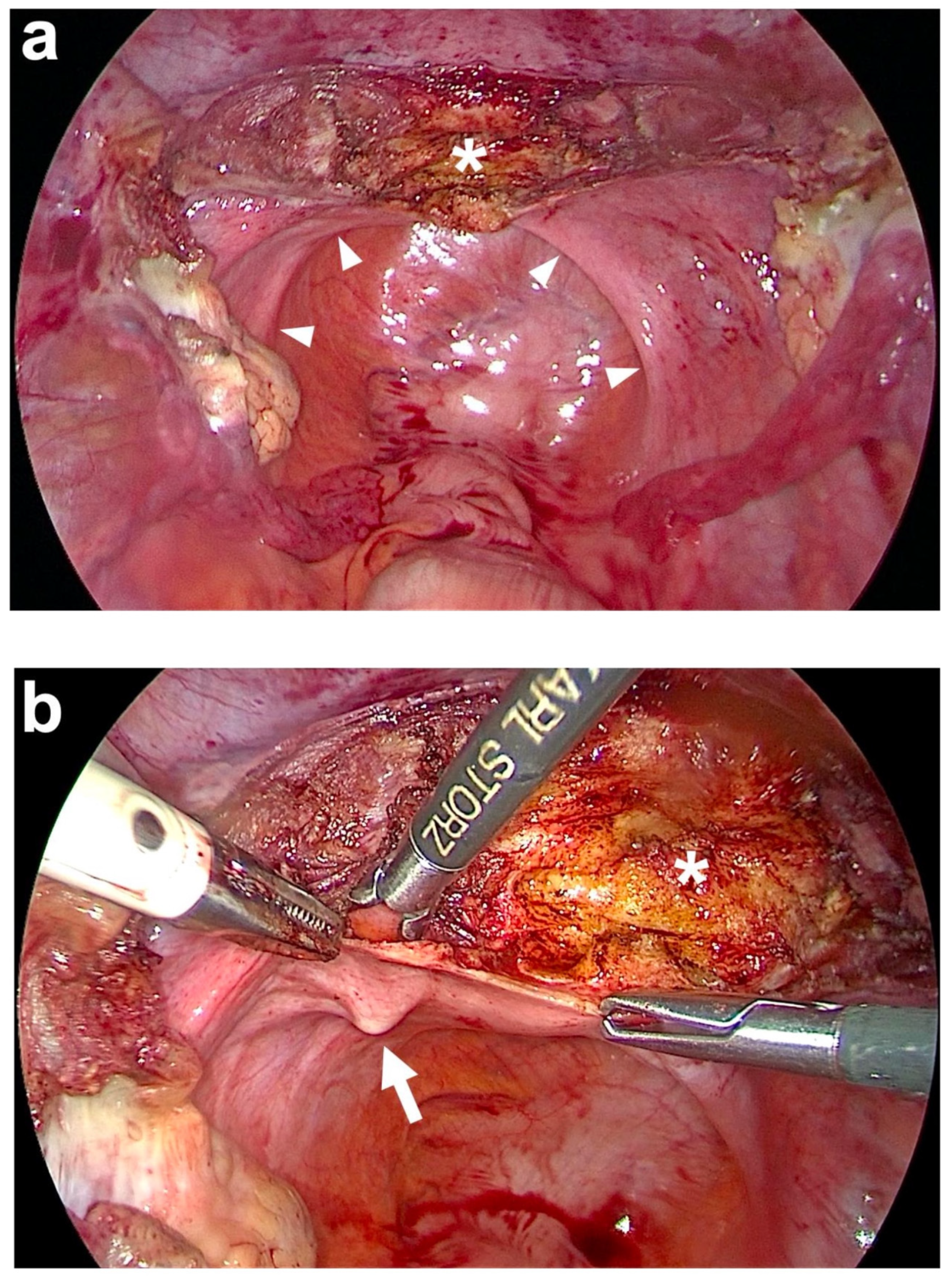
| Preparation of anterior fixation sides | Subtotal hysterectomy (if necessary) with monopolar electric knife above the origin of both USL and at peritoneal fold of bladder’s peritoneum at anterior cervix. | Subtotal hysterectomy (if necessary) with monopolar electric needle above the origin of both USL and at peritoneal fold of bladder’s peritoneum at anterior cervix (Figure 4a). |
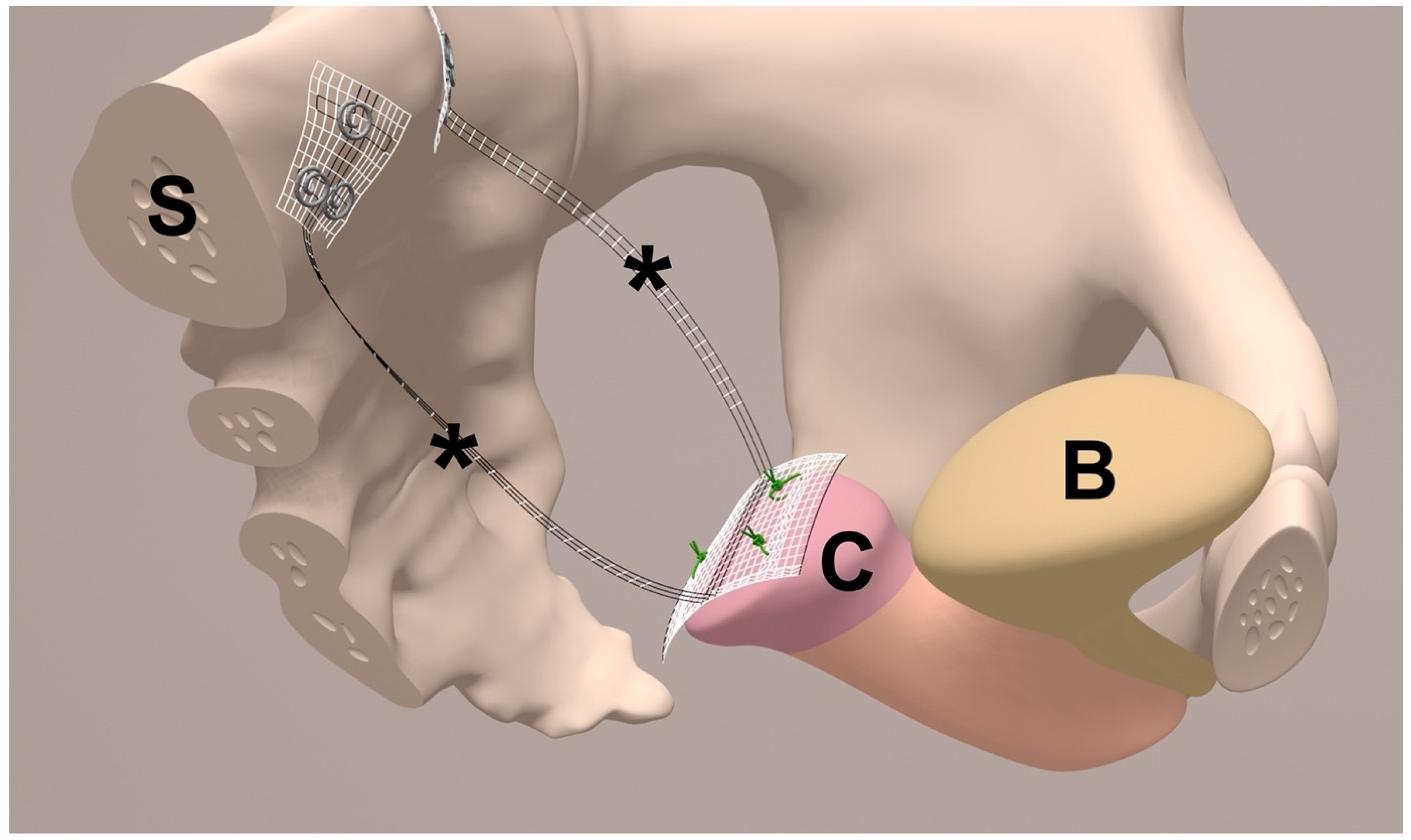
| Anterior fixation of middle part of PVDF structure e (Figure 1) | Sutured to the cut surface of the cervix with 4 interrupted, non-absorbable sutures f. | Sutured to the cut surface of the cervix with 3 interrupted, non-absorbable sutures f (Figure 8a). |
| Instrument for USL replacement (tunneling) | Semi-circular curved hook with blunt tip (tunneling device). | Semi-circular curved hook with blunt tip (tunneling device), inserted via the right lateral trocar incision (after removing the right trocar) (Figure 3). |
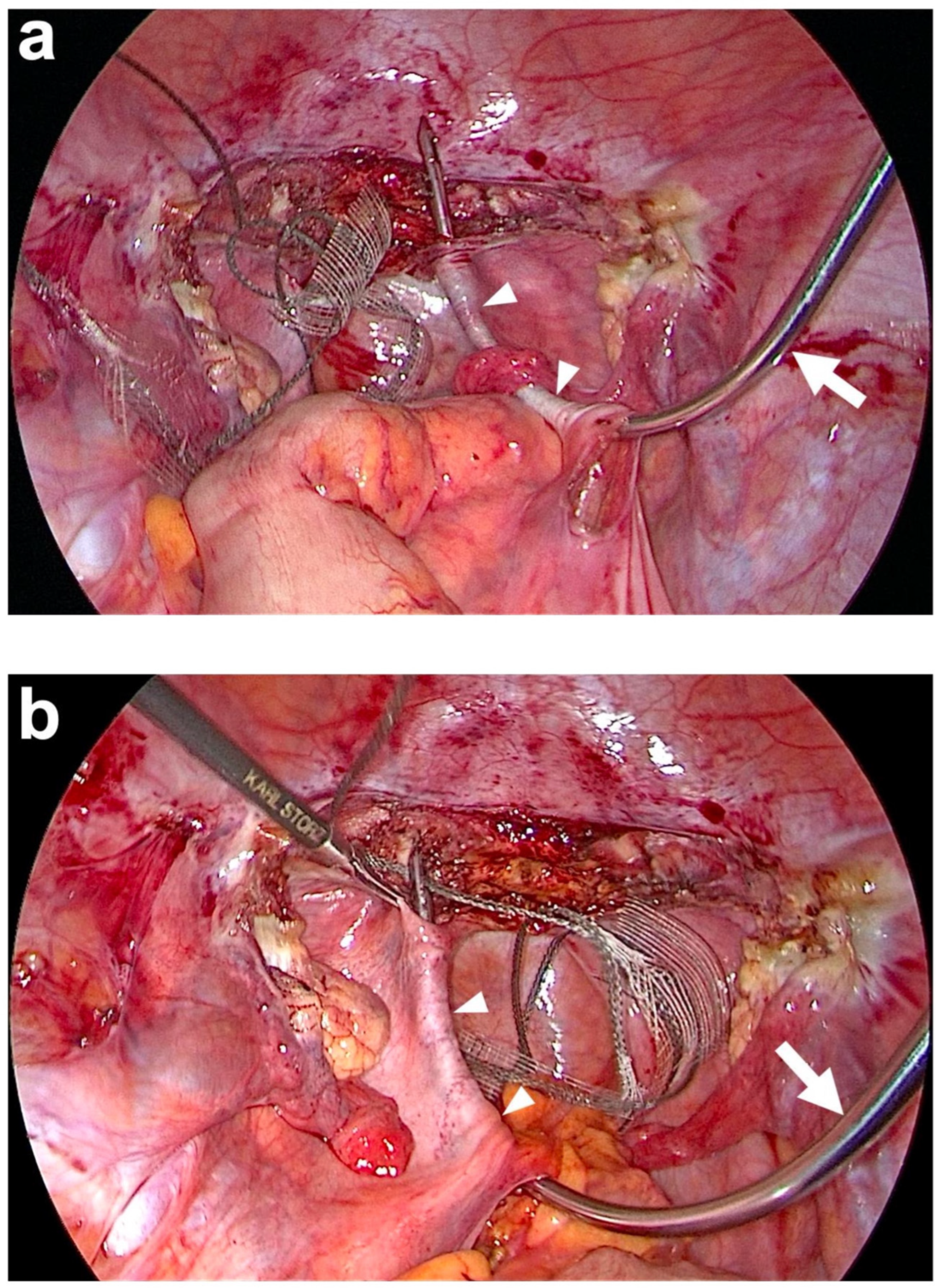
| Tunneling of both USL | The blunt tip of tunneling device is inserted into the left sacral peritoneal window and advanced under the peritoneum towards left paracervical tissue. Threading one lateral end of the PVDF structure through the hole of the tunneling device’s tip and pulling it back. Same procedure on the right side. | The blunt tip of tunneling device is inserted into the left sacral peritoneal window and advanced under the peritoneum towards the left paracervical tissue. Threading one lateral end of the PVDF structure through the hole of the tunneling device’s tip and pulling it back. Same procedure on the right side (Figure 6). |
