
The Impact of Chronic Obstructive Pulmonary Disease Severity on Psychological and Functional Outcomes: A Cross-Sectional Analysis

 , , ,
, , ,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
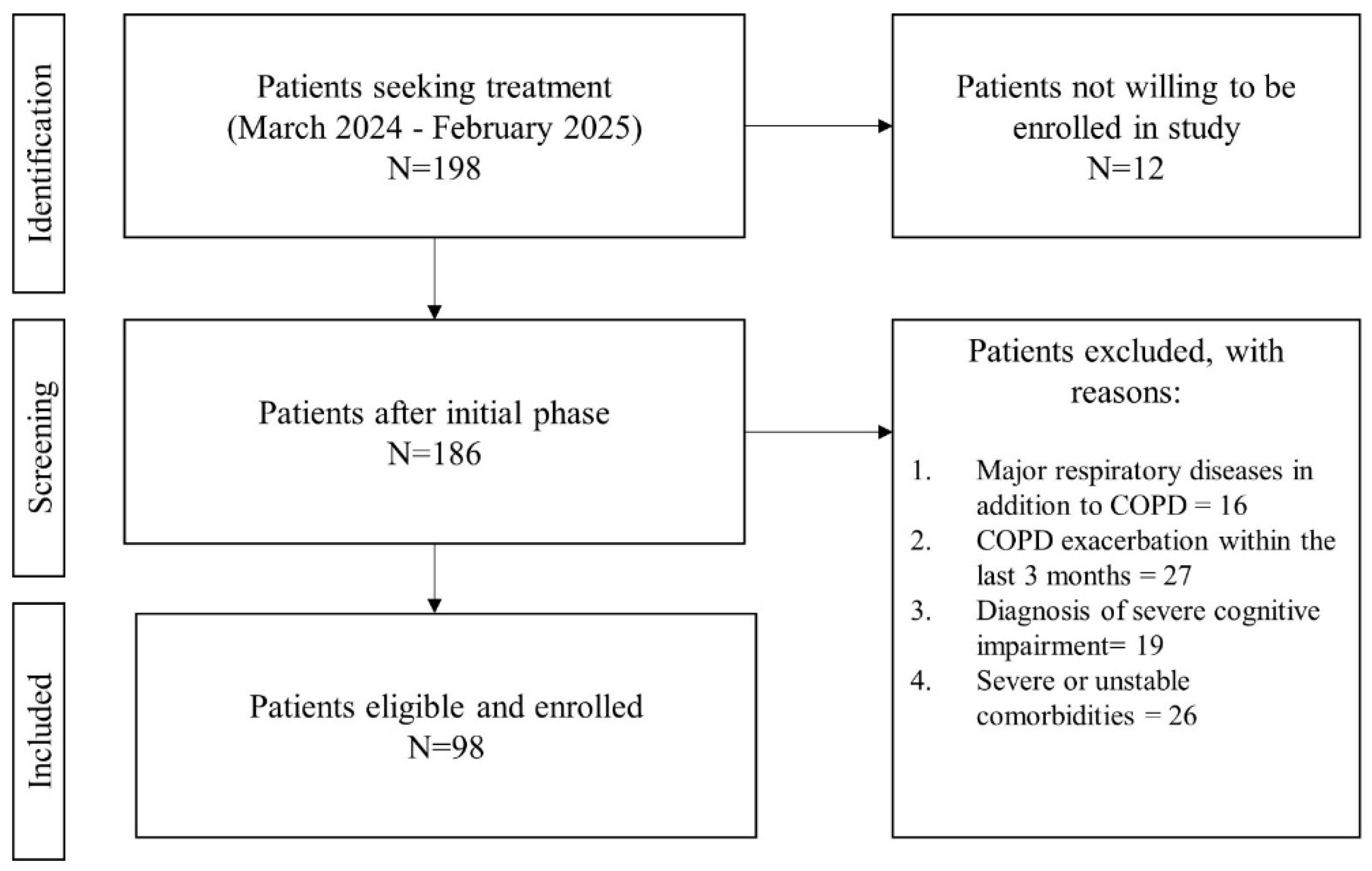
2.2. Participant Recruitment
2.3. Data Collection
2.4. Outcomes
Lung Volume
2.5. Anxiety and Depression
2.6. Impact of the Disease
2.7. Shame and Guilt
2.8. Self-Efficacy
2.9. Fear of Negative Evaluation
2.10. Self-Compassion
2.11. Dyspnea Assessment
2.12. Functional Capacity
2.13. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| COPD | Chronic obstructive pulmonary disease |
| HRQoL | Health-related quality of life |
| FEV1 | Forced expiratory volume in 1 s |
| FVC | Forced vital capacity |
| mMRC | Modified Medical Research Council scale |
| ATS | American Thoracic Society |
| ERS | European Respiratory Society |
| HADS | Hospital Anxiety and Depression Scale |
| CAT | COPD assessment test |
| SSGS | State Shame and Guilt Scale |
| PRAISE | Pulmonary Rehabilitation Adapted Index of Self-Efficacy |
| BFNE | Brief Fear of Negative Evaluation |
| SCS-SF | Self-Compassion Scale—Short Form |
| 6MWT | Six Minute Walk Test |
| SD | Standard deviation |
| IQRs | Interquartile ranges |
| BMI | Body mass index |
References
- Venkatesan, P. GOLD COPD report: 2024 update. Lancet Respir. Med. 2024, 12, 15–16. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Kuhn, M.; Prettner, K.; Yu, F.; Yang, T.; Bärnighausen, T.; Bloom, D.E.; Wang, C. The global economic burden of chronic obstructive pulmonary disease for 204 countries and territories in 2020–50: A health-augmented macroeconomic modelling study. Lancet Glob. Health 2023, 11, e1183. [Google Scholar] [CrossRef] [PubMed]
- Hanania, N.A.; O’donnell, D.E. Activity-related dyspnea in chronic obstructive pulmonary disease: Physical and psychological consequences, unmet needs, and future directions. Int. J. Chronic Obstr. Pulm. Dis. 2019, 14, 1127–1138. [Google Scholar] [CrossRef] [PubMed]
- Yohannes, A.M.; Junkes-Cunha, M.; Smith, J.; Vestbo, J. Management of Dyspnea and Anxiety in Chronic Obstructive Pulmonary Disease: A Critical Review. J. Am. Med. Dir. Assoc. 2017, 18, 1906.e1–1096.e17. [Google Scholar] [CrossRef] [PubMed]
- Yi, Q.F.; Yang, G.L.; Yan, J. Self-Efficacy Intervention Programs in Patients with Chronic Obstructive Pulmonary Disease: Narrative Review. Int. J. Chronic Obstr. Pulm. Dis. 2021, 16, 3397–3403. [Google Scholar] [CrossRef]
- Rahi, M.S.; Thilagar, B.; Balaji, S.; Prabhakaran, S.Y.; Mudgal, M.; Rajoo, S.; Yella, P.R.; Satija, P.; Zagorulko, A.; Gunasekaran, K. The Impact of Anxiety and Depression in Chronic Obstructive Pulmonary Disease. Adv. Respir. Med. 2023, 91, 123–134. [Google Scholar] [CrossRef]
- Miah, A.; Hou, R. Anxiety and depression in Chronic Obstructive Pulmonary Disease: A systematic review and meta-analysis. Eur. Respir. J. 2023, 62, PA4138. [Google Scholar] [CrossRef]
- Liacos, A.; McDonald, C.F.; Mahal, A.; Hill, C.J.; Lee, A.L.; Burge, A.T.; Moore, R.; Nicolson, C.; O’halloran, P.; Cox, N.S.; et al. The Pulmonary Rehabilitation Adapted Index of Self-Efficacy (PRAISE) tool predicts reduction in sedentary time following pulmonary rehabilitation in people with chronic obstructive pulmonary disease (COPD). Physiotherapy 2019, 105, 90–97. [Google Scholar] [CrossRef]
- Harrison, S.L.; Robertson, N.; Goldstein, R.S.; Brooks, D. Exploring self-conscious emotions in individuals with chronic obstructive pulmonary disease: A mixed-methods study. Chron. Respir. Dis. 2016, 14, 22–32. [Google Scholar] [CrossRef]