| Preparation of posterior fixation sides | Incision of lateral peritoneum above S1/promontory for 2 cm on either side of rectosigmoid colon. | Incision of lateral peritoneum above S1/promontory for 2 cm on either side of rectosigmoid colon (Figure 5). |
| Posterior fixation of left and right arm of PVDF structure (Figure 1) | At left and right prevertebral fascial layer at S1 with 2 interrupted, non-absorbable sutures each e within the defined locations at the PVDF structure. | At left and right prevertebral fascial layer on S1/promontory with 3 titanium helices each g within the defined locations at the PVDF structure (Figure 2 and Figure 7). |
| Peritoneal closure | Closure of peritoneum above cut surface of cervix with running, absorbable suture h. | Closure of peritoneum above cut surface of cervix with running, absorbable suture i (Figure 8b). |
| Variable | CESA a (n = 75) | laCESA a (n = 70) | p-Value |
|---|---|---|---|
| Concomitant vaginal surgery, n (%) | |||
| Anterior colporrhaphy | 10 (13%) | 18 (26%) | 0.091 b |
| Posterior colporrhaphy | 1 (1%) | 7 (10%) | 0.029 b |
| Transobturator tape insertion | 0 (0%) | 2 (3%) | 0.231 b |
| Colposuspension | 2 (3%) | 0 (0%) | 0.497 b |
| Vaginal surgery within follow-up, n (%) | |||