- Woo, S.; Zhou, W.; Larson, J.L. Stigma Experiences in People with Chronic Obstructive Pulmonary Disease: An Integrative Review. Int. J. Chronic Obstr. Pulm. Dis. 2021, 16, 1647–1659. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ Br. Med. J. 2007, 335, 806–808. [Google Scholar] [CrossRef] [PubMed]
- Agustí, A.; Celli, B.R.; Criner, G.J.; Halpin, D.; Anzueto, A.; Barnes, P.; Bourbeau, J.; Han, M.K.; Martinez, F.J.; de Oca, M.M.; et al. Global Initiative for Chronic Obstructive Lung Disease 2023 Report: GOLD Executive Summary. Am. J. Respir. Crit. Care Med. 2023, 207, 819–837. [Google Scholar] [CrossRef] [PubMed]
- Graham, B.L.; Steenbruggen, I.; Miller, M.R.; Barjaktarevic, I.Z.; Cooper, B.G.; Hall, G.L.; Hallstrand, T.S.; Kaminsky, D.A.; McCarthy, K.; McCormack, M.C.; et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement. Am. J. Respir. Crit. Care Med. 2019, 200, E70–E88. [Google Scholar] [CrossRef] [PubMed]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- Gupta, N.; Pinto, L.M.; Morogan, A.; Bourbeau, J. The COPD assessment test: A systematic review. Eur. Respir. J. 2014, 44, 873–884. [Google Scholar] [CrossRef]
- Tangney, J.P. Conceptual and methodological issues in the assessment of shame and guilt. Behav. Res. Ther. 1996, 34, 741–754. [Google Scholar] [CrossRef]
- Leary, M.R. A Brief Version of the Fear of Negative Evaluation Scale. Pers. Soc. Psychol. Bull. 1983, 9, 371–375. [Google Scholar] [CrossRef]
- Collins, K.A.; Westra, H.A.; Dozois, D.J.A.; Stewart, S.H. The validity of the brief version of the Fear of Negative Evaluation Scale. J. Anxiety Disord. 2005, 19, 345–359. [Google Scholar] [CrossRef]