| Transobturator tape insertion | 21 (28%) | 18 (26%) | 0.852 b |
| Anterior colporrhaphy | 11 15%) | 9 (13%) | 0.813 b |
| Posterior colporrhaphy | 1 (1%) | 1 (1%) | n.s. b |
| Colposuspension | 2 (3%) | 0 (0%) | 0.497 b |
| Operating time (min), mean (range) | 120 (89–168) | 93 (58–137) c | 0.001 d |
| Hospitalization (days), mean (range) | 5 (3–8) | 3 (1–5) | 0.001 d |
| Intraoperative complications, n (%) | |||
| Bladder injuries e | 1 (1%) | 1 (1%) | n.s. b |
| Bowel injury | 1 (1%) f | 0 (0%) | n.s. b |
| Significant bleeding/Vessel injury | 0 (0%) | 0 (0%) | - |
| Ureter lesion | 0 (0%) | 0 (0%) | - |
| Complications at 1-year postoperative, n (%) | |||
| Obstructed defecation | 0 (0%) | 0 (0%) | - |
| Reoperation for apical prolapse | 0 (0%) | 1 (1%) g | 0.483 b |
| Mesh erosion | 0 (0%) | 0 (0%) | - |
| Urinary retention | 0 (0%) | 0 (0%) | - |
| Clinical Outcome | CESA (n = 75) | laCESA (n = 70) | p-Value |
|---|---|---|---|
| Pelvic organ prolapse a, n (%) | |||
| apical POP-Q stage 0 | 75 (100%) | 70 (100%) b | 0.483 c |
| apical POP-Q stage 1 | 0 (0%) | 0 (0%) | - |
| Urinary continence status | |||
| continent | 34 (59%) d | 29 (60%) e | 0.726 c |
| stress urinary incontinence | 6 (10%) | 8 (17%) | 0.084 c |
| urgency urinary incontinence | 6 (10%) | 3 (6%) | 0.496 c |
| mixed urinary incontinence | 12 (21%) | 8 (17%) | 0.643 c |