- Neff, K. Self-Compassion: An Alternative Conceptualization of a Healthy Attitude Toward Oneself. Self Identity 2003, 2, 85–101. [Google Scholar] [CrossRef]
- Munari, A.B.; Gulart, A.A.; Araújo, J.; Zanotto, J.; Sagrillo, L.M.; Karloh, M.; Mayer, A.F. Modified Medical Research Council and COPD Assessment Test Cutoff Points. Respir. Care 2021, 66, 1876–1884. [Google Scholar] [CrossRef]
- ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: Guidelines for the six-minute walk test. Am. J. Respir. Crit. Care Med. 2002, 166, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Spruit, M.A.; Watkins, M.L.; Edwards, L.D.; Vestbo, J.; Calverley, P.M.; Pinto-Plata, V.; Celli, B.R.; Tal-Singer, R.; Wouters, E.F. Determinants of poor 6-min walking distance in patients with COPD: The ECLIPSE cohort. Respir. Med. 2010, 104, 849–857. [Google Scholar] [CrossRef] [PubMed]
- von Leupoldt, A.; Janssens, T. Could targeting disease specific fear and anxiety improve COPD outcomes? Expert. Rev. Respir. Med. 2016, 10, 835–837. [Google Scholar] [CrossRef] [PubMed]
- Volpato, E.; Farver-Vestergaard, I.; Brighton, L.J.; Peters, J.; Verkleij, M.; Hutchinson, A.; Heijmans, M.; von Leupoldt, A. Nonpharmacological management of psychological distress in people with COPD. Eur. Respir. Rev. 2023, 32, 167. [Google Scholar] [CrossRef]
- Lundell, S.; Kalucza, S.; Coe, A.-B.; Hajdarevic, S.; Blomberg, A. Characteristics of people with COPD associated with emotions of shame and guilt. Eur. Respir. J. 2023, 62, OA4873. [Google Scholar] [CrossRef]
- Benzo, R.P.; Abascal-Bolado, B.; Dulohery, M.M. Self-management and quality of life in chronic obstructive pulmonary disease (COPD): The mediating effects of positive affect. Patient Educ. Couns. 2016, 99, 617–623. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Parameters | Moderate COPD (n = 44) | Severe COPD (n = 54) | p-Value |
|---|---|---|---|
| Age (years) | 65; (62.5, 69.5) | 67; (62, 71) | 0.46 |
| Male gender | 28 (63.63%) | 38 (70.37) | 0.56 |
| Height (cm) | 169.11 ± 6.39 | 167.14 ± 7.27 | 0.15 |
| Weight (kg) | 72.75 ± 10.38 | 73.29 ± 17.40 | 0.84 |
| BMI (kg/m2) | 25.48 ± 3.79 | 26.21 ± 6.03 | 0.46 |
| Comorbidities | 1.8 ± 0.9 | 3.4 ± 1.2 | <0.01 |
| PRAISE | 52; (47, 55) | 46.5; (39, 54) | <0.01 |
| BFNE | 27.5 ± 6.25 | 27.9 ± 6.55 | 0.75 |
| Self-kindness | 3.5; (3, 4) | 4; (3, 4.5) | 0.56 |
| Self-judgment | 3.5; (3, 4) | 3; (2, 3.5) | 0.04 |
| Common humanity | 3; (3, 4) | 3; (2.5, 3.5) | 0.02 |
| Isolation | 3.5; (3, 4) | 3; (2.5, 3) | <0.01 |
| Mindfulness | 4; (3, 4) | 3; (2.5, 3.5) | <0.01 |
| Overidentification | 3; (3, 3.5) | 3.5; (2.5, 4) | 0.84 |
| Total SCS-SF | 3.41; (3.33, 3.58) | 3.16; (2.91, 3.41) | <0.01 |
| Shame | 9; (6.5, 11) | 10; (6, 12) | 0.46 |
| Guilt | 10; (8, 12) | 12; (10, 16) | < 0.01 |
| Total SSGS | 20; (16, 22) | 22.5; (17, 26) | 0.01 |
| Anxiety | 6.5; (5.5, 7.5) | 10; (7, 12) | <0.01 |
| Depression | 6; (5, 7) | 7.5; (4, 9) | 0.06 |
| Total HADS | 13; (10.5, 15) | 16; (13, 20) | <0.01 |
| CAT | 20.77 ± 5.31 | 24.42 ± 5.18 | <0.01 |
| mMRC | 2; (2, 2) | 3; (2, 3) | <0.01 |
| 6MWT (m) | 286.46 ± 77.92 | 217.04 ± 70.16 | <0.01 |
| 6MWT (%) | 65.5; (56.5, 70) | 39.74; (34.74, 51.02) | <0.01 |
| FVC (L) | 2.72 ± 0.31 | 2.29 ± 0.43 | <0.01 |
| FVC (%) | 73.31 ± 3.97 | 66.41 ± 8.69 | <0.01 |
| FEV1 (L) | 1.77; (1.7, 1.91) | 1.09; (0.99, 1.15) | <0.01 |
| FEV1 (%) | 55; (54, 58) | 34; (31, 38) | <0.01 |
| FEV1/FVC | 0.66 ± 0.3 | 0.49 ± 0.9 | <0.01 |