| ICIQ-UI score, mean (range) f | 3 (0–21) | 4 (0–16) | 0.704 g |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ludwig, S.; Pfleiderer, M.; Püchel, J.; Amir-Kabirian, C.; Jeschke, J.; Ratiu, D.; Eichler, C.; Morgenstern, B.; Mallmann, P.; Radosa, J.; et al. Comparison of Open Abdominal and Laparoscopic Bilateral Uterosacral Ligament Replacement: A One-Year Follow-Up Study. J. Clin. Med. 2025, 14, 1880. https://doi.org/10.3390/jcm14061880
Ludwig S, Pfleiderer M, Püchel J, Amir-Kabirian C, Jeschke J, Ratiu D, Eichler C, Morgenstern B, Mallmann P, Radosa J, et al. Comparison of Open Abdominal and Laparoscopic Bilateral Uterosacral Ligament Replacement: A One-Year Follow-Up Study. Journal of Clinical Medicine. 2025; 14(6):1880. https://doi.org/10.3390/jcm14061880
Chicago/Turabian StyleLudwig, Sebastian, Mathieu Pfleiderer, Jodok Püchel, Constanze Amir-Kabirian, Janice Jeschke, Dominik Ratiu, Christian Eichler, Bernd Morgenstern, Peter Mallmann, Julia Radosa, and et al. 2025. "Comparison of Open Abdominal and Laparoscopic Bilateral Uterosacral Ligament Replacement: A One-Year Follow-Up Study" Journal of Clinical Medicine 14, no. 6: 1880. https://doi.org/10.3390/jcm14061880
APA StyleLudwig, S., Pfleiderer, M., Püchel, J., Amir-Kabirian, C., Jeschke, J., Ratiu, D., Eichler, C., Morgenstern, B., Mallmann, P., Radosa, J., & Thangarajah, F. (2025). Comparison of Open Abdominal and Laparoscopic Bilateral Uterosacral Ligament Replacement: A One-Year Follow-Up Study. Journal of Clinical Medicine, 14(6), 1880. https://doi.org/10.3390/jcm14061880