| Parameters | r/rho for Moderate COPD (n = 44) | p-Value | r/rho for Severe COPD (n = 54) | p-Value |
|---|---|---|---|---|
| Anxiety–6MWT (m) | −0.32 | 0.03 | −0.23 | 0.07 |
| Depression–FVC (L) | −0.35 | 0.01 | −0.39 | 0.01 |
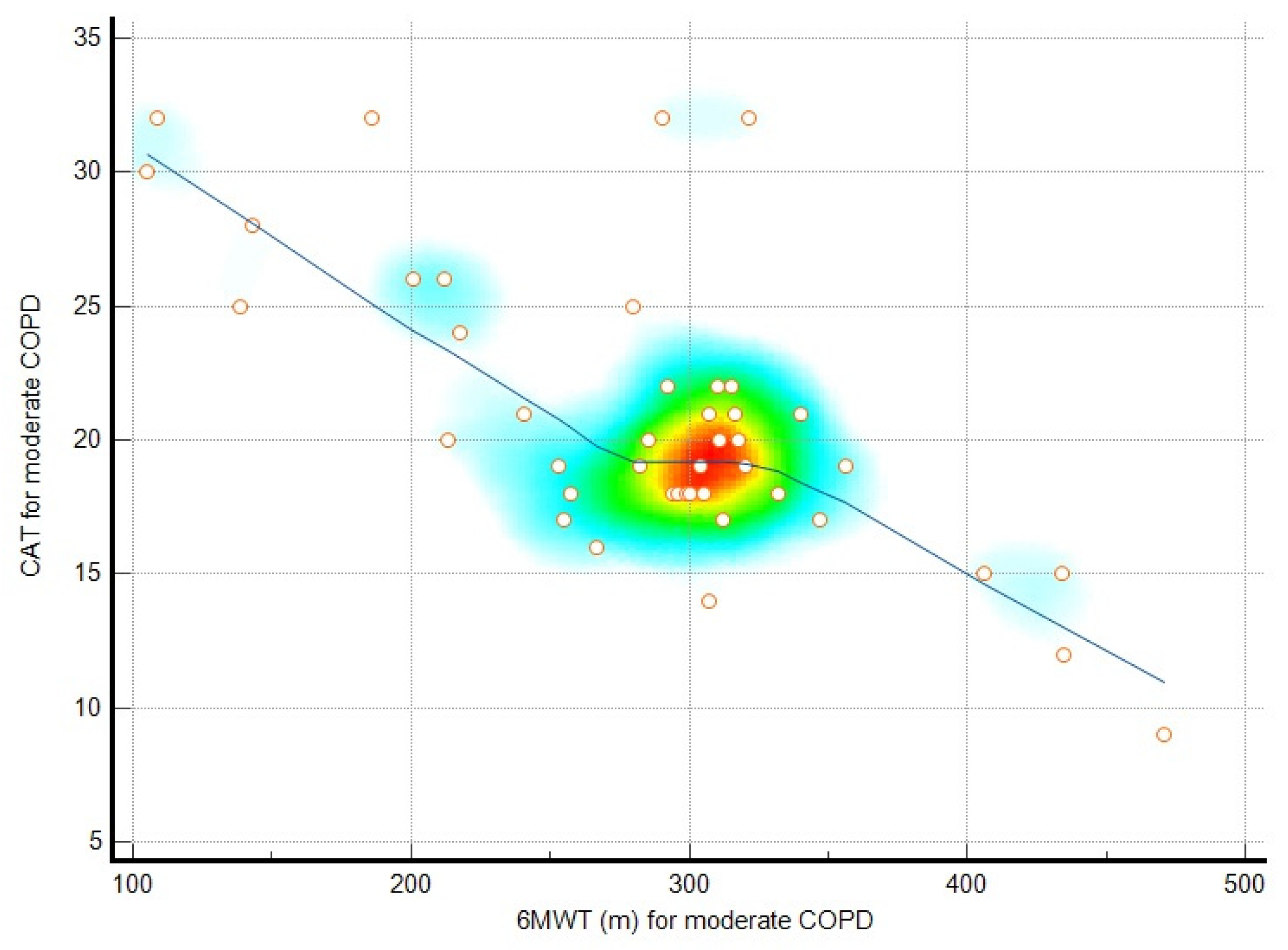
| CAT–6MWT (m) | −0.71 | <0.01 | −0.45 | <0.01 |
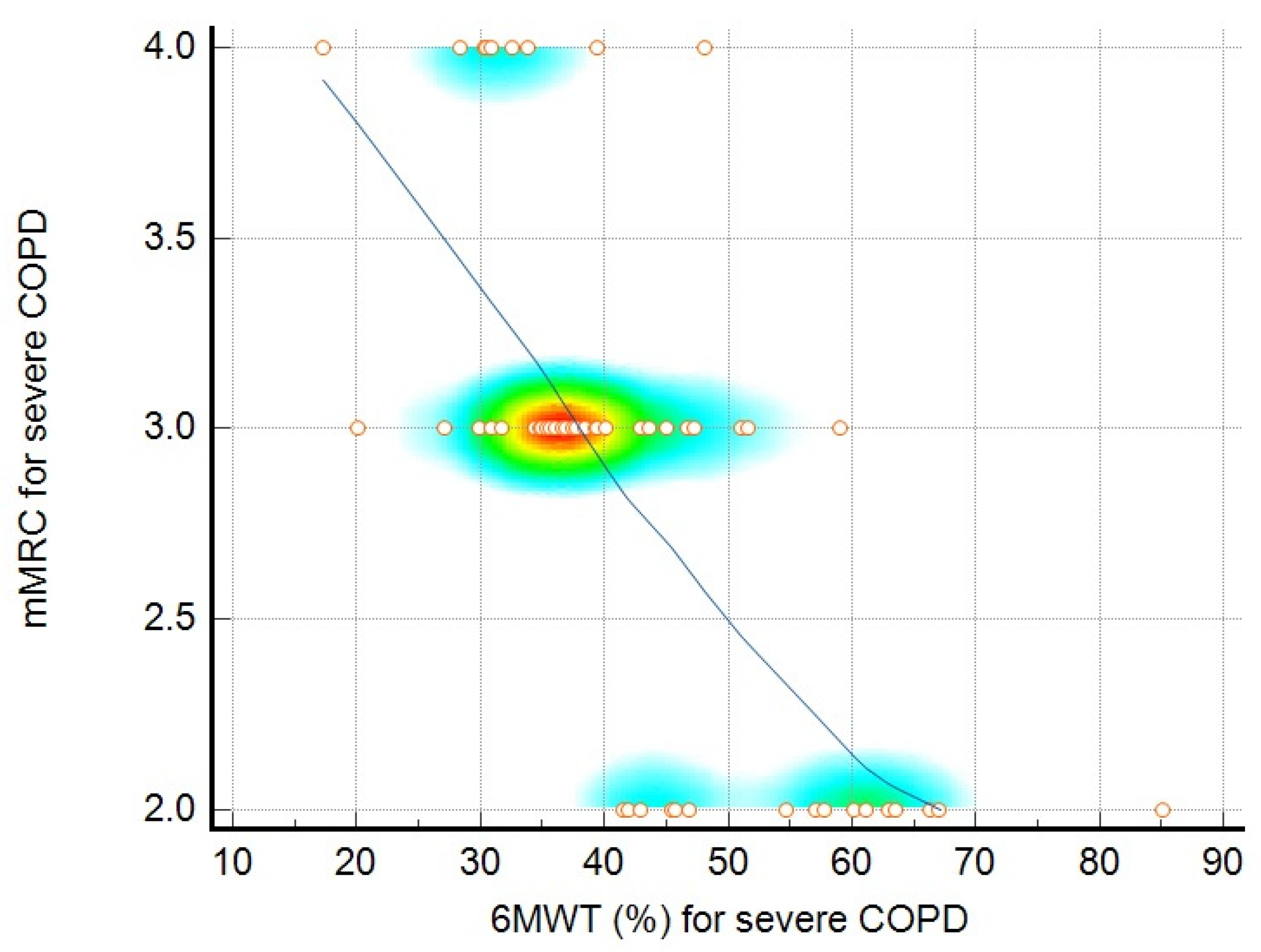
| mMRC–6MWT (%) | −0.46 | <0.01 | −0.70 | <0.01 |
| PRAISE–6MWT | 0.34 | 0.02 | 0.26 | 0.04 |
| Depression–CAT | 0.21 | 0.08 | 0.34 | 0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crisan, A.F.; Pescaru, C.C.; Maritescu, A.; Stoicescu, E.R.; Carunta, V.; Oancea, C. The Impact of Chronic Obstructive Pulmonary Disease Severity on Psychological and Functional Outcomes: A Cross-Sectional Analysis. J. Clin. Med. 2025, 14, 1865. https://doi.org/10.3390/jcm14061865
Crisan AF, Pescaru CC, Maritescu A, Stoicescu ER, Carunta V, Oancea C. The Impact of Chronic Obstructive Pulmonary Disease Severity on Psychological and Functional Outcomes: A Cross-Sectional Analysis. Journal of Clinical Medicine. 2025; 14(6):1865. https://doi.org/10.3390/jcm14061865
Chicago/Turabian StyleCrisan, Alexandru Florian, Camelia Corina Pescaru, Adelina Maritescu, Emil Robert Stoicescu, Vlad Carunta, and Cristian Oancea. 2025. "The Impact of Chronic Obstructive Pulmonary Disease Severity on Psychological and Functional Outcomes: A Cross-Sectional Analysis" Journal of Clinical Medicine 14, no. 6: 1865. https://doi.org/10.3390/jcm14061865
APA StyleCrisan, A. F., Pescaru, C. C., Maritescu, A., Stoicescu, E. R., Carunta, V., & Oancea, C. (2025). The Impact of Chronic Obstructive Pulmonary Disease Severity on Psychological and Functional Outcomes: A Cross-Sectional Analysis. Journal of Clinical Medicine, 14(6), 1865. https://doi.org/10.3390/jcm14061865